Article Text

Abstract
Objectives Dynamic ultrasound (US) imaging shows promising possibilities for accurate imaging in diagnosing anterior cruciate ligament (ACL) tears and can be used as a point-of-care test. The aim of this study is to determine the diagnostic accuracy of dynamic US imaging for detecting partial and complete ACL tears.
Methods 247 patients presenting with knee complaints, who underwent dynamic US imaging as well as arthroscopy for any intra-articular knee pathology, were retrospectively evaluated. We differentiated between partial and complete ACL tears.
Results Dynamic US imaging revealed 95 of 108 arthroscopically confirmed ACL tears (sensitivity 88%, specificity 82%, positive predictive value (PPV) 79%, negative predictive value (NPV) 90%, and diagnostic OR (DOR) of 33.3). Sensitivity of US in the detection of partial ACL tears was 52%, specificity 85%, PPV 52%, NPV 84% and DOR 5.8. Complete ACL tears were depicted with a sensitivity of 79%, specificity of 89%, PPV of 63%, NPV of 95% and DOR 29.8. Multivariate regression analysis adjusting for age (dichotomised per 5 years) and previous knee surgery showed similar DOR.
Conclusion The excellent NPV for complete ACL tears indicates that dynamic US imaging can be used as an initial imaging point-of-care test. However, the clinical presentation should be taken into account, especially in case of subtotal tears. Whereas it seems relatively easy to differentiate between (small) partial ACL tears, complete ACL tears and no tears, it seems to be difficult to differentiate subtotal tears from complete tears.
- ACL
- knee
- ultrasound
- diagnosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What are the new findings?
Our study indicates that dynamic ultrasound (US) imaging of the knee is accurate in diagnosing complete anterior cruciate ligament (ACL) tears, but the sensitivity for partial tears is low.
It seems relatively easy to differentiate between (small) partial ACL tears, complete ACL tears and no tears; however, it seems to be difficult to differentiate subtotal tears from complete tears.
How might it impact on clinical practice?
Since MRI seems not to be superior to dynamic US imaging in diagnosing complete and partial ACL tears, dynamic US imaging can be used as an initial imaging point-of-care test.
The dynamic nature of the US imaging enables us to distinguish between partial and subtotal tears. This finding is of influence in the decision for treatment (either conservative or operative) especially in the sport active younger patients.
Introduction
MRI is an established imaging test for diagnosing anterior cruciate ligament (ACL) tears. According to the guidelines of American Academy of Orthopaedic Surgeons, MRI serves as the non-invasive diagnostic test of first choice for identifying suspected intra-articular knee pathology while arthroscopic surgery is the current gold standard.1 The use of MRI in assessing intra-articular knee pathology has been reviewed excessively. For all ACL tears, a recent meta-analysis showed a sensitivity and specificity of 87% (95% CI 77% to 94%) and 93% (95% CI 91 to 96), respectively.2 However, MRI diagnosis of partial tears seems challenging with sensitivity ranging from 40% to 75%, and specificity from 62% to 89%.3 Unfortunately, MRI has several cons such as high costs, limited availability and the requirement to lie down still.
Dynamic high-resolution ultrasound (US) imaging of the knee shows promising results for accurately imaging of intra-articular pathology.4 A recently published meta-analysis evaluating the diagnostic accuracy of US in detecting complete ACL tears showed a sensitivity of 90% and specificity of 97%.5 This means that for diagnosing complete ACL tears, US seems an effective test. Just like MRI, US also can detect accurately associated lesions, for example, meniscal pathology.6 Moreover, US has the potential to overcome many of the limitations of MRI: quickly executable, relatively inexpensive, easily accessible and offers the opportunity for dynamic examinations. Dynamic US enables pathology not detected in static examination, and visualises the effect of movement on function and stability of the affected knee structures. Furthermore, US has the advantage of being directly interpretable, enabling as a point-of-care test, which speeds up the diagnostic phase.
The authors of the meta-analysis evaluating the diagnostic accuracy of US in detecting ACL tears state that US is an effective test for diagnosing complete tears, but it may not be a suitable test for partial ACL tears, as 85% of them were missed on US (sensitivity of 15%).5 Besides selection and partial verification bias, they reported publication, language and retrieval bias. Another limitation of this study was the low number of partial ACL tears (n=13).5 Therefore, more diagnostic accuracy studies are needed, especially focusing on partial ACL tears, as in most of the cases conservative treatment can be started. The objective of our study was to determine the diagnostic accuracy of dynamic high-resolution US in the diagnosis of ACL tears, differentiating between partial and complete tears. Additionally, we evaluated the influence of patient characteristics on the diagnostic accuracy of US.
Methods
Study design and patients
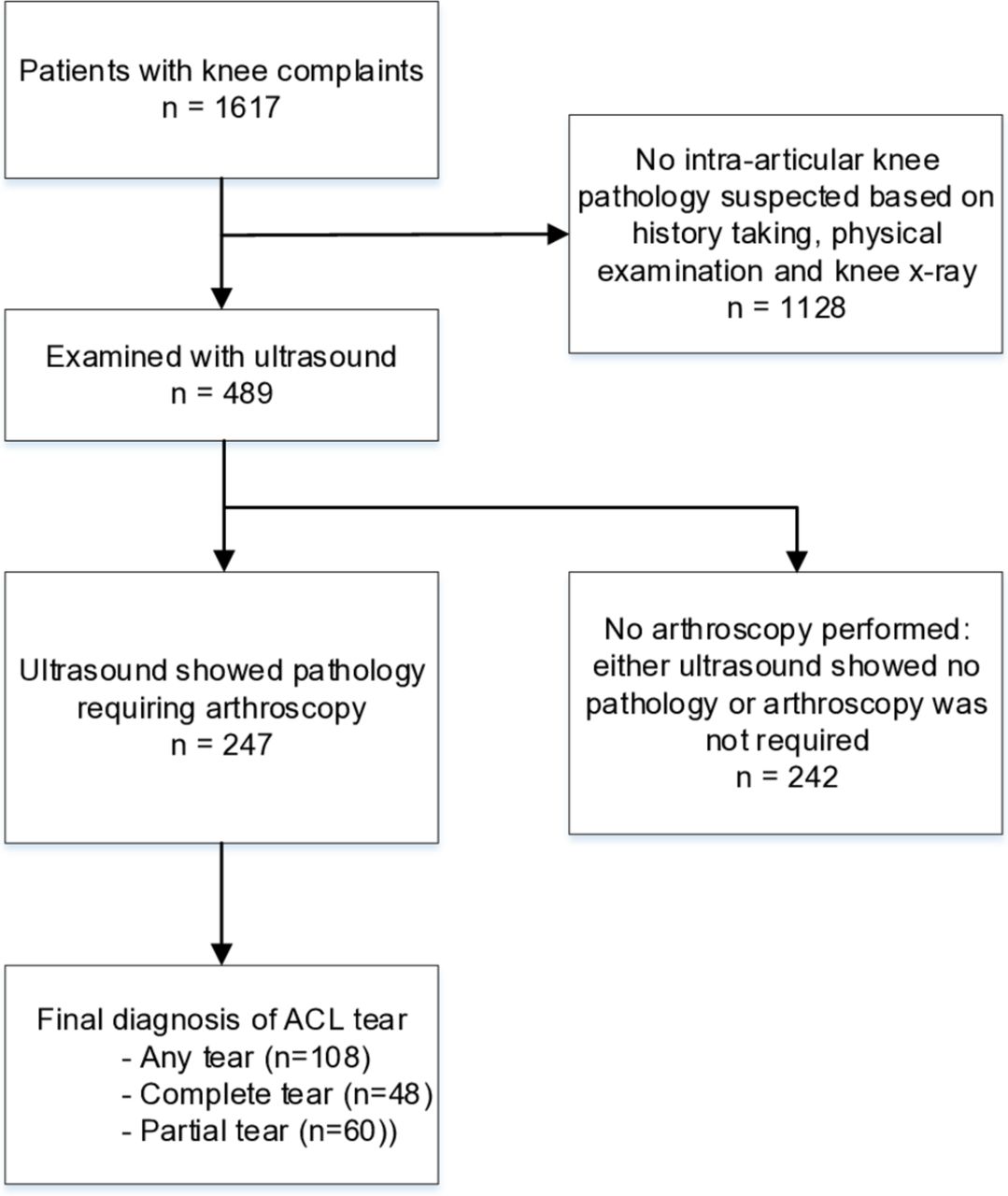
In 2016, a total of 1617 patients presenting with knee complaints (both acute and chronic) were referred to the outpatient clinic ICONE Orthopedics and Sports Traumatology. Of these 1617 patients, 489 patients were examined with US. In our retrospective observational study, patients were included if US showed intra-articular knee pathology requiring arthroscopic surgery, irrespective of the underlying pathology. In all, 49 patients who had a positive US for ACL tear did not receive arthroscopic surgery and could therefore not be included in this study. This resulted in a study population of 247 knees (figure 1 and table 1). All included patients underwent arthroscopy and at least one preoperative US. Patients who did not have any pathology detected by US or did not undergo arthroscopy afterwards for any reason were excluded from this study. ICONE evaluates patients referred by general practitioners and orthopaedic surgeons (for second or third opinions).
Patient characteristics
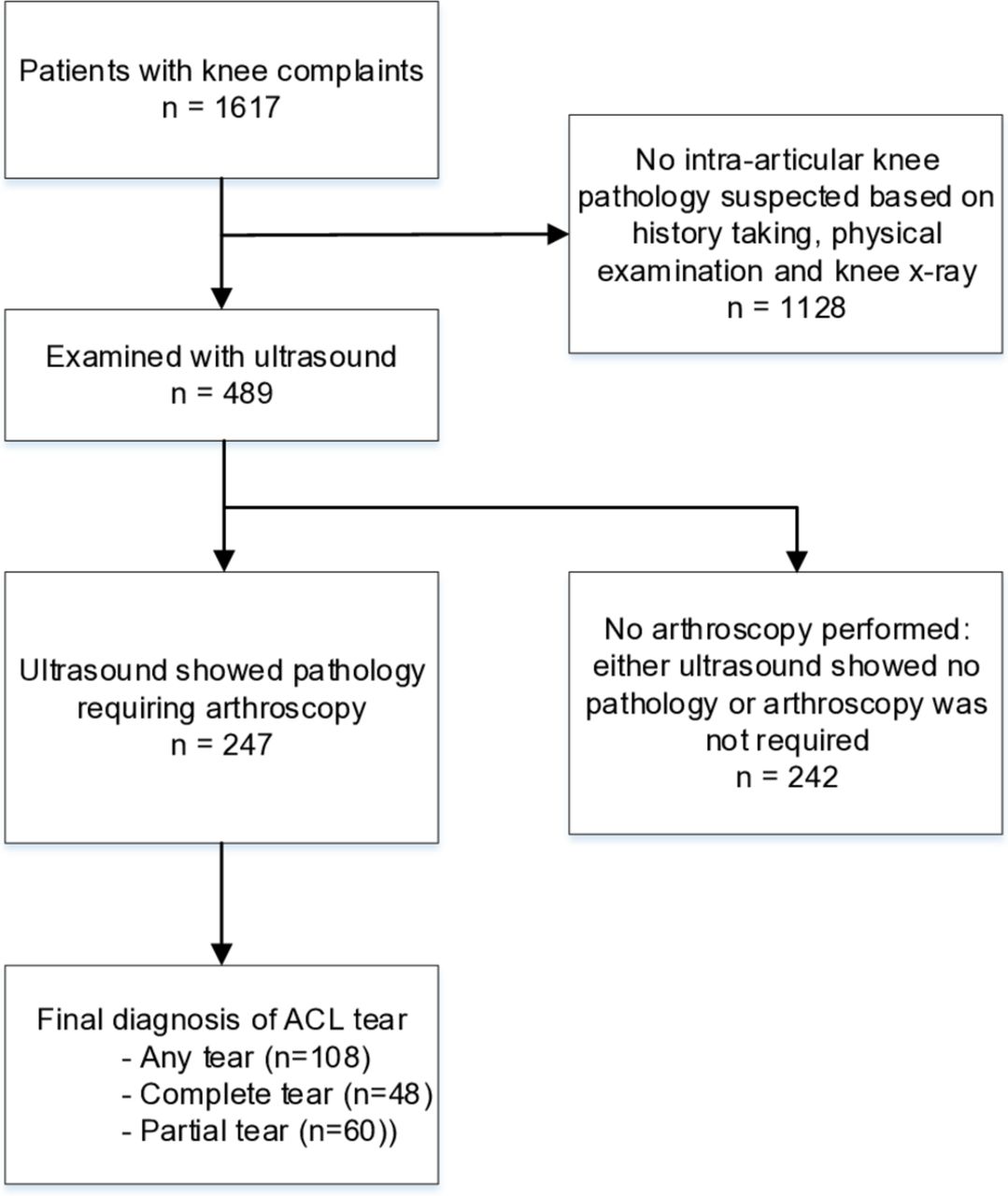
Flow of patients through the study.
All US examinations and arthroscopies were performed over a period of 1.5 years. Data were collected from the ICONE medical database and evaluated retrospectively. Two researchers independently assessed patient charts, US and arthroscopy reports, including age, origin of complaints, and each verified the data entered by the other. Disagreements were discussed and solved with consensus in our research team.
Informed consent was not required as this was a retrospective chart study and data were analysed anonymously.
US imaging
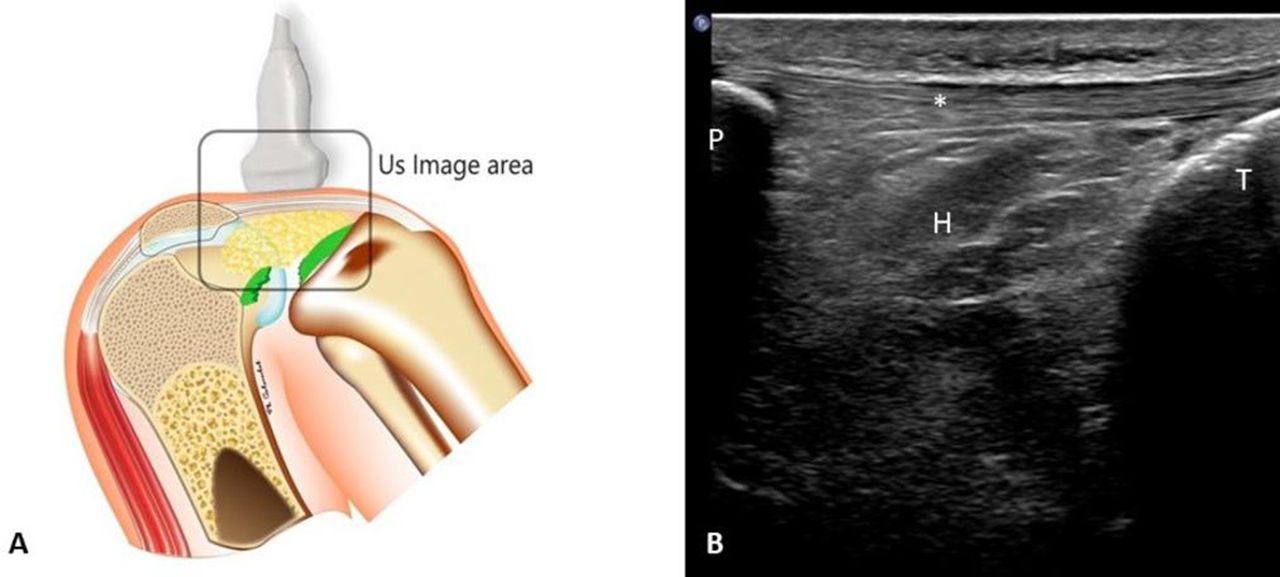
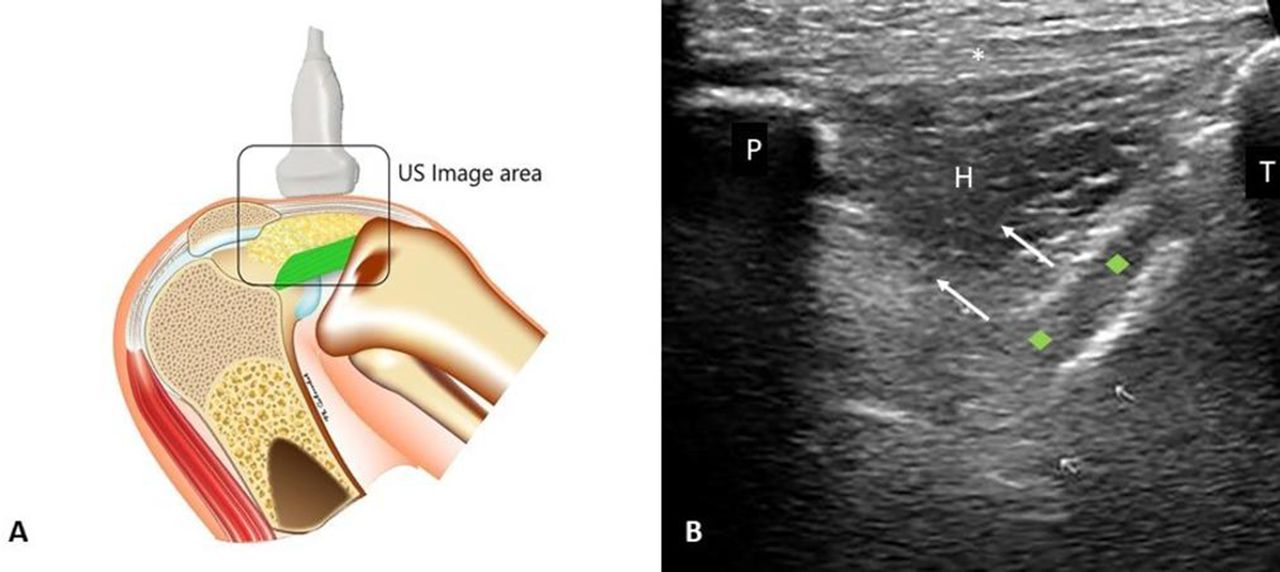
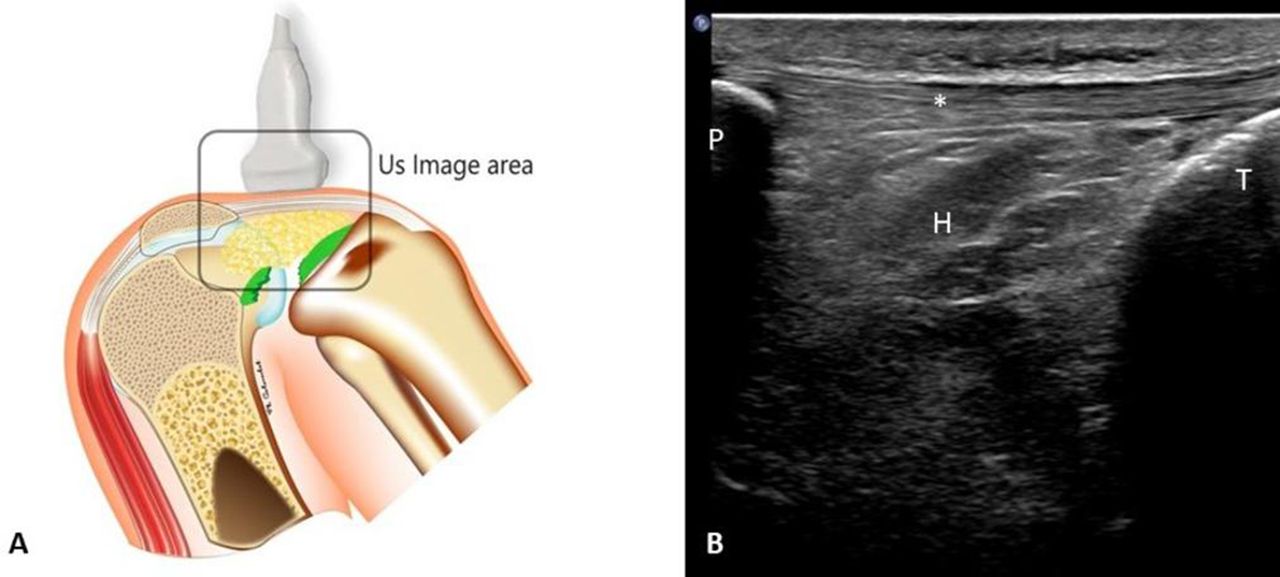
All patients obtained at least one preoperative US of the affected knee. All US examinations were performed by a single sonographer with over 10 years of experience in musculoskeletal US. The examiner was blinded to the results of history taking and physical examination. The US examinations were obtained in real time using a Philips iU22 xMatrix with a 8–12 MHz broadband linear-array transducer. All patients were examined in both supine and prone position. The US examinations took an average 10 min. The following structures were examined: ACL, both menisci, collateral ligaments, osteochondral structures and knee tendons. All structures were investigated from medial to lateral and with the probe in both horizontal and vertical position. ACL examination was performed using a combination of direct and indirect signs. To visualise the ACL in an anterior view, the patient was placed in supine position and the knee in maximal passive flexion. This position enables the examiner to evaluate the condition of the tibial part of the ACL (figures 2 and 3). The transducer was placed on the patellar tendon and the proximal tip of the transducer was slowly rotated towards the medial border of the lateral femoral condyle. In case of an unaffected ACL, the ACL moves upwards during passive extension–flexion movement of the knee, sandwiching Hoffa’s pad between the ACL and the patellar tendon (dynamic direct sign). The ACL can be visualised as a hypoechoic band with sometimes hyperechoic contours due to ageing, while Hoffa’s pad can be visualised as a hypoechoic triangular-shaped structure, which will be pushed upwards during this movement. In case of a complete ACL tear, there will be no upward movement of the ACL and Hoffa’s pad, while in case of a partial ACL tear, scar tissue can be observed, and there will be less upward movement of Hoffa’s pad. The patient was then placed in prone position with the knee flexed 15–20° to investigate two indirect signs. First, the intercondylar fossa was examined for an empty notch sign (intra-articular fluid instead of ligament, static indirect sign),7–9 which is present in the acute phase of an ACL tear. Second, with a qualitative observation, dynamic rotation was performed to investigate the stability of the posteromedial tibia (dynamic indirect sign). In case of an unaffected ACL, there will be little translation of the medial tibia plateau, whereas in case of a complete ACL tear, a clear translation will be observed. In case of a partial ACL tear, there will be more translation of the tibia compared with the unaffected knee. Observed pathology was recorded by the same examiner with a mean number of 8–10 images per patient. A differentiation was made between partial and complete ACL tears. In this study, we scored subtotal tears as being partial tears. Subtotal tears are considered partial tears in which only few ligament fibres are still intact. These fibres will still tighten during the passive movements in dynamic US.
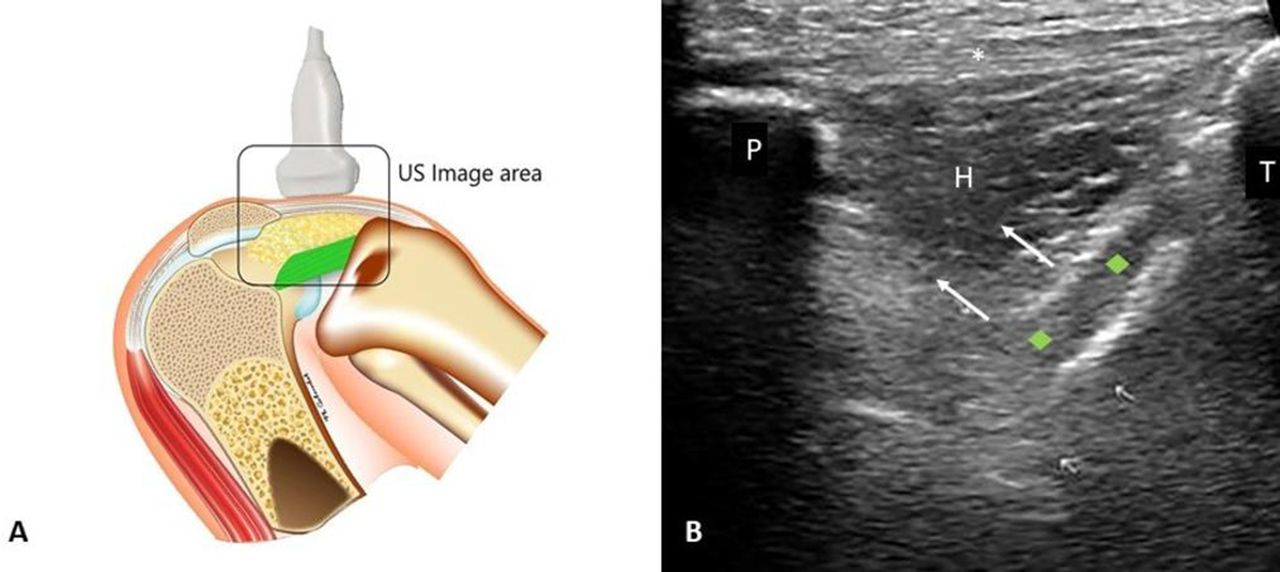
Anatomic drawing of the knee in full flexion (patient in supine position with hip in flexion) with normal ACL and US transducer position (A) and corresponding US image (longitudinal view) (B). P indicates patella; T, tibia; H, Hoffa; * patellar tendon; the green rhombus indicates the ACL between hyperechoic white lines; arrow indicates direction of movement of the ACL and Hoffa’s pad during knee flexion. ACL, anterior cruciate ligament; US, ultrasound.
{kind=link}
{kind=link}
{kind=link}
Anatomic drawing of the knee in full flexion (patient in supine position with hip in flexion) with complete ACL tear and US transducer position (A) and corresponding US image (longitudinal view) (B). Note that the ACL is not visible. P indicates patella; T, tibia; H, Hoffa; * patellar tendon. ACL, anterior cruciate ligament; US, ultrasound.
Arthroscopic surgery
Arthroscopic surgery was used as reference test. All procedures were performed by one of three experienced orthopaedic surgeons, who were unblinded to the US results. The procedure was performed under local anaesthetics and according to ICONE protocol. All observed pathology was recorded. In this study, we focused on the assessment of partial and complete ACL tears. Patients with no ACL tear at US assessment but with other intra-articular knee pathology requiring arthroscopy (eg, meniscal tear) were also assessed to evaluate possibly missed ACL tears in the preoperative US.
Statistical analysis
Sample size was calculated on an expected prevalence of 40%–50% for ACL tears,10 and a sensitivity of 90%.5 Based on a 95% CI and a precision of 5%, this resulted in a required sample size of 225–275.11
Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) and diagnostic OR (DOR) with 95% CIs for partial, complete and any ACL tear were calculated. Logistic regression analyses was performed to determine the association of age and previous knee surgery, and expressed as adjusted DOR. All data were analysed using SPSS V.23.0 (International Business Machines Corp).
Results
Of the included 247 knees, 120 knees showed evidence of ACL tears during US examination. Of these knees, 60 (50%) were described as partial and 59 (49.2%) as complete tears. In one patient, the extent of the tear was not described in the US report and could not be retrieved from the saved images. Therefore, this knee was excluded from the analysis for partial and complete tears (n=246), but included for analysing any tear (n=247). At arthroscopic surgery, 108 ACL tears were found, of which 60 (55.6%) were partial, and 48 (44.4%) were complete tears.
Table 2 shows the results of the US examination and corresponding arthroscopic findings. Sensitivity of US in the detection of complete ACL tears was 79% (37 of 48; 95% CI 64% to 89%), specificity of 89% (177 of 198; 95% CI 84% to 93%), PPV of 63% (37 of 59; 95% CI 49% to 75%), NPV of 95% (177 of 187; 95% CI 90% to 97%) and DOR 29.8 (95% CI 13.0 to 68.1). Partial ACL tears were depicted with a sensitivity of 52% (31 of 60; 95% CI 39 to 65), specificity 85% (157 of 185; 95% CI 78% to 89%), PPV 52% (31 of 60; 95% CI 39% to 65%), NPV 84% (157 of 186; 95% CI 78% to 89%) and DOR 5.8 (95% CI 3.0 to 11.0). US showed a sensitivity of 88% (95 of 108; 95% CI 80% to 93%) in detecting any ACL tear, specificity 82% (114 of 139; 95% CI 74% to 88%), PPV 79% (95 of 120; 95% CI 71% to 86%), NPV 90% (114 of 127; 95% CI 83% to 94%) and DOR of 33.3 (95% CI 16.2 to 68.7).
2×2 cross tables US compared with arthroscopy for ACL tears
Discussion
In this retrospective observational study, we assessed the diagnostic accuracy of dynamic US in diagnosing partial and complete ACL tears in the clinical setting where US is used as an initial diagnostic screening test. We compared US results with arthroscopic surgery findings. To our knowledge, this is the first study differentiating between partial and complete ACL tears. Our study shows that US is accurate in diagnosing any ACL tear. However, we found a higher sensitivity for complete ACL tears compared with partial ACL tears (79% vs 52%).
The recently published meta-analysis assessing the accuracy of US in diagnosing ACL tears included a total of four studies involving 246 patients, of whom 13 had a partial ACL tear,5 whereas our sample size was 247, of whom 60 had a partial tear. In comparison to this study, we found lower sensitivity and specificity for complete tears (79% vs 90% and 89 vs 97%, respectively). However, we observed a higher sensitivity of partial tears (52 vs 15%).5 This finding can be explained by the difference in study populations. In the populations incorporated in the meta-analysis, an ACL tear was highly suspected. This makes these studies susceptible to selection bias and therefore may lead to overestimation of the results. We also included patients who were clinically not suspected for having ACL tears because of other pathology requiring arthroscopy (eg, meniscal tear), making our study less prone for selection bias. A recent validity study, including three static indirect US signs, the empty notch sign, the posterior cruciate ligament wave sign and capsular protrusion sign, showed that if two or three signs were positive, the sensitivity for any ACL tear was 87% and specificity was 88%. In this study, no differentiation was made between partial and complete tears.12 Another important finding of our study is that the diagnostic accuracy of US approaches MRI accuracy in diagnosing any ACL tears, and that US accuracy for diagnosing partial ACL tears is in the range of accuracy results reported for MRI.3 MRI diagnosis of a partial tear can be difficult because various tear patterns may be observed. One study showed that many partial ACL tears show MRI features that are indistinguishable from complete ACL tears or even normal ACL.13
Our data show half of the ACL tears to be partial, and this is not in line with previous studies, that show a prevalence of 5%–28%.3 14 This can be explained in light of the above; the way MRI report ACL tears, some centres fail to differentiate between partial and complete tears resulting in under-reporting of partial ACL tears. Moreover, in most studies, the focus is on complete ACL tears.5
We found a number of subtotal ACL tears in the false-positive group of complete ACL tears: 8 out of 22 patients turned out to have a subtotal tear requiring arthroscopic reconstruction. This indicates that it may be hard to differentiate between subtotal ACL tears and complete tears using US. In the case of partial ACL tears, we found that in five out of nine patients who had an actual complete tear in arthroscopy, US examination showed evidence of a subtotal ACL tear rather than a partial tear. This further supports the suggestion of US having difficulties in discriminating subtotal from complete ACL tears. This might be due to the fact that the few remaining fibres do still contract during passive movement used in dynamic US, making these tears appear as partial. These few fibres may be cut through while introducing the scope during arthroscopy, thereby creating a complete ACL tear. As previously described, we considered all subtotal tears as being partial in this study. If we chose to consider subtotal tears as complete tears, this would have improved sensitivity from 79% to 82%, and specificity from 89% to 93%. From a clinical perspective, this seems defensible as most patients with a subtotal tear experience knee instability like in a complete tear, requiring an ACL reconstruction.
Our study had several limitations that may influence the results found. First, this study had a retrospective observational design, making it subject to confounding and missing data, and making it impossible to blind the orthopaedic surgeon. However, the situation as set in this study reflects daily clinical practice: imaging results are rarely used in isolation, and are normally used in a diagnostic pathway. Orthopaedic surgeons do make their decision whether or not to operate on complimentary diagnostic imaging (eg, US or MRI), and thus are not blind to the outcome of these imaging procedures. Second, we could not asses the outcome in patients in which US did not show any intra-articular pathology requiring arthroscopy, leading to partial verification bias. However, verification bias is only partial since we did include patients with negative US for ACL tears, but who had other intra-articular pathology requiring arthroscopic surgery. In this way, we were able to assess the negative US outcome for ACL. The use of only a single sonographer could be both a pro and a con of our study. The outcome and diagnostic accuracy of US is prone to the experience of the examiner, in particular for the qualitative assessment of the dynamic signs. In our study, the sonographer had over 10 years of experience in musculoskeletal US. Since we did only use a single examiner, inter-observer reliability could not be calculated. Therefore, we cannot be certain the results obtained in this study are applicable to US made by less experienced sonographers. However, one study showed that after a short period of training a high level of accuracy can be reached.15
Considering the availability, and relatively fast learning curve, US seems an ideal diagnostic screening test for ACL tears. Given the excellent NPV for complete ACL tears, we believe a negative US outcome justifies to refrain from MRI and arthroscopic surgery. However, positive US for ACL tears should be interpreted with caution. Yet, in daily practice, also age and clinical presentation are taken into account deciding whether or not to perform arthroscopic surgery. Our study and clinical experience show that even partial tears, especially subtotal tears, may also require ACL reconstruction. The dynamic nature of the US imaging enables us to distinguish between partial and subtotal tears: the empty notch sign is only seen in subtotal and complete tears, while instability of the posteromedial tibia is clearer in subtotal tears. This finding is of influence in the decision for treatment (either conservative or operative) especially in the sport active younger patients. Furthermore, one should also look at other knee pathology depicted at US, such as meniscal tears, medial collateral ligament tears and Segond fractures. Considering the mechanical pathway occurring while tearing these structures, one could also expect the ACL to be affected.16 17 Moreover, the advantage of point-of-care US is that it can be utilised at the time of the patient’s clinical evaluation, so no additional appointments have to be scheduled. This speeds up the diagnostic phase.
Since our study had a retrospective design, future studies should use a prospective design with a period of patient follow-up. This follow-up period enables the clinical course of patients who had an initial negative US for ACL tears, as most of these patients will initially not be operated on. We used a combination of one direct and three indirect signs to assess the integrity of the ACL. Other indirect signs have been described, for example, capsular protrusion and posterior cruciate ligament wave sign, and anterior tibial translation.12 15 Future studies should also include an analysis of several combinations of signs, enabling the most accurate combination. Adding physical examination signs, for example, anterior tibial translation, is likely to improve accuracy. This latter best reflects clinical practice as diagnosis relies on a combination of all signs. We qualitatively assessed the tibial translation, where a quantitative approach seems more valid. However, with the current US software, this is not possible.
Conclusion
We concluded that the excellent NPV for complete ACL tears indicates that dynamic US imaging can be used as an initial imaging point-of-care test. However, the clinical presentation should be taken into account, especially in case of subtotal tears. Whereas it seems relatively easy to differentiate between (small) partial ACL tears, complete ACL tears and no tears, it seems to be difficult to differentiate subtotal tears from complete tears. However, literature shows that MRI seems not to be superior. Further research is required to establish the most accurate combination of signs, where dynamic signs should preferably based on quantitative measurements.
Acknowledgments
We thank Philippe Colombet for the drawings of the knee.
Footnotes
MB and DH are joint first authors.
Contributors RO, GD, SK, and BK originated the idea for the study. MB and DH carried out the data collection and statistical analysis. All authors played a role in the interpretation of data. MB and DH wrote the first draft of the manuscript. BK and SK performed arthroscopy and ultrasound examinations, respectively. All authors critically revised the manuscript for important intellectual content, and approved the final manuscript. RO is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was given by the Medical Ethical Committee of Maastricht University Medical Centre (METC 16-4-272)
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.