Article Text

Abstract
Introduction There is strong evidence that exercise prevents falls in community-dwelling older people. This review summarises trial and participant characteristics, intervention contents and study quality of 108 randomised trials evaluating exercise interventions for falls prevention in community-dwelling older adults.
Methods MEDLINE, EMBASE, CENTRAL and three other databases sourced randomised controlled trials of exercise as a single intervention to prevent falls in community-dwelling adults aged 60+ years to May 2018.
Results 108 trials with 146 intervention arms and 23 407 participants were included. Trials were undertaken in 25 countries, 90% of trials had predominantly female participants and 56% had elevated falls risk as an inclusion criterion. In 72% of trial interventions attendance rates exceeded 50% and/or 75% of participants attended 50% or more sessions. Characteristics of the trials within the three types of intervention programme that reduced falls were: (1) balance and functional training interventions lasting on average 25 weeks (IQR 16–52), 39% group based, 63% individually tailored; (2) Tai Chi interventions lasting on average 20 weeks (IQR 15–43), 71% group based, 7% tailored; (3) programmes with multiple types of exercise lasting on average 26 weeks (IQR 12–52), 54% group based, 75% tailored. Only 35% of trials had low risk of bias for allocation concealment, and 53% for attrition bias.
Conclusions The characteristics of effective exercise interventions can guide clinicians and programme providers in developing optimal interventions based on current best evidence. Future trials should minimise likely sources of bias and comply with reporting guidelines.
- fall
- exercise
- evidence-based
- senior
- review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known
Previous systematic reviews concluded exercise as a single intervention prevents falls in community-dwelling older adults.
Evidence-based practice requires clinicians and service providers to interpret, evaluate, adapt and integrate findings from clinical trials into their practice and policies.
Clinical trials of exercise intervention are heterogeneous in terms of participant characteristics, compliance, intervention content and risk of bias.
What are the new findings
A diversity of effective exercise interventions are available, offering clinicians an opportunity to implement shared decision-making with their patients.
Promotion of long-term exercise is needed.
Existing trials are prone to performance and ascertainment bias, which impedes the implementation of evidence-based medicine.
Further research is needed for interventions targeting males as well as low-income countries.
Introduction
Falls are a significant cause of mortality and can cause serious morbidity such as fracture and head injury in older adults.1 2 Falls substantially reduce the mobility and confidence of older people and impose a significant economic and social burden to society.2 3 Approximately one-third of people aged above 65 years living in the community fall each year4 and the incidence and healthcare cost associated with falls will increase with the ageing population.5 Thus, there is an urgent need for effective falls prevention strategies to be implemented.
Systematic reviews concluded that exercise programmes can reduce the rate of falls and risk of falling in community-dwelling older adults.6–8 In addition, two Cochrane systematic reviews concluded the falls prevention effect of stand-alone exercise interventions is similar to multifaceted interventions.7 9 Translating the research findings from stand-alone exercise intervention trials into clinical practice would therefore be a beneficial and potentially cost-effective public health solution to falls in community-dwelling older adults.10
Our recent Cochrane Review, including 108 trials, co-published in the British Journal of Sports Medicine,11 evaluated the effect of exercise on falls in people aged 60+ living in the community. Exercise interventions that reduced falls involved primarily balance and functional exercise (reduced fall rate by 24%, 95% CI 19% to 35%), Tai Chi (reduced fall rate by 19%, 95% CI 1% to 33%) or multiple exercise components, usually including balance and strength training (reduced fall rate by 34%, 95% CI 12% to 50%).8
Evidence-based practice requires clinicians to interpret, evaluate, adapt and integrate findings from clinical trials into their practice and policies.12 This is challenging with fall prevention trials, due to heterogeneity in participant characteristics and intervention content. Clinicians must consider whether results are generalisable to their patient population, by reviewing the type of exercise, duration, group-based versus individualised delivery and level of supervision provided.13 Considering participant adherence to intervention programmes also facilitates judgement on intervention effectiveness and acceptability.14 Assessment of risk of bias in a trial will also inform its validity.
Describing and understanding the characteristics of the trials included in the Cochrane Review8 evaluating the effectiveness of exercise on falls prevention, especially those studies contributing to effective intervention types, will guide evidence-based practice and future research. This paper aims to describe the following, in randomised controlled trials (RCT) of exercise as a single intervention for falls prevention in community-dwelling adults aged 60 years and older:
Trial and participant characteristics.
Components of exercise programmes that prevent falls (exercise type, duration and hours of intervention, delivery mode, level of supervision, tailored in intensity or type).
Risk of bias.
Methods
Searches
MEDLINE, EMBASE, CINAHL, Cochrane Bone, Joint and Muscle Trauma Group Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL) and the Physiotherapy Evidence Database (PEDro; http://www.pedro.org.au/) were searched from inception to 2 May 2018. The full search strategy is reported in detail in the Cochrane Review protocol15 and the search terms are included in online supplementary material A. The reference lists of previously published systematic reviews were screened and trial authors were contacted to identify additional studies.
Supplemental material
Selection of studies
The detailed methodology for selection of studies was described in the Cochrane Review protocol.15 In brief, RCTs, individual or cluster randomised, evaluating the effect of exercise interventions on falls in older people living in the community were included. Eligible trials had exercise as a single intervention with the mean age minus 1 SD of the participants being greater than 60 years. Eligible trials reported either number or rate of falls. Trials using quasirandomisation were excluded. Studies were excluded if the target population had specified clinical conditions impacting falls, for example, dementia, stroke, Parkinson’s disease, multiple sclerosis, hip fracture and severe visual impairment.
The title, abstract and descriptors of identified studies were screened independently by pairs of review authors (ZAM, AT, NF, CS). From full text, the same two review authors (ZAM, AT, NF, CS) independently assessed each potentially eligible article with disagreements resolved through discussion. If needed, trial authors were contacted for additional information.
Data extraction
A pretested data extraction form based on an earlier Cochrane Review7 was used by pairs of review authors (ZAM, AT, NF, CS, GW, CAN) to independently extract data from all included trials. Disagreements were resolved through discussion. Review authors did not assess their own trials.
The items extracted from the trials included trial and participant characteristics (sample size at randomisation, trial location, age, gender, falls risk at enrolment, inclusion criteria related to falls, compliance) and intervention components (exercise type, duration of intervention, hours of intervention, delivery mode, level of supervision, tailored initially, progressed based on individual assessment, tailored in intensity or type). Falls risk at enrolment was classified as high if the trial’s inclusion criteria were based on specific fall risk factors such as previous falls, poor balance, recent hospitalisation, reduced lower strength, poor mobility, use of mobility aids, frail, prolonged bed rest, recent rehabilitation, functional limitation and all participants greater than age 80. Compliance was classified as good if the attendance rate exceeded 50% and/or 75% or more of the participants attended 50% or more sessions. The intervention type was classified based on taxonomy developed by the Prevention of Falls Network Europe (ProFaNE)16: balance, functional (task) and gait training; strengthening or resistance training; flexibility training; three-dimensional exercise (including Tai Chi and dance); general physical activity; endurance; and other exercises.
The methods for the estimate of the pooled treatment effect of exercise and the application of the Grading of Recommendations Assessment, Development and Evaluation system to establish certainty of evidence are described in detail in the Cochrane Review.8
Risk of bias of studies
Risk of bias was assessed independently by pairs of review authors (ZAM, AT, GW, NF) not blind to the trial authors or sources, using the Cochrane Risk of Bias tool.17 The criteria were: sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective reporting; and ascertainment bias. Disagreements were resolved through discussion. Review authors did not assess their own trials.
Results
The search returned 4006 records, of which 108 trials involving 23 407 participants were eligible for inclusion (figure 1).18 The characteristics of the 108 included trials are summarised in online supplementary material B.10 19–125
Supplemental material
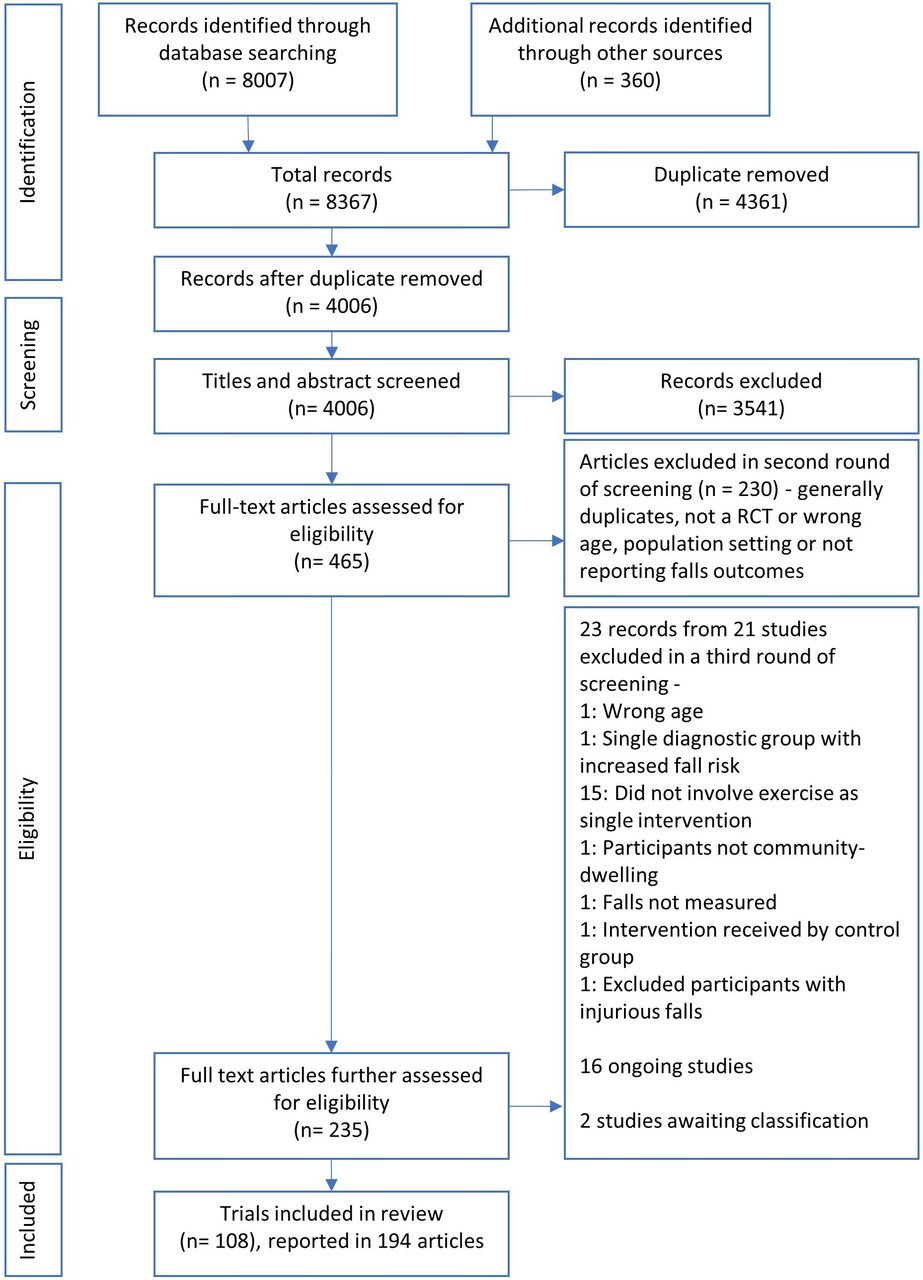
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram18 summarising the study selection process. RCT, randomised controlled trial.
Trial and participant characteristics
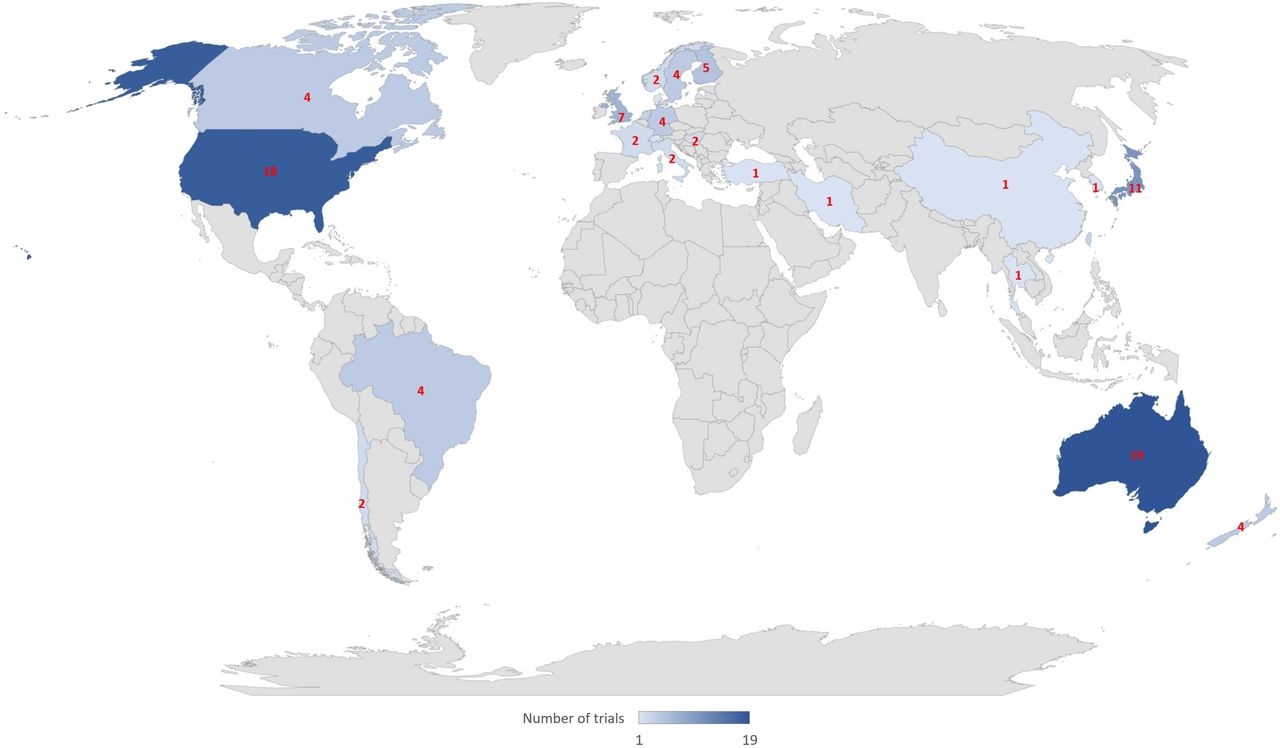
The sample size ranged from 2098 to 1635 participants.47 The included trials were undertaken in 25 countries (figure 2). The highest number of trials took place in Australia (19/108, 18%), followed by the USA (18/108, 17%), Japan (11/108, 10%) and the UK (7/108, 6%). There were three multinational trials.49 72 89 The mean participant age in the reviewed trials ranged from 65 to 88 years old. Ninety-seven (90%) trials had predominantly female participants; 28 (26%) trials were made up of entirely female participants with only one trial100 testing their intervention specifically on the male population. Sixty (56%) trials had elevated fall risk as an inclusion criterion, which was assessed as falls history (33 trials, 31%); poor balance (13 trials, 12%); poor mobility or use of mobility aid (4 trials, 4%); lower limb weakness (3 trials, 3%); functional limitation (3 trials, 3%); age greater than 80 years (3 trials, 3%); recent rehabilitation (2 trials, 2%); and 1 (1%) each for frail and prolonged bed rest, respectively. Fourteen of the trials had multiple inclusion criteria. Seventy-eight (72%) trials satisfied the criteria of good compliance with attendance rate exceeding 50% and/or 75% or more of the participants attending 50% or more sessions.

{kind=link}
{kind=link}
Intervention content and characteristics
There were 146 intervention arms in the 108 included trials. Using the ProFaNE taxonomy the primary intervention component was balance and functional exercise in 79 (54%) intervention arms; three-dimensional exercise (Tai Chi) in 16 (11%) intervention arms; and multiple categories of exercise in 34 (23%) intervention arms (the majority of these (n=19, 51%) included balance and functional exercise in addition to resistance exercise). These primary categories of exercise intervention significantly reduced falls in the Cochrane Review8 and the intervention characteristics are described in online supplementary material C. The remaining types of primary intervention, which did not significantly reduce falls, are described in online supplementary material D: strength or resistance training, 11 (8%) intervention arms; flexibility training, 1 (1%) intervention arm; general physical activity, 5 (3%) intervention arms. No intervention included endurance exercise as the primary component. The duration of the interventions varied from 2 to 130 weeks, with a median of 25 weeks (IQR 12–52) while 75 (51%) interventions lasted less than 24 weeks. The total hours of intervention varied from 6 to 1086 hours, with a median of 44 hours (IQR 24–87). There were 72 (49%) group-based interventions, 15 (10%) supervised individual-based interventions, 29 (20%) intervention arms were unsupervised individual exercise and 30 (21%) interventions were a mixture of group-based and individual exercise. The participant to instructor ratio was not clearly reported in 65 (45%) intervention arms. Of the 82 interventions that reported, 29 were not supervised, 15 had one-on-one intervention and 8 interventions had more than 10 participants per instructor. Eighty-one (55%) intervention arms were tailored to the individual initially and intervention was progressed based on individual assessment in 86 (59%) interventions. Ninety-three (64%) interventions were tailored in intensity or type.
Supplemental material
Supplemental material
Characteristics of studies where the primary exercise components wasere balance, functional and gait training
Compared with control, balance and functional exercises reduced the rate of falls by 24% (rate ratio 0.76, 95% CI 0.70 to 0.81; 7920 participants, 39 studies; high-certainty evidence). The median programme duration was 25 weeks (IQR 16–52). The median total hours of exercise was 52 hours (IQR 24–92). Twenty (39%) of the intervention arms were delivered in a group setting, 3 (6%) provided supervision to individuals, 15 (29%) were individually unsupervised and 13 (25%) involved a combination of group-based and individual exercise. In 20 (39%) interventions the participant-to-instructor ratio was not clearly reported. Of the 31 interventions, three had more than 10 participants per instructor. In 29 (57%) arms, the intervention was tailored to the individual initially and intervention was progressed based on individual assessment in 30 (59%) interventions. Thirty-two (63%) interventions were tailored in intensity or type and the remaining 19 (37%) were not tailored.
Characteristics of studies where the primary exercise component was Tai Chi
Compared with control, Tai Chi reduced the rate of falls by 19% (rate ratio 0.81, 95% CI 0.67 to 0.99; 2655 participants, 7 studies; low‐certainty evidence). The median programme duration was 20 weeks (IQR 15–43), with a median of 45 total hours of exercise (IQR 40–80). Tai Chi was delivered in a group in 10 (71%) intervention arms, delivered individually with supervision in 1 (7%) arm, individually without supervision in 1 (7%) arm; and with a combination of individual and group delivery in 2 (14%) arms. There was 1 (7%) intervention with one-on-one supervision and 7 (50%) interventions where the participant-to-instructor ratio was not clearly reported. Five Tai Chi intervention arms had more than 10 participants per instructor. None of the Tai Chi programmes were tailored to the individual initially and 1 (7%) intervention was progressed based on individual assessment. One (7%) intervention was tailored in intensity or type and the remaining 13 (93%) were not.
Characteristics of studies which involved multiple types of exercise
Multiple types of exercise (most commonly balance and functional exercises plus resistance exercises) reduced the rate of falls by 34% (rate ratio 0.66, 95% CI 0.50 to 0.88; 1374 participants, 11 studies; moderate-certainty evidence). The median programme duration was 25.5 weeks (IQR 12–52) and the median total hours of exercise was 54 hours (IQR 44–91). In 13 (54%) intervention arms, the multitype intervention was delivered in a group; in 5 (21%) arms, it was delivered individually without supervision; and in 6 (25%) there was a combination of individual and group delivery. There was 0 intervention with one-on-one supervision and 13 (54%) interventions where the participant-to-instructor ratio was not clearly reported. No interventions had more than 10 participants per instructor. The intervention was tailored to the individual initially in 18 (75%) and intervention was progressed based on individual assessment in 17 (71%) of interventions. Eighteen (75%) interventions were tailored in intensity or type and the remaining 5 (21%) were not tailored.
Components of studies in categories of exercise not found to prevent falls
The characteristics of studies in categories of exercise not found to be effective in preventing falls are outlined in online supplementary material D.
Risk of bias assessment
The summary of risk of bias is displayed in online supplementary material E. With regard to allocation, risk of selection bias for sequence generation was low in 67% (72/108) of the included trials, and unclear in the remaining 33% (36/108). Risk of selection bias for allocation concealment was low in 35% (38/108) of trials, high in 5% (5/108) and unclear in the remaining 60% (65/108). For blinding, participants and personnel delivering the intervention were potentially aware of their allocation status and falls were self-reported. The risk of performance bias (for blinding of participants and personnel) was low in 5% (5/108) of trials, high in 6% (6/108) and the remaining 89% (97/108) were unclear. The risk of detection bias (for ascertainment of falls) was low in 40% (43/108) of trials, high in 21% (23/108) and unclear in the remaining 39% (42/108). Risk of attrition bias, which may arise from incomplete outcome data, was low in 53% (57/108) of trials, high in 27% (29/108) and unclear in the remaining 20% (22/108). The risk of bias for selective outcome data was low in 12% (13/108) of trials, high in 48% (52/108) and unclear in the remaining 40% (43/108). The risk of ascertainment bias was low in 58% (63/108) of trials, high in 27% (29/108) and unclear in the remaining 15% (16/108).
Supplemental material
Discussion
A variety of clinical trials of exercise as a single intervention for falls prevention in community-dwelling older people have been published. There are clear implications for practice and research. Descriptions of the characteristics of exercise programmes that contributed to effective intervention types may guide clinicians in developing optimal programmes for their patients. Identification of gaps and methodological flaws in fall prevention studies will guide future research.
In summary, most trials took place in developed countries, involved a wide age range and predominantly comprised female participants. Most trial populations had higher risk of falls, indicated by history of falls, poor balance, recent hospitalisation or poor mobility as inclusion criteria. Adherence to exercise was suboptimal. Balance and functional exercises were the most common primary intervention and had the greatest effect on falls. The duration and hours of intervention varied. While most interventions were group based and tailored to the individuals, the level of supervision was not clearly reported. Furthermore, the majority of trials did not clearly report allocation concealment and blinding of participants and personnel.
Implications for practice
Within the effective interventions, involving balance and functional exercises, Tai Chi and multiple types of exercise (typically incorporating balance and strength exercises), there are different ways the interventions can be delivered. Clinicians and exercise programme providers need to note the characteristics of trials that contributed to fall prevention effects, and work with patients to establish the most suitable exercise programme for the individual.126
The updated Cochrane Review8 is consistent with previous systematic reviews6 7 127 that identified greater falls prevention effects from exercise programmes that challenge balance. This element was present in all the effective interventions: balance and functional training, Tai Chi and multiple types of exercise. Challenge to balance can be achieved by progressively reducing the base of support, removing upper limb support and moving the centre of gravity to challenge balance. Strength training alone did not prevent falls, however when included in a programme with balance training, a fall prevention effect was evident. This is consistent with previous research that recommend exercise programmes targeting falls may include strength training in addition to balance training.6 127
For exercise to be effective a sufficient intensity and duration of exercise is required. In the trials with interventions classified primarily as balance and functional training, the median intervention duration was 6 months, with a total of 52 hours (approximately 2 hours per week). In trials with interventions classified primarily as Tai Chi, the median duration was 4 months, with a total of 45 hours (approximately 2.8 hours per week). For trials with interventions that included multiple primary components, the median intervention duration was 6 months, with a total of 54 hours. This is less than the 3 hours of exercises per week recommended for falls prevention, following a previous systematic review with meta-regression.6 In addition, ongoing exercise is needed to maintain the falls prevention benefit of exercise.6 The trial nature of these programmes limited their duration and clinicians need to discuss strategies with their patients to keep them exercising in the long term.
The Cochrane Review found there may be no difference in the effect of exercise on the rate of falls where interventions were delivered in a group setting compared with trials where interventions were delivered individually.8 In the effective intervention types, home-based interventions were frequently delivered as, or based on, the Otago Exercise Program. Home-based interventions, or group-based interventions with less than 10 participants, were mostly tailored in type or progression. For home-based programmes, the instructor usually makes an initial home visit to the participant’s residence to individually tailor the programme, with follow-up sessions for assessment and progression. For the group-based intervention, an instructor may adjust the individual’s tasks within a predefined programme. On the other hand, most group interventions with more than 10 participants per instructor were not tailored to individuals. Clinicians need to balance the increased social support and adherence from supervised group-based intervention with the sustainable self-motivation for exercise from individualised home-based intervention.128 129 Interventions combining both delivery modes have the potential to provide the benefit from both sides.
Optimising adherence is another important consideration during design and implementation of an intervention programme.130 Given the suboptimal level of compliance, clinicians should therefore incorporate effective strategies to promote adherence such as involving the patients in shared decision-making, goal setting and framing the interventions as life enhancing.128 130
There is sufficient evidence available to support the use of exercise to prevent falls, providing clinicians an opportunity to implement evidence-based shared decision-making. Evidence-based medicine requires clinicians to integrate the evidence with patient preferences.131 A decision aid could be developed to help clinicians and patients aware of the options and programmes available to them in the area.132
Implications for research
Several areas of deficiency in the arena of falls prevention research were identified in this review. There is a lack of clinical trials investigating the effect of exercise in preventing falls from the African continent and China, areas that represent a significant proportion of older adults in the world and are ageing rapidly.133 Low and middle-income countries and low-income countries are also under-represented, presenting a barrier in translating cost-effective exercise interventions to clinicians in these countries.12 Furthermore, exercise intervention trials that specifically target males are lacking with only one trial available. While the risk and incidence of falls are greater in females, the mortality rate due to falls is higher for males, suggesting more clinical trials for men are needed in preventing particular circumstances of falls.134 There was insufficient research evaluating programmes containing primarily flexibility and endurance exercise and little research evaluating only resistance training and only walking programmes. Finally, there is a need for cost-effectiveness analysis to investigate any economic benefit of home-based or individually tailored interventions for falls prevention.
Risk of bias and deviation of clinical trials from study design and reporting guidelines reduces their credibility. The reporting of a substantial number of trials did not meet the standards of the Consolidated Standards of Reporting Trials statement,135 for example, one-third omitted a sufficient description of randomisation and almost two-thirds did not describe allocation concealment. Due to the nature of exercise interventions, it is extremely difficult to blind the participants or personnel. This amplifies the need to minimise the risk of ascertainment bias (bias in the recall of falls due to unreliable methods of ascertainment); yet 42% did not satisfy the criteria for low risk. Falls are under-reported when data are collected on a three monthly basis, compared with daily.136 To minimise bias, the ascertainment of falls should follow the ProFaNE consensus137 of daily recording of falls using falls calendars and monthly follow-up analysis performed by researchers blind to participants’ allocation. Almost half of the studies did not report participant-to-instructor ratio; consistent reporting guidelines on the level of supervision should be promoted. Evidence-based medicine is the implementation of high-quality evidence in clinical practice13; however, if the presentation of the evidence is not of high quality, then it would impede the utilisation of the findings by clinicians. Therefore, quality study methodology and satisfaction of the reporting guidelines should be promoted.
This report has limitations. This review did not include trials specifically recruiting older adults with dementia, stroke, Parkinson’s disease, multiple sclerosis or hip fracture. While these conditions are associated with a higher risk of falls, the effect of exercise on falls in these populations has been covered previously138 139 and we aim to make the study results generalisable to the community-dwelling older people. Exercise as part of a multicomponent intervention was excluded from this review as this is covered elsewhere.9 Coding of intervention type was limited to the information available in the papers or provided by the authors, which may be inaccurate. Multiple databases were searched and studies published in language other than English were included in an effort to minimise publication bias. More research is needed for categories of interventions not found to prevent falls and readers should be cautious to interpret it as ‘no evidence of effect’ rather than ‘evidence of no effect’.
Conclusion
This review identified the diversity of trials that evaluate the effect of exercise on falls in community-dwelling older people, in terms of participants’ age and baseline fall risk, intervention type, duration and delivery mode. Implications for clinicians include implementing balance challenging exercise programmes, of adequate duration, in a setting optimal for the patient, with strategies to promote exercise uptake. Further research is needed regarding exercise for fall prevention in low-income countries and in males. Future trials should minimise bias, comply with reporting guidelines and report factors relevant to facilitating translation to clinical practice.
Acknowledgments
We are very grateful for the extensive support from the Cochrane Bone, Joint and Muscle Trauma Group in the preparation of the Cochrane Review. The names of editorial base members, Cochrane editors, external referees, consumer peer referees, copyeditors and other contributors are listed in the Acknowledgements section in the full Cochrane Review.
References
Footnotes
Contributors CAN was involved in data extraction, data analysis, and co‐led the writing of the review. NF was involved in screening, data extraction, data analysis, and co‐led the writing of the review. GW was involved in screening, data extraction, data analysis, and contributed to writing the review. AT and ZAM were involved in screening, data extraction, data analysis, and contributed to writing the review. CS was involved in screening, data extraction, data analysis, co‐led the writing of the review and acted as guarantor of the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer No review author was involved in study selection or processing of any trials in which they were or are involved.
Competing interests CS and AT are currently running trials of fall prevention interventions, funded by national grant agencies, which are not included in this review. CS is an author of several trials considered in this review, including four included trials (Merom et al (2016); Sherrington et al (2014); Vogler et al (2009); Voukelatos et al (2015)). CN, NF, GW, AT and ZAM have no known conflicts of interest.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.