Article Text

Abstract
Objectives The purpose of this review was to synthesise both injury prevention and performance tackle-related research to provide rugby stakeholders with information on tackle injury epidemiology, including tackle injury risk factors and performance determinants, and to discuss potential preventative measures.
Design Systematic review and narrative synthesis.
Data sources PubMed, Scopus and Web of Science.
Eligibility criteria Limited to peer-reviewed English-only publications between January 1995 and October 2018.
Results A total of 317 studies were identified, with 177 in rugby union and 13 were in rugby sevens. The tackle accounted for more than 50% of all injuries in rugby union and rugby sevens, both at the professional level and at the lower levels, with the rate of tackle injuries higher at the professional level (mean 32/1000 player-hours) compared with the lower levels (mean 17/1000 player-hours). A player’s tackle actions and technical ability were identified as major risk factors for injury and a key determinant of performance.
Summary/conclusion Evidence-based education, progressive tackle technique training with a high potential to transfer and law changes have been proposed as key modifiers of player tackle actions and technical ability. Conceivably, all three modifiers working in unison (as opposed to separately) will have a higher potential at reducing tackle injury risk while enhancing performance. With the guidance of tackle injury and performance studies, as well as stakeholder engagement, experiential and explorative tackle research has the potential to inspire innovative injury prevention and performance strategies.
- rugby
- contact sports
- injuries
- performance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known
The physical and dynamic nature of rugby union and rugby sevens exposes players to high risk of injury.
The tackle is the contact event that has the highest injury incidence.
To effectively reduce the risk of injury and optimise performance, it is recommended a sport injury prevention or sport performance process model be followed.
What this study adds
Tackle injury rates are higher at the professional level compared with the lower levels.
Tackle injury frequencies are similar between the ball carrier and tackler.
A major risk factor for tackle injury and a key determinant of tackle performance is the player’s technical ability.
A player’s technical ability can be improved through boosting coaching competencies. An example of such a coaching competency is how to monitor and progress tackle training to ensure optimum transfer to matches.
Introduction
The physical and dynamic nature of rugby union and rugby sevens expose players to high risk of injury. The majority of injuries in these rugby codes, at all levels, occur during the contact events: the tackle, ruck, maul, line-out and scrums.1–4 The tackle is the contact event that has the highest injury incidence (injuries per 1000 player-hours), while the ruck and scrum have the second and third highest injury incidences, respectively.1–4Also, while the majority of spinal cord injuries occur in the scrum, the tackle has the highest incidence for the most severe injuries.5 During the tackle, both the player in possession of the ball (ball carrier) and the player(s) attempting to contest the ball and territory (tacklers) are at risk of injury,6–9 although the mechanisms of injury may differ.10 11 Although the tackle is a high-injury risk contest, the ability to repeatedly win the contest is also a key performance indicator, with successful teams winning more tackles.12
To effectively reduce the risk of injury and optimise performance, it is recommended a sport injury prevention or sport performance process model such as the Translating Research into Injury Prevention Practice (TRIPP) model13 (involving six stages) or the Applied Research Model for the Sport Sciences14 (involving eight stages) be followed. These models outline a sequence of stages that need to be completed to ensure the uptake and sustainability of an injury prevention or performance initiative in the ‘real world’.13 The first stage proposes establishing the extent of the injury problem through injury surveillance studies. Thereafter, the aim is to understand why and how these injuries occur, that is, identifying injury risk factors (stage 2). Stage 3 seeks to develop potential preventive measures for testing in ideal or controlled conditions (stage 4). Stage 5 aims to understand the implementation context, and the final stage (stage 6) monitors the effectiveness of the preventive measure in the real world.
Owing to the high risk of injury and performance demands, the tackle has been a research focus within rugby compared with other contact events.15 Seemingly, each of these studies have contributed to a stage in the injury prevention or performance process models. However, these studies have not been consolidated to determine the state of tackle-related research at each stage for both injury prevention and performance. For instance, while systematic reviews on injury rates in rugby union and rugby sevens have been published1–4 to address stage 1 of injury prevention models, and despite knowing the high incidence of tackle injury, no review to date has synthesised tackle injury frequencies and rates by playing levels and competition, and by role (ball carrier or tackler). Therefore, using the first three stages of the TRIPP model13 as a guide, the purpose of this review was to consolidate both injury prevention and performance tackle-related research. The intention of this review was to synthesise both injury prevention and performance tackle-related research to provide rugby stakeholders with information on tackle injury epidemiology, including tackle injury risk factors and performance determinants, and to discuss measures that may improve tackle performance and reduce the risk of tackle injuries.
Methods
A narrative synthesis format was chosen to review and synthesise the pool of literature. A narrative synthesis is an ‘approach to the systematic review and synthesis of findings from multiple studies that relies primarily on the use of words and texts to summarise and explain the finding of the synthesis’.16 17 Narrative syntheses can be used to review and assess quantitative and qualitative data and, in contrast to ‘narrative reviews’ and ‘evidence syntheses’, involve a systematic and predefined search strategy with a focus on producing a more textual synthesis versus other types of systematic reviews such as quantitative meta-analyses.
Search strategy
A search was conducted for published studies that reported on tackle-specific factors in rugby union and rugby sevens (rugby league studies were included in the search but removed at the final stage of the selection process). Three electronic databases (PubMed, Scopus and Web of Science) were searched using the keyword combinations ‘rugby’ AND ‘contact’, ‘rugby’ AND ‘tackle’, and ‘rugby’ AND ‘union’ OR ‘league’ OR ‘sevens’ AND ‘injur*’.
Eligibility criteria
The search was limited to peer-reviewed English-only publications between January 1995 (the advent of professionalism in rugby union) and October 2018. Articles that involved quantitative data on rugby union or rugby sevens (including all ages and levels of play, and male and female players) were included. Only studies that included tackle-related testing protocols and match or training data (pertaining to tacklers and/or ball carriers) were included. The studies had to clearly define the tackle or ball carry as part of their analysis and not group the tackle into general contact/collision data.
Overall and/or time-loss tackle injury rates (only studies reporting number of injuries per 1000 exposure) and frequencies (percentages) were tabulated according to rugby code and level of play (tables 1–3). A time-loss injury was defined as an injury that resulted in a player being absent from normal match/training/recreational activities for more than 24 hours or 7 days (depending on the specific study’s definition) after the incident. Medical attention injuries were injuries that required treatment from a doctor/healthcare professional but resulted in no time away from normal match/training/recreational activities. Overall injuries included both medical attention and time-loss injury events. Injury case studies specific to tackle events were also reviewed (see online supplementary appendix 1). Overall tackle numbers and rates (only studies reporting total number of tackles per match, and/or number of tackles per game or per minute) were tabulated in tables 4 and 5. Narrative literature reviews, systematic reviews, meta-analyses, editorials, journal letters, book chapters, conference proceedings, discussions and qualitative research studies were excluded from the analysis. All other quantitative study types and case studies were accepted for review.
Supplemental material
Tackle-related injury frequencies and rates in professional rugby union
Tackle-related injury frequencies and rates in semiprofessional, amateur and youth rugby union
Tackle-related injury frequencies and rates in rugby sevens (all levels of play)
Tackle numbers and rates in rugby union (all levels of play)
Tackle numbers and rates in rugby sevens (all levels of play).
Screening process
A five-step approach was followed to identify the final group of articles that would eventually be included in the final review (figure 1). Two authors (NB and SH) independently screened the titles using the eligibility criteria. The reliability of the authors was assessed by comparing the results of the title-screening process. Disparities in the results were discussed and resolved by the authors. NB continued the screening process of the abstracts and full-text articles. The articles were excluded at each step if they met the exclusion criteria or did not meet the inclusion criteria.
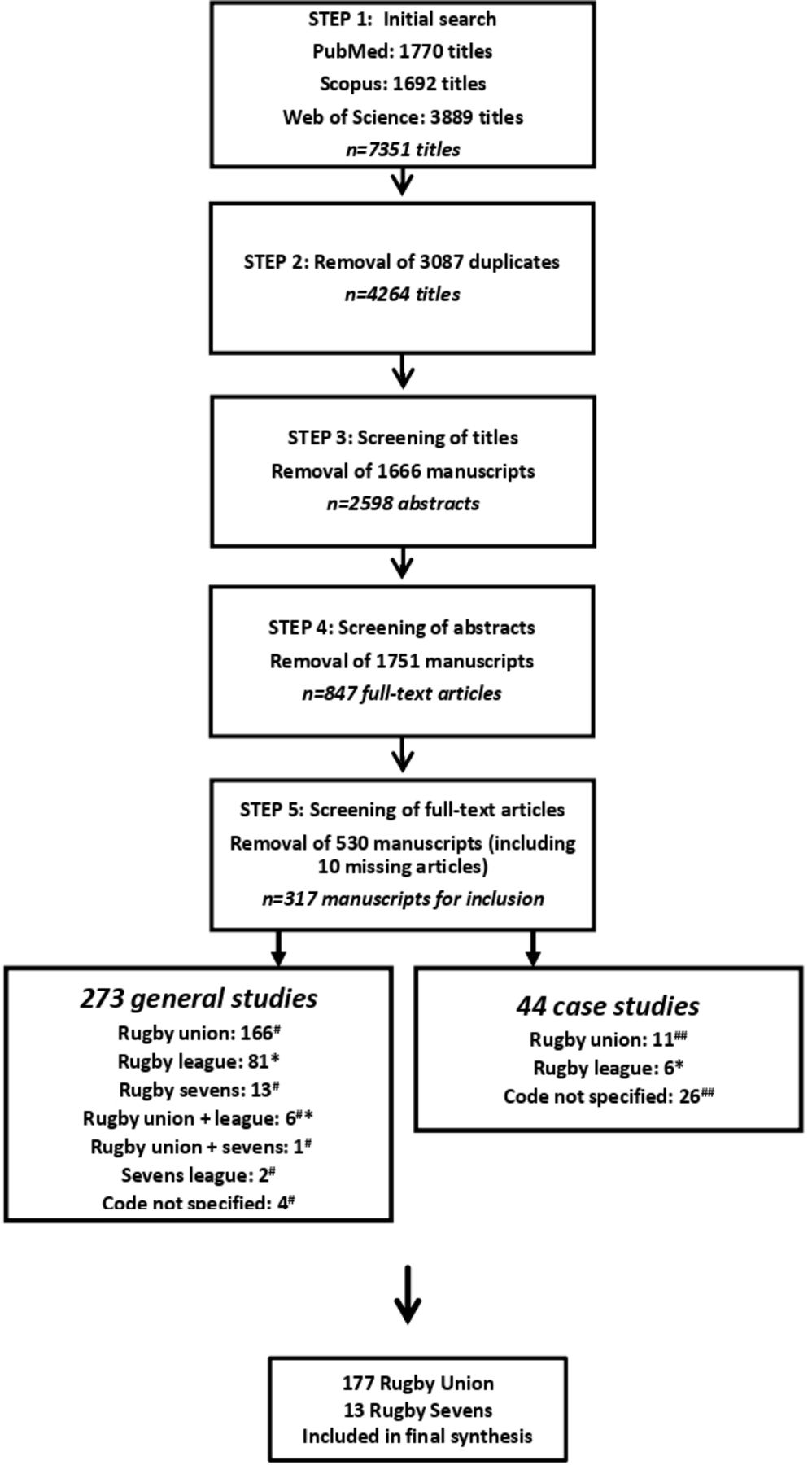
{kind=link}
Summary of the literature screening process. #, manuscripts included in rugby union/sevens analysis; ##, manuscripts included in rugby union/sevens appendix; *, manuscripts included in separate rugby league analysis/appendix.
Data interpretation
Only the main findings (relating to tackle events) from each study were presented in this review. Confidence intervals (90% or 95% CIs) and standard deviations (±SDs) were provided in the tables, depending on their availability. All values and percentages were rounded off to a maximum of two decimal places where necessary. Results are organised according to the first three stages of the TRIPP model.
Results
Injury epidemiology and tackle frequencies
General rugby union and sevens injury studies provided details pertaining to one or more tackle-related factors, including but not limited to injury rates, player injured (ie, ball carrier or tackler), player position (eg, forward or back), injury location (eg, head/neck, lower-limb or upper-limb), injury type/diagnosis (eg, concussion, fracture or bruise/contusion), tackle direction (eg, front-on or from behind) and player running speed prior to injury.6–11 18–52 The tackle consistently accounted for more than 50% of all injuries in rugby union and rugby sevens, both at the professional level and at the lower levels. The rate of tackle injuries are higher at the professional level (mean 32/1000 player-hours) compared with the lower levels (mean 17/1000 player-hours). At all levels, the frequency of injury between the ball carrier and tackler were not largely dissimilar.
Certain studies also focused on niche areas including head injuries and concussions,31 40 53–70 spinal and neck injuries,71–79 shoulder injuries,34 80–88 knee and ankle injuries,89–93 and the influence of tackle technique on injuries.61 64 65 69 94–96 Overall and time-loss injury frequencies and rates for rugby union (tables 1 and 2) and sevens (table 3) were tabulated (all injury types included). Tackle-related injury case studies were also summarised for all levels of rugby union and sevens from 1995 to 2018 (see online supplementary appendix 1).
The total number of tackles per match and tackle rates (tackles per game or per minute) for all levels of play for rugby union and sevens are summarised in tables 4 and 5, respectively. Successful and unsuccessful tackles were also included.
Injury risk factors and performance determinants
In matches, proper contact technique during the tackle, for both the ball carrier and tackler, has been identified as a key injury risk factor and performance determinant.61 64 65 69 94–96 For example, ball carrier and tacklers that fail to ‘leg drive’ after contact have a higher risk of injury and a reduced chance of winning the tackle.56 94 95 97 In another example, ball carriers fending the tackler on contact have a reduced risk of injury and are more likely to offload or break the tackle.48 98 Not surprisingly, high, dangerous and illegal tackles are also a major risk factor for tackle injuries. A match contextual factor that has also been identified as a risk factor for injury is match quarter. Tackle injuries are reported to occur more frequently during the latter stages of matches,15 16 which are attributed to a decrease in tackle technique. The physical and physiological demands of the tackle during matches, such as tackle velocity and muscle damage, have also been reported.99–123
Players’ and coaches’ knowledge, attitudes and behaviours pertaining to the tackle have been studied, including risk factors for injury and determinants of performance, both in training and matches.68 124–130 For instance, players who rated tackle training to prevent injuries important (player attitude) and who spent more time on technique training to prevent injuries (player behaviour) reported safer behaviours for the tackle during matches. Also, coaches seem to be aware of the risk of injury in the tackle and the importance of coaching of proper technique.131 However, this positive knowledge and attitudes from the coaches did not transfer into tackle training (coach behaviour).
Studying the tackle in controlled settings
Within lab settings, the physiological and biomechanical loads of the tackle have been studied.99 101–113 These studies suggest that the movement patterns and the production of force are weaker on the non-dominant shoulder.103 117 For example, Seminati et al reported a 13% higher impact force from the dominant shoulder.132 Players seem to have poorer shoulder positional sense of their non-dominant shoulder while tackling133 and adopt a more passive biomechanical strategy to generate the drive needed to stop a ball carrier.132 As such, tackles on the dominant shoulder produce higher impact forces on contact, whereas the non-dominant shoulder produces force over longer durations.132 In addition, tackles on the non-dominant shoulder were characterised by less control of head movement, which had a more flexed and laterally bent position compared with tackles on the dominant shoulder.132
Discussion
It is well established that a player’s tackle actions and technical ability are major risk factors for injury and key determinants of performance.61 64 65 69 94–96 The question is how can we modify player action and improve tackle technique? One answer to this question is player, coach and referee education. Using evidence from tackle injury mechanism and performance determinant studies, national injury prevention programmes such as New Zealand’s Rugby Smart and South Africa’s BokSmart programmes aim to educate rugby stakeholders on safe and effective tackle techniques.124 134 These educational tools are intended to modify player, coach and referee attitudes and behaviours, both in training and during matches. While these national injury prevention programmes have shown positive changes in player, coach and referee knowledge,124 125 this may not be enough to drive positive behaviour change. Indeed, Hendricks et al showed that even though a sample of youth coaches were aware of the high risk of injury during the tackle and the importance of proper tackle technique, this knowledge did not transfer into their actual tackle training sessions.131 Therefore, the next logical step is to apply the knowledge gained from tackle injury mechanism and performance determinant studies to improve tackle training.
The tackle is a highly technical and physical skill and, like any skill, should be developed though training.15 135 Despite this, research comparing training and matches suggests that tackle contact preparation during training is not adequate to meet the demands of tackle contact during matches.131 136 137 Implementation research in sport argues that the ability to coach technique depends on how competent the coaches believe they are to do so138; this is also true for coaching tackle technique.131 136 From a behaviour change perspective, to increase the likelihood of a desired behaviour requires a specific action plan139 140 and the fostering of competencies, a concept known as ‘boosting’.141 In line with these arguments, a group of rugby researchers and practitioners designed a tackle contact skill framework and training plan based on skill acquisition and skill development literature.142 The framework describes measurements that can be used to monitor and progress tackle training to ensure optimum transfer to matches.142 Although the efficacy and effectiveness of such a tackle training programme has yet to be studied, the framework and training plan serves as a starting point to design tackle training programmes and further develop tackle training concepts such as contact readiness (when introducing players to rugby), contact readiness as part of match warm-up, return to contact (for players returning from injury), contact capacity (maintaining proper technique while fatigued) and contact efficiency (highly proficient contact technique with minimal physical effort). Also, how other forms of physical preparation, for example, resistance training, influences tackle ability is yet to be investigated. Finally, most of what we know about tackle training is based on questionnaire studies; therefore, to better understand the implementation context, as well as barrier and facilitators to implementing a tackle training programme, coach engagement and systematic observations of tackle training sessions are required.
Another strategy to modify player tackle action during matches is through changing the laws of the game. To specifically reduce head injuries during the tackle, the sport’s governing body, World Rugby, have recently recommended stronger sanctioning of reckless and high tackles and proposed a reduction in tackle height of a legal tackle,61 from above the line of the shoulders to above the line of the armpit. These law changes are seemingly based on the behavioural principle known as ‘nudging’, that is, changing the external environment to achieve a predicable outcome.141 Changing tackle laws also has a more immediate effect compared with education and training programmes. With that said, the actual effect of these law changes on tackle injury risk and player tackle actions is yet to be published.
Although results from lab-based studies may have limited applicability to match situations due to its controlled nature, studying the tackle in the lab allows for experiential and explorative study designs. Experiential and explorative study designs may offer deeper insights into the demands and movement patterns of the tackle (eg, tackle biomechanics),103 as well as test the effects of different conditions (eg, physical fatigue) and interventions (video feedback)143 on tackle technique. Not all research on the tackle needs to have a direct application, and experiential and explorative work is important to inspire innovative tackle injury prevention and performance strategies.144 Having said that, findings from tackle injury and performance studies in matches, as well stakeholder engagement, should guide the questions and design of lab-based studies.
Conclusion
The purpose of this review was to synthesise both injury prevention and performance tackle-related research to offer rugby stakeholders (researchers, practitioners, policymakers and coaches) with tackle-specific injury epidemiology and frequencies, an overview of tackle injury risk factors and performance determinants, discuss measures to improve tackle performance and reduce the risk of tackle injuries. The tackle consistently accounted for more than 50% of all injuries in rugby union and rugby sevens, both at the professional level and at the lower levels, with the rate of tackle injuries higher at the professional level (mean 32/1000 player-hours) compared with the lower levels (mean 17/1000 player-hours). Also, the frequencies of injury between the ball carrier and tackler were not largely dissimilar. A player’s tackle actions and technical ability has been identified as a major risk factor for injury and a key determinant of performance. Evidence-based education has been used, and progressive tackle technique training with a high potential to transfer and law changes have been proposed, as key modifiers of player tackle actions and technical ability. Conceivably, all three modifiers working in unison (as oppose to separately) will have a higher potential at reducing tackle injury risk while enhancing performance. With the guidance of tackle injury and performance studies, as well as stakeholder engagement, experiential and explorative tackle research also has potential to inspire innovative tackle injury prevention and performance strategies.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.
- 146.
- 147.
- 148.
- 149.
- 150.
- 151.
- 152.
- 153.
- 154.
- 155.
- 156.
- 157.
- 158.
- 159.
- 160.
- 161.
- 115.
- 163.
- 164.
- 165.
- 166.
- 167.
- 168.
- 169.
- 170.
- 171.
- 172.
- 173.
- 174.
- 175.
- 176.
- 177.
- 178.
- 179.
Footnotes
Twitter @it_is_burger, @MikeLambert 01, @Sharief_H
Contributors NB conducted the search and review, NB and SH cowrote the first draft, and all authors provided input to the final version.
Funding This work was supported by the UCT Faculty of Health Sciences Postgraduate Publication Incentive Award and the National Research Foundation (NRF).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.