Article Text

Abstract
Background/Aim This scoping review examined the breadth and outcomes of controlled trials testing the effect of physical activity and exercise interventions across all mental health outcomes for mental health promotion and indicated prevention studies in young people.
Methods The literature search was conducted using ‘Evidence Finder’.
Results Thirty publications were included. Available evidence suggested that interventions of varying intensity may lead to a reduction in depression symptoms and that moderate-to-vigorous-intensity and light-intensity interventions may reduce anxiety symptoms. Effects of physical activity/exercise interventions on additional mental health outcomes were also shown; however, the number of studies was small, indicating a limited evidence base. Robust research regarding the effects of physical activity/exercise on mental health promotion and as an indicated prevention strategy in young people is lacking.
Conclusion The available evidence suggests that physical activity/exercise is a promising mental health promotion and early intervention strategy and warrants further investigation.
- well-being
- physical activity
- prevention
- adolescent
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known
Considerable impairment in functioning is associated with elevated mental disorder symptoms in young people, which are equally, if not more, prevalent than diagnosed disorders.
Young people are often reluctant to seek help for mental health concerns; therefore, interventions need to be youth-friendly, acceptable, feasible and non-stigmatising.
Physical activity/exercise is a non-stigmatising intervention with few side effects and is viewed by young people as helpful in promoting mental health and treating mental health problems.
What are the new findings
Interventions of varying intensity may lead to a reduction in depression symptoms.
Moderate-to-vigorous-intensity and light-intensity interventions may reduce anxiety symptoms.
Effects of physical activity/exercise interventions on additional mental health outcomes were also shown; however, the number of studies was small, indicating a limited evidence base.
Introduction
Youth mental health disorders are expected to be a leading cause of disability in developed countries by 2020.1 Therefore, the promotion of mental health and the prevention of mental health disorders are paramount. Significantly impaired function is associated with increased mental health disorder symptoms in young people, such as depression and anxiety symptoms, which are equally, if not more, prevalent than diagnosed disorders.2–4 Indeed, young people with increased risk of or increased incidence of mental disorder symptoms have significant social and occupational functioning impairments and experience high levels of psychological distress.5 Given the high prevalence, interventions that promote mental health as well as target the early phases or subthreshold levels of disorder are urgently required.6
Access to interventions that promote mental health and that are effective in the early stages of illness has the potential to rapidly improve the mental health and functioning of young people and prevent the negative impact of persistent mental illness.7 Young people are often reluctant to seek help for mental health concerns; therefore, interventions need to be youth-friendly, acceptable, feasible and non-stigmatising8 and matched to their specific needs.9–11
Physical activity (PA)/exercise is a non-stigmatising intervention with few side effects12 and is viewed by young people as helpful in promoting mental health and treating mental health problems.13 Despite these positive beliefs, disengagement from regular exercise, PA and sporting clubs steadily increases during adolescence,14 15 coinciding with the average age of onset of mental health problems.16
Rationale
While emerging evidence indicates that PA/exercise is effective in reducing depression symptoms in young people,17 18 few studies have examined PA/exercise as a mental health promotion strategy for other mental health problems. One single meta-analysis has demonstrated the benefits of PA on mental health in adolescents up to the age of 18 years.19 There are no existing systematic or scoping reviews across all youth mental health outcomes of PA/exercise for mental health promotion and indicated prevention that include people aged up to 25 years.
Objectives
This review addressed the following research question: what is known about the effectiveness of PA/exercise for mental health promotion and as an indicated prevention strategy in young people? (in all contexts: university/school, community, hospital, correctional facility). ‘Physical activity’ is defined as any bodily movement produced by skeletal muscles that results in energy expenditure, and ‘exercise’ is the planned, structured and repetitive undertaking of PA for the purpose of maintaining or improving health-related or skill-related components of physical fitness.20 21 The term ‘mental health outcomes’ refers to mental health symptoms collected by specific quantitative outcome measures of symptom severity, for example, depression symptoms as measured using the Depression Anxiety Stress Scale. It also refers to general indicators of mental health, such as quality of life and well-being,22 including depression symptoms, anxiety symptoms, stress, mood states, substance use, self-esteem, affect, resilience, self-confidence and self-concept.
We aimed to provide a comprehensive overview of the breadth and outcomes of controlled trials testing the effect of PA/exercise across all mental health outcomes. Therefore we included both mental health promotion and indicated prevention studies. We also aimed to describe the nature of the interventions, including specification of dose of the activity, as an initial contribution to informing translation into practice. We have selected these outcomes so that the findings can be interpreted in relation to current government guidelines for recommended amounts of PA engagement in the general population, which focus on engagement in moderate-vigorous-intensity PA/exercise.23–25
The following were the objectives:
To examine the extent and range of outcomes from PA/exercise prevention interventions in a youth mental health context.
To collate mental health, quality-of-life and functioning outcomes.
To present an overview of the impact of PA/exercise across mental health symptomology.
To examine the specification of dose (intensity) of PA/exercise interventions.
Methods
Protocol and registration
The review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) guidelines26 and the five-stage framework outlined in Arksey and O’Malley.27 A review protocol was not published.
Eligibility criteria
To determine study eligibility, the following criteria were applied: young people (mean age between 12 and 25.9 years); published from 1980 to 2017 as youth mental health was not considered a discrete field prior to 198028; included a PA/exercise intervention and a comparison condition; reported on the quantitative effects of at least one mental health symptom, such as depression symptoms; PA/exercise interventions lasted longer than 3 weeks in duration29 30; study designs were randomised controlled trials (RCTs) or non-RCTs; and studies were published in English. Excluded studies were unpublished studies or studies with a population that had a diagnosis of a mental disorder, as we have examined PA/exercise as a treatment for mental illness in our companion paper to this article,31 and non-intervention studies.
Information sources
We have included a broad range of outcomes associated with the risk of mental health problems, such as stress and body image, and examination of the dose of PA/exercise in the interventions. The search was conducted using ‘Evidence Finder’ (www.orygen.org.au), which is a comprehensive database of all available published controlled trials and systematic reviews of interventions in the youth mental health field.28 32 The ‘Evidence Finder’ is an Australian initiative developed by Orygen, The National Centre of Excellence in Youth Mental Health and headspace, National Youth Mental Health Foundation.26 27 The searchable database is populated annually using comprehensive and systematic searches of the Embase, MEDLINE, PsycINFO and Cochrane Library databases, coupled with strict and reproducible inclusion criteria to identify studies (see refs 26 27 for detailed methodology). It includes research published from 1980 to 2017 and contains all available prevention, treatment and relapse prevention studies in young people (mean age 6–25 years), across the following mental illnesses: anxiety, depression, bipolar, eating disorders, psychosis, substance use and suicide-self harm. It contains controlled trials (including RCTs and quasi-randomised studies), systematic reviews and meta-analyses, published in English. Unpublished trials are not included within the Evidence Finder. Searches were conducted in July 2018 (updated April 2019) and all studies classified as ‘Physical activity/Exercise’ were screened. Reference lists of identified literature were searched for suitable primary research based on titles in the first instance, and if relevant abstracts and full-text review.
Search
The following criteria were applied to the ‘Evidence Finder’ search engine (https://www.orygen.org.au/Training/Evidence-Finder): (1) mental health or substance use problem: ‘all’; (2) stage of illness: ‘all’; (3) treatment/intervention: ‘complementary and alternative interventions (CAM)’, followed by ‘Physical activity/exercise’; (4) publication date: ‘all’; and (5) keyword: none. Advanced options selected include systematic reviews, RCTs and controlled clinical trials.
Selection of sources of evidence
Title/abstract screening was undertaken by two authors (MP, AP). Full texts were independently reviewed by two authors (MP, AP, MC). There were no conflicts.
Data charting process
Data charting27 was undertaken by a single author (MP) using a specifically designed extraction form (online supplementary tables 1 and 2). Data charting was done independently by a single author and extraction was checked by a second author (TC, APB). Data were obtained directly and only from the published articles.
Supplemental material
Two assessors (NS, RP) reviewed each study for objective (heart rate (HR), %maximal HR, %HR reserve, %1-repetition maximum, per cent of maximal oxygen uptake (%VO2max)) and subjective (ratings of perceived exertion) measures of PA/exercise intensity. Using these measures, interventions were classified as light intensity, light to moderate intensity, moderate intensity, moderate to vigorous intensity, or vigorous intensity for aerobic30 and resistance exercise.33 In cases where the exercise interventions were poorly described, we attempted, where possible, to estimate an exercise intensity based on the compendium of exercise energy expenditure.34 We did not contact authors when insufficient information was provided in the published articles.
Data items
The following data were extracted: mental health outcomes assessed, tools used to measure mental health outcomes assessed, country of study origin, setting of study conduct, study design type, participants, sample size, mean age, overall findings, assessment timepoints if intention-to-treat analysis was used (as shown in online supplementary table 1), characteristics of the intervention, characteristics of the control group, personnel delivering the intervention, delivery format, and duration and frequency of the delivered intervention (as shown in online supplementary table 2).
Critical appraisal of individual sources of evidence
A critical appraisal of individual sources of evidence was not conducted in the current scoping review.
Synthesis of results
A ‘descriptive-analytical’ method was applied which involved applying a common analytical framework, which was the mental health outcome.27
PA/exercise interventions generally vary the dose, where the combination of intensity (light, moderate or vigorous) and duration (min/week) determines the session and intervention dose. Due to heterogeneity of the duration of interventions and that PA/exercise intensity is strongly linked to affective responses and sustainability, we focused on PA/exercise intervention intensity.
Results
Selection of sources of evidence
Eighty-three records were returned in ‘Evidence Finder’ and were screened for eligibility, and an additional 19 eligible papers were identified via screening of the references lists of reviews identified by ‘Evidence Finder’. As shown in figure 1, after full-text screening, a total of 29 studies met the inclusion criteria and were included in the current scoping review.
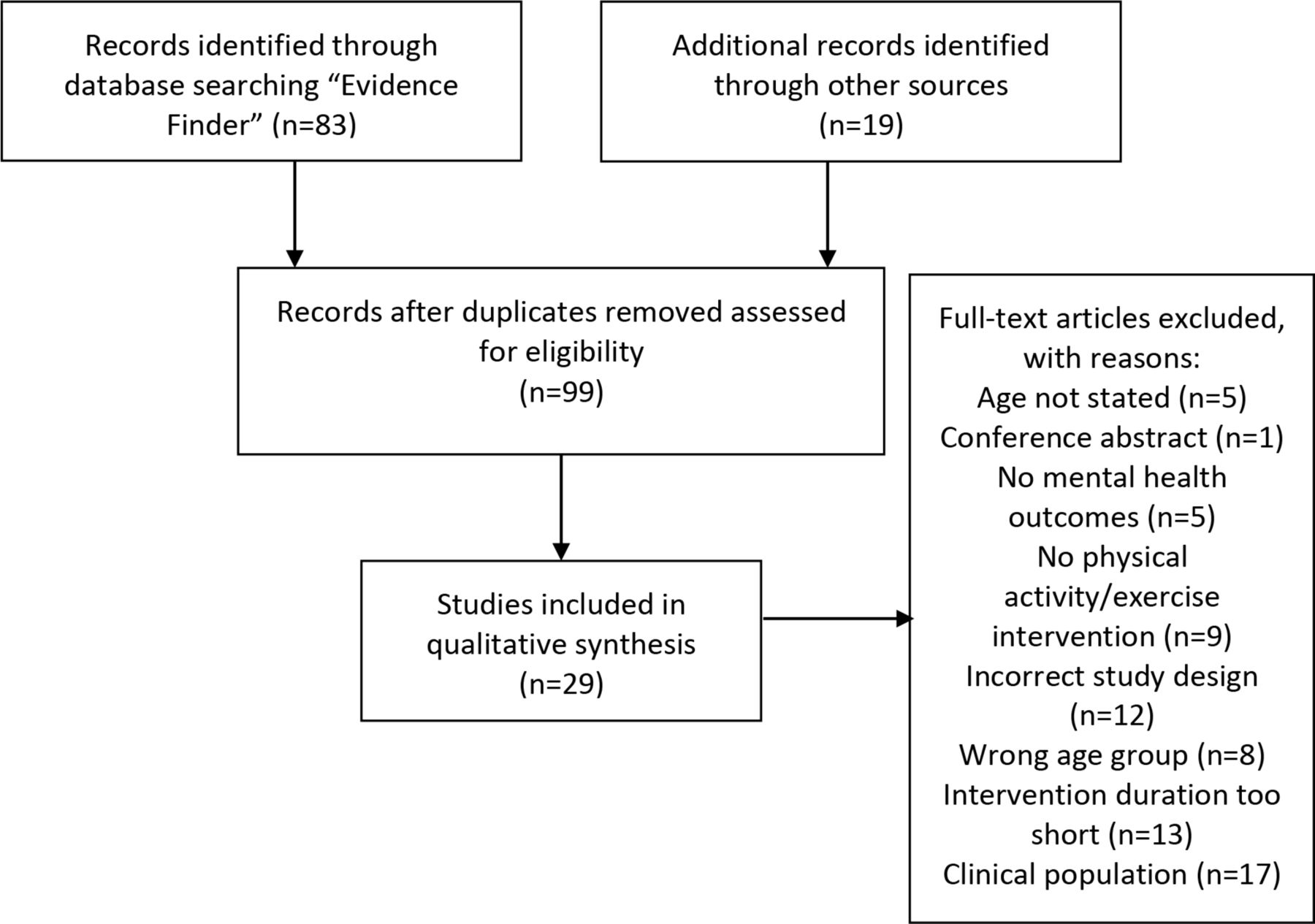
PRISMA flow diagram showing reasons for study exclusions. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of sources of evidence
Online supplementary table 1 shows that 4 trials were not randomised,35–38 1 was a cross-over RCT,39 5 were cluster RCTs40–44 and 20 were RCTs. Eight studies included young people with elevated mental disorder symptoms at baseline, including anxiety sensitivity,45 anxiety or depression symptoms,37–39 46 47 or high substance use,48 49 and the remaining 22 involved young people without mental health symptoms. Figure 2 shows the distribution of mental health outcomes studied. Online supplementary table 2 shows that 3 interventions were delivered individually, 9 did not state the mode of delivery and 18 were group-based. All but seven studies delivered supervised PA/exercise interventions. These seven studies did not specify if interventions were supervised or not.
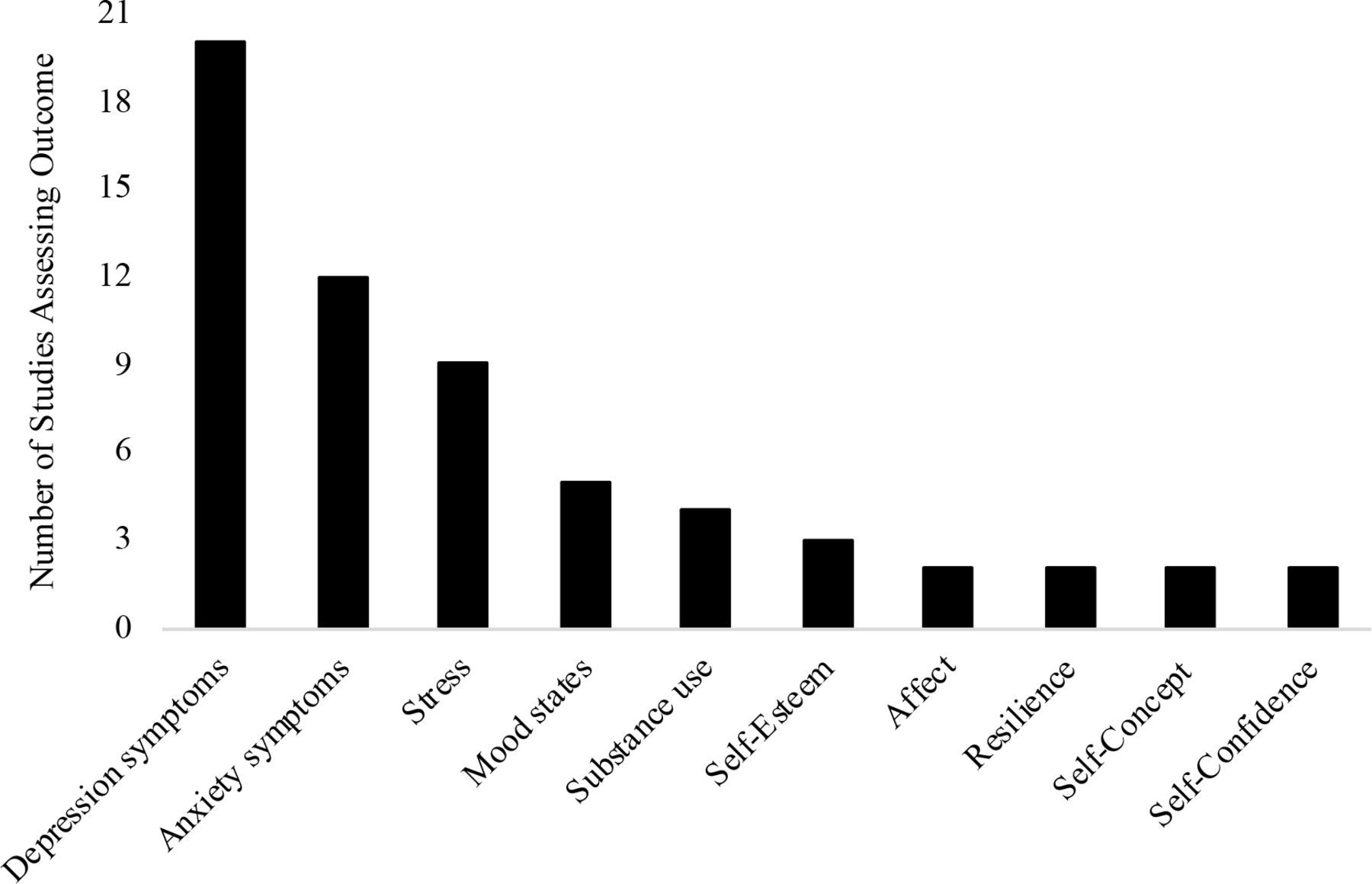
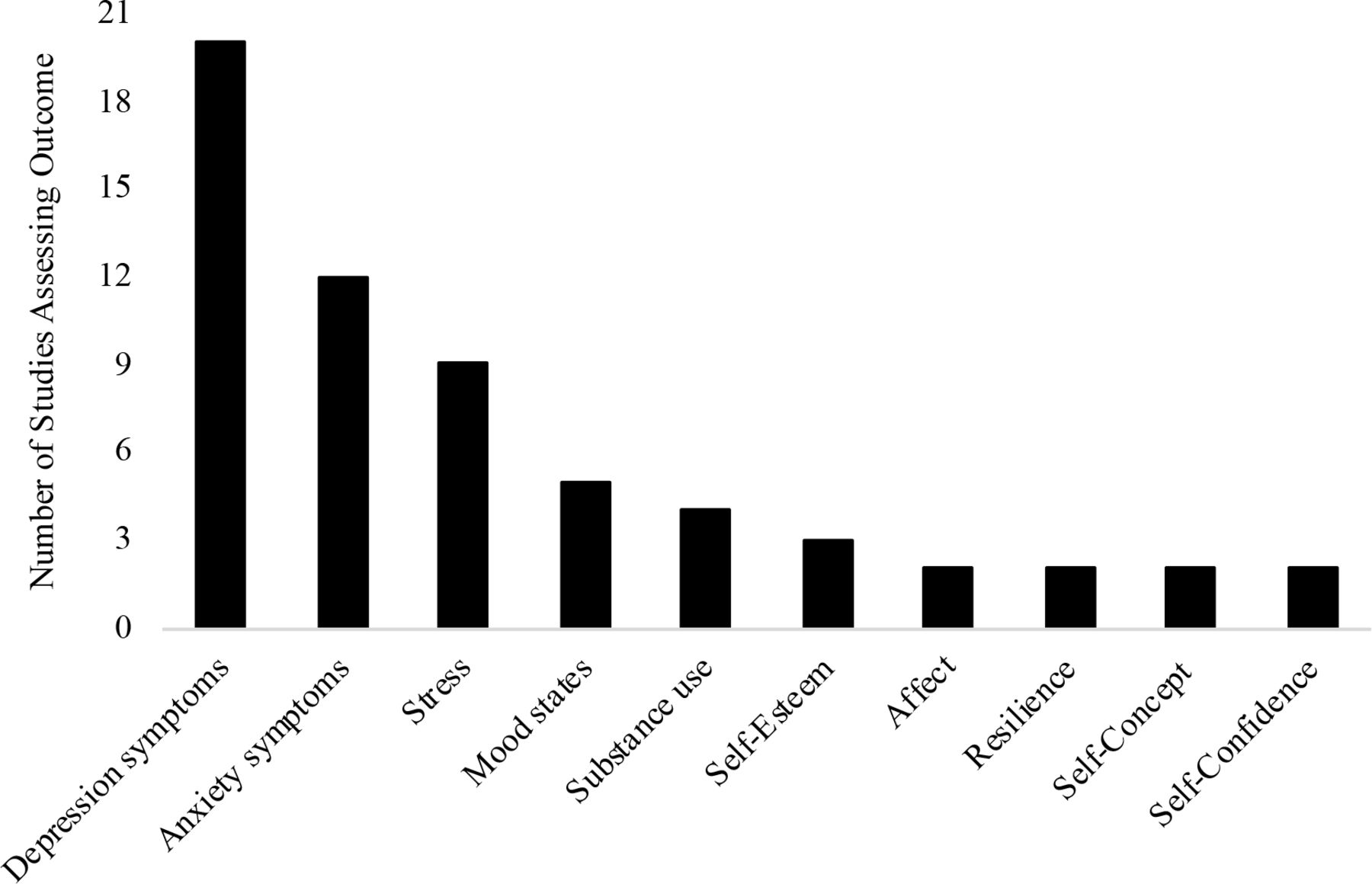
Distribution of mental health outcomes studied. The following outcomes were measured only once and are not depicted in figure 1: anger, anxiety sensitivity, body image, burn-out, fatigue, functioning, hopefulness, life purpose and satisfaction, mindfulness, psychological symptoms and distress, quality of life, self-perception, situational motivation, and social skills.
Results of sources of evidence
The relevant extracted data relating to the review questions and objectives are shown in online supplementary tables 1 and 2.
Types of interventions
Figure 3 shows the distribution of interventions studied by PA/exercise intensity, most commonly delivered in supervised group settings. Moderate-to-vigorous-intensity interventions were the most frequently examined, encompassing a broad range of activities, including strength training, gymnastics, enhanced physical education classes and aerobic exercises. Moderate-intensity interventions formed a considerable portion of those examined, and included activities such as team sports, cycling, jogging and exercising to music. Finally, a smaller proportion of studies examined light-intensity activities, including yoga, t’ai chi, and conditioning or stretching exercises.

{kind=link}
{kind=link}
{kind=link}
Distribution of interventions studied by intensity.
Synthesis of results
Depression symptoms
Twenty studies assessed depression symptoms. As several studies included more than one active intervention condition (ie, three-arm or four-arm studies), the number of comparisons reported here is greater than 20. Three studies assessed vigorous-intensity interventions, and two of these showed decreases in depression symptoms. One of these included incarcerated male adolescents and compared a vigorous-intensity with a moderate-intensity intervention.35 The second included university students and compared vigorous-intensity PA/exercise with progressive muscle relaxation (PMR); however, in this study, a reduction in depression symptoms was only reported at mid-intervention.50 In the third study, a vigorous-intensity intervention did not improve depression symptoms in unemployed young men, compared with a wait-list group.51
Three studies assessed moderate-to-vigorous-intensity interventions and a further three assessed interventions of unspecified intensity, but likely moderate-to-vigorous. In five of these, the interventions decreased depression symptoms.47 52–55 Four of these compared moderate-to-vigorous-intensity with no intervention,47 53–55 and the remaining study used a standard rehabilitation programme.52 The sixth study compared two moderate-to-vigorous-intensity interventions and found no effect of either on depression symptoms.40
Three studies delivered moderate-intensity interventions and a further four assessed interventions of unspecified intensity, but likely moderate. In two of these, moderate-intensity interventions decreased depression symptoms, one compared with a wait-list group39 and the other with health promotion, but only in the subsample of adolescents with elevated baseline depression symptoms.42 In the remaining five studies, moderate-intensity interventions had no effect on depression symptoms, compared with wait-list,56 no intervention,37 57 vigorous-intensity intervention35 or health education.41
One study assessed a light-moderate-intensity intervention and found no reduction in depression symptoms in women with high anxiety sensitivity, compared with health education.45 One study assessed a light-intensity intervention56 and a further three assessed interventions of unspecified intensity, but likely light-intensity.38 55 58 In one of these, the light-intensity intervention decreased depression symptoms compared with no intervention.38 The remaining three studies found no effect.55 56 58 A single study assessed a psychological intervention with a light-intensity component, finding it decreased depression symptoms in university students, compared with a moderate-intensity intervention and no intervention.57
Two studies did not provide sufficient information to assess intervention intensity, and neither showed reductions in depression symptoms.36 46
Anxiety symptoms
Twelve studies assessed anxiety symptoms, and six studies included more than one active intervention condition. In five studies, PA/exercise reduced anxiety symptoms.38 40 52 57 59 One study assessed a vigorous-intensity intervention and found no effect in university students with a high number of negative life events, compared with PMR or no intervention.50 One study assessed a moderate-to-vigorous-intensity intervention and found that both it and a likely light-intensity intervention decreased anxiety in university students, with no difference between the groups.55 A further five studies did not specify intensity but were likely moderate-to-vigorous.40 47 52 59 60 In two of these, the moderate-to-vigorous-intensity intervention reduced anxiety symptoms in adolescents compared with a second moderate-to-vigorous intervention (two types of physical education classes)40 and in adolescents in juvenile detention, compared with a rehabilitation programme.52 An additional study analysed the results of two moderate-to-vigorous-intensity interventions, by combining the resistance and aerobic exercise groups together, and found that these reduced anxiety in male university students with elevated anxiety/depression symptoms, compared with no intervention.47 The fourth study found that a moderate-to-vigorous-intensity intervention reduced anxiety symptoms from preintervention to postintervention in university students. This study however did not state whether the moderate-to-vigorous-intensity intervention influenced anxiety symptoms compared with the no-intervention group.60 The fifth study found a moderate-to-vigorous-intensity intervention had no effect in university students, compared with a stress management intervention or no intervention.59
Four studies did not specify intensity, but were likely moderate. In two of these, moderate-intensity interventions did not reduce anxiety compared with health promotion education.41 42 In another study, both a likely moderate-intensity intervention and a stress management intervention decreased anxiety, but a likely moderate-to-vigorous-intensity intervention did not.59 In the fourth study, a moderate-intensity intervention did not reduce anxiety, but a light-intensity intervention that also contained mindfulness and cognitive components did reduce anxiety, compared with no intervention.57
One study found a light-to-moderate-intensity intervention did not reduce anxiety symptoms in women with high anxiety sensitivity, compared with health education.45 Three studies did not specify intensity but were likely light intensity, and all decreased anxiety in university students.38 55 57 In one of these, a second light-intensity intervention did not improve anxiety compared with no intervention.38 The remaining two studies, as described above, found that the light-intensity interventions reduced anxiety as effectively,55 or more effectively, than moderate-intensity interventions.57
Stress
Nine studies assessed stress. As several studies included more than one active intervention condition, the number of comparisons reported here is greater than nine. Two studies delivered a vigorous-intensity intervention, and one of these found it decreased stress in adolescents, compared with no intervention.61 The second study found that the intervention did not decrease stress among unemployed young men, compared with a wait-list group.51
Three studies assessed a moderate-to-vigorous-intensity intervention or a likely moderate-to-vigorous-intensity intervention.44 53 59 In one of these, the intervention decreased stress, as did a moderate-intensity intervention and a psychological intervention, compared with no intervention, in university students.59 In the remaining two studies moderate-to-vigorous-intensity intervention had no effect on stress in individuals who were included on the basis of low levels of PA, compared with no intervention,53 or in adolescents when compared with a light-intensity intervention.44
One study of a moderate-intensity intervention found that it decreased stress in adolescents, compared with no intervention,61 and a further three did not specify intervention intensity but were likely moderate.43 57 59 In one of these, both the moderate-intensity intervention and the psychological treatment condition decreased stress in university students, compared with no intervention, as stated above.59 In the remaining two studies43 57 moderate-intensity interventions had no effect on stress compared with a likely light-intensity intervention43 or no intervention.57
One study assessed a light-to-moderate-intensity intervention and found that it decreased stress in women with high anxiety sensitivity, compared with health education.45 Three studies did not specify intervention intensity but were likely light-intensity.38 43 44 Only one of these found that the intervention decreased stress in university students with elevated combined symptoms of depression, anxiety and stress, compared with no intervention,38 with the remaining two interventions showing no effect on stress compared with a moderate-intensity intervention43 and a moderate-to-vigorous-intensity intervention44
Mood states
Five studies assessed mood states. One study assessed a vigorous-intensity intervention and found it improved mood states in adolescents, compared with a moderate-intensity intervention and no intervention.61
Two studies examined moderate-to-vigorous-intensity interventions,61 62 and a further two did not specify intensity but were likely moderate-to-vigorous-intensity.44 52 In two of these, the moderate-to-vigorous-intensity interventions improved mood states, compared with a rehabilitation programme52 and no intervention.62 In one of these, the comparison interventions (PMR and discussion) also improved mood states (stress only) compared with no intervention.62 Moderate-to-vigorous-intensity intervention had no effect on mood states in the remaining two studies, compared with no intervention61 or a light-intensity intervention.44
Two studies examined moderate-intensity interventions, and neither had an effect on mood states in adolescents, compared with no intervention61 or a light-intensity intervention.43 The second study found that the light-intensity intervention improved mood states.43
Summary of mood state findings
Table 1 shows the percentage and frequency of the total number of reviewed studies that showed beneficial effects of a PA/exercise intervention compared with (1) a non-PA/exercise control group intervention, (2) a wait-list or no intervention and (3) a second PA/exercise intervention. Table 2 shows the percentage and frequency of the total number of reviewed studies that showed beneficial effects of a PA/exercise according to the intensity of the delivered intervention.
Percentage (frequency) of total reviewed studies that showed beneficial effects of physical activity (PA)/exercise interventions compared with a control intervention
Percentage (frequency) of total reviewed studies that showed beneficial effects of physical activity/exercise interventions depending on the intensity of the intervention
Substance use
Four studies measured substance use. In one of these, a vigorous-intensity intervention decreased methamphetamine use in unemployed young men, compared with a wait-list group.51 In another, the likely moderate-intensity intervention decreased substance use, when delivered to university students with high anxiety sensitivity scores, compared with health education.42 The remaining two studies compared two PA/exercise interventions in sedentary university students who engaged in hazardous drinking. In one of these, contracting to complete light-moderate-intensity activities plus contingency management did not influence substance use, compared with a single session of motivational enhancement therapy for exercise.48 These same authors later found that both contingency management (to contract to complete moderate-to-vigorous activities) and contingency management, in addition to reinforcing participants for completion of moderate-to-vigorous exercise activities, decreased alcohol use, with no difference between the groups.49
Self-esteem
Three studies measured self-esteem. One study found that a moderate-to-vigorous-intensity intervention improved self-esteem in adolescents, compared with a second moderate-to-vigorous-intensity intervention (two variations of physical education classes).40 A second study found that a moderate-to-vigorous-intensity intervention improved self-esteem compared with a rehabilitation programme in adolescents in juvenile detention.52 The third study found that an unspecified, likely light-intensity intervention improved self-esteem in university students and employees, compared with no intervention.58
Affect
Two studies measured affect and both included a moderate-intensity and light-intensity intervention, or unspecified but likely moderate-intensity and light-intensity. In one study, neither intervention influenced affect compared with wait-list in children with obesity.56 In the second study, the light-intensity intervention improved affect compared with the moderate-intensity intervention in adolescents.43
Resilience
Two studies measured resilience and compared two PA/exercise interventions in adolescents. In one of these the light-intensity intervention increased resilience while the moderate-to-vigorous-intensity intervention decreased resilience.44 In the second study, there was no difference between a light-intensity intervention and a moderate-intensity intervention.43
Self-concept
Two studies measured self-concept, which refers to one’s views, attitudes and beliefs about the self. In one, a vigorous-intensity intervention improved self-concept, compared with a likely moderate-intensity intervention, in incarcerated adolescents.35 In the second study, a light-intensity intervention improved self-concept, compared with a likely moderate-to-vigorous-intensity intervention in secondary schools students.63
Self-confidence
Two studies measured self-confidence. A moderate-to-vigorous-intensity intervention improved self-confidence compared with no intervention in university students.60 There was no difference between a likely light-intensity intervention and moderate-intensity intervention, both of which did not influence self-confidence during periods of stressful life events in secondary school students.44
Outcomes reported once
Both a light-to-moderate-intensity intervention and a health education intervention reduced anxiety sensitivity in women with high anxiety sensitivity, with no difference between groups.45 A likely light-intensity intervention improved fatigue and quality of life, while a resistance-based intervention of unspecified intensity improved body image, in university students and employees, compared with no intervention.58 Hopefulness increased following two likely light-intensity interventions in university students with elevated depression symptoms compared with no intervention.38 A likely light-intensity intervention and a moderate-intensity intervention had no effect on mindfulness, anger expression and positive psychology,43 or on life purpose and satisfaction, in secondary school students.44 The likely light-intensity intervention did, however, improve anger control.44 Light-intensity intervention or moderate-intensity intervention had no effect on scholastic competence and social competence in children with obesity; however, in this same study, the moderate-intensity intervention improved physical self-worth, global self-worth, strength competence and attractive body adequacy, and the light-intensity intervention improved global self-worth, compared with wait-list.56 Social skills improved following a likely moderate-intensity intervention in university students with high anxiety sensitivity, compared with health education.42 A likely moderate-intensity intervention, a likely moderate-to-vigorous-intensity intervention or stress management did not decrease personal burn-out among university students compared with no intervention.59 Vigorous-intensity intervention had no effect on psychological symptoms and distress in university students, compared with no intervention or PMR.50 Situational motivation increased following an intervention of unspecified intensity in university students, compared with stretching.46
Intensity of interventions
Of the studies that examined vigorous-intensity interventions, a considerable proportion found positive outcomes on depression symptoms,35 50 51 stress43 and mood states,61 but not for anxiety.50 Moderate-to-vigorous-intensity interventions showed improvements in depression symptoms,40 47 52–55 anxiety symptoms,40 47 52 55 59 60 self-esteem40 52 and mood states.52 62 There was less support for moderate-intensity interventions in reducing depression symptoms, with only two positive studies from seven39 42 and only one positive study for anxiety59 and stress59 from the four that measured these outcomes. There was no support for moderate-intensity interventions in improving mood states from the two studies that measured this. The current review identified seven studies assessing the impact of light-intensity interventions on mental health outcomes, and the results of these were generally positive for anxiety,38 55 57 mood states43 44 and affect,43 but not for depression55 56 58 and stress.38
Discussion
This scoping review examined the extent and range of outcomes from PA/exercise interventions in youth mental health. We presented an overview of the effects of PA/exercise interventions across mental health outcomes and mental health-related factors. We examined outcomes according to intervention intensity in order to facilitate the translation of research findings into clinical practice.
Summary of evidence
Elevated mental disorder symptoms
The range of mental health and quality-of-life outcomes examined may indicate the broad applicability of PA/exercise as an intervention for emerging mental health problems in young people. Of the eight included studies that recruited participants on the basis of elevated symptoms of mental health disorder at baseline, five demonstrated the effect of PA/exercise interventions in reducing symptoms of depression38 39 46 47 and high substance use,49 indicating the potential of PA/exercise as an indicated or targeted prevention strategy.
A mental health-promoting strategy
Of the 22 included studies that did not recruit participants on the basis of elevated symptoms of mental health disorder, there was a demonstrated effect of PA/exercise improving mental health in 17 of these: affect,43 anxiety symptoms,40 52 57 59 body image,58 depression symptoms,35 52–55 57 fatigue,58 functioning,44 mood states,43 44 52 61 62 self-perception,56 quality of life,58 resilience,44 self-concept,35 63 self-esteem,40 52 social skills,42 stress57 59 61 and substance use,42 51 indicating that PA/exercise has a potentially promising effect as a mental health-promoting strategy.
Future research and practice
There are indications that outcomes may vary depending on intervention intensity. Given the mixed findings in regard to intensity, a future research agenda could be testing and comparing the feasibility, acceptability and effectiveness of different intensities head to head, to seek a threshold dose for benefit. Current government guidelines for recommended amounts of PA engagement in the general population focus on moderate-vigorous-intensity PA/exercise23–25; however, the results of this scoping review indicate that light-intensity PA/exercise shows benefit for some mental health outcomes. This is important as the experience of negative affect when participating in higher-intensity PA/exercise is more likely to occur compared with participating in lower-intensity PA/exercise.64 As affect appears to be an important factor in predicting adherence to PA/exercise,64 65 light-intensity interventions may be beneficial for people who are unlikely to adhere to more vigorous-intensity interventions or are commencing from a very low baseline level of PA. Light-intensity interventions may also have the capacity to be delivered by a range of professionals across different settings,66 be less reliant on group-based formats and may also be a good basis on which to develop self-efficacy for PA/exercise,67 which might then lead to uptake of more intensive types of PA/exercise,68 providing impetus to examine these interventions. Given that our review identified findings to indicate that likely light-intensity interventions improve anxiety symptoms38 55 57 and mood states,43 44 further research should be conducted to better understand the potential benefits of light-intensity interventions in youth mental health.
Future research should also consider the importance of self-selection of activity type and intensity as autonomy is proposed as one of the three basic psychological needs fundamental to positive mental health,69 70 and as when intensity is self-selected, rather than imposed, participants experience greater tolerance to higher-intensity PA/exercise.64 This indicates health promotion strategies should be designed to suit a diverse range of needs and preferences, and should be designed to be driven by individuals, in order to improve uptake and adherence.
The results of the present scoping review highlight the importance of maintaining and building PA and exercise programme in primary, secondary and tertiary education settings in order to promote mental health among young people. In general, preventive interventions are not currently widely implemented in schools and communities.71 72 Mendelson et al73 recently highlighted that school-based interventions have small but significant effects in terms of preventing the onset of depression in young people. Even if modestly effective, the population-level implementation of prevention interventions would help young people to develop healthy coping strategies that could protect them against the development of depression.74 Therefore, it would be valuable in future research to explore the implementation barriers and facilitators to the successful implementation and maintenance of PA programmes in education settings.
Strengths and limitations
The strengths of this scoping review are that it (1) is the first examining the effects of PA/exercise across mental health outcomes for non-clinical populations of youth aged 12–25; (2) provides a synthesis of intervention intensity; (3) was conducted in concordance with a framework and reported per PRISMA guidance; and (4) identified the distribution of the evidence base for PA/exercise as a preventative intervention for mental health, highlighting patterns of positive findings and where more research is needed. A number of limitations exist. Only five studies included follow-up assessments39 42 46 50 56 and none assessed whether PA/exercise prevented the onset of future episodes of threshold mental disorder, rendering longer-term preventive effects unknown. As only nine studies included a comparison group that delivered an intervention41 42 45 46 50 52 59 61 75—the remaining included a wait-list or additional PA/exercise group—in the majority of studies it remains unknown if the observed effects are due to PA/exercise or from non-specific time/attention effects. Only 12 studies provided sufficient information to confidently assess intervention intensity, highlighting a need for better specification and clearer reporting of PA/exercise interventions. We described interventions in terms of intensity; however, there may be other potentially important aspects such as duration and adherence. Indeed, previous research has demonstrated that the frequency, intensity, time, type and context of PA are all critical factors in mental health outcomes in young people.76 These authors highlight that PA provides an opportunity to increase social interaction, self-efficacy and perceived competence, improvements in body image and self-perceptions, as well as autonomy, factors which are commonly agreed to contribute to mental well-being.77 78 Indeed in the current scoping review we have not explored the impact of these factors. In the current study we have reviewed the impact of PA/exercise in different populations; however, it is also possible that there may be differences between populations, such as that effect may differ between university students and incarcerated young men. This question is beyond the scope of the current study; however, it is an important area of future research in order to better understand for whom certain interventions are more appropriate. We have not undertaken quality appraisal of individual trials, given it is outside the scope of this review. In future studies, it might also be worth searching a wider range of databases than those covered by ‘Evidence Finder’, as well as grey literature using ProQuest dissertations and theses.
Conclusions
This review aimed to determine the breadth and outcomes of intervention studies testing the effect of PA/exercise across mental health outcomes in young people who may or may not have been currently experiencing elevated symptoms of mental health disorders. We found evidence that PA/exercise interventions of varying intensities may decrease depression symptoms and some evidence that moderate-to-vigorous-intensity and light-intensity interventions reduce anxiety symptoms.
The mood-enhancing effects of light-intensity interventions have not been as widely researched, but the limited available evidence is positive, highlighting the need to explore the effectiveness and maintenance of PA interventions across the intensity spectrum.79 In adults, mental health benefits are associated with lower levels of PA than required for physical health benefits,80–82 and it is possible that this relationship also holds for younger people; however, this would require additional rigorous empirical support.
Investigation of the effects of PA/exercise interventions using robust designs is a research priority. Significant effects of PA/exercise interventions on additional mental health outcomes were identified in this review; however, few studies were available and findings were inconsistent, indicating that research regarding the impact of PA/exercise interventions on mental health outcomes, other than depression, is lacking.
This review found preliminary evidence for the beneficial effects of PA/exercise interventions as a mental health promotion and early intervention strategy among young people, and future research is required to confirm or refute these findings and fill identified gaps in knowledge. We recommend that future studies include follow-up assessments and appropriate control groups not engaging in PA/exercise. Studies should specify the details of the PA/exercise interventions supported with quantifiable measures, to facilitate replicability and translation into practice. Findings from this review will be valuable for the design of future PA/exercise intervention studies attempting to prevent or intervene early with mental health problems commonly emerging in adolescence and early adulthood.
References
Footnotes
Contributors MP, AP, MC conducted the literature search. MP designed the figures and tables. All authors contributed to study design. MP, AP, APB, NS, RP, TC contributed to data collection. MP, AP, APB, NS, RP, TC contributed to data analysis and data interpretation. All authors contributed to writing and reviewing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.