Article Text

Abstract
Introduction Proteinuria increases at altitude and with exercise, potentially as a result of hypoxia. Using urinary alpha-1 acid glycoprotein (α1-AGP) levels as a sensitive marker of proteinuria, we examined the impact of relative hypoxia due to high altitude and blood pressure-lowering medication on post-exercise proteinuria.
Methods Twenty individuals were pair-matched for sex, age and ACE genotype. They completed maximal exercise tests once at sea level and twice at altitude (5035 m). Losartan (100 mg/day; angiotensin-receptor blocker) and placebo were randomly assigned within each pair 21 days before ascent. The first altitude exercise test was completed within 24–48 hours of arrival (each pair within ~1 hour). Acetazolamide (125 mg two times per day) was administrated immediately after this test for 48 hours until the second altitude exercise test.
Results With placebo, post-exercise α1-AGP levels were similar at sea level and altitude. Odds ratio (OR) for increased resting α1-AGP at altitude versus sea level was greater without losartan (2.16 times greater). At altitude, OR for reduced post-exercise α1-AGP (58% lower) was higher with losartan than placebo (2.25 times greater, p=0.059) despite similar pulse oximetry (SpO2) (p=0.95) between groups. Acetazolamide reduced post-exercise proteinuria by approximately threefold (9.3±9.7 vs 3.6±6.0 μg/min; p=0.025) although changes were not correlated (r=−0.10) with significant improvements in SpO2 (69.1%±4.5% vs 75.8%±3.8%; p=0.001).
Discussion Profound systemic hypoxia imposed by altitude does not result in greater post-exercise proteinuria than sea level. Losartan and acetazolamide may attenuate post-exercise proteinuria, however further research is warranted.
- altitude
- exercise physiology
- kidney
- mountain
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Post-exercise proteinuria is not directly related to systemic hypoxia but it is related to exercise intensity.
Losartan may attenuate post-exercise proteinuria by maintaining the charge-selectivity function in the glomerular filter, although further investigations are warranted.
Future proteinuria research should aim to include urinary alpha-1 acid glycoprotein and it should consider analyses using automated turbidimetric immunoassays.
Introduction
Proteinuria typically results from protein leakage from the capillary lumen through the glomerular filter,1 with some removal in the tubules, as shown by studies inhibiting renal tubular reabsorption with lysine infusions.2 Comparisons between albumin, a selectively reabsorbed,3 66 kDa, negatively charged (pI 4.7) protein that passes through the glomerular membrane via the slit diaphragm pores,4 and alpha-1 acid glycoprotein (α1-AGP),5–7 a smaller (41–43 kDa) and more negatively charged protein (pI 2.7)5 7 indicate that urinary α1-AGP is a more sensitive marker of glomerular leakage than albumin.7–9 Urinary α1-AGP excretion has implicated the glomerular origin of the proteinuria exhibited with both, altitude7 and post-exercise.5 Hypothesised mechanisms for such glomerular leak have included changes in renal blood flow,5 10 increases in peritubular pressure and blood pressure2 (BP), hypoxia11 and acid–base disturbances,2 although the mechanisms remain unclear.12 The contributions of BP and hypoxia, especially to post-exercise proteinuria may be uniquely evaluated with altitude exercise.
At altitude, exercise BP is amplified13 14 and such exaggerations are responsive to antihypertensive therapies such as angiotensin II type 1 (AT1) receptor antagonists or blockers (ARBs).13 15 ARBs reduce BP via several mechanisms, including selectively blocking angiotensin II (A-II) from binding to AT1s within the vasculature,16 promoting vasodilation. Specific to the kidney, ARBs (eg, losartan) ‘block’ vasoconstriction imposed by A-II on afferent arterioles.17 ARBs also limit both, vasopressin secretion and aldosterone production, further adding to its BP lowering effect.16 Considering these factors, it would be reasonable to expect altitude post-exercise proteinuria to be greater than at sea level and that AT1 blockers such as losartan could attenuate the post-exercise response. To evaluate this, we planned to compare post-exercise α1-AGP excretion between (1) sea level and altitude exercise and (2) losartan and placebo groups following exercise at altitude.
Exercise oxygen saturation is also altered at altitude and it is profoundly lower compared with sea level18 but it can be improved by acetazolamide,19 a carbonic anhydrase inhibitor commonly used to prevent altitude illness.20 21 By inhibiting carbonic anhydrase, a catalyst of the reversible CO2 hydration reaction, acetazolamide promotes carbonic acid formation and dissociation of H+ and bicarbonate in the blood21 which limits hypoxia-induced alkalosis and improves oxygen saturation.21 Assuming hypoxia as the main mechanism of post-exercise proteinuria, altitude exercise would be expected to produce larger increases in post-exercise proteinuria compared with sea level. In addition, subsequent improvements in arterial oxygenation would be expected to have the ‘reverse’ effect. To evaluate this, we planned to compare post-exercise α1-AGP between (1) sea level and altitude and (2) placebo and placebo +acetazolamide groups at altitude.
We hypothesised that exercise at altitude would increase post-exercise α1-AGP levels compared with sea level, primarily due to greater systemic hypoxia, and that losartan and acetazolamide would attenuate the observed increases by improving blood and peritubular pressures16 and alleviating renal hypoxia,22 respectively.
As part of an expedition to Quito, Ecuador, we measured post-exercise urinary α1-AGP excretion in 20 pair-matched individuals once at sea level (before placebo or losartan administration) and twice at altitude as outlined in the following sections.
Methods
Design and participants
Twenty participants (14 men, 6 women) free of any pre-existing conditions were included in the study. ACE genotyping (II, ID or DD) was performed to limit potential differences between groups that could be attributed to ACE genotype (eg, response to losartan,23 response to altitude,24 etc.). Participants were pair-matched participants for ACE genotype, age, sex, previous altitude exposure and glomerular filtration rate (GFR, obtained 4 weeks prior to ascent) (figure 1).
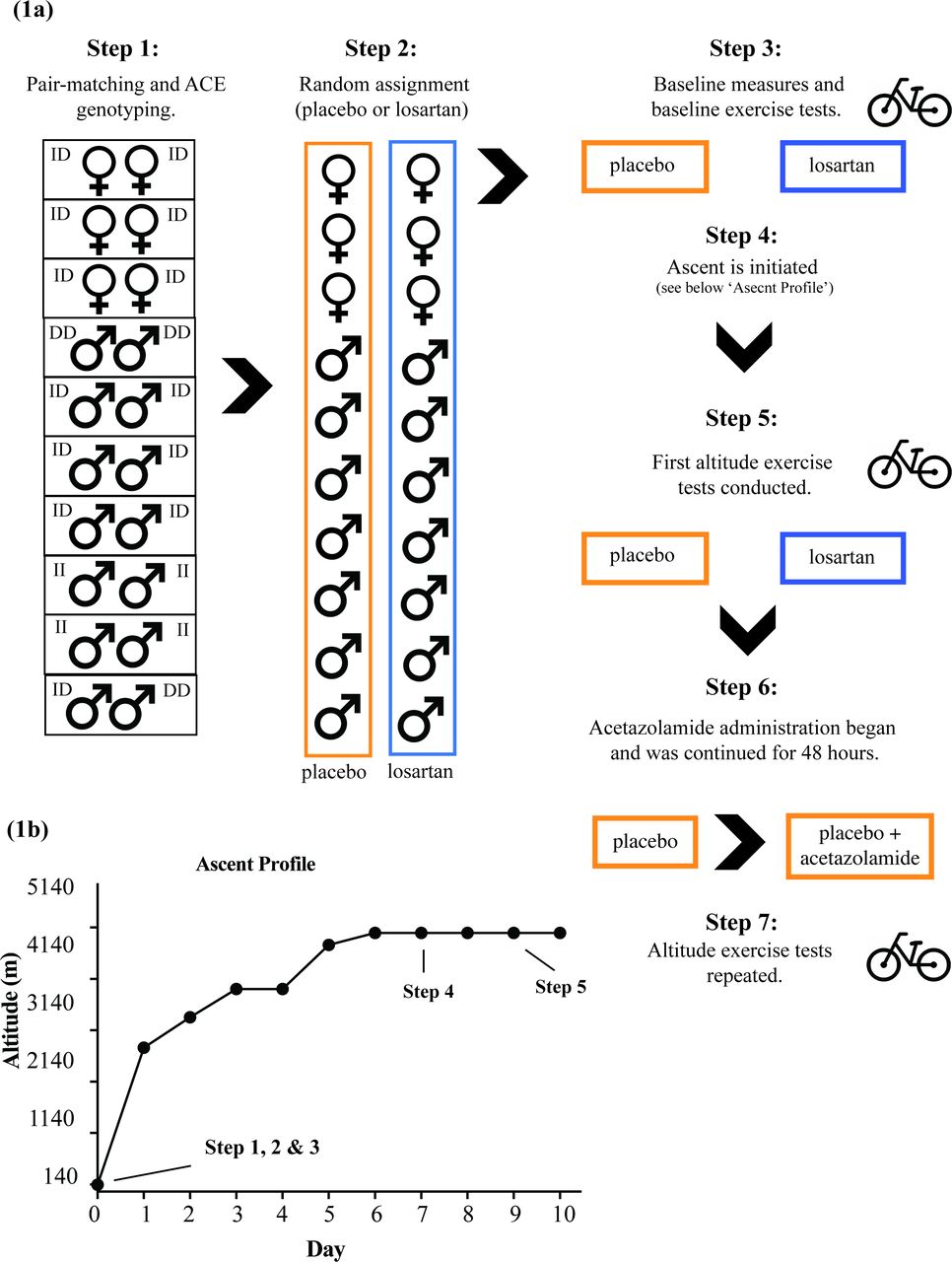
(A) Visual representation of the study design. Step 1: Participants were matched for: ACE genotype (II, ID or DD; see table 3), age, sex previous altitude exposure, and GFR. Step 2: Within each pair, participants were randomly assigned to placebo or losartan groups. Step 3: Baseline characteristics were recorded and baseline exercise tests were conducted (4 weeks before ascent) and were followed by the initiation of losartan administration (21 days before ascent). Step 4: Ascent is initiated with both groups ascending together in accordance with (B). Step 5: The first round of altitude exercise tests were conducted for members of both groups (5035 m). Step 6: Immediately following the first altitude exercise tests, acetazolamide was administered (125 mg orally, two times per day) and continued for 48 hours until next exercise test. Step 7: Repeat altitude exercise tests were conducted for all individuals (only placebo group data reported). (B) Expedition ascent profile. Day 0: Birmingham, UK (130 m), day 1: Quito, Ecuador (2800 m), day 2: Quito, Ecuador (2800 m), day 3: bus to Chunquiragua in Chaupi (3400 m), day 4: bus to Estrella del Chimborazo MARCO cruz (3950 m), day 5: Estrella del Chimborazo MARCO cruz (3950 m) with day hike to 5000 m and back, day 6: bus to Carrel hut (4800 m), days 7–10: Whymper hut (5035 m). GFR, glomerular filtration rate.
Following matching, a double-blind, randomised, placebo-controlled trial design was adopted. Individuals within each pair were randomly assigned to either placebo or losartan group (figure 1). Losartan administration (100 mg/day or placebo) began in the UK 21 days prior to departure for Quito, Ecuador (2850 m). On arrival at Quito, participants ascended over 10 days to the Whymper Hut on the flank of Chimborazo volcano (5035 m, figure 1).
Baseline and daily measures
Baseline measures of height, body mass, GFR and creatinine (μmol/L) were recorded 4 weeks prior to ascent (figure 1A). Estimated GFR (eGFR) was calculated for each individual using the Modification of Diet in Renal Disease study equation25:

During ascent (figure 1B), resting measures of systolic BP (SBP) and diastolic BP (DBP) were collected each morning using a manual sphygmomanometer.
Exercise protocols and measures
Sea-level exercise
Baseline sea-level graded maximal exercise tests were performed 4 weeks prior to ascent on a cycle ergometer (Alticycle) designed for altitude studies26 (figure 1A). Volitional fatigue was used as the primary end point criterion for the test.27 Maximal power output (Wattmax) was measured by the Alticycle and heart rate (HR) recordings were facilitated by telemetry (Polar Electro, UK).
Altitude exercise
The first altitude exercise tests were commenced on arrival to the Whymper Hut for five pairs (day 7) and completed on the following day (day 8) for remaining pairs (figure 1). These initial tests were immediately followed by acetazolamide administration (125 mg orally, two times per day) which occurred 48 hours prior to the second round of altitude exercise tests in all participants. Similar to the first tests, the second round of altitude exercise tests were performed across 2 days (on days 9 and 10, figure 1).
At altitude, pre-exercise measurements of oxygen uptake (VO2), carbon dioxide production (VCO2), ventilation (VE), HR, SBP and DBP were collected. Participants undertook a 5 min self-paced warm-up followed by a modified graded exercise test on the Alticycle which was commenced at 30% of sea-level Wattmax. Intensity was increased every 3 min by 10% until the participant reached 80% of sea-level Wattmax. From this point, intensity was increased by 10% each minute until volitional fatigue. Expired respiratory gases were analysed breath-by-breath using a Cosmed K4b2 (Metabolic Company, Rome, Italy) portable metabolic system alongside continuous measurements of HR (via three-lead ECG), pulse oximetry (SpO2, Datex Ohmeda 3900, GE Healthcare, USA) and beat-to-beat measurements of SBP and DBP by photoplethysmography (Portapres, Finapres Medical Systems BV, The Netherlands). Change in SBP and DBP was calculated as the difference between pre-exercise and the value obtained at Wattmax. Urine specimens were collected surrounding exercise as outlined in the following section.
Urine collection and storage
Twenty-four-hour urine samples were collected over 1 day at sea level and on each day of the expedition (10 days) with four aliquots (2 mL each) taken from each daily collection and frozen on dry ice.
For pre-exercise collections, participants were instructed to drink 500 mL of water between 90 and 30 min pre-exercise and to provide a timed (60 min) urine specimen immediately prior to exercise. Post-exercise urine specimens were collected at 60, 120 and 180 min. Four aliquots (2 mL each) were taken from exercise specimens and frozen on dry ice, with the residual volumes returned to each individual’s 24 hours collection bottle. Urine samples were transported back to Birmingham, UK and stored at (–80°C) until analysis.
Urine analysis
All samples were thawed at room temperature for 1 hour before analysis. The 24-hour urine samples were first analysed for α1-AGP using radial immunodiffusion (RID; Talks et al., 2018)7 and the results were converted to excretion rates (mg/24 hours or μg/min). A subset of samples (119 out of 201) were then analysed using a latex-enhanced immunoassay on the Optilite turbidimetric analyser (The Binding Site, Birmingham, UK; online supplementary appendix 1). This automated method was used for all exercise samples, with the analysed concentrations (mg/L) converted to excretion rates (μg/min) based on sample volumes and collection durations.
Supplemental material
Data analysis
Statistical analyses were performed using SPSS (IBM SPSS Statistics, V.25). Normality of distribution was determined by the Shapiro–Wilk test, with data (24-hour urinary α1-AGP excretion) log-transformed where possible. Continuous variables are presented as mean±SD or median ±IQR where appropriate. All tests for significance were two-tailed with statistical significance set at p≤0.05 unless otherwise indicated.
We used independent t-tests to compare group means (placebo vs losartan) where data were normally distributed and when measures were not repeated (eg, age and baseline HR). We used repeated-measures ANOVA with pairwise comparisons (Bonferroni corrected) to determine group (placebo vs losartan) and interaction effects (where appropriate) across days for normally distributed data (eg, transformed 24-hour α1-AGP, DBP and SBP). We used Friedman tests to determine the main effect of time on α1-AGP excretion surrounding exercise (ie, pre-60, post-60, post-120 and post-180 min) where data were not normally distributed. These results are presented as ‘χ2(df), p value’. When appropriate, the post-hoc Wilcoxon signed rank test with Bonferroni correction for repeated measures was used to distinguish significance between time points (significance set at p≤0.0125; ie, corrected for three comparisons). We then used Mann–Whitney U tests to compare significant time points between groups (ie, placebo vs losartan at post-60 min).
To avoid any superimposed effects of the two drugs on results, we limited comparisons between the two altitude tests (before and after acetazolamide administration, placebo vs placebo +acetazolamide) to individuals from the placebo group completing both tests (n=9, tables 1 and 2). For these comparisons, we applied the Friedman test and Wilcoxon signed rank test as previously described with additional use of the Wilcoxon signed rank test to compare α1-AGP excretion rates (within-individuals) between placebo and placebo +acetazolamide at post-60 min. We used Spearman’s correlation to evaluate relationships between daily measures (eg, DBP and 24 hours α1-AGP excretion) and exercise measures (eg, SpO2 and post-exercise α1-AGP excretion).
Maximal exercise test results compared between groups at baseline and twice at altitude
Comparisons of pre-exercise and post-exercise α1-AGP excretion between groups at sea level and twice at altitude
We calculated ORs for urinary α1-AGP excretion in placebo and losartan groups at rest (pre-exercise and post-exercise at 120 and 180 min) and with exercise (at post-60 min) based on the relative changes (relative increase (+) or decrease (−)) from baseline sea-level measures within each individual.
Patient and public involvement
This study was supported by the Birmingham Medical Research Expeditionary Society which provided input for the conduct of the research. Patients were not included. Public involvement was limited to recruitment. Notification was given to participants at the time of consent that acquisition of personal data was permitted on request. Permission was also obtained at this time for the dissemination of de-identified data within the research team and only externally when a reasonable request was submitted directly to the corresponding author(s) of the present study within 6 months of its publication. A portion of the cohort was invited to review the research methods for accuracy and readability.
Ethics approval
This study did not aim to investigate any safeties or efficacies of the already Food and Drug Administration (FDA)-approved drugs included, thus no clinical trial approval was obtained. There were no active FDA recalls for either drug for the duration of the study.
Results
Baseline measures
Baseline data are presented in table 3. Placebo and losartan groups were not significantly different at baseline for measures of age, body mass, height, GFR, eGFR or creatinine. ACE genotype was exactly matched in 9 out of 10 pairs, with all allelic variations represented (ID, n=13; II, n=4 and DD, n=3; table 3).
Baseline sea-level characteristics
Daily measures
Results for daily measures are presented in figure 2. Collectively with ascent, daily DBPs increased significantly (p=0.04) while SBP increased, although not significantly (p=0.17). Daily SBPs and DBPs remained similar between groups with ascent (SBP, p=0.71; DBP, p=0.72; figure 2A,B).
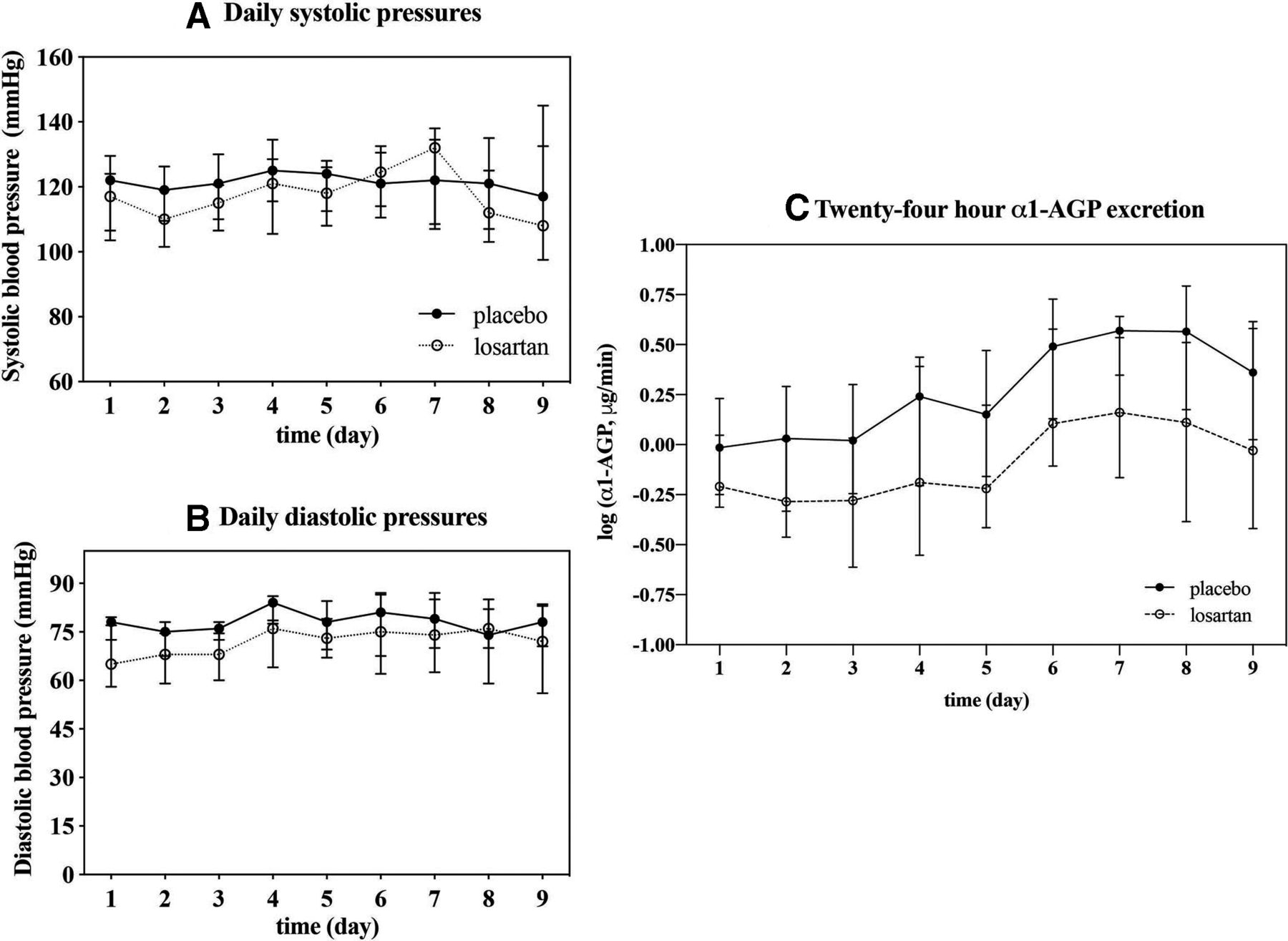
Daily measures of blood pressure and 24-hour urinary α1-AGP excretion rates with ascent. (A) Daily SBPs (mm Hg). (B) Daily DBPs (mm Hg). Data are plotted as daily medians with error bars representing the respective IQRs. (C) Log-transformed 24-hour urinary α1-AGP excretion rates (μg/min) by days with ascent. Data are plotted as the mean log of 24 hours α1-AGP with error bars representing SD of the respective group mean on each day. Twenty-four-hour urinary α1-AGP excretion collectively increased with ascent (p<0.01) with no difference between groups (p=0.97). α1-AGP, alpha-1 acid glycoprotein; DBPs, diastolic blood pressures; SBPs, systolic blood pressures.
Exercise studies
Baseline sea-level exercise
Baseline exercise data are presented in table 1. All 20 participants achieved exhaustion during baseline sea-level exercise tests. Baseline measures of HRmax, absolute Wattmax and relative Wattmax were not different between groups (table 1).
Altitude exercise (losartan vs placebo)
Altitude exercise data are presented in table 1. Pre-exercise measures of SpO2, HR, SBP and DBP were not different between groups. All participants achieved exhaustion during the first altitude exercise tests. At altitude, both absolute Wattmax and relative Wattmax were reduced by ~40% compared with sea level but remained similar between groups. HRmax, SpO2 at Wattmax, SBP at Wattmax and DBP at Wattmax were also similar between groups. Changes in SBP and changes in DBP did not differ between groups.
Altitude exercise (placebo vs placebo +acetazolamide)
Nine individuals from the placebo group went on to complete the second altitude exercise test following acetazolamide administration. These data are presented in table 1. Pre-exercise HR, SBP and DBP were no different between placebo and placebo + acetazolamide, although pre-exercise SpO2 was significantly improved with acetazolamide (p<0.01).
Altitude exercise measures of absolute Wattmax, relative Wattmax, SBP at Wattmax, DBP at Wattmax and HRmax were similar before and after acetazolamide, as were the changes in SBP. In contrast, changes in DBP were significantly greater with acetazolamide (p=0.04). SpO2 at Wattmax was significantly increased with acetazolamide (p<0.01).
Urine studies
Twenty-four-hour excretion
Twenty-four-hour urinary α1-AGP excretion (μg/min) significantly increased with ascent (p<0.01) although no differences were observed between groups for log-transformed excretion rates (p=0.97, figure 2). Twenty-four-hour urinary α1-AGP excretion correlated with DBP but not with SBP on days 1 (r=0.63, p=0.05), 6 (r=0.75, p=0.01) and 9 (r=0.90, p=0.04) of the expedition in the losartan group only.
Baseline sea level
Baseline urine results are presented in table 2 and figure 3A. Urinary α1-AGP excretion rates were no different between groups before exercise. Exercise increased urinary α1-AGP excretion in both placebo groups with excretion rates peaking at post-60 min (figure 3A). Urinary α1-AGP excretion at post-60 min was similar between groups (p=0.63) and resolved after 120 min in both groups (figure 3A).

{kind=link}
{kind=link}
{kind=link}
Pre-exercise and post-exercise urinary α1-AGP excretion (μg/min) rates. (A) Comparisons between placebo versus losartan groups at baseline sea level; (B) comparisons between placebo versus losartan groups at altitude (first altitude exercise); (C) comparisons between placebo versus placebo +acetazolamide at altitude (second altitude exercise); (D) comparisons between baseline versus altitude in both placebo and losartan groups (change in α1-AGP from pre-60 min to post-60 min, Δα1-AGP) and (E) comparisons between placebo versus placebo +acetazolamide. Results are plotted as the group median (or individual values, D) with error bars representing the relative IQRs of the group. Significance was set to p value ≤0.05 unless otherwise indicated. Representing significance: * for the significant effect of exercise on urinary α1-AGP excretion; ** for the significant difference between groups at post-60 min and *** for the significant difference between placebo and placebo +acetazolamide for Δα1-AGP (D) or for the trend (p=0.059) of difference between baseline and the first altitude for Δα1-AGP (E). α1-AGP, alpha-1 acid glycoprotein.
Altitude (placebo vs losartan)
Altitude exercise results are presented in table 2 and figure 3B. Collectively, pre-exercise α1-AGP excretion was elevated at altitude compared with sea level, although excretion rates were similar between groups (p=0.62). The odds ratio (OR) for a relative increase in α1-AGP excretion at rest (pre-120, post-120, post-180 min) was 2.16 times greater without losartan at altitude.
Altitude exercise significantly increased urinary α1-AGP excretion in both placebo (χ2(3)=10.73, p=0.013) and losartan (χ2(3)=15.86, p<0.01) groups (figure 3B). Post-60 min α1-AGP excretion was lower with losartan compared with placebo, although the difference was not statistically significant (p=0.28, figure 3B and table 2).
In the losartan group only, the change in α1-AGP excretion from pre-60 min to post-60 min was lower compared with those changes observed at baseline, although this difference was not significant (p=0.059, figure 3D). The OR for reduced urinary α1-AGP excretion at post-60 min (sea level vs first altitude test) was 2.25 times greater with losartan.
Altitude (placebo vs placebo +acetazolamide)
Results for comparisons of post-exercise α1-AGP between placebo and placebo +acetazolamide are presented in tables 1 and 2 and figure 3C,E. As with placebo, altitude exercise tests, placebo +acetazolamide exercise resulted in an increase in urinary α1-AGP excretion (χ2(3)=10.73, p=0.01, figure 3C). Despite similar exercise peak power outputs (table 1) between placebo and placebo +acetazolamide tests, post-exercise α1-AGP excretion (at 60 min post-exercise) was significantly lower following placebo +acetazolamide exercise (p=0.025, figure 3C). Exercise-induced increases in α1-AGP excretion (change from pre-exercise to post-60 min) were significantly reduced (p=0.036) with acetazolamide by nearly threefold (figure 3E). These changes were not correlated (r=−0.10, p=0.82) with the significant improvements in pre-exercise SpO2 or SpO2 at Wattmax with acetazolamide administration (table 2). No difference was observed between losartan and losartan +acetazolamide tests (data not shown).
Discussion
Compared with sea level and despite substantial systemic hypoxia at Wattmax, post-exercise α1-AGP excretion was not greater at altitude suggesting that hypoxia is not the primary mechanism. Altitude-related reductions in exercise intensity could, in part, explain this result,30 but they would fail to explain the increased likelihood for post-exercise α1-AGP to be lower with losartan compared with placebo when exercise intensities were similar. We had expected that losartan would mitigate BP amplifications and thus lower post-exercise α1-AGP, however we observed no difference in the BP response to exercise between groups. Therefore, we have no evidence to attribute post-exercise α1-AGP responses to alterations in 31BP or peritubular pressures.32
The direct action of ARBs within the glomerular filtration barrier on ATIs of podocytes16 could provide an alternative explanation. Activation of AT1s on podocytes induces heparanase expression, which promotes the cleavage of heparan sulfate and inhibits the production and secretion of heparan sulfate proteoglycans (HSPGs).33 The net result is neutralisation of the negatively charged HSPGs which limits the charge-selective function of the glomerular basement membrane (GBM).34 Blocking AT1s with losartan thus promotes the localised retention of negatively charged proteins at the GBM35 and limits the charge-selectivity impairment36 which, in the present study, manifests as a reduction in the extent of post-exercise α1-AGP. This hypothesis is consistent with findings related to the intensity-dependent increases in angiotensin-II37 and exercise-related increases in α1-AGP,38 although further investigations are required.
Reductions in post-exercise α1-AGP by acetazolamide were unrelated to the significant improvements in exercise SpO2 at similar intensity (these effects of acetazolamide on exercise performance were previously published and support previous findings).26 39 On its own, this would provide further support indicating that hypoxia is not the primary mechanism of post-exercise proteinuria. Unfortunately, the post-exercise effects of acetazolamide cannot be separated from the acclimatisation effect. Thus, no definitive conclusion regarding acetazolamide’s effects on post-exercise proteinuria can be provided. Future research is required to evaluate acetazolamide-related changes in post-exercise proteinuria. Nonetheless, acetazolamide results support recent evidence demonstrating performance limiting effects of acetazolamide despite of its ability to elicit improvements in oxygen saturation.40
Limitations and future directions
The inability to control for extraneous variables (eg, activity, sleep, environmental conditions) as well as low subject numbers were weaknesses of the present study but they are common limitations for such field-based research. Not controlled for were the inter-individual variability7 and between-day variations in α1-AGP excretion which could have impacted results. Future research could be strengthened by incorporating a sea-level control arm that compared post-exercise proteinuria between exercise tests executed 48 hours apart. Benefit could also be gained by using a less complex design and avoiding overlapping factors (eg, acclimatisation status and time course of exercise tests in this case). Lastly, further research is needed in order to confirm the relationship between DBP and 24 hours α1-AGP excretion.
Conclusion
Our findings suggest that post-exercise α1-AGP is (1) more related to exercise intensity than degree of hypoxia or BP and (2) possibly influenced by activation or inhibition of AT1 receptors. Losartan may limit post-exercise proteinuria by helping to maintain the charge-selectivity function in the glomerular filter, although further investigations are required for evaluation.
Acknowledgments
The authors would like to thank Gregg Wallace and the Research and Development Team at The Binding Site for their kind assistance during the development of the immunoassay and subsequent urinalysis. The authors would also like to thank the Birmingham Medical Research Expeditionary Society.
References
Footnotes
Contributors All authors listed contributed substantially to the work and by ICMJE 2018 standards meet at minimum satisfy criterion No. 1, No. 3 and No. 4 with additional support for No. 2 provided by KEJ, SJEL, AF, AW, JD and AB.
Funding The research was partially funded by JABBS Foundation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval This observational study was approved by the Chichester University Research Ethics Committee (protocol number: 1314 42) and was performed according to the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data are owned by the University of Birmingham and can be obtained upon reasonable request from either the corresponding author or the Sport, Exercise, and Rehabilitation Sciences department +44 (0)121 414 9286. Reuse is not permitted unless otherwise indicated at the time of reasonable request. There is no additional relevant information.