Article Text

Abstract
Objectives Evaluate if socioecological and biological factors, at the age of 8 years, are associated with lower level of physical activity (PA) 2 years later.
Method In a study cohort of 199 children aged 7.8±0.6 years, we used questionnaires and physical measurements to evaluate biological (eg, sex), social (eg, parental PA) and environmental (eg, school settings) factors. Objective PA was measured 2 years later with accelerometers. General PA (GPA) was defined as mean counts per minute (cpm) and moderate to vigorous PA (MVPA) as min/day >3500 cpm. We used analysis of covariance to evaluate if socioecological factors at age 8 are associated with level of PA 2 years later.
Results Daily GPA was 690.5±216.6 cpm and the children spent 40.9±18.3 min on MVPA. Female sex is associated with −131.1 (−183.4, –78.7) cpm GPA, each 10 cm shorter body height with −48.7 (−94.8, –26.5), each unit higher body mass index (BMI) with −26.0 (−37.5, –14.5) and allocation to 60 min school PA/week with −73.8 (−131.5, –16.2) compared with allocation to 200 min school PA/week. Female sex is associated with −10.3 (−14.8, –5.7) min of MVPA and each unit higher BMI with −1.9 (−2.9, –0.9) min.
Conclusion Female sex, shorter body height and higher BMI are at age 8 years associated with lower level of PA 2 years later. It appears possible to increase PA by daily school PA.
Trial registration number NCT00633828.
- children's health and exercise
- sedentary
- physical activity promotion in primary care
- physical activity
- children
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- children's health and exercise
- sedentary
- physical activity promotion in primary care
- physical activity
- children
Introduction
Physical inactivity is a risk factor for several diseases including stroke,1 depression,2 hypertension1 and type II diabetes.3 As physical activity (PA) levels track from childhood to adulthood,4 beneficial PA habits should be implemented already in early years of life. Currently, only one-fifth of children globally meet the WHO’s recommendation of minimum 60 min of PA/day,5 and the gap between the most and least physically active children has widened during the recent decades.6
Cross-sectional studies have proposed several socioecological factors that are associated with childhood PA.7–10 The next step is to test these findings with higher level of evidence, to answer if socioecological and biological factors also are associated with future PA levels. This study aims to evaluate if (1) socioecological and biological factors and (2) ecological factors (ie, daily school-based PA) are associated with lower PA levels in 8-year-old children 2 years later.
Materials and methods
The paediatric osteoporosis prevention study
This study uses baseline (collected in 1999–2000) and 2-year data (collected in 2001–2002) from the paediatric osteoporosis prevention (POP) study, a prospective controlled school PA intervention study conducted in four schools in the city of Malmö, Sweden.11–15 After the baseline exam, one school increased duration of school PA from the Swedish standard of 60 min/week to 200 min/week (40 min/school-day). The global recommendations are minimum 60 min PA/day but in our study we use 40 min/day as the current recommendations were not established when our study started in year 1999–2000. The three neighbouring control schools continued with 60 min/week. The children were allocated to each school according to their residential address and all school PA was mandatory. The additional school PA required no extra resources as it included ordinary school curriculum activities and were supervised by the regular teachers.
Study participants
All 564 children in first or second grade in the four schools were invited to participate in the POP study. Out of them, 343 (61%) children aged mean 7.8±0.6 years agreed and participated at baseline. We excluded two children due to diseases affecting their ability to be physically active. At the baseline examination, the children underwent anthropometric measurements and answered a non-validated questionnaire that was not pilot tested. Two years after baseline, at mean age 9.8±0.6 years, 250 children (44% of all invited children) attended the 2-year examination that included an accelerometer-based measurement.
Socioecological factors evaluated at baseline
Data on socioecological factors were collected at baseline and classified into biological, social and environmental domains.16 We selected factors that previously have been found to be associated with childhood PA.7–10 Biological factors comprised sex, age and relative age (born between 1 January and 30 June or 1 July and 31 December), body height (measured with a Harpenden Stadiometer; Holtain, Pembrokeshire, UK) and weight (measured with an HL 120 electric scale; Avery Berkel, West Midlands, UK). Body mass index (BMI) was calculated as weight/height2 (kg/m2). Social factors were evaluated with a non-validated questionnaire7 17–19 that the children answered together with their parents (online supplementary appendix 1). One part of the questionnaire targeted the children’s parents and was answered by them. In the environmental domain, we defined if the children were allocated to the intervention school (200 min school PA/week) or to any of the three control schools (60 min school PA/week). All children in this study lived within the same Swedish middle-class geographical area and we could therefore not distinguish or include other environmental factors of interest (such as the built environment, access to green parks and living in urban/suburban neighbourhoods9).
Supplemental material
Objectively measured PA 2 years after baseline
The endpoint variables were general PA (GPA; counts per min (cpm)) and moderate to vigorous PA (MVPA; min/day), measured 2 years after baseline by the MTI (Manufacturing Technology, Fort Walton Beach, FL, USA) accelerometer model 7164. Based on previous studies,20 21 we defined GPA as mean cpm per valid minute of recording and MVPA as minute spent >3500 cpm.
The accelerometer was worn with a belt around the waist and measured vertical acceleration in cpm. The children were instructed to wear the accelerometer for 4 days during all kinds of activities, except water activities as the equipment was not water resistant. The accelerometers were programmed to start measuring during the morning of the first day and continue recording counts during 4 days in 10 s epochs. Missing data, defined as continuous sequences of more than 60 serial epochs (ie, 10 min) of 0 cpm, were deleted. To be included in the analysis, the children had to wear the accelerometer during a minimum of 3 days and at least during 8 hours/day. Forty-five children (20%) wore the accelerometer for 3 days and 184 (80%) during 4 days. Before recording, all accelerometers were calibrated to a standardised vertical movement.
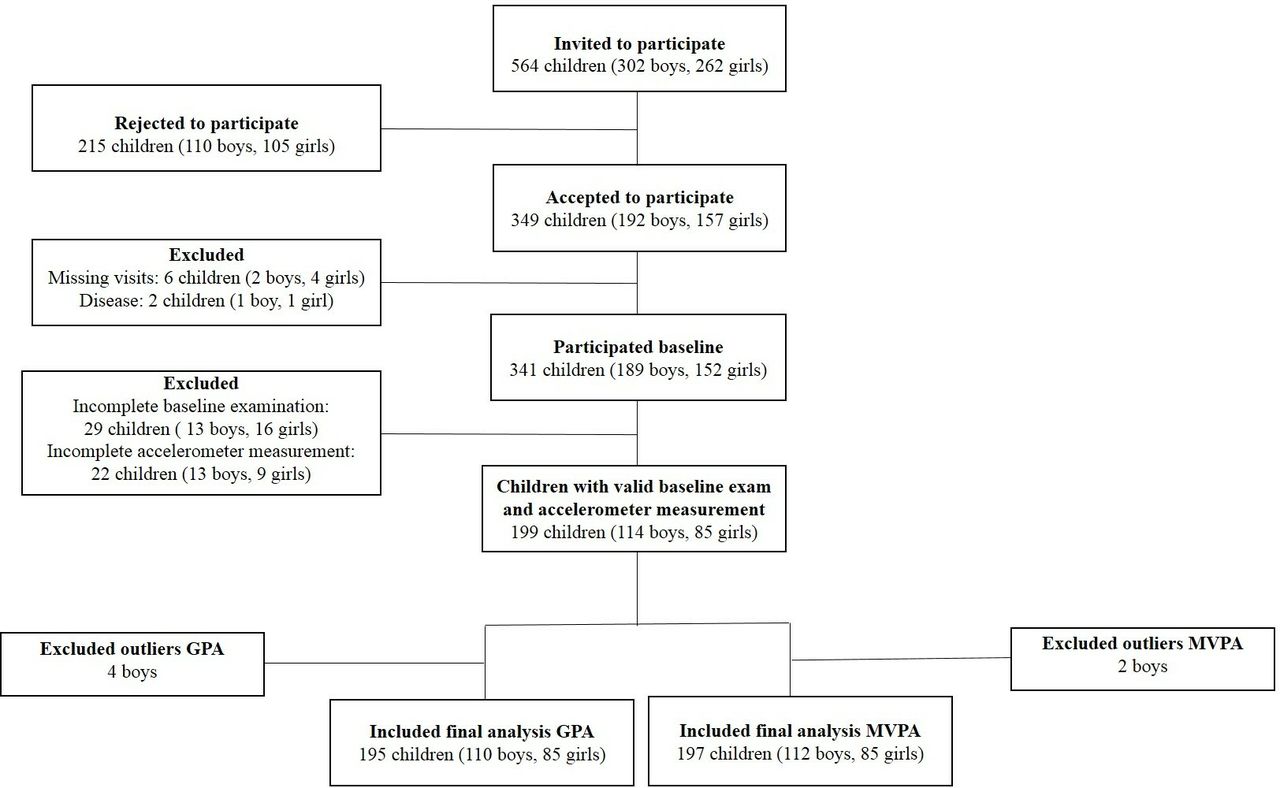
To be included in the final analysis, the children had to have a complete baseline examination and a valid accelerometer measurement. One-hundred and ninety-nine children met these inclusion criteria. From these 199 children we excluded four outlier values in the accelerometer measurements for GPA and two for MVPA, resulting in 195 children in the GPA analysis and 197 in the MVPA analyses (figure 1).
{kind=link}
Flow chart of the study population. GPA, general physical activity; MVPA, moderate to vigorous physical activity.
Statistics
For statistical analysis, we used IBM SPSS V.25. We presented descriptive statistics as numbers (n), proportions (%) or means±SDs and inferential statistics as means with 95% CIs. We plotted the residuals for all PA outcomes as boxplots in order to define outlier values (defined as lower than the first quartile–1.5*IQR or values higher than the third quartile+1.5*IQR) and to check for normality. We used analysis of covariance to determine any association between the included factors, GPA and MVPA, unadjusted and adjusted for all factors in the model.
In summary, the final model was adjusted for biological factors of sex, age, relative age, body height and BMI, social factors of the children’s screen time activity, if the children partake in organised leisure time PA or not, if the children have any sibling(s) active in a sport association or not (the no category also includes those without sibling(s)), duration of organised parental PA, having minimum one parent who agreed to the statement ‘in our family it is important to exercise’ or having no parent who agreed to this statement, and if the children had minimum one parent with postsecondary degree compared with having no parent with this educational level, and environmental factors including being allocated (then followed by) 60 min school PA/week or to 200 min school PA/week. At baseline, the age range of the children was 5.9–9.0 years, but this did not affect the relative age evaluation as the model also was adjusted for chronological age. Accelerometer measurements were undertaken in adjunct to the 2-year examination between August and December and we therefore also adjusted the model for months between the baseline exam and the 2-year follow-up exam.
Results
Descriptive characteristics of the included children are presented in table 1. Mean daily GPA was 690.5±216.6 cpm (boys: 747.7±236.8, girls: 613.8±157.5) and the children spent mean 40.9±18.3 min/day on MVPA (boys: 45.5±19.8, girls: 34.6±13.8).
Descriptive characteristics of the 199 study participants
General physical activity
The included factors explained 29% of the variance in GPA. Female sex was associated with −131.1 (−183.4, –78.7) GPA compared with male sex, each 10 cm shorter body height with −48.7 (−94.8, –26.5), each unit higher BMI with −26.0 (−37.5, –14.5) and allocation to 60 min school PA/week with −73.8 (−131.5, –16.2) compared with allocation to 200 min school PA/week (table 2).
Descriptive characteristics, collected at mean 8 years of age, and association to general physical activity (GPA) 2 years later
Moderate to vigorous physical activity
The included factors explained 25% of the variance in MVPA. Female sex was associated with −10.3 (−14.8, –5.7) min/day of MVPA compared with male sex, and each unit lower BMI with −1.9 (−2.9, –0.9) (table 3).
Descriptive characteristics, collected at mean 8 years, and association to moderate to vigorous physical activity (MVPA) 2 years later
Discussion
In this prospective controlled study, we found that in 8-year-old children, female sex, shorter body height and higher BMI are factors independently associated with lower PA levels 2 years later. As children’s sex, body height and BMI are already evaluated in the compulsory school health examinations, future studies ought to evaluate if these factors could be used as screening tools, on a group level, to identify children at risk of developing lower future PA levels. If so, preventive interventions could possibly be initiated timely, already before inactivity occurs. Our findings also infer that daily school PA is an effective strategy to promote childhood PA. As the daily school PA required no additional costs, it appears probable that the programme could be implement on a national level.
PA levels usually decline in adolescence and so more in girls than boys, thus resulting in significant sex differences in PA levels.22 23 Interventional studies often target adolescent girls to counteract this decline,24–26 but the referred studies have only shown weak effects. In line with another report27 our study infers that sex differences in PA develop before adolescence. We therefore speculate that PA interventions should be initiated at younger ages than in cited studies24–26 to prevent this decline.
Previous studies have found various results regarding PA and its effect on BMI. One review found only weak to modest relationships between PA and overweight/obesity28 whereas others suggest that PA is a modifiable key component in fighting obesity in school-age children.29 Our study supports an association between BMI and future PA levels, but we cannot state that higher BMI leads to lower PA levels or vice versa, only that there is an association.
Shorter body height was also associated with lower future PA levels. An explanation could be that shorter children may have disadvantage in sport performance compared with taller children,30 and therefore tend not to perform PA. Commonly, there is an association between being born early on the year and taller body height/early maturation,31 but we could not identify a true relative age effect (ie, an association between being born early or late on the year and PA).32–34 To promote shorter children to exercise, it would be interesting to group children into chronological age and according to height.
In our study, screen time activity was not associated with lower future PA levels. The level of screen time in our study cohort was relatively low (approximately mean 12 hours/week) compared with another study that examined screen time among almost 6000 children around the world which found that mean 10-year-old children spend almost 9 hours/day on sedentary activities.35 This discrepancy may have been due to that rapid increase of technical devices and the use of smartphones during the last decades36 compared with 1999–2000 when the POP study was started. We therefore cannot exclude that this association exists among schoolchildren in the modern society, a question that future studies ought to evaluate.
Study strengths include the prospective controlled study design, the use of objectively measured PA and a previous dropout analysis that found anthropometrics in the children who attended the baseline exam similar to those who did not,17 which reduces the risk of bias. Study limitations include the short period of accelerometer measurements37 and that we may have underestimated PA during activities with low vertical movement and water activities. As all children lived within a similar Swedish middle-class geographical area, the generalisability is limited to these settings. In addition, we can only make inferences with respect to association, not causality. For example, the causality could be that lower level of PA leads to higher BMI and not vice versa. The small sample size is also a weakness.
In summary, in 8-year-old children, simple variables of sex, height and BMI are associated with lower future PA levels. In addition, daily school PA appears to promote childhood PA. Future studies should evaluate if these factors could be used to predict lower levels of PA and if they can be used to identify children suitable for preventive interventions. It should also be tested if our inferences apply in other settings.
References
Footnotes
Contributors AL is the corresponding author of the study; provided extensive work on cleaning, analysing and interpreting the data; drafted and revised the paper. BER contributed to interpretation of data for the work and revised it critically and provided important intellectual content; provided final approval of the version to be published. JAN provided substantial contributions to the statistical design and analysis and revised the work and provided valuable, intellectual, important content; provided final approval of the version to be published. MD collected accelerometer data and contributed to the work by providing interpretation to the work and revising it for the final approval. MKK was responsible for collection of data and substantial contributions to the analysis and interpretation of the data of the work and revising the draft several times. All authors have given an agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Financial support was received from the Swedish Research Council for Sport Science.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study was approved by the Ethics Committee of Lund University, Sweden (LU 453-98; 1998-09-15), registered as clinical trial (ClinicalTrials.gov) and conducted according to the Declaration of Helsinki. Written consent was obtained from the parents of all participating children.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.