Article Text

Abstract
Background The primary aim of the present study was to investigate the effects of aerobic interval training (AIT) versus moderate intensity continuous exercise (MICE) on aerobic exercise capacity (V̇O2peak), in women only, with coronary artery disease (CAD) and who were referred to a large, 24-week outpatient cardiac rehabilitation (CR) programme. Secondary objectives included comparing the effects of AIT versus MICE on cognition, cardiovascular risk profile, adherence and quality of life before and after the 24-week CR programme.
Methods Thirty-one postmenopausal women with CAD (left ventricular ejection fraction >35%; 68.2±9.2 years of age; V̇O2peak: 19.1±3.5 mL kg-1 min-1) were randomised to 24 weeks of usual care MICE (60%–80% of V̇O2peak, five times per week) or AIT (four 4-min intervals at 90%–95% of peak heart rate, three times per week+two times per week usual care MICE). Differences between and within groups were assessed using independent samples t-tests and paired samples t-tests, respectively. Treatment effect analysis of AIT on V̇O2peak and secondary outcomes was determined using analysis of covariance with baseline values as covariates.
Results A randomised controlled trial study design was unfeasible in this female CAD population. Unanticipated challenges in recruitment availability and eligibility, in combination with a 59% and 50% attrition rate in the AIT and MICE group, respectively, rendered this study underpowered to detect differences between groups. The per protocol treatment effect analysis, however, unveiled a 0.95 mL kg-1 min-1 improvement in V̇O2peak in response to AIT over MICE (p<0.001).
Conclusions Further research is necessary to elucidate the patient profile and circumstances under which the potential for the implementation of AIT may be individualised, and offered in clinical practice.
Trial registration NCT02966158.
- coronary artery disease
- interval training
- women
- aerobic exercise capacity
- cardiac rehabilitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
A randomised controlled trial study design investigating the effects of aerobic interval training (AIT) versus moderate-intensity continuous exercise (MICE) in an exclusively female population with coronary artery disease (CAD) poses great challenges in feasibility.
AIT performed as consecutive 4-min intervals at an intensity of 90–95% of peak heart rate was both daunting and unfeasible for the majority of female CAD patients.
There was a significant per protocol treatment effect of 0.95 mL kg-1 min-1 favouring AIT over MICE.
The implementation of AIT into clinical practice is complex for female CAD patients and warrants further investigation.
Background
Cardiovascular disease (CVD) is pervasive around the world and persists as the number one killer among non-communicable chronic diseases, and it is responsible for claiming the lives of an estimated 17.9 million people every year.1 The common misconception that CVD predominantly affects men is quelled with recent statistics from the WHO, indicating that 1.1 million more older women (over the age of 60 years) die from CVD each year compared with older men.2 Exercise-based cardiac rehabilitation (CR) programme have been shown to be an effective intervention for the reduction of cardiovascular and all-cause mortality in patients with coronary artery disease (CAD).3 In the current CR setting, the standard of care for best practice involves prescribing moderate intensity continuous exercise (MICE) at a frequency of three to five times per week, traditionally in the form of walking or cycling, at an intensity of 40%–80% of maximal aerobic exercise capacity (V̇O2peak) for approximately 30–60 min,4 yielding an average improvement of 20% in V̇O2peak.3 Recently, there has been much debate and controversy surrounding the optimal exercise regimen that will elicit the most beneficial health outcomes in CAD patients, with the emergence of aerobic interval training (AIT).
The concept of AIT is not a novel one, and in fact, it was a form of exercise training that was methodically imposed on high performance or elite athletes, in order to maximise athletic performance almost eight decades ago.5 This training involves performing shorter bouts of exercise, generally one to 4 min in duration, near maximal intensity, interspersed with active or passive recovery periods. In the CAD population, the AIT intervention group in several studies6–9 experienced greater improvements in V̇O2peak, and a meta-analysis quantified this improvement to be approximately 1.5–2 mL kg-1 min-1 greater than the MICE (control) group.10 These results are compelling, particularly in the context of a potential 10%–25% reduction in cardiovascular mortality risk11–13 above and beyond what would have been conferred by standard care MICE prescription. However, it is important to recognise that the findings supporting the feasibility and benefits of AIT may not be generalisable to the majority of heterogeneous CAD patients in a standard CR setting.
Perhaps the most important limitation that has jeopardised the generalisability of the potential superiority of AIT over MICE in improving V̇O2peak in CAD patients is the gross under-representation of women included in these studies, or their outright exclusion altogether,8 compared with men.9 14 In light of evidence suggesting that women experience sex bias in referral to outpatient CR programme,15 and that they are 36% less likely to enrol in CR compared with men,16 women should be represented in studies investigating the optimisation of exercise-based CR programme to maximise the potential gains in aerobic exercise capacity.10 This representation may be integral to improving not only patient outcomes, but to the continual and evolving process of determining best practice and standard of care.
Therefore, the primary aim of the present study was to investigate the effects of AIT versus MICE on V̇O2peak, in women only, with CAD and who were referred to a large, 24-week outpatient CR programme. Secondary objectives included comparing the effects of AIT versus MICE on cognition, CV risk profile, adherence, and quality of life before and after the 24-week CR programme.
Methods
Study design
This study is the first RCT to investigate the effects of AIT versus MICE on aerobic exercise capacity in exclusively women with CAD, who were referred to the 24-week outpatient CR programme at the Toronto Rehabilitation Institute (TRI)-Cardiac Rumsey Centre.
Participants
Thirty-one female CAD patients (≥50 years of age) referred for CR were enrolled in this RCT. Inclusion criteria were: (1) postmenopausal women with documented CAD, (2) in sinus rhythm, (3) left ventricular ejection fraction >35%, (4) >3 weeks postmyocardial infarction or percutaneous coronary intervention, (5) >8 weeks postcoronary artery bypass graft (post-CABG) and (6) ability to provide written and informed consent. Patients were excluded from the study if they presented with (1) any major musculoskeletal, pulmonary, or psychiatric comorbidity that precluded participation in aerobic or resistance exercise training; and/or (2) Canadian Cardiovascular Society contraindications on initial intake cardiopulmonary exercise assessment (CPA), which include unstable class II-IV angina, uncontrolled significant arrhythmia, or >1 mm horizontal or down sloping ST-segment depression. Once written and informed consent was obtained, patients were randomised 1:1 to a 24-week programme of AIT or MICE, using an eight-block randomisation allocation that a third party, independent researcher with no affiliations to the study generated using a computerised random number generator on ‘Random.org’ (https://www.random.org). The authors of this study were blinded to the details of randomisation allocation until study completion, and were blinded to group allocation until after the collection of baseline data. Study participants were also blinded to group allocation until after the collection of baseline data was completed.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy. Patients were; however, invited to focus group sessions to share their experiences with the study intervention, in order to inform future research studies and clinical practice in this domain.
Exercise training
Both the MICE and AIT arms of the study consisted of patients attending one, supervised exercise session per week at the TRI-Rumsey Centre, and they aimed to perform four additional unsupervised home-exercise sessions per week for a total of five exercise sessions per week as the goal. The MICE group (control group) performed usual care CR, which involved sessions of either walking or jogging on the track or treadmill for approximately 30–40 min, performed at an intensity of 60%–80% of V̇O2peak, in addition to a warm-up and cool down period, as described previously by our group.17
AIT intervention
The AIT group began with 6 weeks, ‘run-in’ period where patients performed current usual care CR programming, which was identical to the MICE group. In the seventh week of the study intervention, patients began performing AIT 3 days per week, with one of those AIT exercise sessions occurring at the Rumsey Centre under supervision, and two sessions per week of MICE, which again consisted of the approximate 30–40 min of walking/jogging at an intensity of 60%–80% of V̇O2peak, with an allotted warm up and cool down period. The AIT exercise protocol has been described in detail by others.18 19 It comprised: (1) a warm-up period of 5–10 min of walking performed at 60%–70% of Peak HR, and/or RPE of ~10–12 on the 6–20 Borg Scale; (2) four 4-min intervals of walking/jogging performed at an intensity targeting 90%–95% of Peak HR, and/or RPE ≥17 on the Borg Scale, interspersed with 3 min of active recovery performed at an intensity of ~50%–70% of Peak HR; and (3) a cool-down period of 5 min of walking performed at an intensity of ~50%–70% of Peak HR, and/or RPE ~10–12 on the Borg Scale. The AIT intervention (ie, 4-min intervals) replaced the usual care aerobic exercise component of CR only, and was not performed in addition to it. Otherwise, participants in the AIT group continued to participate in all other aspects of usual care CR with respect to the educational and RT components.
Clinical measurements
Cardiopulmonary exercise assessment
Aerobic exercise capacity, as measured directly by V̇O2peak, was acquired by a metabolic cart (Vmax Encore, SensorMedics, Yorba Linda, California, USA) that performed breath-by-breath gas exchange analysis, while a patient participated in an incremental protocol to exhaustion on a cycle ergometer (Ergoselect 200P, Ergoline, Bitz, Germany). Workload was increased by 16.7 Watt increments each minute, and VO2 was recorded continuously throughout the CPA as 20 s averages.4 V̇O2peak was captured in the last minute of exercise prior to reaching exhaustion and/or test termination, and documented as the highest 20 s average, normalised for body mass (reported as mL kg-1 min-1). Respiratory exchange ratio, which is a marker of metabolic effort,4 was calculated as the ratio of carbon dioxide to oxygen in breath-by breath gas samples acquired at the time of V̇O2peak measurement. Resting and maximal physiological measurements, such as heart rate and blood pressure, were measured and recorded as standard practice during CPA. Exercise prescriptions were based on maximal heart rates achieved during the CPA at intake, and adjusted accordingly at the 12-week (half-way point) CPA for the majority of patients who performed it.
Cardiovascular risk profile, adherence and quality of life
Cardiovascular risk profile, included fasting blood sugar, cholesterol and triglyceride levels, in addition to the measurement of anthropometrics, such as height, body mass, abdominal girth, and systolic and diastolic blood pressure values measured before and after the 24-week interventions. Adherence to exercise protocols during the supervised exercise sessions performed at the centre was captured by HR and speed data, using the Garmin Forerunner 620 GPS watch (Garmin, Olathe, Kansas, USA) and accompanying heart rate monitor. Adherence to the unsupervised, home-exercise sessions was evaluated by patients’ self-reported, weekly exercise diaries, in which patients were asked to record their frequency, distance, duration and intensity of exercise sessions (using HR and RPE) performed. Patient reported information was captured in the standard of care Cardiovascular Prevention & Rehabilitation Medical Health Questionnaire, which includes questions regarding the patient’s living situation/support structure, self-reported perceived quality of life, and the Centre for Epidemiological Studies Depression Scale (CES-D). Social support was measured using the 16-item Tangible, Informational, and Emotional Social Support Survey (TIES), because of its reliability and validity in ascertaining conspicuous nuances of social support that are particularly relevant in promoting health behaviour modification in patients with CAD.20
Cognitive assessments
A battery of neuropsychological tests was chosen based on harmonised standards in accordance with the National Institute of Neurological Disorders and Stroke and Canadian Stroke Network.21 Executive function and processing speed were assessed using the Trail-Making Test Part B. The Digit Symbol Encoding Task was administered as a measure of complex attention and psychomotor processing speed from the Wechsler Adult Intelligence Scale, third edition. Verbal memory performance was tested using the immediate, short, and long delayed free recall of the California Verbal Learning Test, second edition (CVLT-II) word list, while the Digit-Span Test Forwards and Backwards were administered to measure attention. All cognitive assessments were administered at a standardised time (ie, 09:30±30 min), for a duration of approximately 35–45 min, and subjects refrained from caffeine consumption for a minimum of 4 hours prior to testing. Z-scores were determined for each cognitive test shown, using pre-existing age-matched and sex-matched norms. With this approach, the population mean of each test variable is represented by zero (0), with positive values indicating better performance, and negative values indicating poorer performance, using the assumption of a normal distribution.
Sample size and power
Using recent data from a 2015 meta-analysis10 investigating the effects of AIT versus MICE on aerobic exercise capacity, as measured directly by V̇O2peak in patients with CAD, the observed effect size in V̇O2peak (the primary outcome measure for this study) between the AIT and MICE groups was 1.21.10 Recognising that this observed effect size was quite large, with the sample sizes composed predominantly of men, and that women commonly do not reap the benefits of exercise-based CR and improvements in aerobic exercise capacity to the extent often observed in men,22 the authors chose a more conservative estimate of effect size, namely an effect size that was ~60% of that observed in the 2015 meta-analysis.10 Therefore, conducting a G*Power Sample Size calculation for ‘t-tests’, and the statistical test of means between two independent samples for an a priori analysis, using an effect size of 0.74 (~60% of 1.21), an alpha level of p=0.05 for a two-tailed test, a power of 0.8, and an allocation ratio of 1 (N2/N1), 30 patients were required in each group for a total sample size of n=60. However, taking into consideration the 25%–30% attrition rate that has been observed in the CR population at our centre,23 and also reported by others,24 25 the target total sample size was adjusted to n=80 with a target of 40 patients in each study arm.
Statistical analysis
Data are presented as mean±SD, or number/percentage after confirming that the data were normally distributed using the Shapiro-Wilk test. In order to determine the treatment effect of AIT compared with MICE on CV risk profile characteristics, quality of life, Z-scores of cognitive tests, and the primary outcome measure of V̇O2peak after the 24-week programme, analysis of covariance (ANCOVA) was performed using baseline values as covariates. Baseline values were used as covariates in an attempt to mitigate any associations with the dependent variables of interest, such that we were isolating the treatment effect of the AIT intervention. ANCOVA was performed in R Programming (V.3.3.1, available at no cost at www.R-project.org, Vienna, Austria). The main analyses were performed using the intention-to-treat (ITT) principle,26 in which all patients were analysed according to their initially assigned group of AIT or MICE at baseline, irrespective of study adherence or completion. The baseline values for those subjects who dropped out from the study were used as the missing values at 24 weeks (postintervention), using the single imputation method of ‘last observation carried forward’. Since it was our intention to investigate the treatment effect of AIT, per protocol analysis was also performed that included only those patients who completed the original treatment allocation.27
Independent-samples t-tests were performed to assess differences between the AIT and MICE groups, while paired-samples t-tests were performed to assess within group differences. All t-tests were performed using SPSS (V.21.0). P values reflect the associated t-test for equality of means between or within the groups, with p<0.05 indicating statistical significance.
To explore if any factors could explain subjects completing the programme or not, stepwise linear regression was used to identify the subset of independent variables (IVs) corresponding with the best performing model, through the process of iteratively adding and removing IVs that minimised the error in model prediction. Prior to performing stepwise regression, the variable reduction technique of calculating a variance inflation factor (VIF) for each IV was performed to identify collinearity among the IVs. A stepwise approach was used in calculating VIFs for each variable, such that the iterative removal of variables resulted in a final subset of IVs with VIF values all below the threshold of 10.28 Only those remaining IVs were entered into the stepwise linear regression analysis. All analyses regarding the variable reduction technique and stepwise regression were conducted in R Programming (V.3.3.1, Vienna, Austria).
Results
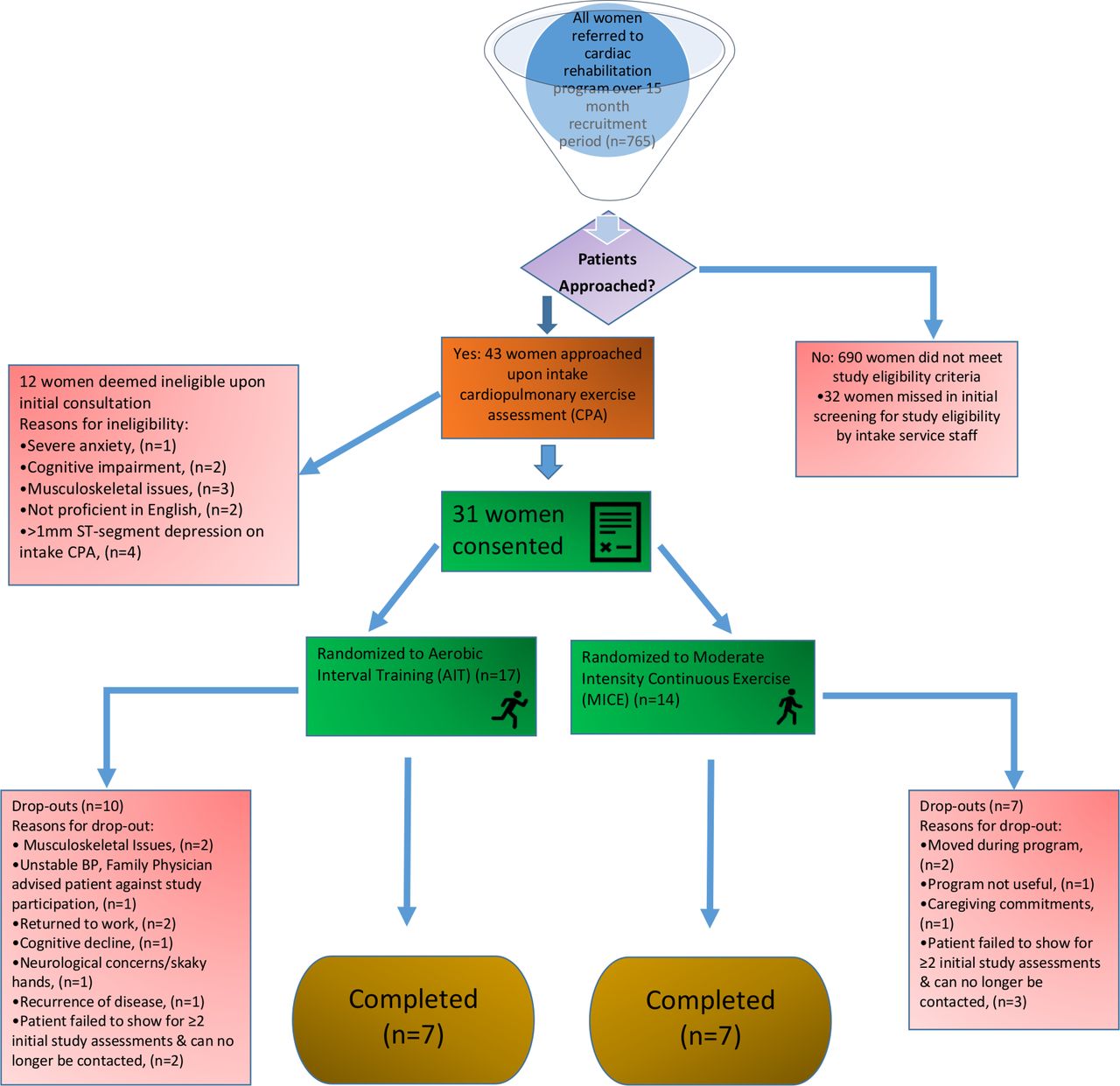
Figure 1 illustrates the process of study enrolment, randomisation and completion. Between 1 April 2017 and 30 June 2018, 765 women were referred to the 24-week CR programme. As shown in table 1, 690 women did not meet the study inclusion criteria according to their primary disease diagnoses and/or corresponding reasons for referral, or experienced a significant English language barrier that precluded participation in the study. Thus, only 10% of the 765 women referred met the study inclusion criteria, of which 57% (n=43) were flagged by clinical intake personnel to alert the researcher to the possibility of recruitment on intake CPA. From this significantly smaller group, 31 women consented to study enrolment, yielding 17 and 14 women initially randomised to AIT and MICE, respectively. As shown in figure 1, 59% of the women dropped out from the AIT group, while 50% of the women dropped out from the MICE group. The power calculations indicate that with 14 patients completing the study (n=7 in each group), there was insufficient power to detect statistically significant differences between the AIT and MICE groups. Thus, for the majority of the following subsections, we preface that none of the differences that we report are statistically significant unless explicitly indicated, and we present the data for hypothesis generating ideas and relationships that can be addressed in future research.
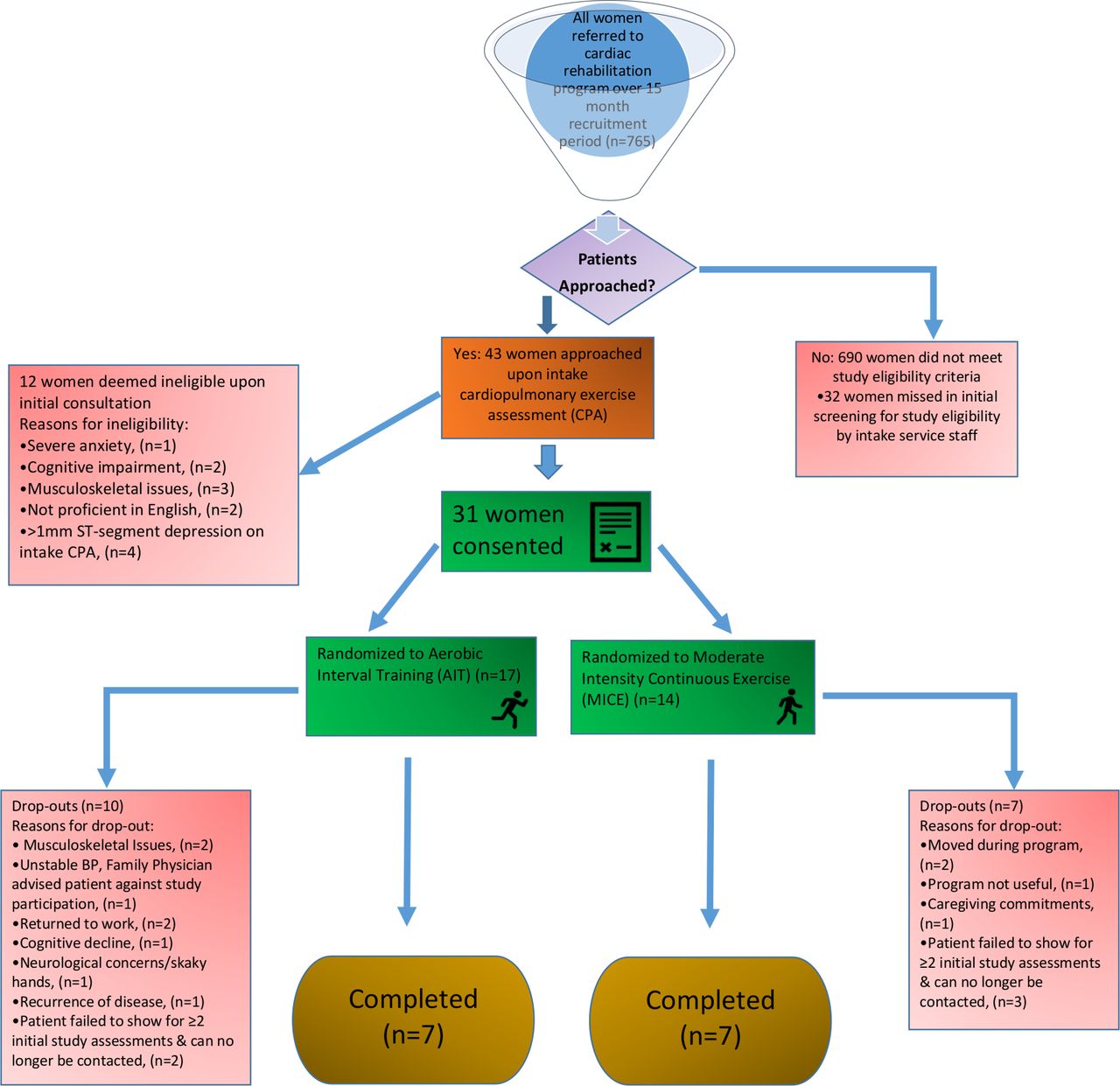
Flow chart of the process of study enrolment, randomisation and completion. BP, blood pressure; n, number of patients.
Primary disease diagnoses and reasons for excluding n=690 women from study participation
Baseline clinical and cardiovascular risk profile characteristics
Table 2 describes the baseline characteristics of all patients who were initially randomised to the two groups (n=31). Despite the prospective, randomised approach employed in this study, the small sample size and random chance alone account for the overall differences observed in weight, primary disease diagnosis, medications, marital status and CV risk profile characteristics between the groups.
Descriptive baseline and cardiovascular risk profile characteristics of study patients
Factors associated with predicting programme completion or non-completion
The stepwise variable reduction technique of calculating and iteratively removing IVs, with VIFs exceeding the threshold of 10, resulted in six remaining IVs suitable for entry into the stepwise regression analysis: body fat percentage, V̇O2peak, abdominal girth, resting HR, TIES score and CES-D score. None of these IVs were shown to significantly predict programme completion, or non-completion in our sample of 31 women with CAD, using stepwise regression analysis.
Cardiovascular risk profile characteristics and quality of life
As shown in table 3, the AIT group exhibited a more favourable CV risk profile postprogramme, with respect to body mass index, abdominal girth, body fat percentage, blood lipid levels, fasting blood glucose, and HbA1c (glycated haemoglobin) levels compared with the MICE group. Numerically greater reductions in abdominal girth and body fat percentage were observed in the AIT group. Both groups endorsed fewer depressive symptoms after the programme, as measured by the CES-D (with scores ≥16 indicative of clinical depression), with the AIT group demonstrating a larger reduction in symptoms postprogramme. The AIT group had greater social support than the MICE group, as indicated by higher TIES scores postprogramme. TIES scores increased in both groups after the programme, with the MICE group showing greater improvement than the AIT group. There was no significant treatment effect of AIT on any of the CV risk profile characteristics or quality of life measures, as assessed by both ITT and per protocol analyses.
Cardiovascular risk profile characteristics of all participants
Exercise-related outcome variables
Exercise-related outcome variables for all subjects are shown in table 4. Resting HR decreased in both groups following the programme. Peak HR was significantly higher in the AIT group compared with the MICE group postprogramme (p=0.023). V̇O2peak was significantly higher in the AIT group compared with the MICE group postprogramme (p=0.036), with only the AIT group demonstrating a statistically significant improvement postprogramme (p=0.04). Figure 2 illustrates the individual variability in all patients in both AIT and MICE groups that was observed with respect to the change in V̇O2peak over the 24-week programme. AIT had a significant treatment effect of improving the primary outcome measure of V̇O2peak by 0.95 mL kg-1 min-1 compared with the MICE group (p<0.001) in the per protocol analysis only. The ITT analysis, however, revealed no significant treatment effect of AIT on V̇O2peak, or any of the other exercise-related outcome variables. Similarly, the per protocol analysis did not significantly differ from the ITT analysis, with the exception of V̇O2peak.
Exercise related outcome variables

{kind=link}
{kind=link}
Individual plots demonstrating the variability in the change in aerobic exercise capacity (V̇O2peak) in patients randomised to performing either aerobic interval training (AIT) (n=7), or moderate intensity continuous exercise (MICE) (n=7). The thicker lines represent the mean values across time, with a significant difference observed between AIT and MICE groups (p=0.005). Four patients in the MICE group and one patient in the AIT group failed to attend their 12-week CPA. CPA, cardiopulmonary exercise assessment.
Adherence to exercise programme and exercise intensity in completers
For those who completed the programme, adherence was high. On average, patients completed 72.2%±15.2% of the five exercise sessions prescribed per week for the 24-week period in the MICE group, and the AIT group completed 76.2%±13.6% of their 5 weekly exercise sessions, with no significant differences between groups (p>0.05). Patients in the MICE group attended 2015–17 19–23 of the possible 24 once weekly on-site supervised sessions, while patients in the AIT group attended 2115–17 19–22 of the 24 sessions. HR and RPE were monitored during supervised exercise sessions at the CR centre. The MICE group exercised at a mean intensity of 68%±7.3% of Peak HR, and reported an RPE of 11.2±1.3 on the Borg Scale. The AIT group exercised at a mean intensity of 88.5%±2.9% of Peak HR, and reported an RPE of 16.7±0.6 on the Borg Scale. Mean exercise intensity and self-reported RPE were significantly higher in the AIT group (p<0.01 for both).
Cognitive function
Both ITT and per protocol analyses revealed no significant treatment effect of AIT on any of the cognitive domains postprogramme, and there were no within group differences in any of the measures in the AIT or MICE groups (table 5).
Cognitive test results expressed as Z-Scores
Adverse events in all patients
The patients did not experience any serious adverse events or require hospitalisation during, or within 3 hours after performing an exercise session of either MICE or AIT at home or at the CR centre. There were two women who dropped out from the AIT intervention group due to musculoskeletal complaints: one woman accidentally slipped on ice and fell and tore her meniscus in her knee, which was unrelated to the intervention, while another woman had worsening osteoarthritis in her knee. This was a pre-existing condition prior to the intervention, thus rendering it difficult to determine whether it was the specific nature of the intervention itself, or just exercise participation in general that exacerbated her symptoms.
Discussion
The present study is the first attempt at conducting a randomised controlled trial investigating the effects of AIT versus usual care MICE in exclusively female CAD patients, referred to a 24-week outpatient CR programme. The main finding was that this prospective study design was unfeasible in this female CAD patient population, and that the challenges encountered with the number of women meeting study inclusion criteria, in addition to the unexpectedly high attrition rates, ultimately rendered a sample size that was underpowered to adequately detect differences between the groups. Furthermore, with approximately 50% of the women dropping out from each arm of the study, there were no significant factors found to predict programme completion or non-completion. These barriers notwithstanding, the treatment effect analysis unveiled a 0.95 mL kg-1 min-1 improvement in the primary outcome measure of V̇O2peak in favour of AIT over MICE in the per protocol analysis. In agreement with two of the largest, randomised multicentre trials that implemented the ‘Norwegian’ four by 4-min AIT protocol in populations of CAD18 and chronic heart failure (CHF)29 patients, this study also found achieving exercise intensities of 90%–95% of Peak HR for the entire duration of 4-min intervals to be impracticable in our female CAD population.
Recruitment and eligibility
In the initial design phase of this RCT, we felt well-positioned to be successful in recruiting and having 30 women complete both arms of the study, given that we were conducting recruitment at the largest, outpatient CR programme in North America. Despite the relatively large sample of women who were referred to the programme during our 15-month recruitment period (n=765), we failed to anticipate that the majority of women referred were for primary prevention, or had several other primary disease diagnoses outside of our inclusion criteria of stable, documented CAD, such as valvular heart disease, cardiomyopathy, heart failure, stroke and so on. Therefore, only 10% of the referred population of women was initially eligible for this study. Moreover, many women had language barriers. This finding has important implications for conducting future, large-scale RCTs not only at this institution, but similar institutions located in diverse, multicultural cities around the world where such language barriers are of major significance. Given the nature of a busy clinical setting, and our reliance on personnel within the patients’ circle of care to screen and introduce potentially eligible study candidates for recruitment, it was unfortunate, but conceivable that 43% of the potentially eligible patient pool was missed. Irrespective of these challenges, we achieved a 72% success rate in obtaining consent from the 43 women that were approached on intake CPA, resulting in a total of 31 consented and randomised women in our study. Our 72% success rate of enrolling eligible patients into this study was quite high relative to the 27% participation rate of women reported in the large, multicentre RCT investigating the effects of AIT versus MICE in CAD patients.18 With respect to our CR centre, these findings highlight the enthusiasm and willingness of selected female patients with CAD who perceive AIT to be an acceptable modality for their rehabilitation programme. The 31 women that initially consented into our single-centre study was greater than the number of women who consented into Conraads et al’s study18 (n=20, 10% of the sample), despite their 28-month recruitment period compared with our 15-month recruitment period. In Ellingsen et al’s29 multicentre RCT investigating AIT versus MICE in heart failure patients, a total of 40 women (19% of the sample) were recruited over a 48-month recruitment period. Therefore, our difficulties in recruiting a sample size of eligible female patients to adequately power our study from the available population corroborated the experiences of others, who have conducted similar studies.18 29
Attrition
The challenges associated with sample size; however, extended beyond concerns of recruitment and the eligibility pool. Previous work conducted at our centre has indicated that women are much more likely than men to withdraw from CR for comorbid health conditions, namely concurrent disease or illness and musculoskeletal issues, in addition to familial obligations.23 Though we were prepared to account for a 25%–30% attrition rate in our sample size calculation, we had not anticipated a 59% and 50% attrition rate in our AIT and MICE groups, respectively. This exceeds the 35% drop-out rate (7/20) of women with CAD observed by Conraads et al.18 The majority of women in our study dropped out due to comorbid health conditions, in agreement with previous findings,23 and non-compliance to study assessments/CR classes. Thus, the unforeseen attrition rate combined with our difficulties with recruitment availability and eligibility rendered our study design unfeasible, and insufficiently powered to assess differences between our intervention and control groups. Despite our attempt to explore the factors that may have been associated with programme completion or non-completion, the stepwise linear regression model failed to identify any significant predictors of completion or drop-out. Given that approximately 50% of the women dropped out from each of the study arms, perhaps it is unsurprising that the regression analysis failed to reveal any significant predictors. The small sample size may have also contributed to a less robust linear model, therefore further perpetuating the negative findings.
In light of evidence suggesting that resistance training as a standalone intervention can improve not only muscular strength, but also V̇O2peak in young and older healthy, untrained adults,30 patients with CAD,31 and patients with CHF,32 33 this modality may serve as a feasible alternative to MICE or AIT for individuals who are unable to perform aerobic exercise due to comorbid health conditions. Usual care CR involves performing 2 days per week of resistance training, and thus it is conceivable that with the resources and equipment already available to patients at a CR centre, it would be feasible to include a third day of resistance training for those patients who cannot participate in aerobic exercise training. Perhaps, resistance training as a single intervention can also be offered to those patients who simply have no preference for aerobic exercise, and who would potentially show greater adherence to a resistance training-only programme. A recent meta-analysis showed that a standalone resistance training programme yielded a weighted mean difference (WMD) improvement in V̇O2peak of 0.92 mL kg-1 min-1 in CAD patients who were <65 years of age compared with usual care control.31 The same study demonstrated that CAD patients ≥65 years of age experienced a WMD improvement in V̇O2peak of 0.70 mL kg-1 min-1 compared with usual care control.31 These findings suggest that resistance training as a single intervention for CAD patients has a clinically relevant effect on improving V̇O2peak.11–13 This may have important implications for future exercise training modalities that CR programme may consider offering their patients in a concerted effort to minimise attrition rates, and to maximise both exercise adherence and patient health outcomes.
Improvement in the primary outcome measure of aerobic exercise capacity
The improvement in V̇O2peak in the women randomised to AIT was 3.4±2.5 mL kg-1 min-1 in the per protocol analysis, which is similar to the 3.6±3.1 mL kg-1 min-1 improvement that was observed in another small study that comprised 15 patients with coronary heart disease in the AIT group (four women), and 13 patients in the MICE group (one woman).9 The women randomised to MICE in our study achieved a 0.9±2.3 mL kg-1 min-1 improvement in V̇O2peak in the per protocol analysis, which is lower than the 1.7±1.7 mL kg-1 min-1 increase observed by Keteyian et al.9 Although the majority of patients were men in Keteyian et al’s9 study, those results were achieved over a shorter time period of 12 weeks, compared with our 24-week programme. After randomising CAD patients to a 10-week rehabilitation programme of AIT (n=8, two women) or MICE (n=9, one woman), Rognmo et al6 reported an approximate 6 mL kg-1 min-1 and 2.7 mL kg-1 min-1 improvement in V̇O2peak in those groups, respectively. Those improvements were greater than those found in our study; however, it is difficult to compare our results directly with others without isolating findings by sex. We have previously shown at our centre that women with CAD who performed 6 months of usual care CR involving MICE experienced an approximate 3 mL kg-1 min-1 improvement in V̇O2peak.17 Thus, in contrast with our previous findings,17 this small sample of women who were randomised to the MICE group and completed the programme achieved lower than expected improvements in V̇O2peak, which may be attributable to random chance alone. Nevertheless, both groups in our study that completed the interventions likely achieved improvements in V̇O2peak that were of clinical significance, based on seminal findings indicating that even a marginal gain of 1 mL kg-1 min-1 in V̇O2peak is associated with a 10% reduction in cardiac mortality over a 15-year period, in women with CAD.12 Taken within this context, and acknowledging our limitations associated with small sample size, the significant treatment effect of 0.95 mL kg-1 min-1 in favour of AIT over MICE that we found in the per protocol analysis is at the very least hypothesis-generating, in the potential for AIT to be an effective exercise training modality for certain female patients who may prefer it.
Exercise training intensity and initial female perspectives regarding AIT
The average training intensity of the AIT group was approximately 88% of Peak HR, which was lower than the prescribed target of 90%–95% of Peak HR. Our findings are similar to Conraads et al18 who also reported an average training intensity of 88% of peak HR in their AIT group, and to Ellingsen et al29 who found a median relative training intensity of 90% of Peak HR (IQR 88%–92%) in their AIT group. Importantly, 51% of patients in the AIT group were unable to exercise at the prescribed 90%–95% of Peak HR in Ellingsen et al’s29 study, while Conraads et al18 described having to lower the training intensity for patients, so that they could continue to exercise without stopping and to prevent severe hyperventilation. In accordance with those findings,18 29 we also contend that exercising at 90%–95% of Peak HR for consecutive 4-min intervals is unfeasible and unrealistic in the majority of women with CAD in the real-world CR setting. Using a qualitative approach in a separate substudy that will be published elsewhere, we captured the experiences and perspectives of the women with respect to being randomised to and performing AIT. Overall, the women described AIT to be a daunting undertaking. They expounded on the physical discomfort of their: biomechanical limitations to jogging or running, back or hip pain, shortness of breath and hyperventilation. Finally, the women spoke of comorbid health conditions that prevented or hampered their ability to perform AIT. Although some women expressed the sense of enjoyment and accomplishment associated with performing AIT, the majority of women expressed their preference for performing MICE over AIT. These novel findings compel us to consider the complexity of implementing AIT into clinical practice, and emphasise the need for considering psychosocial elements and patient preferences, in addition to physical fitness components in individualising CR programme that may involve AIT. Thus, we believe that the discussion surrounding the inclusion of AIT into standard care of patients with CAD is inconclusive, and warrants further quantitative and qualitative exploration in larger samples of men and women alike with CAD.
Cardiovascular risk profile characteristics
With respect to CV risk profile characteristics, we did not observe any changes in cholesterol levels, triglycerides, or blood pressure following 24 weeks of CR in either group, as they were likely well-controlled in both groups with optimal drug therapies. Similar to our previous findings in this population,17 greater reductions in abdominal girth, body fat percentage, and depression score were observed in the AIT group following 24 weeks of CR, though we did not have the power to detect statistical differences between groups. Both groups demonstrated improvements in depression score and social support relevant to promoting health behaviour modification,20 which highlights the beneficial psychosocial aspects of CR in improving the quality of life of patients with CAD,34 irrespective of exercise training modality.
Cognitive function
In light of evidence demonstrating a significant positive association between V̇O2peak and cognition in patients with CAD, independent of other CV risk factors,35 we sought to describe changes in cognitive function (as a secondary objective) in response to AIT compared with MICE. The patients in our study scored average compared with sex-matched and age-matched norms with respect to executive function, complex psychomotor processing speed, attention, and verbal memory at baseline, with their scores remaining unchanged following 24 weeks of AIT or MICE. In older adults, and especially in a population of women with CAD who is at higher risk for cognitive dysfunction,35 36 it remains unknown which type of exercise training is most beneficial for improving cognitive function, and warrants future research in much larger, representative sample sizes.
Strengths and limitations
The strength of this study is that it is the first to attempt to address the paucity of representation of female patients, in the investigation of the generalisability of the potential superiority of AIT compared with MICE in improving V̇O2peak, and secondary health outcomes in the CAD population. Though we were unsuccessful in conducting an RCT with sufficient power to detect differences between the intervention and control groups, we have gathered important lessons and information that will help pave the way for future research, and particularly in the design of study interventions in this domain. We have discussed study limitations extensively in this manuscript; however, we recognise that our eligibility criteria should have extended beyond patients with stable, documented CAD, to allow for the inclusion of the majority of female patients who are now being referred to outpatient CR programme. Furthermore, our exclusion criteria detailing any conditions that precluded participation in resistance training would have also been a limitation to this study, as individuals who may have been able to participate in the trial would have been excluded for conditions that did not necessarily preclude them from participating in the aerobic exercise component of AIT or MICE. However, we were fortunate in this study not to exclude potential individuals from participating in the trial exclusively for the reason of not being able to participate in resistance training, while still being able to perform either AIT or MICE. Our small sample was also homogeneous, with predominantly Caucasian, middle to upper-class women.
Conclusions
The first attempt at addressing the generalisability of the potential superiority of AIT over MICE in improving aerobic exercise capacity in women with CAD, using an RCT study design, was unfeasible in a standard outpatient CR setting. The myriad challenges in recruitment eligibility, combined with unexpectedly high attrition rates in both study arms, rendered the study insufficiently powered to adequately detect differences between groups. AIT performed as consecutive 4-min intervals at an intensity of 90%–95% of Peak HR was both daunting and unfeasible for the majority of female CAD patients. Despite the small sample size, there was a significant treatment effect of AIT in improving V̇O2peak compared with MICE in the per protocol analysis. Thus, further research is required to elucidate the patient profile and circumstances under which the potential for the implementation of AIT may be individualised, and offered in clinical practice.
Acknowledgments
The authors extend their sincerest gratitude to: the entire Human Performance Laboratory staff at the Rumsey Centre, under the supervision of Rene Belliard; the team of Cardiac Rehab Supervisors who shared their class time and space, under the supervision of Valerie Skeffington; Prathiba Shammi and Walter Swardfager for their expertise, training and consultation in administering and analysing the neuropsychological cognitive tests; Jessica Nooyen and Chineze Nwebube for conducting study randomisation and allocation; Sonia Watson for booking CPA appointments; and Karen Dobson, Betty Chau and Emily Oleynik for the screening of potential study patients.
References
Footnotes
Twitter @LeannaTri
Contributors LSL, DB, M-CT and PIO contributed to the conceptual design of the study. M-CT and LSL provided the statistical analysis for the data. LSL and PIO provided the clinical interpretation of all of the patient data. LSL wrote the manuscript, and PIO and DB critically reviewed it, and all authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the University Health Network Research Ethics Board (ID#16–5900).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.