Article Text

Abstract
Objectives The global lack of sports and exercise medicine (SEM) teaching at medical schools contrasts with evidence that physical activity (PA) plays a major role in preventing and treating non-communicable diseases (NCDs). The aims of this study were to (a) examine whether Swiss medical students are expected to acquire SEM-related skills and knowledge, (b) systematically reviewed SEM teaching in the Swiss undergraduate medical curricula, (c) assess if Swiss medical students are aware of SEM and (d) whether they would like SEM to be included in their curricula.
Methods Two authors independently screened the ‘Principal Relevant Objectives and Framework for Integrative Learning and Education in Switzerland’ (PROFILES) for SEM-related learning objectives and reviewed the curricula. 7708 Swiss medical students were invited to participate in an online survey.
Results 32 SEM-related learning objectives were identified in PROFILES with 20 of them linked to PA. Four of eight Swiss medical schools display limited mandatory SEM teachings. 1764 students participated in the survey (482.0% of the necessary sample size, 22.9% of all Swiss medical students). One in two students knew that SEM includes preventing and treating NCDs. Almost 95% of the participants would like SEM to be included in the curricula.
Conclusion Despite its inclusion in PROFILES and comprehensive evidence that SEM should be taught at medical schools, this is scarcely the case in Switzerland. Swiss medical students have limited understanding of SEM, but are keen to have it included in the curricula. This study highlights the need for more comprehensive SEM teaching at Swiss medical schools.
- sports and exercise medicine
- undergraduate
- teaching
- online survey
- medical students
- Switzerland
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings?
Sports and exercise medicine (SEM)-related learning objectives, mainly linked to physical activity, are included in the official document setting the skills and knowledge Swiss medical students have to acquire during medical school.
Despite this, SEM is scarcely taught at Swiss medical schools.
Swiss medical students have limited understanding of SEM with only half of them aware that exercise medicine is a part of SEM.
An overwhelming majority of respondents would like to have SEM included in their curricula.
Introduction
Sports and exercise medicine (SEM) encompasses two different but related topics, namely sports medicine and exercise medicine.1 ‘Sports medicine is involved with prevention, diagnosis and management of musculoskeletal disorders and medical issues related to physical activity (PA), while exercise medicine aims to use PA to prevent and treat chronic diseases’.1 2 SEM is now a recognised medical specialty in 26 countries worldwide.3 4 Nevertheless, SEM is still scarcely taught at the undergraduate level even in the above-mentioned countries.5 6
Musculoskeletal conditions are highly prevalent within the general population and greatly limit daily activities and productivity within developed and developing countries.7–9 Sports injuries are frequent, with an annual prevalence around 20% in a representative sample of the general Danish population.10 Furthermore, with rising rates of non-communicable disease (NCDs) the search for cost-effective measures of prevention and treatment has become a priority worldwide.4 11 12 PA is one of the means to combat NCDs.13–15 Physical inactivity has been recognised as the fourth leading cause of death worldwide, and is described as a pandemic by the WHO.13 16 In 2018, the WHO published the ‘global action plan on PA 2018–2030 which aims towards a ‘15% reduction in the prevalence of physical inactivity by 2030’.17 To reach this aim, one of the principle points in these guidelines is to educate health professionals about PA promotion and prescription.17
Since 2000, several studies have highlighted that medical doctors, particularly general physicians, are not knowledgeable enough about PA benefits and prescription and thus neither confident to prescribe it nor to refer patients to an SEM specialist.18–21 Similarly, a British study showed that ‘medical students underestimate the risk of physical inactivity, do not know the PA guidelines and feel unconfident about giving PA advice’.22 This systemic lack of knowledge and teaching at medical school markedly contrasts with the evidence that PA plays a major role in preventing and treating almost all the NCDs.13–15 Yet, some data suggest that medical students are keen to learn more about SEM.23 Moreover, examples of successful sports and/or exercise medicine implementation in the undergraduate curriculum have been shown in Nottingham (UK), South Carolina (USA) and in Tehran (Iran).24–26
The ‘Principal Relevant Objectives and Framework for Integrative Learning and Education in Switzerland’ (PROFILES), written by Swiss experts under a mandate of the Joint Commission of the Swiss Medical schools, sets out the skills and knowledge Swiss medical students have to acquire during the 6 years of study.27 ‘PROFILES displays three different chapters: a first chapter listing general objectives related to the different roles of doctors, a second chapter presenting entrustable professional activities reflecting the main medical tasks that a physician must be able to perform autonomously on the first day of his residency and a third chapter listing 265 common clinical situations that a doctor is expected to deal with after passing the Swiss Federal Licensing Examination’.27 Each university then has the autonomy to organise its own undergraduate curriculum to fit with the objectives of PROFILES.
This study had four aims. First, to determine whether Swiss medical students are expected to acquire SEM-related skills and knowledge according to PROFILES. Second, to systematically review SEM teaching in the Swiss undergraduate medical curricula. Third, to determine if Swiss medical students are aware of SEM, and fourth whether they want it included in their curricula.
Method
PROFILES
Two authors (JC and TP) independently reviewed PROFILES for SEM-related learning objectives. A learning objective was considered SEM-related if it matched at least one key SEM domain of the ‘syllabus for the medical specialty of sport and exercise medicine’ written by the ‘International Syllabus in Sport and Exercise Medicine Group (ISSEMG)’.2 The key domain ‘intrinsic skills of an SEM physician’ covering ‘core skills which all physicians should learn during basic training’ was not taken into account here.2 A learning objective could match several key domains and all matches were recorded. A consensus meeting discussed all discrepancies between the two authors and if there was no resolution following this, a third author was asked to give judgement to form a conclusion.
Systematic review of SEM teaching in the Swiss undergraduate medical curricula
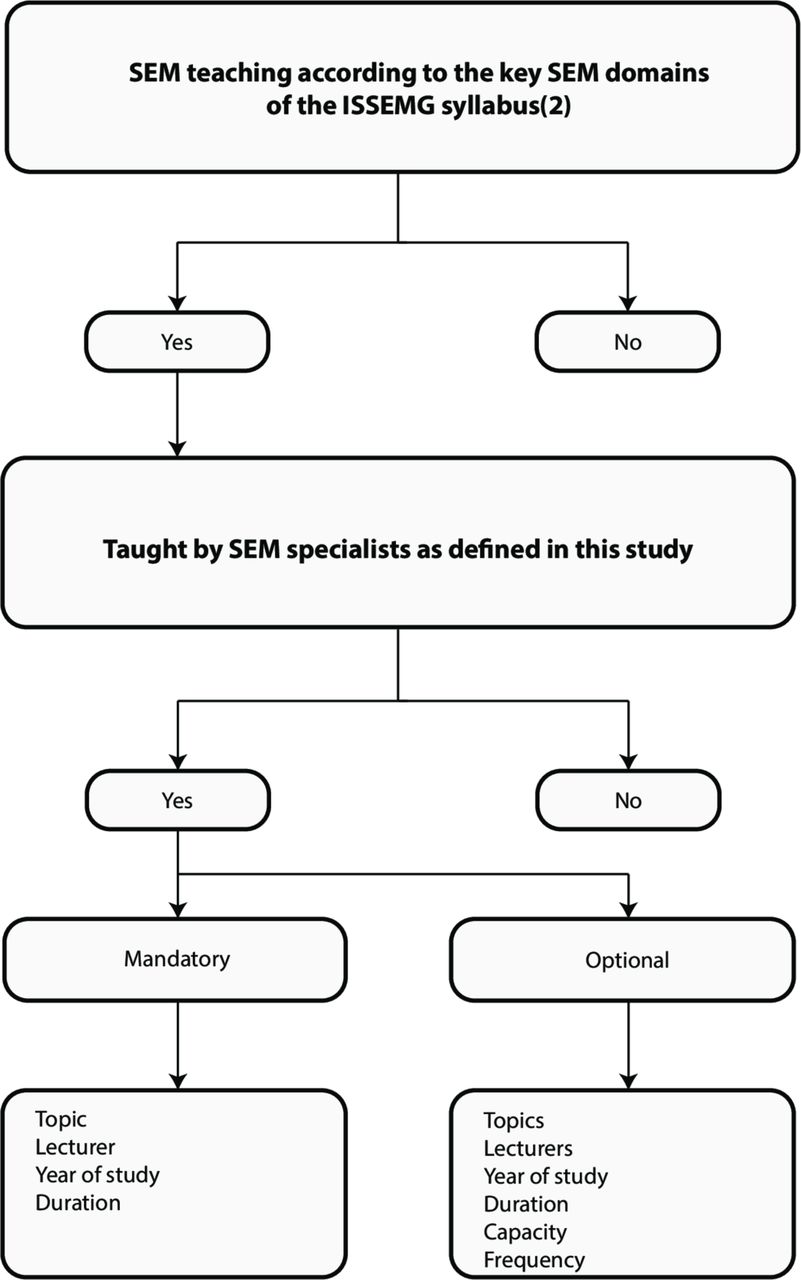
Two authors (JC and LN) independently reviewed the SEM teaching in the 2018–2019 curricula of the eight Swiss universities offering medical training. To be classified as SEM teaching, two criteria had to be fulfilled. First, the teaching title had to match at least one key SEM domain of the ISSEMG syllabus.2 Again, the key domain ‘intrinsic skills of an SEM physician’ was not taken into account.2 Second, it had to be taught by an SEM specialist. For this purpose, SEM specialists were defined as SEM doctors (medical specialists holding the subspeciality title of the Swiss Society of Sports Medicine), sports physiologists/scientists (graduates of sport physiology/sciences degrees), sports physiotherapists (physiotherapists holding the sports physiotherapy specialty of Sportfisio), sports psychologists (psychologists holding a postgraduate degree in sports psychology) and sports nutritionists (nutritionists holding the postgraduate certificate of the Swiss Sports Nutrition Society). SEM specialists holding equivalent foreign titles were considered too. A consensus meeting discussed all discrepancies between the two authors and if there was no resolution following this, a third author was asked to give judgement to form a conclusion. Finally, local leading SEM physicians were asked to check the accuracy of the results (except for the University of Neuchâtel, which does not employ an SEM physician).
As illustrated in figure 1, after being divided into mandatory and optional, teaching was further characterised according to topic(s) taught, lecturer(s), study year and duration. For optional teaching, class capacity and frequency were also recorded.
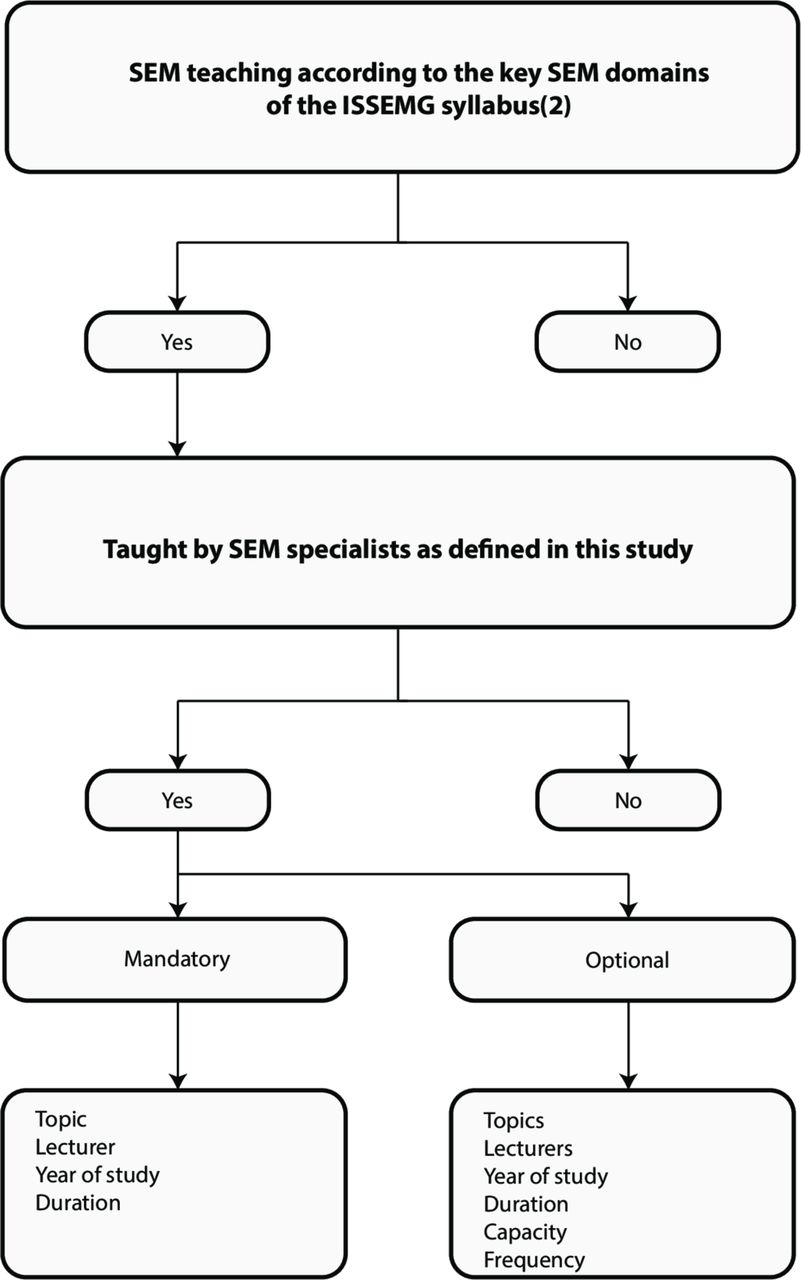
Systematic review process of SEM teaching in the Swiss undergraduate medical curricula (ISSEMG, International Syllabus in Sport and Exercise Medicine Group).
The medical curricula of the universities of Basel, Bern, Geneva, Lausanne, Neuchâtel and of the Swiss Federal Institute of Technology in Zurich (ETHZ) were accessible online.28–33 The curriculum of the University of Fribourg was not openly accessible online but access was provided by a local medical student.34 The University of Zurich, whose curriculum was not accessible online, was contacted but denied access to the authors for ‘data privacy protection’ reasons. Therefore, its curriculum was evaluated based on its description in the study years booklets.35
Survey
An online survey (www.evalandgo.com, France) was conducted between 21 April and 21 October 2017 among the 7708 Swiss medical students of the seven Swiss Universities offering medical training (the ETHZ Bachelor of Medicine was established in September 2017). Local medical students’ societies forwarded an e-mail twice, over a 6-month period, to all their students inviting them to participate in the survey. In addition, student members of the Swiss Society of Sport Medicine presented the survey to every year group studying in the universities in question, in a lecture.36
The first three questions of the survey aimed to characterise participants according to gender, university and study year distribution. Questions 4–8 aimed to determine their knowledge and teaching preferences in SEM. Answers were chosen from a list of predefined options. Answer options of question 5 were developed to match the definition of SEM provided by Jaques and Loosemore.1 Due to the multilingual nature of Switzerland, the survey was conducted in German and French. Results were directly processed by the online survey platform.
Sample size calculation
Assuming that the true proportion, p, of Swiss medical students that are keen to have SEM included in the undergraduate curricula is 0.5, a sample size of 366 students is necessary to estimate the proportion of a small finite population with a margin of error of 5% using a 95% CI as shown below.37

where p is the proportion of a small finite population, z is the  -quantile of a standard normal distribution, e is the margin of error and n is the population size.
-quantile of a standard normal distribution, e is the margin of error and n is the population size.
Comparison sample and population
Features available for both the sample and the Swiss medical student’s population (gender, university and academic level) were compared. χ2 tests were run to check if differences between both groups were significant.
Results
PROFILES
Table 1 shows that 32 SEM-related learning objectives were identified (eight general objectives, seven entrustable professional activities and 17 situations as starting points). All discrepancies could be resolved during the consensus meeting. The key domain ‘PA and human health’ could be matched with 20 learning objectives, while key domains ‘extrinsic skills of an SEM physician’ and ‘injuries related to sport and exercise’ could be matched with 13 and 11 learning objectives, respectively. Four others domains matched with learning objectives: ‘medical issues related to exercise’ (five matches), ‘nutrition’ (two matches), ‘specific groups undertaking sports and exercise’ and ‘sports team care and sports event medical management’ (one match each).
SEM-related learning objectives in profiles
Systematic review of SEM content in the Swiss undergraduate medical curricula
Mandatory and optional SEM courses are presented in tables 2 and 3, respectively. The authors agreed on all findings without the need for a consensus meeting. Four of eight universities display limited time and content, in mandatory SEM teachings. Four universities offer more comprehensive optional SEM courses. Local leading SEM physicians confirmed the accuracy of the results. Course content, which relates to exercise but did not meet inclusion criteria, is presented as a online supplementary file. This includes basic exercise physiology lectures and two lectures on sports injury and PA given by physiologists, orthopaedic surgeons and an epidemiologist, respectively.
Supplemental material
Mandatory SEM teachings in the Swiss undergraduate medical curricula
Optional SEM teachings in the Swiss undergraduate medical curricula
Survey
Sample size
1764 students participated in the survey (482.0% of the required sample size and 22.9% of all Swiss medical students). If the sample is considered a random sample, the margin of error would be 2% (calculated as shown below).37

where  is the
is the  -quantile of the standard normal distribution,
-quantile of the standard normal distribution,  sample estimate of the proportion, n is the sample size and N is the population size.
sample estimate of the proportion, n is the sample size and N is the population size.
Comparison sample and population
Figure 2 illustrates the response rate according to gender (A), university (B) and academic level (C). Panel D shows the sample distribution according to the year of study. χ2 tests show significant differences between the sample and the population regarding gender (χ2 (1)=35.6, p<0.01), university (χ2 (6)=112.6, p<0.01) and academic level (χ2 (1)=109.4, p<0.01).

{kind=link}
{kind=link}
Sample, population and response rate according to gender, University, academic level and study year. (A) response rate according to gender, (B) response rate according to university, (C) response rate according to academic level and (D) sample distribution according to study year. In panels (A–C), grey columns represent the number of students in the Swiss medical students’ population. In panels (A–D), black columns represent the number of students in the sample. Data on the top of each column are expressed in %. Given that the exact number of medical students in each study year was not available for all universities, it was not possible to calculate a response rate according to the year of study. The University of Fribourg offers only a bachelor of medicine, while the University of Neuchâtel offers only the first year of study. BS=University of Basel, BE=University of Bern, FR=University of Fribourg, GE=University of Geneva, LS=University of Lausanne, NE=University of Neuchâtel, ZH=University of Zurich and n=nth year of study.
Survey results
As indicated in table 4, the result for question 4 of 3.29 on a 5-point rating scale being just above the neutral value of 3 shows that students felt that they have limited understanding of SEM. Only 50.3% (n=887) and 67.2% (n=1186) of students associated SEM with treatment and prevention of chronic diseases, respectively. Conversely, about 90% of them considered medical care of athletes and sports-related health issues as part of SEM.
Questions 4–8 targeting SEM knowledge and preferences of the students. Several answers were allowed for questions 5 and 6, while only one answer was allowed for questions 4, 7 and 8
53.7% (n=948) of students expressed a desire for a mandatory SEM course, while 54.0% (n=953) would like an optional course in SEM. Finally, the result for question 8 of 4.05 on a 5-point rating scale shows that students would be motivated to follow SEM courses.
Discussion
The lack of SEM teaching at medical schools is a global concern, as highlighted by several recent publications from around the world.5 6 22 23 25 26 38–40 This study aimed to determine whether Swiss medical students are expected to acquire SEM-related skills and knowledge, to determine if SEM is currently taught in Swiss medical schools and finally to assess knowledge and interest of Swiss medical students regarding SEM.
32 SEM-related learning objectives were identified in PROFILES. 20 of them are related to the key SEM domain of ‘PA and human health’. It is noteworthy that PA, like other healthy habits (eg, tobacco abstinence), is not explicitly mentioned in PROFILES but included in terms like ‘health and lifestyle’. SEM-related general objectives mainly highlight the need to teach medical students about healthy lifestyles, while entrustable professional activities emphasise musculoskeletal examination and reviewing lifestyle choices. According to the entrustable professional activity EPA 7.1, a physician must be able to ‘incorporate the prescriptions of physiotherapy and physical rehabilitation, dietetic and lifestyle advice into the management plan’ on the first day of his residency. These results clearly show that SEM could and should be part of the Swiss undergraduate medical curricula.
Four of eight Swiss medical schools display very limited mandatory SEM teachings. Furthermore, it appears that the key SEM domain ‘PA and human health’ is not taught in Switzerland (with the exception of the University of Fribourg, offering lectures on ‘applied exercise physiology’). Four Swiss medical schools offer more comprehensive optional SEM courses, but the latter are only able to educate between 12 and 40 students a year. Despite the overwhelming evidence for its importance in primary and secondary prevention of most NCDs, the field of SEM has consequently been neglected in the education of future Swiss physicians.
While most students associate SEM with athletes’ care and sports-related health issues, only one in two realises that SEM physicians have the skills to treat patients with, or at risk of developing, NCDs. Given that SEM, and particularly exercise medicine, is currently insufficiently addressed at the Swiss medical schools, these results are not surprising. They do, however, bring cause for concern, as exercise medicine provides an evidence-based solution to one of the biggest current public health issues.41 Fortunately, about 95% of the participants are willing to be taught in SEM, which is consistent with the results of Osborne et al.23
Limitations
First, the systematic review excluded SEM content not taught by SEM specialists. The authors acknowledge that some non-SEM specialists might be competent in particular SEM topics (eg, orthopaedic surgeons in managing musculoskeletal injuries). Moreover, every medical specialty should ideally emphasise the health benefits of being physically active. However, now that SEM is an internationally recognised medical specialty, the authors advocate that SEM specialists should teach key SEM domains in medical schools worldwide.2
Second, the study year booklets, used to evaluate the curriculum of the University of Zurich, describe the topics taught and the lecturers involved, but do not list every single teaching session. Even if the leading SEM physician of the University of Zurich confirmed that the results were accurate, it is possible that SEM-related teachings could have been missed.
Third, students were contacted via their local medical students’ societies, which forwarded an e-mail to all of them. The University of Bern posted the information on their medical students’ website instead because the local students’ society was not permitted to forward the intended email. Consequently, as students from this university were not individually alerted to the study, it is possible that some of them were not aware this survey was ongoing.
Moreover, fifth year students of the universities of Basel, Bern and Zurich as well as sixth year students of the universities of Geneva and Lausanne were on placement all year round. Therefore, an oral presentation of the survey was not possible in these study years.
Next, a selection bias is likely, as students less interested in SEM may not have participated to the same extent as SEM interested students. However, even if the latter are over-represented in the sample, results show that students have limited understanding of SEM. Therefore, SEM understanding might be even lower in the Swiss medical student’s population.
Furthermore, the survey did not clarify whether or not participants followed SEM courses. Only a minority of students could possibly have participated in optional SEM courses. While more students took part in mandatory SEM courses, these are limited in time and content. Nevertheless, students that had followed SEM courses might be over-represented in the sample. Thus, the willingness to include SEM in the curricula might be lower in the population than in the sample; however, SEM understanding may be lower too.
To test sample representativeness, features having the potential to influence survey participation and outcomes should ideally have been compared between the Swiss medical students’ population and the sample. Such features could include individual weekly PA or injury history for example. Unfortunately, the only features available about the Swiss medical students’ population were gender, university and academic level distribution.42
In question 6, it was possible to check both mandatory and optional courses. 223 students would like either mandatory or optional SEM courses offered separately or both together, in their curriculum. Consequently, it is not possible to determine whether a mandatory or an optional SEM course is preferred.
Both women and bachelor students were over-represented in the sample. It has been reported that gender influences online survey participation, with women participating more than men.43 Bachelor students might be more open to new medical disciplines than master students (who often have a more elaborated idea which kind of specialities they want to pursuit).
Even though unlikely, it was theoretically possible to participate several times in the survey, by using multiple IP addresses.
Conclusion
PROFILES contains several SEM-related learning objectives, mainly linked to PA, while SEM is scarcely taught at Swiss medical schools. Despite striking evidence that PA promotion and prescription should be included in undergraduate medical training, this is still not the case in Switzerland. Swiss medical students have limited understanding of SEM with only one in two aware that exercise medicine is a part of SEM. An overwhelming majority of respondents in our survey would like to have SEM included in their curricula. Based on these results, Swiss medical schools should take steps to implement SEM into their curricula.
Acknowledgments
We thank the Swiss Society of Sports Medicine for their support, the board members of ‘Students & Junior Doctors SGSM/SSMS’ for their intellectual input, Dr Shona Kohlhardt (Sheffield University, United Kingdom) and Dr Flora Colledge (University of Basel, Switzerland) for linguistic support.
References
Footnotes
Contributors JC, AS-T and SK designed the screening and the systematic review, JC and TP screened PROFILES, JC and LN systematically reviewed the Swiss undergraduate curricula, JC, LN and SK designed the survey and JC conducted the survey. JC, TP, AS-T, DI and SK analysed and interpreted the data. JC, LN and SK drafted the work. TP, DI and AS-T revised it critically from an intellectual point of view. All authors approved the final version of the work and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The Swiss Society of Sports Medicine paid 394 Swiss Francs for the online Evalandgo account.
Competing interests JC is a board member of the Swiss Society of Sports Medicine and the president of its junior section called ‘Students & Junior Doctors SGSM/SSMS’, LN is a board member of ‘Réseau Romand de la Médecine de l’Exercice et du Sport’, TP is a board member of the UK ‘Undergraduate Sports and Exericse Medicine Society’ and SK is a past president of the Swiss Society of Sports Medicine.
Patient consent for publication Not required.
Ethics approval According to the Swiss Federal Act on research involving human beings (section one, article 2), an ethics approval was not necessary to conduct this anonymised survey of opinions containing no person identifiable data.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.