Article Text

Abstract
Objective Sildenafil is a pulmonary vasodilator that may reduce the decrement in endurance performance in moderate hypoxia. We assessed the efficacy of sildenafil to improve performance in hypoxia.
Data sources/eligibility Criteria We systematically searched electronic databases (until August 2018) for randomised trials comparing sildenafil with placebo. We also examined the effect of sildenafil on pulmonary artery pressure (PAP), cardiac output (CO) and pulse oxygen saturation (SPO2) compared with placebo in hypoxia. Fourteen studies were included; 210 subjects received sildenafil 40, 50 or 100 mg/day.
Results Sildenafil showed a large effect for decreasing PAP during exercise and at rest, a small effect for increasing CO during exercise and a moderate effect at rest, a moderate effect for increasing SPO2 and a small effect for improving performance. In a subgroup analysis, there was no statistically significant difference between 100 and 50 mg sildenafil dose on SPO2. Sildenafil had a moderate effect on increasing SPO2 and performance at terrestrial hypobaric altitude but only a small effect on both in normobaric hypoxia. Regression analysis showed that hypoxic dose (PO2) and metabolic rate do not account for a significant portion of the variance in effect size for sildenafil on PAP, CO, SPO2 and performance.
Conclusion This meta-analysis indicates that sildenafil reduces PAP, has a moderate to small effect on CO and SPO2, and no effect on performance.
- altitude
- exercise physiology
- physiology
- pulmonary
- performance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Research summary
What is already known?
Several studies have examined the effect of sildenafil on reducing pulmonary artery pressure (PAP), increasing oxygen saturation (SPO2) and improving endurance performance with varied results.
By reducing ventilation/perfusion mismatch, sildenafil may increase hypoxic maximum aerobic capacity by between 6% and 12%.
What are the new findings?
This meta-analysis found a large effect of sildenafil in increasing PAP, a moderate effect in increasing cardiac output and SPO2, and no effect on performance.
The type of hypoxia (normobaric vs hypobaric) and the level of hypoxia (FIO2) do not alter the effects of sildenafil.
Introduction
The pulmonary vasculature is dynamic, dilating and constricting through a complex mechanism that regulates lung perfusion to optimise pulmonary blood pressure and gas exchange. Pulmonary artery smooth muscle relaxation occurs when nitric oxide (NO) diffuses from the vascular endothelium to smooth muscle cells where it increases the formation of cyclic guanosine 3′, 5′ monophosphate (cGMP), which activates protein kinase G. This in turn decreases intracellular calcium concentrations, inhibiting the actin–myosin cross-bridge cycle, allowing the smooth muscle to relax. Phosphodiesterase-5 (PDE-5) is the main cGMP-hydrolysing enzyme.1 High levels of cGMP cause smooth muscle cell relaxation while the presence of PDE-5 causes vasoconstriction. Sildenafil is a PDE-5 inhibitor with a molecular structure similar to cGMP. By occupying binding sites on PDE-5, sildenafil prevents cGMP breakdown, increasing the concentration available for pulmonary smooth muscle relaxation.2
Sildenafil, a medication primarily prescribed for erectile dysfunction, benefits patients with heart failure because of its limited hypotensive effect on the systemic circulation. Sildenafil produces small but physiologically insignificant reductions (8/6 mm Hg) in systemic blood pressure (BP) while supine3 and has a modest effect on systemic vascular resistance (maximum decrease of 16%).4 One important note is that participants with the greatest baseline BP show the greatest reductions in BP when using sildenafil.5 Because the decrease in BP is so small, there is no change in heart rate (HR) associated with therapeutic doses (40–100 mg) of sildenafil.4 Brachial artery diameter and flow-mediated dilatation, both estimates of endothelial function, are unaffected in healthy participants by 50 mg of sildenafil.6 Sildenafil also appears to have very little impact on the coronary vasculature in healthy humans. Likewise, there is very little evidence that sildenafil has an inotropic effect in humans.4 7 There are no changes in cardiac output (CO) or cardiac index associated with sildenafil and sildenafil does not change the force of cardiac contraction or cardiac performance in patients with stable ischaemic heart disease at rest.4 In one study of the sympathetic activity of sildenafil, BP and HR were unaffected, while muscle sympathetic nerve activity and plasma catecholamine levels increased,8 an indicator that sildenafil may be causing sympathetic activation independently of its haemodynamic effects.
Sildenafil is a highly selective PDE-5 inhibitor.3 The difference in its effect on the systemic vasculature described above and on the pulmonary vasculature is the result of PDE-5 distribution throughout the body. As PDE-5 is highly prevalent in the pulmonary arteries compared with the coronary and systemic circulation,7 9 10 a greater impact on pulmonary artery pressure (PAP) compared with systemic BP is expected.10
In addition to its therapeutic use, sildenafil has been recently studied for its potential to enhance exercise performance, specifically in hypoxia. Athletes routinely compete at moderate altitudes 2000–4000 m) where they are exposed to decreased atmospheric pressure (Patm). Decreases in the PaO2 of oxygen (PO2) leads to decreased arterial O2 saturation (SaO2) and a significant and variable decrement in performance.11 Low arterial PO2 triggers hypoxic pulmonary vasoconstriction (HPV) of the precapillary blood vessels resulting in increased PAP and decreased CO that may lead to further reductions in SaO2 and therefore performance. If the HPV response contributes to a loss in SaO2, reversing it pharmacologically may help to maintain SaO2 and reduce the decrement in endurance performance experienced at altitude.
Ghofrani et al were the first to report the effects of sildenafil on exercise performance in hypoxia.12 They found a significant improvement in exercise capacity and hypothesised that sildenafil improved hypoxic exercise tolerance by blunting the pulmonary hypertensive response, decreasing PAP, and thereby reducing right ventricular afterload allowing an increase in CO. Since increases in mean power output during a time trial are directly related to performance outcomes, there is potential for sildenafil to be used as an ergogenic aid in endurance sport. Subsequent investigations of the effects of sildenafil on endurance performance in hypoxia using various doses of sildenafil, measures of endurance performance and fitness of participants have been inconsistent, with some showing a benefit12–14 and others showing no significant effect1 15 16 when compared with placebo.
Purpose
We aimed to systematically review studies of the efficacy of sildenafil on exercise performance in hypoxia in healthy humans by meta-analysis. We also evaluated the effects of covariates in study methodology on sildenafil’s effects on PAP, CO, SPO2 and endurance performance.
Methods
Identification of studies
A systematic literature review was carried out to identify original research investigating sildenafil use and exercise performance in hypoxia according to PRISMA guidelines and checklist. The online databases Medline (Ovid), PubMed and Web of Knowledge were searched up to August 2018. Keywords used in the search included (sildenafil) AND [(exercise) OR (performance)] AND [(hypoxia) OR (altitude)]. From each paper examined, references were manually reviewed for additional eligible research. Only peer-reviewed journal articles that reported original research using a randomised, placebo-controlled, cross-over design, on healthy human participants with sildenafil used in isolation and with a quantifiable measurement of exercise performance (V̇O2max test or time trial) were included. Studies without a measure of exercise performance were included if they had valuable haemodynamic measures (PAP, CO or SPO2) that would contribute to the secondary analysis and met the remaining criteria. To ensure bias was minimised within the systematic review, we did not deviate from the defined inclusion criteria and thoroughly evaluated related research, including existing literature reviews. A funnel plot analysis was performed to determine the possibility of publication bias.
Data extraction
Outcomes assessed in the statistical analysis included measures of exercise performance, CO during rest and exercise, systolic PAP during rest and exercise, and estimates of SaO2 using pulse oximetry (SPO2) during rest and exercise. Exercise performance data were obtained in the form of peak power output during maximal exercise or mean power during fixed duration efforts or as peak oxygen uptake (V̇O2) during exercise in hypoxia and normoxia. Mean, SD and sample size for each variable were extracted. When required, SD was calculated from 95% CIs using the equation (SD=√n×(upper limit–lower limit)/3.92). When median was reported, mean was estimated according to Hozo et al.17 If data were provided in a figure but not in numeric form, the authors were contacted and requested to provide values. If no response was received, figures were measured with a ruler to determine approximate values. If a study carried out repeated measures (eg, in multiple levels of hypoxia), only the most severe level of hypoxia was included in this meta-analysis as this would likely show the greatest effect of hypoxia and therefore, sildenafil. Hypoxic dose (PO2) was calculated from atmospheric pressure (Patm) and reported as fraction of inspired O2 (FIO2).18 If Patm was not reported and the study took place at sea level, 760 mm Hg was used. Percentage of VO2max was determined by calculating the fraction of maximum power output (W) that was maintained during submaximal exercise. If power output was not reported, V̇O2 data were substituted. If V̇O2 was not reported, age was used to calculate predicted maximum HR that was compared with test HR. Data are presented in this analysis in the form of mean (±SD).
Analyses
The standardised mean difference between placebo and sildenafil were determined with 95% CI using Comprehensive Meta-Analysis Software (Biostat, Englewood, New Jersey, USA). Given the small sample size (n<20) of all but one study (Jacobs et al, n=35),16 Hedges’ g was selected as the measure of effect size19 using the random-effects model (chosen because each study represents a unique sample population), with interpretations of magnitude set at small (>0.2), moderate (>0.5) and large (>0.8).20 The I2 measure of inconsistency was used to assess between-study variability.21 We chose values <30% to represent low heterogeneity, values from 30% to 60% to represent moderate heterogeneity and values >60% to represent high heterogeneity. Subgroup analysis was performed based on the exertion level: rest and exercise, the type of hypoxia: normobaric (NH) and hypobaric (HH), and sildenafil dose administered in each study: 50 mg and 100 mg. Meta-regression analysis was completed using test hypoxic dose and metabolic rate (percentage of maximal capacity) as variables.
Results
Descriptive data
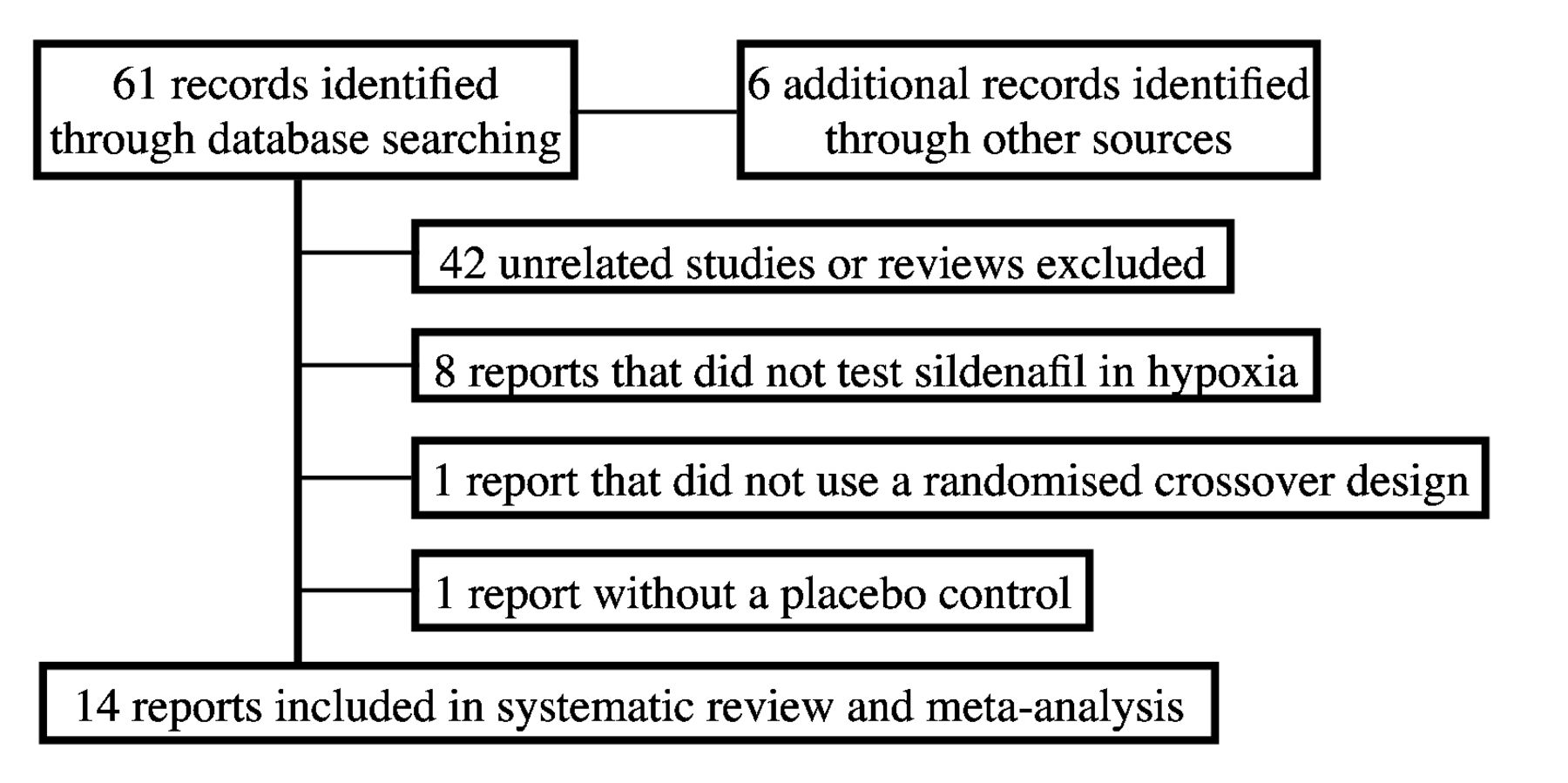
Sixteen studies of sildenafil use in hypoxia were originally identified (figure 1). Of these, two were excluded due to a lack of placebo control,22 or randomised cross-over design.23 The remaining 14 studies included 210 total participants (157 male, 53 female), shown in online supplementary table 1 (web appendix). Of these, four studies were included that had a measure of SPO2 or PAP but not a performance variable (n=42).24–27 All studies used a randomised cross-over design with a placebo and at least one sildenafil condition. Each data set was analysed separately. Each study recruited ‘trained’ participants; however, only nine studies reported V̇O2max values at sea level. Mean fitness levels ranged from 36.0 (±6.0) mL kg−1 min−128 to 68.6 (±8.0) mL kg−1 min−1.11
Supplemental material

PRISMA diagram for meta-analysis.
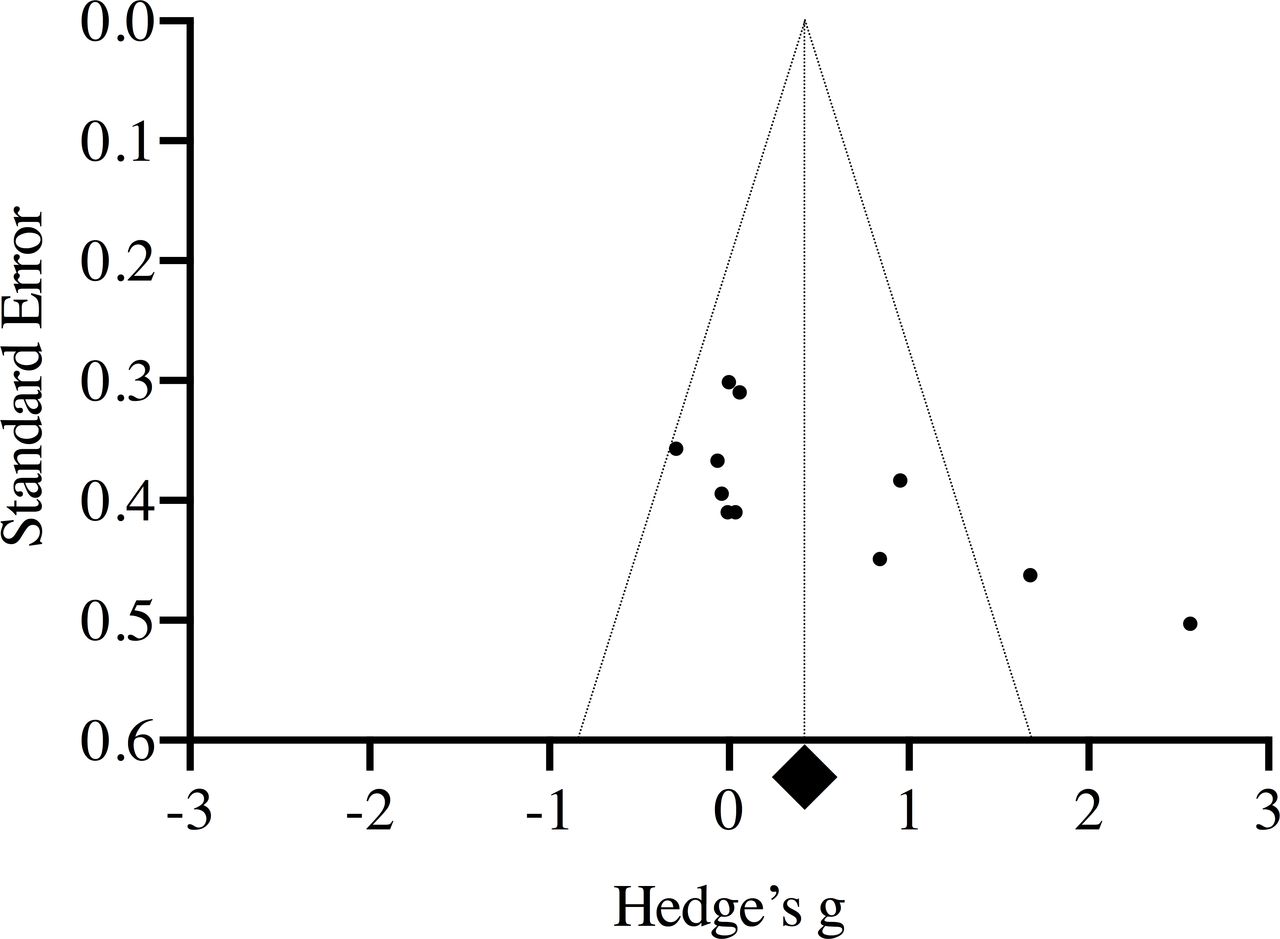
More than half of the research was conducted in NH, that is, manipulating FIO2 at a constant Patm. Only three studies used HH exposures13 24 29 where FIO2 is kept constant and Patm is reduced. One study used two levels of NH: moderate (MH, FIO2=0.162) and severe (SH, FIO2=0.128)1 though only the latter was included in our analysis. Sildenafil was administered in a 50 mg dose in all studies except two that used a 40 mg dose13 26 and three that administered 100 mg.24 25 30 Fourteen studies examined the effect of acute supplementation with prescription of sildenafil ranging from 30 to 120 min before exercise. The remaining study, by Richalet et al, used a 2-day supplementation protocol with 40 mg doses taken three times daily.13 Funnel plot analysis shows a potential asymmetry, suggesting the existing literature surrounding sildenafil and performance in hypoxia may be missing non-significant studies (figure 2).
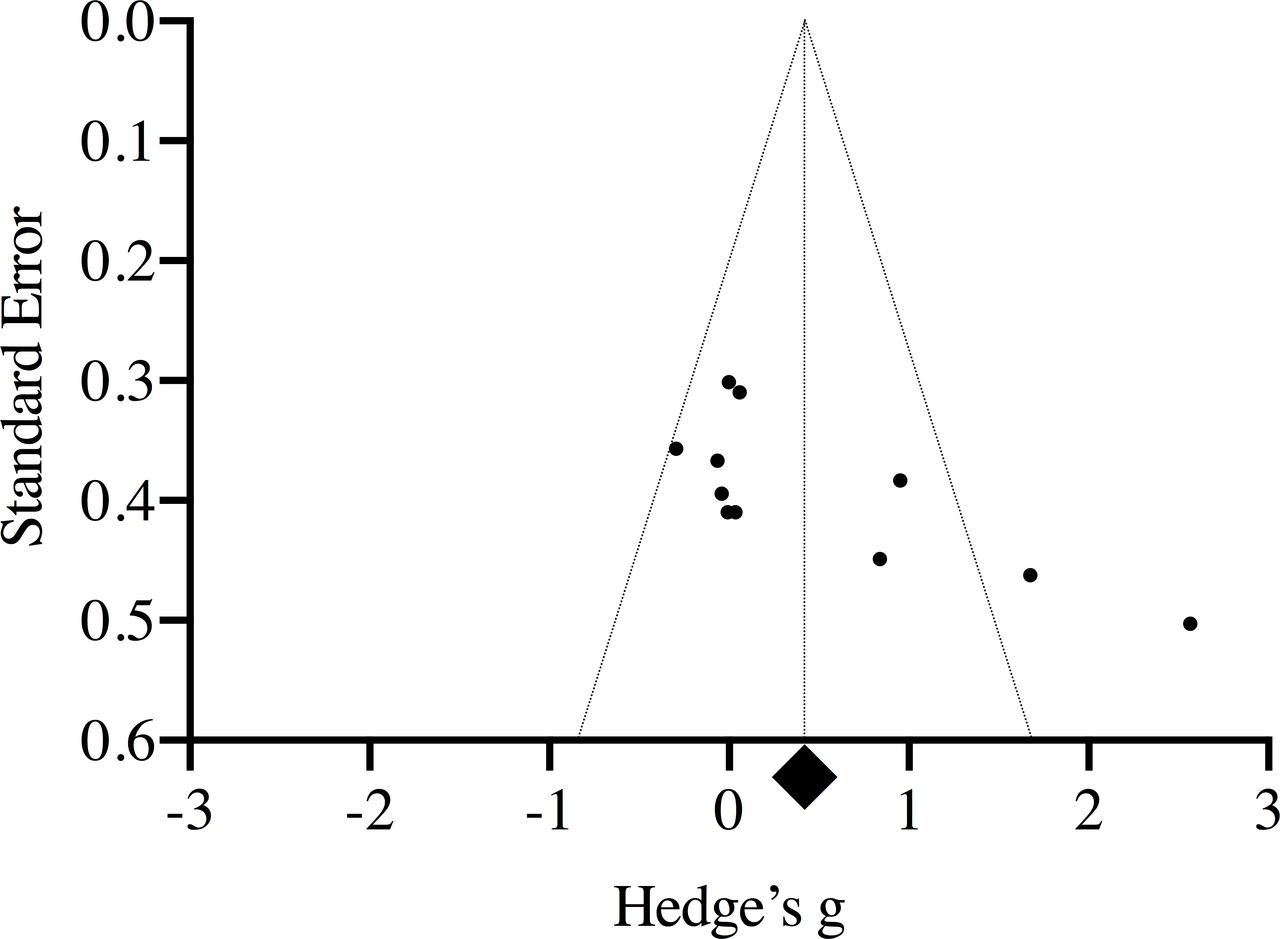
Funnel plot for publication bias.
Pulmonary artery pressure
PAP was evaluated in seven studies (figure 3) using the tricuspid jet method with six datasets at rest12 15 24 25 27 28 and four during exercise.12 13 24 28

Pulmonary artery pressure forest plot.
At rest, the pooled corrected effect size was −1.523 (95% CI −0.818 to −2.229) indicating a large effect in favour of sildenafil over placebo in reducing PAP with six of six trials reporting significantly decreased PAP at rest (p<0.05) and an I2 value of 76.0% (n=83).
For studies of exercising PAP, I2 was 81.5% (n=57). The pooled corrected effect size was −1.195 (−0.262 to −2.128) indicating a large effect in favour of sildenafil over placebo with three of four trials reporting significantly decreased PAP during exercise despite high heterogeneity.
Cardiac Output
CO was evaluated in nine studies with a total of 16 datasets (figure 4) using several different methods including impedance,1 13 14 16 nitrous oxide gas rebreathing,12 28 fingertip BP waveform analysis30 and echocardiography.11 15 Seven resting trials and nine exercise trials were included in the analysis.

Cardiac output forest plot.
For studies of resting CO, I2 was 65.3% (n=95). The pooled corrected effect size was 0.551 (0.059 to 1.042) indicating a moderate effect in favour of sildenafil over placebo with three of seven datasets reporting significantly increased CO at rest (p<0.05).
For studies of exercising CO, I2 was 29.4% (n=126). The pooled corrected effect size during exercise was 0.303 (0.011 to 0.595) indicating a small effect in favour of sildenafil over placebo with only two of nine datasets reporting significantly increased CO during exercise (p<0.05).
Oxygen saturation
Oxygen saturation was measured using pulse oximetry in 14 studies either during exercise or rest (figure 5). Three datasets were from studies conducted at altitude (n=36) and 12 datasets were from studies conducted in NH (n=189). In all trials (n=225), I2 was 43.7%. The pooled corrected effect size was 0.47 (0.22 to 0.73) indicating a moderate effect in favour of sildenafil over placebo.

Oxygen saturation forest plot. HH, hypobaric hypoxia; NH, normobaric hypoxia; SPO2, oxygen saturation.
Performance
Exercise performance (figure 6) was evaluated in 10 studies using either maximal exercise tests or time trials. The performance metric measured in each study is listed in (online supplementary table 1 (web appendix). All trials were conducted on an upright bicycle ergometer except for one that used a semi-supine (recumbent) position.12 Three trials were conducted at altitude (n=35) and five were conducted in NH (n=119). In all trials (n=154), I2 was 75.4%. The pooled corrected effect size was 0.474 (0.012 to 0.936) indicating a small effect in favour of sildenafil over placebo.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Performance forest plot. HH, hypobaric hypoxia; NH, normobaric hypoxia.
Subgroup analysis
Subgroup analyses were completed to evaluate the sensitivity to the dose of sildenafil and the type of hypoxic exposure. The most common dose of sildenafil used was 50 mg followed by 100 mg. Alternative doses are shown in online supplementary table 1 (web appendix) . Type of hypoxic exposure was classified as NH or HH for the SPO2 and performance datasets (also shown in online supplementary table 1 web appendix).
The only dataset with four or more sildenafil dose data points was SPO2 and the pooled corrected effect size for the 100 mg dose group was 0.343 (95% CI 0.715 to −0.029) indicating no effect in favour of sildenafil or placebo with zero of four datasets reporting significantly increased SPO2. The pooled corrected effect size for the 50 mg dose was 0.525 (95% CI 0.772 to 0.278), indicating a small effect in favour of sildenafil but one that was not statistically different from the 100 mg dose with only two12 15 of nine datasets reporting significantly increased SPO2.
For studies of SPO2 at actual altitude (figure 5), the pooled corrected effect size was 0.380 (95% CI 0.126 to 0.635) indicating a small effect in favour of sildenafil over placebo with zero of three trials reporting significantly increased SPO2 (p<0.05). For studies of SPO2 in NH, the pooled corrected effect size was 0.50 (95% CI 0.19 to 0.82) indicating a moderate effect in favour of sildenafil over placebo with only two12 15 of 12 datasets reporting significantly increased performance (p<0.05).
For studies of performance at altitude (figure 6), the pooled corrected effect size was 0.533 (95% CI −0.520 to 1.585) indicating a moderate effect in favour of sildenafil over placebo with one13 of three trials reporting significantly increased performance (p<0.05). For studies of performance in NH, pooled corrected effect size was 0.457 (95% CI −0.090 to 1.004) indicating a small effect in favour of sildenafil over placebo with two12 28 of eight datasets reporting significantly increased performance (p<0.05).
Regression analysis
The hypoxic dose (PO2) for every study was calculated from reported FIO2, PB and study altitude. For studies during exercise, the metabolic rate (% maximum) was determined. Both variables online supplementary table 1 (web appendix) were included in meta-regression to account for variance in each dataset (PAP, CO, SPO2 and performance). The p value for each covariate in each dataset is >0.05, indicating these covariates do not explain a significant portion of the variance in effect size.
Adverse events
Two studies reported minor headache in three participants.12 24 Kressler et al measured headache scores in all participants (using the Lake Louise Score) and found that participants who used sildenafil had slightly but not significantly higher headache scores.1 One subject reported flushing of the skin and no subjects reported any erectile response.24
Discussion
In our meta-analysis of the efficacy of sildenafil in decreasing PAP to increase CO, and thereby SPO2 and exercise performance, we found that sildenafil has a large effect in reducing PAP at rest and during exercise in otherwise healthy humans at altitude. From our analysis of the pooled data, this effect on PAP leads to a moderate increase in CO at rest and a small increase in CO during exercise, driven primarily by one study with a significant increase. A reduction of SaO2 is believed to be one of the primary determinants of the decrement in maximal exercise performance in hypoxia.31 Several studies have associated a reduction in SPO2 with the decrement in maximal exercise performance.31 Our pooled results showed a moderate increase in SPO2 with sildenafil driven by only two studies12 15 that showed significant increases. There was only a small effect of sildenafil in increasing performance. Our results indicate that as we successively examine the expected mechanisms of action of sildenafil on PAP, CO, SPO2 and finally performance, the effect size is reduced at each step. This finding indicates that the contribution to the decrement in performance at altitude from hypoxic pulmonary vasoconstriction (and the improvement in performance from sildenafil) is likely small. In addition to examining the overall effect of sildenafil and its effect on several variables that impact performance, we examined several methodological factors that might modulate the effectiveness of sildenafil on our outcome variables including sildenafil dose, type of hypoxic exposure, hypoxic dose and metabolic rate.
Subgroup analysis
Sildenafil was delivered orally in all studies ranging in dose from 40 mg to 100 mg acutely. It is unlikely that differences in effect size are due to dosage as the inhibitory concentration (IC50=3.5 nM) of sildenafil is very low, meaning a small dose is sufficient to significantly inhibit PDE-5.3 It is unknown if a multiday (chronic) dosing strategy is more efficacious compared with an acute dose for improving exercise performance. Only one study employed a full day loading protocol (three doses of 40 mg sildenafil over 24 hours before testing).13 The remainder of the studies in this analysis used an acute dose of either 50 mg or 100 mg and were included in a subgroup analysis of the SPO2 dataset that showed no significant difference between the two doses. This finding supports the conclusion that a supratherapeutic dose does not increase the likelihood of a benefit in SPO2 and therefore performance. A study examining the difference between acute and chronic dosing procedures, specifically in healthy exercising humans, may be useful to determine the effect of each on exercise performance. Serum cGMP was measured in only two studies. Snyder found that cGMP was significantly higher in the group treated with sildenafil28 while Richalet found that cGMP was non-significantly higher in the group treated with sildenafil at the timepoint (day 1) from which data were included in this analysis.13 Zhao et al did measure cGMP in murine participants in their study and found it significantly increased by sildenafil but did not measure cGMP in the human participants. Improved measures of the effect of sildenafil on PDE-5 inhibition would strengthen future research.
We looked at the effect of hypoxia on the outcome variables in two ways, first by examining the difference in the type of hypoxic exposure. The difference in the physiological response between equivalent PAO2 at differing PB (NH and HH) is a highly contentious one.32 The primary difference between NH and HH has been attributed to the density of air, which is lower in HH exposures, and may account for small differences in breathing frequency, dead space ventilation and total ventilation.32 The majority of the studies included in our research were carried out in NH; only three studies in the SPO2 and performance datasets used HH.13 29 30 There was no significant difference between the HH and NH pooled effect sizes on either SPO2 or performance indicating that the type of hypoxic exposure does not impact the effect of sildenafil on these variables. This finding is consistent with the mechanism of action of sildenafil, which should reduce PAP and not affect ventilatory responses.
Hypoxic dose varied between datasets attempting to simulate a variety of different altitudes. Studies in terrestrial altitude ranged from 2 m above sea level (control condition) to 5245 m. The fraction of inspired O2 ranged from 0.21 to 0.10. When the equivalent altitude PO2 was calculated, dose ranged from 104 to 70 mm Hg which represents an approximate range in simulated altitude from 2750 to 5500 m online supplementary table 1 (web appendix). Using meta-regression techniques in each dataset (PAP, CO, SPO2 and performance), we determined that differences in study PO2 (true or simulated altitude) did not account for variance in the outcome variables with sildenafil use. Further research at varying PO2 is necessary, however, because of the methodological heterogeneity described above.
It has been hypothesised that a threshold altitude may limit the usefulness of sildenafil at lower altitudes while allowing greater benefits above.1 Only one study examined the effect of sildenafil during exercise in moderate NH (~2100 m, 0.162 FIO2).1 The results closely match those of the non-responders in the study by Hsu et al and no improvement in performance was found. A longer (15 km) time trial was used to maximise the aerobic component of exercise. The authors concluded that below 3000 m, the HPV response does not increase CO enough for sildenafil to cause a recognisable improvement in performance and CaO2 is the primary limiting factor of performance. Unfortunately, because of the measurement technique used in the study, CO was measured in only 8 of 21 participants. Only one study was included at a PO2 equivalent to less than 3000 m,29 so our meta-regression does not test the existence of a threshold altitude below that limit. While it may be true that sildenafil is unlikely to be effective at improving endurance performance below 3000 m, it is more likely a continuum with very few participants who have a significant HPV response below that altitude who would then benefit from the effects of sildenafil.
The studies of exercise performance all used maximal exercise tests or time trials as their primary outcome while studies of PAP, CO and SPO2 used a mix of maximal and submaximal exercise. Maximal test protocol was described by Ghofrani et al12 as a stepwise increase in power with participants cycling to volitional exhaustion. Results were reported as power output (at V̇O2max) in watts except by Richalet et al, who reported the percentage decrease in V̇O2max compared with normoxia.13 For time trial studies, power was reported in mean wattage. Time trials varied in distance from 6 km to 16.1 km online supplementary table 1 (web appendix). Our meta-regression analysis showed that metabolic rate (as a percentage of maximum) did not account for the variance in the outcome variables with sildenafil use. While metabolic rate would have a significant impact on the absolute values for PAP, CO and SPO2, the effect of sildenafil on the variables was unaffected. In these exercise protocols, significantly different energy systems are used and metabolic variations could account for the differences in results, especially in trained athletes. It is possible that during submaximal exercise, a buffer may remain for sildenafil to increase CO while during maximal exercise, there is no additional capacity, so performance remains compromised.
Additional influencing factors
To complete our analysis, we considered several other factors that might modulate the effectiveness of sildenafil including the possibility of responders and non-responders, the influence of central regulation on exercise, and outlier studies. These concepts were not included in the statistical analysis but deserve mention.
Our results indicate that sildenafil is an effective pulmonary vasodilator in hypoxia that may increase CO but may not have a significant effect on overall performance outcomes in all athletes. Of particular interest is the 2006 study by Hsu et al. Several of the participants showed a significant improvement in time trial performance following sildenafil administration. These participants also showed an exaggerated decline in exercise performance in hypoxia.14 By grouping their participants according to those with a greater than or less than 1 min improvement in time trial performance between placebo and sildenafil, the authors classified participants as responders and non-responders. The responders had higher pulmonary vascular resistance (PVR) due to increased PAP and resultant increased RV afterload. In these participants, sildenafil improved performance by decreasing PAP and PVR, reducing RV afterload and improving V/Q mismatch. Non-responders had no such increases in PAP, PVR or performance after taking sildenafil. The authors also noted that the responders appeared to have a slightly (but not significantly) higher aerobic fitness level than non-responders. Criticisms of the study include the small sample size and the time trial distance (6 km). Kressler et al believe that a 6 km time trial may be too short with a minimal aerobic component such that it is not possible to detect performance improvements with sildenafil.1 These criticisms were supported by a study from the same research group as the Kressler paper, with a much larger sample size (n=35) and found no significant improvement in performance with sildenafil using a similar 6 km time trial protocol.16 Kressler acknowledges that responders (as described by Hsu) may represent only a small fraction of the population and may not have been included in the larger study.1 An attempt by Carter et al to compare the effect of sildenafil on performance with the decrement in performance caused by hypoxia found no correlation.11 No other study has sought to determine the existence of responders and non-responders while several showed no effect of sildenafil in all participants. It is possible that significant differences in methods related to sample population or exercise type may affect the outcome of the experiments, especially noticeable when dealing with the small margins that constitute differences in athletic performance at a high level. The potential for sildenafil responders requires further research with an emphasis on minimising methodological differences, perhaps by screening for participants with higher than normal pulmonary vascular resistance and increased PAP. Similarly, many of the studies included in this analysis included both male and female participants but no studies specifically examined any sex differences in response to sildenafil; this is an area that merits future research.
In individuals with increased PAP, determinants of performance, such as efferent commands to the heart and muscle, may be restricted by central mechanisms to protect the brain from hypoxia. If the athlete were to further increase CO, transit time might be reduced sufficiently to reduce SaO2 to the point that brain oxygenation is negatively affected. If the brain is centrally regulating exercise output in hypoxia, this might represent a protective mechanism that is circumvented by using sildenafil as an ergogenic substance. For this reason, future research should also consider the relationship between changes in performance in hypoxia and SaO2 and not just examine PAP.
Throughout our analysis, one study stood out as showing a strong effect of sildenafil on each outcome without any major methodological heterogeneity.12 Without the study by Ghofrani et al, the pooled effect of sildenafil on SPO2 and CO would be low. This study also contributed to the moderate to high I2 values. We believe it is important to note this as an outlying data point, and that its effect on the conclusion should be considered carefully. The potential lack of published negative studies would further skew the pooled effect towards a positive effect of sildenafil.
Limitations
Questions surrounding methodology remain; however, none of the studies we identified examine the relationship between increased PAP and decreased exercise performance in hypoxia or evaluated the effectiveness of sildenafil directly on the individual decrement in performance in hypoxia. Oxygenation is often unmeasured or left out from analysis despite being an important determinant of performance in hypoxia.
Conclusion
Sildenafil was investigated as an ergogenic substance during endurance exercise in hypoxia because it is believed that reductions in PAP will allow increases in CO and therefore exercise capacity through a reduction of right ventricular afterload. This meta-analysis reveals that while sildenafil is effective in reducing PAP, it has a moderate to small effect on CO and SPO2 and does not reliably affect performance. We can neither rule out a trivial, or truly nil, effect of sildenafil on performance. Thus, while PAP is moderately reduced due to sildenafil, other factors appear to be involved in regulation of exercise performance as well.
Future research must focus on (1) the mechanism through which HPV contributes to the decrement in exercise performance and (2) the relationship between decreased exercise capacity in hypoxia and increased capacity after sildenafil administration. Future studies should measure blood oxygenation, by ensuring pulse oximeter readings are reliable, or via arterial blood gas measurements, as well as consider monitoring muscle oxygenation so that investigators begin to understand all the factors that contribute to hypoxic exercise.
Acknowledgments
The authors wish to thank Dr William K Milsom for his contribution to the conception of this meta-analysis as well as his input on the manuscript.
References
Footnotes
Contributors EAC was responsible for conception of the meta-analysis, data collection, statistical analysis and preparation of the manuscript. KL assisted with conception of the meta-analysis, statistical analysis and manuscript preparation. WS assisted with conception of the meta-analysis and manuscript preparation. MK assisted with conception of the meta-analysis, statistical analysis and manuscript preparation. All coauthors have reviewed and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.