Article Text

Abstract
Objectives This study aimed to determine if ball position influences the risk of lower limb non-contact injury in hockey sweep pass. It also aimed to determine a ball position that minimises excessive strain placed on the lower limb joints of the lead leg during the sweep pass.
Methods A cohort of 18 female hockey-playing volunteers (age: 19.7±1.5 years; height: 165.5±5.4 cm; body mass: 66.4±7.0 kg) were recruited. Participants performed the sweep pass using three different ball positions: in front, in line with, and behind the heel of the lead (left) foot.
Motion analysis and force plate data were collected. Moments and angles in all three planes of motion for the three main lower limb joints were then calculated using Vicon software. Results were statistically analysed using SPSS software.
Results Significant differences (p<0.05) were found between the three tested ball positions for the mean maximum angles and moments, and mean ranges of motion produced at the lead three main lower limb joints. Positioning the ball in line with the heel of the lead foot resulted in the lowest moments and angles when compared with the other two ball positions.
Conclusions The results indicate that positioning the ball in line with the heel of the lead foot is recommended to minimise the risk of injury to the lower limb joints during the hockey sweep pass. It is hoped that these findings will result in this position being implemented by players new to hockey or those returning to the sport following injury.
- hockey
- sweep pass
- injury
- ball position
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
There is a scarcity of research regarding the sport of hockey. There are currently no published papers regarding the sweep pass, and few that discuss the role of ball position in injury prevention.
Ball position affects the moments and angles experienced at the lead lower limb joints during the sweep pass.
Positioning the ball in line with the heel of the lead foot reduces the risk of excessive strain at the lower limb joints during the hockey sweep pass.
Introduction
Field hockey (hockey) is played in 132 countries with the majority registered as amateur players.1 For example, in Scotland, there are 12 510 registered players with 12 390 being amateurs (communication with Scottish Hockey Union). Despite its popularity, when compared with other sports, hockey is the primary focus of substantially fewer published research papers.2
In the present literature, there are no papers that focus on the biomechanics of the hockey sweep pass. The sweep pass is versatile and can be used by any outfield player.3 The dynamics of the sweep pass are depicted in figure 1.

The sweep pass.
Lower limb and non-contact injuries are frequently reported to be the most common types of injuries sustained during hockey participation.4–7 Ankle sprains have been reported to be the single most common mechanism of injury, followed by those affecting the structures of the knee.5 Hip strains are also among some of the most common forms of injury.5
Ball position as a modifiable factor that could influence injury risk in hockey passes has scarcely been investigated, despite the fact that ball position has been shown to affect the direction and magnitude of forces experienced in the lower limbs during a hit.8 Hitting the ball in front of the lead toe, as opposed to behind or in line with it, increases the risk of damage to the lateral structures of the ankle and knee.8
Reference values for the lower limb joints
Ranges of motion
The range of motion (ROM) that each joint can safely achieve varies between individuals. The risk of sustaining an injury depends on interplaying factors. Therefore, it is not possible to state with certainty that above a certain ROM injury will occur. Maximum ROMs quoted in the literature are approximations and are not applicable to every individual. However, in the present study these will be used as reference values to determine whether the angles the joints are subject to result in an increased risk of injury.
From the literature, the typical ROM was determined at the ankle as 10°–20° dorsiflexion, 40°–55° plantarflexion, 23° inversion and 12° eversion.9 In the transverse plane, 19.6°–35.4° of motion is reported as possible.10
With regard to the knee, it has been reported that 155° flexion and 3° extension are typical.11 A few degrees of adduction and abduction can be achieved if the knee is flexed at 30°.11 A maximum of 25° internal rotation can be achieved.11 However, this is restricted by flexion greater than 120° and by full extension.11 A maximum of 18° external rotation can be achieved when the knee is at 30°–40° flexion.11
The typical ROM at the hip has been reported as 140° flexion, 15° extension, 25° adduction, 30° abduction, 70° internal rotation and 90° external rotation.11 Extension restricts the degree of rotation possible in the transverse plane.11 However, another article stated that the hip can achieve 120° flexion, 10° extension, 70° adduction, 70° abduction, 50° internal rotation and 50° external rotation.12 These quoted values are similar, but discrepancies exist, and this must be considered during the analysis of the present study results.
Moments during gait
Reference values to compare results from the present study will be taken from the maximum moments present during gait. These are standardised to account for variances in individuals’ body mass. During gait the maximum moments experienced at the ankle are 1600 Nmm/kg (plantarflexion) and 200 Nmm/kg (dorsiflexion).11 However, moments in the coronal and transverse planes are not reported.11 The maximum moments experienced by the knee are as follows: 200 Nmm/kg (flexion), 600 Nmm/kg (extension), 400 Nmm/kg (abduction), 180 Nmm/kg (internal rotation) and 150 Nmm/kg (external rotation).11 A small adduction moment is also present.11 The maximum moments at the hip are stated as: 1000 Nmm/kg (flexion), 5000 Nmm/kg (extension), 300 Nmm/kg (adduction), 700 Nmm/kg (abduction), 180 Nmm/kg (external rotation).11 A slight internal rotation moment is also present.11 Increase in external moments was shown to increase the risk of injury.13–16
The principal aim of this study was to evaluate the effect of ball positioning on the biomechanics of the hockey sweep pass. This study aimed to determine if ball position affects the moments and angles experienced at the lead lower limb joints during this pass. It also aimed to determine the ball position that minimises excessive strain on the lead lower limb joints during this pass.
Methods
Participant procedure
Twenty-one participants were recruited from the local amateur hockey club. Participation was voluntary. The requirements to participate in this study were: female, between the ages of 18 and 25; regular hockey player (defined as currently participating in hockey at least once a week for the duration of the past season); currently uninjured; and in good general health.
A participant’s data were discounted if there was not three adequate trials per ball position. Subsequently, three participants were discounted and 18 participants (age: 19.7±1.5 years; height: 165.5±5.4 cm; body mass: 66.4±7.0 kg) contributed to the results.
Participants were required to wear sports shorts and a sports bra to aid accurate marker placement on the skin. Standard hockey shoes, stick and ball were provided for use during the study. Retroreflective markers were attached to the participant’s skin to detect full-body movement as shown in figure 2.17

Marker placement.17 LANK, Left Ankle (Lateral); LASI, Left ASIS; LBHD, Left Back Head; LELB, Left Elbow; LFHD, Left Front Head; LHEE, Left Heel; LKNE, Left Knee (Lateral); LMANK, Left Ankle (Medial); LMELB, Left Elbow (Medial); LMKNE, Left Knee (Medial); LPSI, Left PSIS; LSHO, Left Shoulder; LTHI, Left thigh; LTIB, Left Tibia; LTOE, Left Toe; LWRA, Left Wrist; LWRB, Left Wrist; RANK, Right Ankle (Lateral); RASI, Right ASIS; RBHD, Right Back Head; RELB, Right Elbow; RFHD, Right Front Head; RHEE, Right Heel; RKNE, Right Knee (Lateral); RMANK, Right Ankle (Medial); RMELB, Right Elbow (Medial); RMKNE, Right Knere (Medial); RPSI, Right PSIS; RSHO, Right Shoulder; RTHI, Right thigh; RTIB, Right Tibia; RTOE, Right Toe; RWRA, Right Wrist; RWRB, Right Wrist.
Confidentiality was ensured as data were collected and stored anonymously.
Anthropometric measurements conducted comprised: height, weight, lower limb length (from anterior superior iliac spine[ ASIS] to medial malleolus), knee width (width across the femur) and ankle width (width across the two malleolus).
Laboratory layout
Data were collected using a Vicon Nexus 2.8.1 motion analysis system, 14 Vicon motion analysis T-series cameras and an AMTI force plate.
A safety net was hung across the gait laboratory in front of the area where the sweep passes were conducted. A 3×4 m2 of dry water-based AstroTurf was placed on the laboratory floor. This laboratory layout is shown in figure 3.18 A line was marked at a 45° angle from the long side of the force plate for the trail leg to line up with during address. The point where the heel of the lead foot should be placed was marked, and a line was drawn in line with the trail leg line to indicate lead foot placement. Three more lines were taped to indicate ball positions, one in line with the heel of the lead foot and the other two were 30 cm either side of this. The markings for ball and foot positions are shown in figure 4.
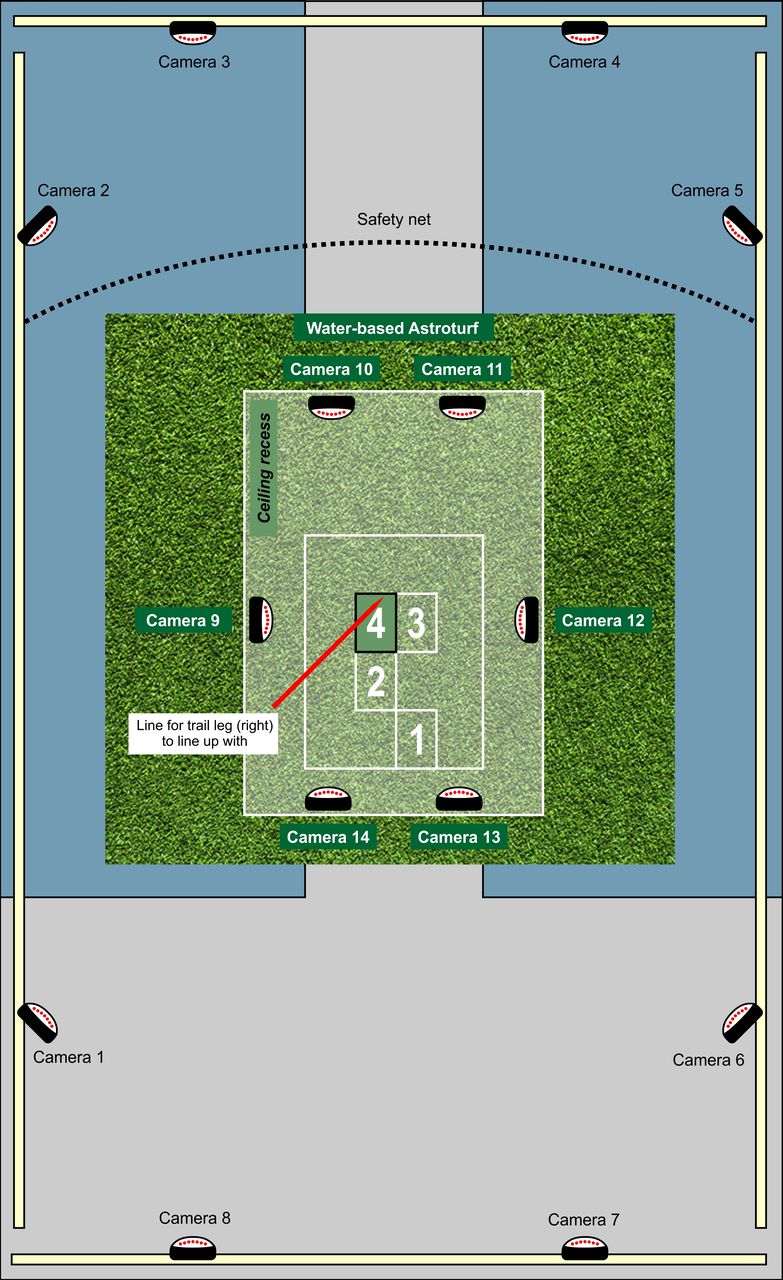
Laboratory layout.18

Ball and foot positions.
Data collection
Participants performed a short warm-up routine before practising the sweep pass using the marked positions for the trail leg and lead foot. This allowed familiarisation with the required angles of address. Their preferred ball position was marked to ensure all tested ball positions lined up with this in relation to their lateral distance from the heel of the lead foot. This ensured that lateral discrepancies between ball positions did not affect results.
Each ball position was then tested. For every ball position, data were collected three times. Ball and foot position were confirmed by observation of the lead investigator. If there was any deviation from the correct positions the trial was discounted, and the attempt repeated.
Data analyses
Data were processed and labelled using Vicon software. The maximum angles and moments, and ROM produced at the lead ankle, knee and hip during stance phase were extracted.
Statistical analysis was undertaken using the SPSS software V.22. The data from each of the three ball positions were analysed and compared using the general linear model and pairwise comparisons. Results were considered significantly different if p<0.05.
Patient and public involvement
No patients were involved in this study. Participants, who were members of the general public, were not involved in the design of the study. They first became involved in the research process during recruitment via email or seeing a volunteer recruitment poster. They were not asked to assess the burden of intervention or time required, nor were they involved in result dissemination. All participation was entirely voluntary and without remuneration or incentive. Volunteers were able to withdraw from the study at any time and without having to give reason.
Results
Where one ball position was found to cause an angle/moment that was significantly lower than the other two positions, it was considered to result in the lowest angle/moment. If the angles/moments produced by the other two positions were statistically similar both were considered to result in the greatest angle/moment. The inverse was considered true where one position’s result was significantly greater than the other positions’ results which were statistically similar. Where there was no significant difference between results, all positions were considered to cause the lowest angle/moment. In this way the ball position that caused the greatest mean maximum angles/ROM/moments in each direction will be described. The moments and angles produced at each position and p values for significant differences (p<0.05) between positions are shown in table 1.
Mean maximum angles and moments (with 95% CI) produced at each ball position Foot and ankle movements are as defined by Abboud26

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean maximum angles and moments (with 95% CI) produced at each ball position at each of the main lower limb joints.
Ankle angles and moments
Significant results were found in the maximum abduction and eversion angles, and maximum dorsiflexion and adduction moments. The furthest back position resulted in the greatest maximum abduction angle (p<0.001). The maximum eversion angle was greater with the ball in line than with the ball in front (p=0.037). The greatest maximum dorsiflexion moments were produced with the ball in line and in front. The greatest maximum adduction moment was produced when the ball was in front (p<0.05).
Knee angles and moments
The ball placed behind resulted in the greatest maximum adduction angle, extension moment and external rotation moment (p<0.05).
Hip angles and moments
The greatest maximum flexion angle was produced with the ball in front (p<0.05). Overall sagittal ROM was greater with the ball behind than when the ball was in line (p<0.05). The greatest maximum adduction angle was produced when the ball was in front (p<0.001). The greatest coronal ROM was produced with the ball in front (p<0.05). The greatest maximum abduction angle was produced when the ball was placed behind (p<0.05). The maximum adduction moment produced was greater when the ball was positioned in front than when it was behind (p<0.05).
Discussion
The ball position considered to minimise the risk of lower limb injury was that which produced the lowest maximum angles and moments least often.
Ankle
The ankle is vulnerable to injury in many sports.19 Ankle sprains are the single-most common cause of injury in hockey.7 Hence, it is crucial to consider how to reduce their incidence.
Positioning the ball behind resulted in the greatest abduction angle (22.5°). The maximum transverse ROM has previously been reported to lie between 19.6° and 35.4°.10 The proportion of this ROM that consists of possible abduction is not reported.10 However, 22.5° is greater than the lowest boundary for transverse ROM. Therefore, positioning the ball behind could pose a significant risk of injury to the ankle as an increased abduction angle is a contributing risk factor for medial ankle sprains.19
Ball position was seen to affect the dorsiflexion and adduction moments at the ankle. Positioning the ball behind produced the lowest dorsiflexion moment (1038 Nmm/kg; p<0.05). Therefore, positioning the ball in line or in front resulted in the greatest dorsiflexion moments. However, all dorsiflexion moments produced were at least fivefold greater than the 200 Nmm/kg moment present during normal gait.11 As a result, and regardless of ball position there is a large dorsiflexion moment present during the sweep pass which may potentially damage ankle structures if sustained repeatedly. The adduction moment produced was greatest with the ball placed in front (367 Nmm/kg; p<0.05). This high adduction moment places the ankle at risk of a lateral ankle sprain.19 This is the most common type of ankle injury seen in sport and the same is possibly true for hockey.19
These results have demonstrated that the ball placed in front resulted in high dorsiflexion and adduction moments. Therefore, this position places the ankle, especially the lateral structures, at an increased risk of injury.13–16 20 However, positioning the ball behind increased the risk of damage to the medial structures and positioning the ball in line resulted in a high dorsiflexion moment. Therefore, although it would be recommended from these results that the ball is placed in line with or behind the heel of the lead foot when addressing the sweep pass, this is a weak recommendation.
Knee
The knee is commonly injured in hockey.7 Ball position has been shown to influence the risk of injury to the lateral structures of the knee.8
In the present study, significant findings were reported in the knee adduction angle produced between ball placements. Positioning the ball behind resulted in the greatest angle (22.7°) compared with positioning the ball in front (20.2°) or in line (20.4°). The knee is only reported to be capable of a few degrees of adduction when the knee is in 30° of flexion.11 The concurrent degree of knee flexion is unknown for when these peak angulations are produced. However, all three adduction angles produced were much greater than the normal ROM even if the knee was in the optimal 30° of flexion. However, positioning the ball behind resulted in the greatest adduction angle and thus was most likely to result in the greatest risk of medial compartment injury to the knee.21
The greatest maximum extension and external rotation moments were produced when the ball was positioned behind. The ligaments that encapsulate the knee joint resist excessive extension and rotation, and if strained may tear. In particular, risk factors for an ACL injury include increased extension and external rotation.22 Therefore, positioning the ball behind may pose the greatest risk for injury to the ACL. However, the maximum extension and external rotation moments produced at all three ball positions were many times greater than those typical during normal gait, and therefore all may potentially pose an injury risk.11
It is clear from these results that positioning the ball behind the heel of the lead foot most frequently caused the greatest angles and moments. Therefore, it is recommended that the ball be positioned in line with or in front of the heel of the lead foot to minimise the risk of knee injury during performance of the sweep pass.
Hip
Injuries at the hip during hockey participation are less commonly reported than for the ankle and knee.7 However, drag-flick technique has been linked to hip injuries.23 Due to a deficit of research into the sweep pass and its similarities to the drag-flick, it may also put the hip at risk of injury.
Positioning the ball in front produced the greatest maximum flexion angle (123.3°; p<0.05). However, all ball positions caused a degree of flexion similar to the reported maximum range possible (120°–140°).11 12
The greatest adduction angle (7.8°) was produced with the ball in front and the lowest when the ball was behind. All adduction angles produced were much lower than the 25° of abduction possible.11 Therefore, all positions may pose a low risk of injury to the hip due to adduction, but with the ball placed in front the risk is relatively higher.
The greatest abduction angle was produced with the ball behind (35.0°) and the lowest when the ball was in front (31.8°). These are greater than the reported 30° of possible abduction.11 Therefore, all ball positions could pose an injury risk to the hip, with ball behind posing the greatest relative risk. The coronal ROM was greatest with the ball in front (39.6°). The reference coronal ROM is reported as 55°, greater than the angles produced at all ball positions in the present study.11
Positioning the ball in front resulted in a greater adduction moment (1116 Nmm/kg) compared with when the ball was positioned behind (947 Nmm/kg) (p=0.041). However, all ball positions resulted in at least a threefold greater adduction moment than that present during normal gait.11 Therefore, all ball positions may pose a significant risk to injury to the hip due to a high adduction moment. In addition, if the ball is placed in front this risk is greater than if it is placed behind.
The ball positions behind and in front of the heel of the lead foot are most likely to result in the greatest extremes of angulation at the hip, and the ball in front may produce a greater injury risk from an adduction moment. Therefore, the ball in line would be recommended to reduce risk of injury to the hip.
Limitations
The results are perhaps only applicable to amateur female players. It has been reported in previous studies that males and females differ biomechanically in how they conduct a pass.24 Likewise, there are key differences in the execution of a pass between amateur and professional players.25 Hence, it would be justifiable to repeat this study with male only and equally with professional players of both genders to assess if there are differences rather than speculating on outcomes. In addition, the net joint moments do not represent the load on the joint structures (ie, the forces in the ligaments and tendons) and as such these should be investigated in future studies.
Conclusion
Ball position significantly affects the angles and moments experienced at the lower limb joints. Positioning the ball in line with the heel of the lead foot was most likely to result in the lowest angles and moments during execution of the sweep pass.
The findings of this study indicate the relevance of ball position in hockey due to its effect on lead lower limb joint biomechanics. It is hoped that this can lead to better education of players and coaches so that they consider ball position when participating in hockey and implement this safer position. It is unlikely that this change will be implemented by experienced, uninjured players as they are more likely to have a firmly established natural ball position to address the sweep pass. However, new players and players returning from injury could implement this position at an early stage and thus lower their risk of future lower limb joint injury during this pass.
Acknowledgments
The authors would like to thank Mr Ian Christie for his valuable assistance in the production of bespoke images.
References
Footnotes
Contributors JA: planning the study, conducting the study, analysing the data, reporting the study, generating the draft write-up, responsible for overall content as guarantor. GA: data collection for study and Vicon markers repeatability. SN: data collection for study and Vicon software reliability. WWW: statistical analysis of data. RA: reporting the study, revising the original and revision manuscript critically for intellectual content, submitting the study, responsible for overall content as guarantor.
Funding The study was funded internally by the department. No external funding was sought or received.
Competing interests None declared.
Patient and public involvement statement No patients were involved in this study. Participants, who were members of the general public, were not involved in the design of the study. They first became involved in the research process during recruitment via email or seeing a volunteer recruitment poster. They were not asked to assess the burden of intervention or time required, nor were they involved in result dissemination. All participation was entirely voluntary and without remuneration or incentive. Volunteers were able to withdraw from the study at any time and without having to give reason.
Patient consent for publication Not required.
Ethics approval The study was approved by the Medical School Research Ethics Committee – ID SMED REC 111/18.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.