Article Text

Abstract
Objective To compare the effects of moderate intensity continuous training (MICT) and high intensity interval training (HIIT) on adult lipid profiles; to identify training or participant characteristics that may determine exercise-induced change in total cholesterol (TC), triglycerides (TRG), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C).
Design Systematic review and meta-analysis.
Data sources English language searches of several databases were conducted from inception until September 2019.
Eligibility criteria for excluding studies Inclusion: (1) published randomised controlled human trials with group population n≥5; (2) intervention duration ≥4 weeks; (3) comparing HIIT with MICT; and (4) reporting pre–post intervention lipid measurements. Exclusion: subjects with chronic disease, <18 years, pregnant/lactating, in elite athletic training; and studies with a dietary or pharmaceutical intervention component.
Results Twenty-nine data sets (mmol/L) of 823 participants were pooled and analysed. Neither HIIT nor MICT was better in decreasing TC (0.10 (−0.06 to 0.19), p=0.12, I2=0%), TRG (−0.05 (−0.11 to 0.01), p=0.10, I2=0%), LDL-C (0.05 (−0.06 to 0.17), p=0.37, I2=0%), or TC/HDL-C (−0.03 (−0.36 to 0.29), p=0.85, I2=0%). HIIT significantly raised HDL-C (0.07 (0.04 to 0.11), p<0.0001, I2=0%) compared with MICT.
Conclusion Neither HIIT nor MICT is superior for altering TC, TRG, or LDL-C, or TC-HDL-C ratio. Compared with MICT, HIIT appeared to significantly improve HDL-C. Clinicians may prescribe either protocol to encourage participation in exercise and reduce cardiovascular risk. To raise HDL-C, HIIT may result in a larger effect size compared with MICT.
PROSPERO registration number CRD42019136722.
- lipids
- cholesterol
- triglycerides
- lipoprotein
- exercise training
- exercise intensity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known?
Aerobic physical activity positively impacts blood lipids, however lack of time and enjoyment are cited as impediments to exercising.
High-intensity interval training (HIIT) appears to offer greater benefits compared with moderate intensity continuous training (MICT). Protocols are formulated to require less time spent training, however higher intensity may negatively impact enjoyment.
Sufficient volume of aerobic physical activity is necessary to induce changes to blood lipids, however little agreement exists as to whether the shorter session duration of high-low intensity intervals or the moderate intensity of longer session steady-state exercise best changes effect size.
What are the new findings?
HIIT does not out-perform MICT in positively affecting total cholesterol (TC), triglycerides (TRG), low-density lipoprotein cholesterol (LDL-C) and the TC/high-density lipoprotein cholesterol (HDL-C) ratio. However, MICT seems to be inferior to HIIT for inducing positive changes to HDL-C.
Participant (age, gender and presence of Metabolic Syndrome (MetS) or MetS factors/risk) and intervention (weight-bearing) characteristics do appear to influence effect size.
The multiplicity of HIIT protocols is an obstacle to endorsing a specific HIIT regime most effective for positively impacting blood lipids while accounting for time and enjoyment needs, although HIIT could be chosen in preference to MICT for improving HDL-C.
Introduction
An abnormally elevated or lowered blood lipid profile, known as dyslipidaemia, is a significant risk factor of cardiovascular disease (CVD)1 2; ischaemic stroke3; non-alcoholic fatty liver disease (NAFLD)4; and chronic pancreatitis.5 6 Dyslipidaemia frequently coexists with other Metabolic Syndrome (MetS) factors such as obesity (Ob)7 and type 2 diabetes (T2D)8 9; and MetS is implicated in CVD risk.10 Moderate-intensity and vigorous-intensity aerobic physical activity positively impacts MetS factors, thus lowering CVD risk.11 12 Studies13 14 and systematic reviews15 16 have shown aerobic exercise reduces elevated total cholesterol (TC), triglycerides (TRG) and low-density lipoprotein cholesterol (LDL-C) and increases high-density lipoprotein cholesterol (HDL-C) in subclinical and clinical populations.
Much published work has examined and confirmed the beneficial physiological effects of aerobic physical activity or moderate intensity (55%–70% of maximal heart rate (MHR), rate of perceived effort (RPE) of 11–13 on the Borg scale)17 continuous training, known as MICT. The WHO recommends a minimum of 150 min per week of aerobic physical activity at moderate continuous intensity, or 75 min at higher intensity, to maintain or achieve health. However, WHO reports insufficient aerobic physical activity levels among adults>18 years.18 Poor adherence to such recommended aerobic activity or MICT protocols results from lack of time,19 and lack of support.20 Although enjoyment of exercise is positively associated with incidence of physical activity in adults, absence of enjoyment has not been significant in explaining lack of exercise, and attitudes towards exercise lack positive association with incidence of aerobic physical activity.21 Such findings have prompted searches for alternatives to MICT in order to address continuing insufficient aerobic physical activity levels.
High intensity interval training (HIIT) is a protocol of short work intervals<60 s–8 min22 of vigorous (70%–90% MHR or RPE Borg scale 14–16)17 to high intensity (≥90% MHR or ≥RPE Borg scale 17)17 interspersed with active (40%–70% MHR or RPE Borg scale 8–13)17 or passive (cessation of movement) recovery periods of 1–5 min.22 HIIT has been employed since the mid-20th century to improve athletic exercise performance.22 Contemporary protocols developed for non-athletes are intended to reduce session time and provide a greater stimulus for physiological and psychological adaptation compared with MICT.
HIIT has been shown to increase peak oxygen consumption (VO2MAX or VO2PEAK) compared with MICT in cardiovascular disease (CVD) populations,23 despite VO2MAX being only one component of positive changes to cardiorespiratory fitness.24 Studies indicate that a positive impact on biomedical health indices is protocol dependent in clinical25 and healthy26 populations.
To encourage individuals to undertake aerobic physical activity, both HIIT27 and MICT28 are promoted as enjoyable and effective, although no consensus exists as to which aerobic exercise protocol is more so. Studies have shown a minimum volume of weekly aerobic exercise for a minimum duration29 and a weekly aerobic exercise energy expenditure (EEE) threshold of 1200–2200 kcal30 is necessary to induce positive changes to lipids. Systematic reviews and meta-analyses of the effect of aerobic physical activity on lipid levels have established that longer intervention and session duration results in greater effects.31 32
A systematic review comparing HIIT against MICT found no difference on blood lipids in healthy and clinical populations, but no meta-analysis was conducted.33 A pooled analysis comprising only three studies and consisting of CVD, MetS and overweight populations unsurprisingly showed equivocal effects on serum lipids.34 Other systematic reviews16 35 36 and meta-analyses15 37–40 have investigated the effect of exercise on lipids, but have not compared HIIT against MICT. Thus no previously published meta-analysis exists that has examined the effects of HIIT versus MICT on lipids in subclinical populations.
The aim of this study was therefore to conduct a systematic review and meta-analysis comparing the effects of HIIT and MICT on TC, TRG, HDL-C, LDL-C and TC/HDL-C in subclinical populations and to examine whether one protocol surpassed the other.
Methods
This systematic review and meta-analysis was registered in the International Prospective Register of Systematic Reviews.41 Its results are presented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.42
Search strategy
GW and NS conducted systematic English-language searches of PubMed, all EBSCO health and medical databases including SPORTDiscus, MEDLINE and CINAHL, as well as Web of Science and EMBASE from inception to September 2019.
Searches included a mix of MeSH and free text terms relevant to the concepts of: exercise training intensity for example, (high OR HIIT OR sprint OR SIT OR vigorous AND moderate continuous OR MICT OR moderate intensity continuous exercise (MICE) OR continuous moderate exercise (CME)); interval training for example, (intermittent OR interval OR reps AND training OR exercise); intervention duration for example, (weeks NOT single bout); exercise-induced lipid metabolism; metabolic syndrome for example, (metabolic syndrome OR MetS OR T2D OR diabetes OR hypertension OR overweight OR obese); and blood lipids for example, (lipids OR cholesterol OR lipoprotein OR triglycerides). Searches excluded for pregnancy, lactation, elite athletes, juveniles, CVD, stroke, cancer and NAFLD. Systematic reviews and reference lists of papers were hand searched for additional studies.
Participants and interventions inclusion/exclusion criteria
Subclinical (healthy or overweight or MetS or MetS factors such as hypertensive), and clinical (Ob and T2D) participants taking usual medications, and with a sample size population of n≥5 in HIIT and MICT groups were included.
Two distinct exercise protocols differentiated by effort as per established guidelines17 and described as either steady state (MICT) or higher effort plus active or passive recovery intervals (HIIT), separate to warm up and cool-down, were required. No restrictions were placed on exercise session time, number and time length of work and recovery intervals or exercise type. Levels and measurement of effort such as percentage of VO2PEAK or VO2MAX, percentage of peak heart rate (HRPEAK) or MHR or heart rate reserve or individual anaerobic threshold heart rate (HRIAT), Borg scale, metabolic equivalent (MET), or percentage of workload or watts (WMAX or WPEAK) were required. Resistance-training or combined-training interventions without separate HIIT and MICT interventions as comparators were excluded.
Comparator
HIIT protocols as the intervention were compared against MICT protocols as the control for differentiated impacts on blood lipids.
Outcomes
Pre–post intervention lipid measurements reported as mmol/L or mg/dL for any of TC, TRG, HDL-C, LDL-C or TC/HDL-C were required.
Study selection
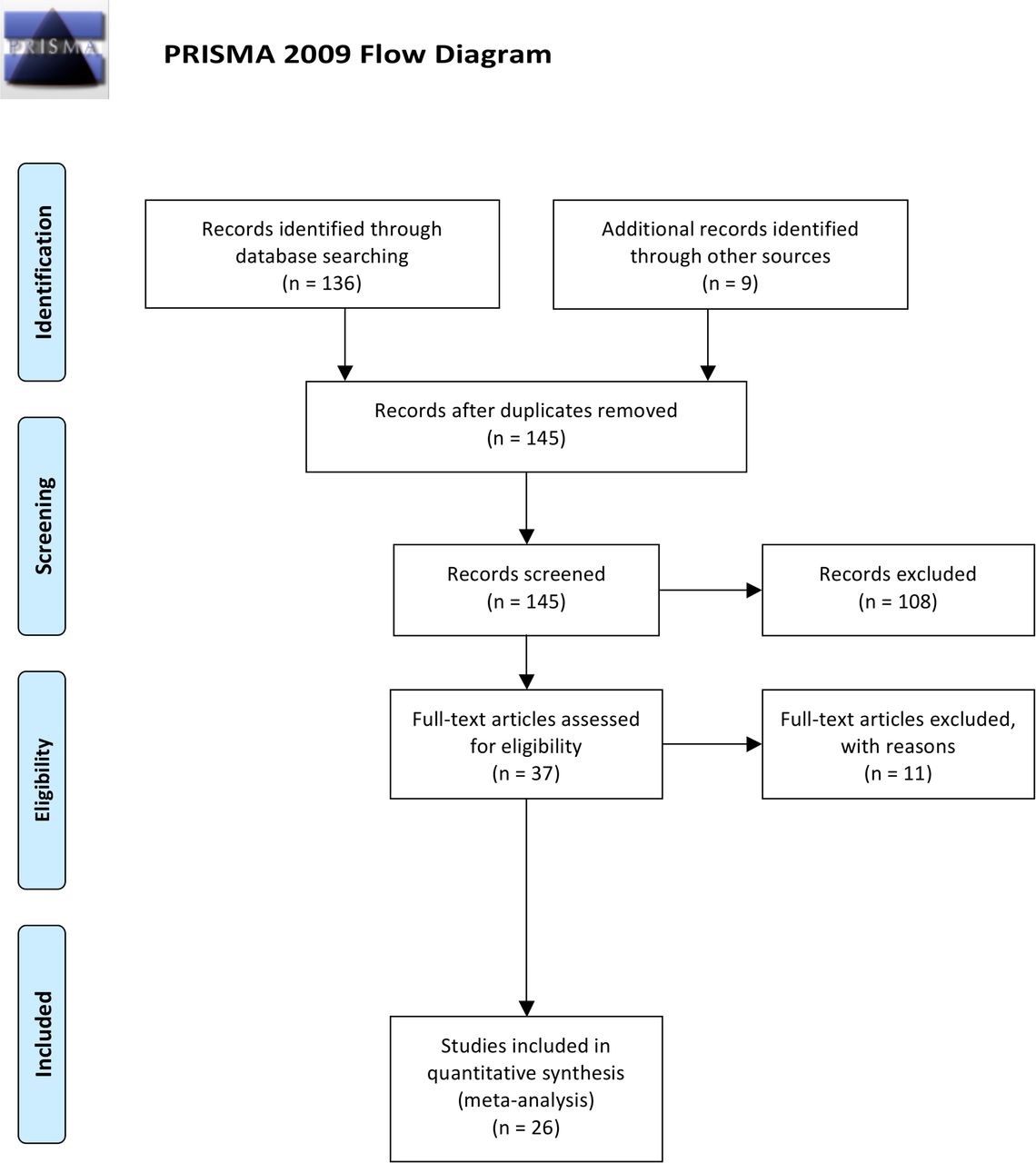
GW and NS assessed the resulting titles and abstracts of randomised controlled trials (RCTs) lasting ≥4 weeks, which compared HIIT and MICT protocols, and reported pre–post intervention lipid measurements in humans≥18 years. Subsequently, the full text of potentially eligible studies was reviewed according to participant, intervention and outcome inclusion and exclusion criteria. TvdT was consulted to resolve disputes. The flow of papers through the search and inclusion process is presented in figure 1.
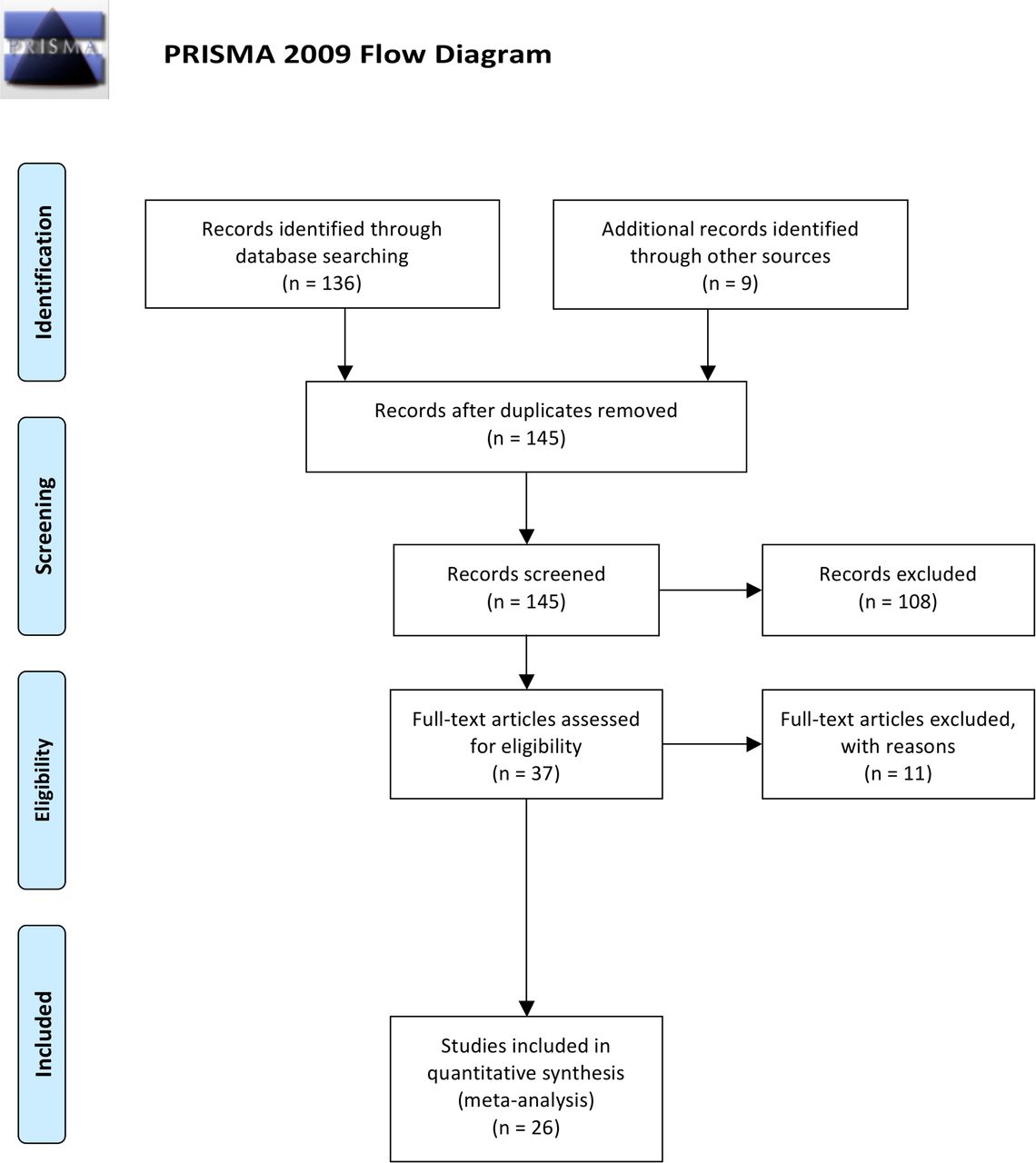
PRISMA flow diagram adapted from Moher et al.42 PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data extraction
GW and AM extracted the data to a pre-established extraction form and NS and TvdT confirmed the data extraction. For each study the following information was extracted: (1) author(s), year of publication and study design characteristics, (2) demographic and clinical characteristics, (3) HIIT intervention and MICT control protocols, (4) values before and after HIIT intervention and MICT control for any of TC, TRG, HDL-C, LDL-C or TC/HDL-C ratio and expressed as mean (M) or mean difference (MD), SD or converted to SD (SE using SD=square root (Sample Size) x SE), as well as main findings concerning lipids.
Data synthesis
Statistical analyses were performed using Revman V.5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark) for continuous data by using the MD and SD of the MD. Where the MD and SD of the MD were not reported, the MD was calculated by subtracting the preintervention M from the postintervention M. The SD of the MD was calculated as follows: SD=square root [(SDpre-treatment)2 + (SDpost-treatment)2 – (2 r x SDpre-treatment x SDpost-treatment)], assuming a correlation coefficient (r)=0.5, considered a conservative estimate.43 Revman V.5.3 also enabled calculations of the SD of the MD using group sample size and p values or 95% CIs when provided. Where data was not presented in text or tables and authors could not be reached, data presented in figures was extracted where possible.
Data were pooled for meta-analysis when two or more studies measured the same outcome and provided data in a format suitable for pooling. Where a study included multiple HIIT groups, data were entered separately for each group and the sample size of the MICT group was divided by the number of HIIT groups to eliminate inflation of the sample size. GW entered the data in Revman V.5.3; TvdT reviewed the data entry for accuracy. A random effects inverse variance model was used with the effects measure of MD, a 5% level of significance and a 95% CI to report change in outcome measures. This model was chosen to allow for different effect sizes achieved across selected studies.44
Meta-analysis and subanalyses
For meta-analysis of the four cholesterol fractions and single ratio, all included studies were grouped under each fraction and data was pooled. Subanalyses were conducted according to: age; gender; presence or absence of MetS risk and/or factor(s) or T2D; and weight-bearing or non-weight-bearing exercise.
Sensitivity analysis
In order to evaluate the influence of each study on the overall effect size of pooled data, we conducted iterative leave-one-out sensitivity analyses.45 Where subanalyses gave rise to significance, iterative leave-one-out analysis (K−1, where K=the number of studies, and each study is excluded from the pool analysis one at a time) was also conducted.
Heterogeneity and publication bias
Heterogeneity was quantified using the I2 test where heterogeneity values range from 0% (homogeneity) to 100% (complete heterogeneity).46 Visual inspection of funnel plots was used to assess risk of publication bias.47 If the 95% CIs of a study were outside the pooled 95% CIs, the study was removed as an outlier.48
Study quality
Study quality was assessed by AM and GW and reviewed by NS and TvdT, using the validated Tool for the Assessment of Study Quality and Reporting in Exercise (TESTEX),49 a 15-point scale specific to exercise training studies. A score ≥10 indicates a better study quality and reporting. In the case of discrepancies NS was consulted. A study quality subanalysis of studies grouped according to TESTEX scores (≥10,<10) was also conducted.
Results
Combined searches generated a total of 126 articles. After removal of duplicates and exclusion of articles based on abstract and title, 37 full-text articles remained for screening. One study using a non-HIIT protocol,50 two studies using dietary intervention,51 52 two studies of increasing intensity not high-intensity intervals,13 53 one study with no MICT group,54 one study reporting only preintervention values,55 one study combining outcome measures of both protocols,56 and a feasibility study57 were excluded. One study tested two HIIT protocols, one of which was excluded.58 Two further excluded studies were non-RCTs.59 60 Three studies61–63 tested two HIIT protocols against the same group of MICT participants, hence after screening, a total of 29 data sets from 26 studies24 25 58 61–82 met the stated inclusion criteria.
Study, participant, and intervention characteristics
Summarised descriptions of studies, participants and interventions included in trials are provided in Table 1 below and detailed descriptions in online supplementary file 1.
Supplemental material
Studies and PICO
Comparative outcome measures
Total cholesterol
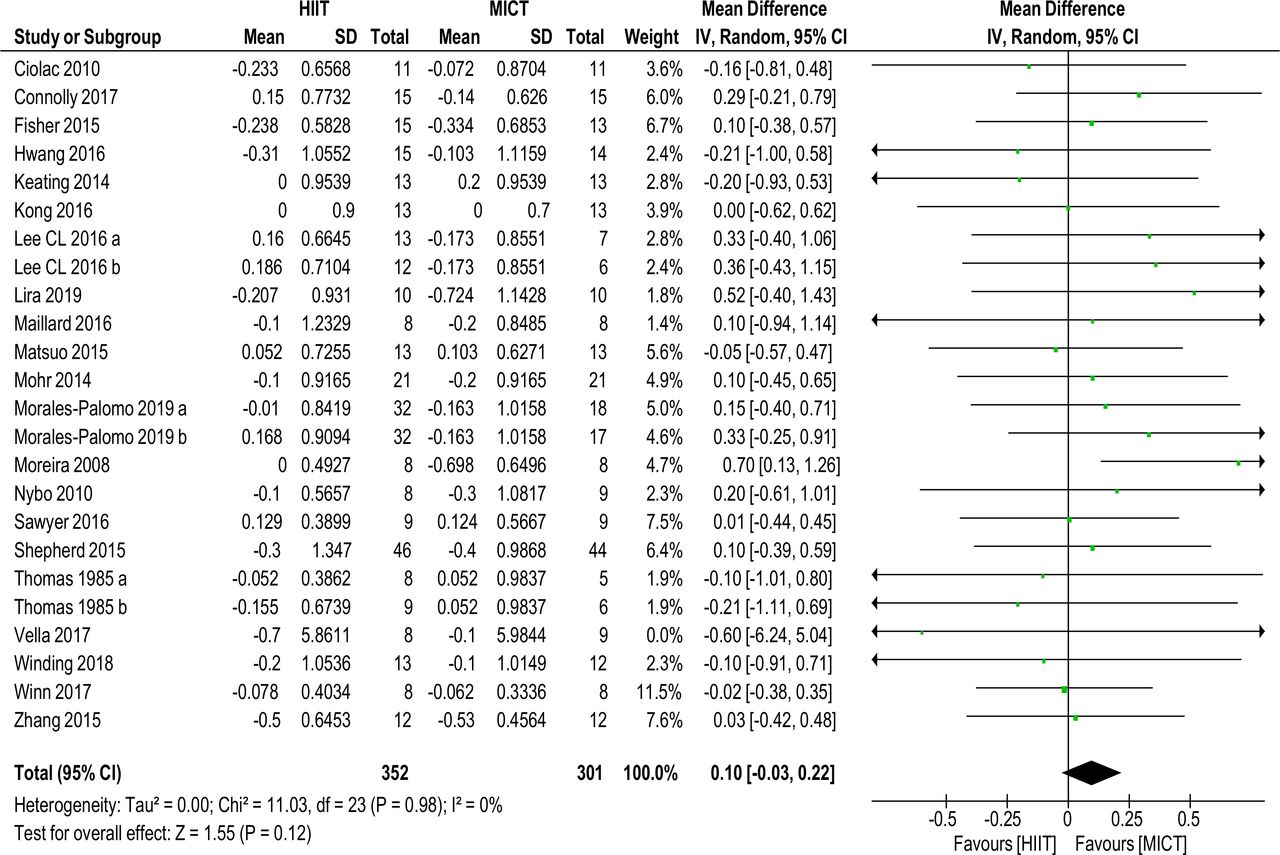
Twenty-one studies of 24 data sets with a total of 653 (352 HIIT, 301 MICT) subjects reported on TC MD (0.10 mmol/L (−0.03 to 0.22), p=0.12, I2=0%), shown in figure 2. No significance was found. Sensitivity analysis (K−1) did not change results.
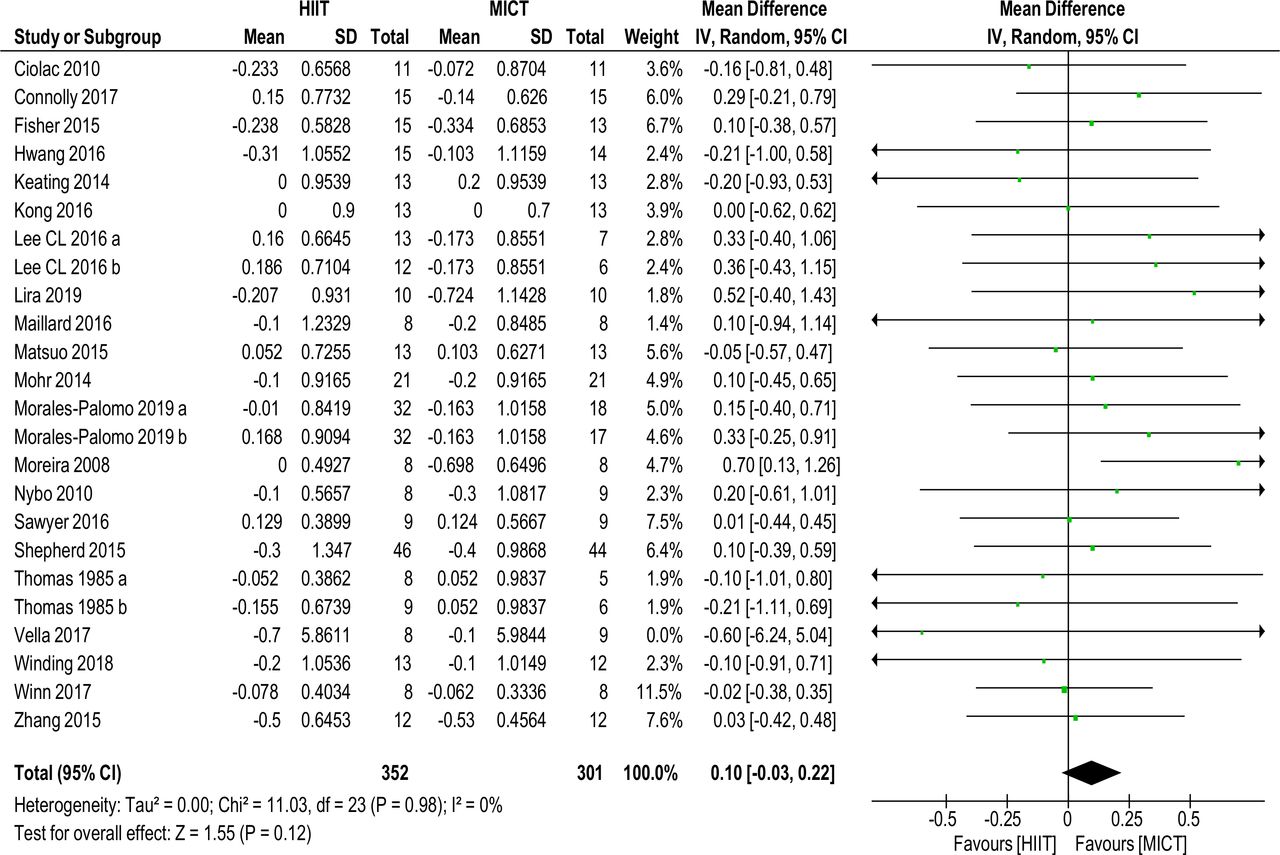
Total cholesterol. MD and SD expressed as mmol/L; Total = number of participants. HIIT, high intensity interval training; MICT, moderate intensity continuous training, MD, mean difference.
Subanalyses did not change significance, see online supplementary files table 2.
Triglycerides
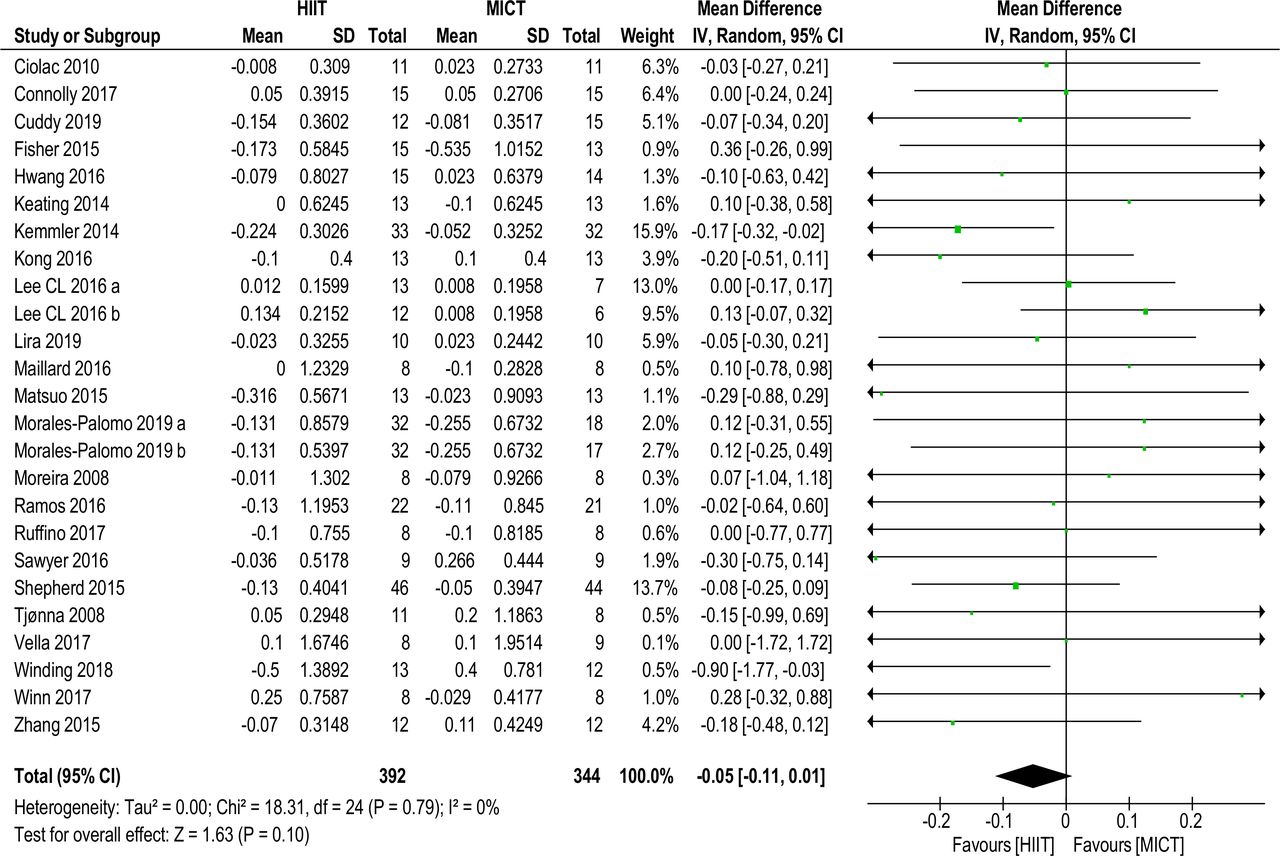
Twenty-three studies of 25 data sets with a total of 736 (392 HIIT, 344 MICT) subjects reported on TRG MD (−0.05 mmol/L (−0.11 to 0.01), p=0.10, I2=0%), shown in figure 3. No significance was found. Sensitivity analysis (K−1) did not alter significance.

Triglycerides. MD and SD expressed as mmol/L; Total = number of participants. HIIT, high intensity interval training; MICT, moderate intensity continuous training, MD. mean difference.
Subanalyses changed significance in favour of HIIT for (1) age grouping 35–55 years (−0.10 mmol/L (–0.19 to –0.01), p=0.03, I2=0%); (2) Mets or MetS factors/risk (−0.10 mmol/L (–0.18 to –0.02),p=0.01, I2=0%); and (3) weight-bearing protocols (−0.11 mmol/L (–0.21 to 0.00), p=0.04, I2=0%). Sensitivity analysis (K–1) of these these subanalyses resulted in no significance with the removal of one study,24 see online supplementary files table 2.
High-density lipoprotein cholesterol
Twenty-six studies comprising 28 data sets with a total of 739 (384 HIIT, 355 MICT) subjects reported on HDL-C MD (0.07 (0.04 to 0.11), p<0.0001, I2=0%), as shown in figure 4, and favoured HIIT. Removal of one outlier70 did not alter significance. Sensitivity analysis (K–1) resulted in insignificance with the removal of one study,24 HDL-C MD (0.04 mmol/L (0.00 to 0.08), p=0.06, I2=0%), see online supplementary files table 2.

High density lipoprotein-cholesterol. MD and SD expressed as mmol/L; Total = number of participants. HIIT, high intensity interval training; MICT, moderate intensity continuous training, MD. mean difference.
With the exception of age (all) and gender (females), subanalyses remained significant for HIIT. Applying sensitivity analysis (K–1) to subanalyses resulted in insignificance for the weight-bearing grouping only, see online supplementary files table 2.
Low-density lipoprotein cholesterol
Twenty data sets of 580 (313 HIIT, 267 MICT) subjects reported on LDL-C MD (0.05 mmol/L (−0.06 to 0.17), p=0.37, I2=0%), shown in figure 5. No significance was found. Sensitivity analysis (K–1) did not change significance.

Low density lipoprotein-cholesterol. MD and SD expressed as mmol/L; Total = number of participants. HIIT, high intensity interval training; MICT, moderate intensity continuous training, MD. mean difference.
Subanalyses did not change significance, see online supplementary files table 2.
TC/HDL-C ratio
As shown in figure 6, three studies with a total of 72 subjects reported on the TC/HDL-C ratio MD (−0.03 mmol/L (−0.36 to 0.29), p=0.85, I2=0%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
TC/HDL-C ratio. MD and SD; Total = number of participants. HDL-C, high-density lipoprotein cholesterol; HIIT, high intensity interval training; MICT, moderate intensity continuous training, MD. mean difference; TC, total cholesterol.
Heterogeneity and publication bias
Meta-analyses indicated zero heterogeneity for all lipid fractions, and the TC/HDL-C ratio. Visual inspection of funnel plots showed moderate-to-high likelihood of publication bias for TC and TRG, and low-to-moderate likelihood for HDL-C and LDL-C, see online supplementary files figures 2-6.
Study quality and reporting
A median TESTEX score of 11 out of 15 was obtained (range 7 to 13). TESTEX scores (≥10 or<10) did not alter significance and heterogeneity, moreover sensitivity analysis (K–1) did not affect these results, see online supplementary files table 3. No study was excluded based on its TESTEX score.
Lipid assessment
Lipid assay details are provided in online supplementary files table 4. No study was excluded based on lipid assay reporting.
Discussion
Meta-analysis
This systematic review and meta-analysis aimed to compare the effects of HIIT and MICT on adult blood lipid profiles in subclinical populations and to examine whether one protocol was superior to the other. Our review is the first to include more than eight trials and compare the effect size of intermittent high–low intensity and continuous moderate intensity in positively altering TC, TRG, HDL-C, LDL-C and the ratio of TC/HDL-C in subclinical populations. Our analysis, of 29 data sets from 26 studies, assessed the effects on lipids of weight-bearing and non-weight bearing HIIT and MICT exercise therapies excluding concurrent dietary or pharmaceutical interventions. Although HIIT and MICT appear to induce positive changes, our analysis did not demonstrate that intermittent high-intensity out-performed continuous moderate-intensity protocols in achieving better lipid outcomes.
Outcome measures
Total cholesterol
We found no statistically significant evidence showing a benefit in favour of HIIT or MICT in reducing TC. Our results are similar to a previous qualitative review comparing exercise with no exercise.33 Our results differ from the findings of others38–40 whose works did not differentiate for continuous or interval protocols. We also included papers with intervention duration of 4–6 weeks; these are arguably of insufficient duration to effect change.33 MICT has been shown to prioritise fat as a primary substrate fuel in subclinical populations,83 hence it could be reasonably expected that MICT would outperform HIIT. However, a weekly energy expenditure30 or volume15 29 31 is required before impacts on lipids can be observed, and a number of included protocols likely fell short of this threshold. We excluded studies including dietary intervention which may have impacted our results.84
Triglycerides
We found no difference in effect size between HIIT and MICT in positively altering TRG except for subanalyses. Our results broadly agree with a recent meta-analysis,85 although we excluded trials of cardiac patients. Our results also agree with a previous qualitative review.33 We differ from the work of others,38–40 possibly because we included mixed populations or because we differentiated for protocol and intensity. A systematic review suggested TRG responded favourably to increased exercise intensity in MetS populations,16 agreeing with a previous meta-analysis,39 and our subanalysis (MetS or MetS factors/risk) found HIIT significantly lowered TRG more than MICT.
High-density lipoprotein cholesterol
HIIT showed significance compared with MICT for affecting HDL-C, however sensitivity analysis (K–1) contradicted this result. Our findings agree with a previous meta-analysis,39 although this work compared exercise with no exercise only and focussed on overweight and obese populations. We also agree with the results of a recent meta-analysis comparing intensity, although this work focussed on studies of subjects with cardiovascular conditions.85 Our results are dissimilar to other systematic reviews,16 33 36 and two (one female and one male) meta-analyses,38 40 although none of these works compared for intensity. Given the greater impact on cardiorespiratory fitness of HIIT compared with MICT,23 55 our result is not unexpected, as HIIT would most likely outperform MICT in optimising lipid transport via an improved microvascular capillary network. However, both HIIT and MICT have been shown to equally improve muscle microvascular density.86
Low-density lipoprotein cholesterol
We found no significance for preferring HIIT to MICT for positively changing LDL-C. Our findings agree with other meta-analyses.39 85 We differ from two meta-analyses comparing exercise with no exercise and examining general populations,38 40 as well as a meta-analysis comparing intensity and examining LDL-C in overweight and obese populations.87 We surmise this is a corollary of our inclusion of studies with healthy participants, although our subanalyses of clinical and subclinical participants did not affect significance. Previous work showing that LDL-C falls when accompanied by weight loss has been corroborated by a later meta-analysis comparing exercise with no exercise in overweight and obese groups.30 39 A recent meta-analysis of HIIT compared with MICT in these populations showed no preference for either protocol in achieving weight loss.86 88 Existing higher base levels of lipids in these populations7 may have led to sufficient decrease in LDL-C to demonstrate significance for HIIT protocols.14 According to one systematic review, increasing intensity is required to impact LDL-C,16 hence MICT by its nature should have shown inferiority to HIIT. Insufficient intervention duration and probable similar overall intensity in the protocols of included studies may have obfuscated our results.
TC/HDL-C ratio
HIIT and MICT were equivalent in reducing TC/HDL-C ratio.
Clinical significance and future research
Our meta-analysis results indicate HIIT seems to be superior to MICT in affecting HDL-C. Either HIIT or MICT can be prescribed to positively affect TC, TRG, LDL-C and the TC/HDL ratio, as part of efforts to increase exercise participation to meet current aerobic physical activity guidelines.18 Previous studies and reviews suggest a weekly minimum EEE of >1200 kcals and time commitment >150 min of aerobic physical activity at vigorous intensity is necessary to positively impact lipids.26 30 31 33 These indicative minimum requirements exceed current weekly aerobic physical activity guidelines of 150 min at moderate intensity or 75 min at vigorous intensity.89 Sharing the results of these studies and reviews may motivate some demographics to participate in and/or increase aerobic physical activity.
Based on the number of HIIT or MICT sessions per week, our included studies generally met the minimum weekly time requirements of current aerobic physical activity guidelines.89 The EEE, effort, session duration and frequency achieved in several studies were unlikely to meet the levels required to positively impact lipids.26 30 31 33 We propose that future research should address the following criteria to ascertain whether HIIT or MICT is better in inducing desirable changes in TC, TRG and LDL-C for varying populations: interventions should aim for duration >8 weeks (excluding familiarity sessions) as previously established31 33; protocols should achieve a weekly EEE threshold >1200 kcals,30 or minimum session duration and frequency26; and HIIT interventions should ensure that the overall effort (work:recovery ratio and repetitions) remains at or close to vigorous intensity per session, since higher intensity has been shown to impact more favourably on lipids than lower intensity.13 26
Strengths and limitations in the systematic review and meta-analyses
This review has a number of strengths. To our knowledge, this review and quantitative meta-analysis is the first to compare the effects of intermittent high-intensity and continuous moderate-intensity weight-bearing and non-weight bearing protocols on cholesterol fractions and the TC/HDL-C ratio in healthy, subclinical and clinical adult populations.
Previous systematic reviews did not use the validated exercise study evaluation tool TESTEX48 to measure the quality of included studies. We followed a rigorous inclusion and exclusion protocol to ensure minimisation of confounding factors among the study populations.90
A major limitation of this review is the relatively small number of studies used in our subanalyses. This is compounded by the varying populations studied and the different exercise protocols (number and length of effort and recovery intervals, intensities, session and intervention duration, session frequency and energy expenditure) used for comparing HIIT against MICT. Some studies did not report all lipid fractions. In addition, reporting of protocol adherence and intensity used objective for example, electronic devices as well as subjective measures for example, Borg scale, self-reported HR, log books, denoted by different indices of intensity (energy expenditure, VO2MAX, MHR, METs, Borg scale).
Aerobic physical activity protocols mainly consisted of running, swimming, walking, or cycling, which could have influenced results. While the majority of studies included in the analysis specified intervention duration ≥8 weeks, a small number of included studies used an intervention duration of 4–6 weeks, which may have weakened results.
With respect to data pooling, we measured the difference between preintervention and postintervention means; in cases where the MD SDs were not available, we imputed the SD using pre–post SDs, p values, and 95% CIs, and hence statistical analyses depended on extrapolated data. Our imputation was conservative, and sensitivity analyses (leave-one-out) were conducted. This approach may have weakened results.
The results of our analysis may have been affected because some of the studies measured lipids as secondary and not as primary outcomes. We therefore infer that some studies were perhaps not designed with the primary goal of lipid lowering. In the paragraph on clinical significance above, we have demonstrated that earlier reviews suggest a minimum weekly EEE of >1200 kcals, thus some of the studies that met our inclusion criteria may have failed to meet the minimum applicable EEE, session duration and session frequency required to positively impact lipids.
Conclusion
Pooled analysis indicated that aerobic physical activity intensity did not influence effect size for change in TC, TRG, LDL-C and TG/HDL-C. Change in the effect size of lipids seems to be sensitive to physical activity volume rather than intensity. The exception to this appears to be HDL-C which improved more with HIIT than MICT. Our findings suggest that HIIT protocols do not confer greater improvements in lipid profiles over MICT protocols. Clinicians and allied health specialists should therefore endeavour to encourage people to undertake aerobic physical activity at or above the minimum threshold (about 1200 kcal weekly) as a treatment or prevention strategy likely to be effective in managing lipid profiles and reducing CVD risk.
References
Footnotes
Contributors GW and NS designed the systematic review and meta-analysis, and performed searches. TvdT reviewed search results. Data extraction was performed by GW and AM. Data validation was performed by GW, AM, NS and TvdT. Data synthesis was performed by GW and AM. The article was written by GW with revisions suggested by AM, NS and TvdT.
Funding GW is supported by an Australian Government Research Training Program (RTP) Scholarship. This work received no other financial support and has no relationship to industry.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This systematic review and meta-analysis used pooled data from previously published peer-reviewed articles for which the corresponding ethics approval was obtained by the authors of these previously published studies.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on request.