Article Text

Abstract
Introduction We tested whether physical activity (PA) engagement is subsequently associated with additional health-promoting behaviours in a large-scale, real-world programme leveraging technology and behavioural science to reward healthy lifestyle behaviours.
Methods In this observational, longitudinal study, we compared participants’ verified and self-reported health behaviours prior to and following their first verified engagement in PA recorded on the Vitality programme between 2014 and 2017.
Results Of 34 061 participants, the mean duration in the programme was 40.1 (SD 12.6) months, and the median time until the first PA was 13.1 (SD 16.6) months, with a mean age of 42.0 (SD 11.1) years and 14 881 (43.7%) being male. Baseline weekly PA minutes were mean 62.8 (SD 129.7), 98 (SD 26.0) and 282.9 (SD 230.0) for the low, moderate and high groups, respectively. In the 12 months following the first PA, the low group increased weekly active minutes by 156% (40 (95% CI 28.6 to 51.0) to 102 (95% CI 94.5 to 109.8)); the moderate group increased weekly active minutes by 60% (85.0 (95% CI 76.4 to 93.5) to 136 (95% CI 130.2 to 141.8)); and no change was seen for the high group. Overall, individuals exhibited an increase of 26% in their weekly active minutes from an average of 130 min (95% CI 121.2 to 139.4) to 164 min (95% CI 157.5 to 169.8). Overall, fruit and vegetable daily servings increased from 2.7 (95% CI 2.6 to 2.8) to 2.9 (95% CI 2.9 to 3.0); Kessler Stress Scores decreased from 17.4 (95% CI 17.2 to 17.6) to 17.0 (95% CI 16.9 to 17.1); sedentary hours decreased from 11.3 (95% CI 11.1 to 11.5) to 10.8 (95% CI 10.7 to 11.0); alcohol consumption decreased from 1.8 (95% CI 1.7 to 2.0) to 1.6 (95% CI 1.5 to 1.7) weekly units; sleep increased from 7.1 (95% CI 7.06 to 7.16) to 7.2 (95% CI 7.13 to 7.20) hours/night.
Conclusions PA was followed by other health-promoting behaviours. PA interventions should also evaluate the indirect impact on other health behaviours.
- physical activity
- risk factor
- cardiovascular
- nutrition
- sedentary
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What are the new findings?
In our longitudinal study, participants who engaged with the proprietary Vitality short-term incentives programme increased their physical activity (PA) and other health-promoting behaviours, including fruit and vegetable intake, time spent in sedentary activity (eg, in front of a screen), alcohol intake, sleep, stress and overall health scores.
How might they impact on future clinical practice?
Programmes that offer PA, for example, workplace programmes, should also evaluate the indirect impact on other lifestyle behaviours such as dietary changes.
Multibehaviour programmes may benefit from the synergy between healthy lifestyle behaviours.
Introduction
Physical activity (PA) is a leading contributor to death and disability arising from many chronic diseases. The WHO recommends that individuals undertake 150 min of moderate or 75 min of vigorous PA weekly, yet an estimated one in four people are not active enough.1
The WHO in its Global Action Plan on Physical Activity sets targets to reduce physical inactivity by 10% by the year 2025 and 15% by the year 2030.2 Yet, progress against this target is failing,3 and novel approaches to tackling physical inactivity are required.
The Vitality programme is a global behaviour-change platform that underpins insurance and corporate wellness products, which leverage technology and behavioural science to encourage and reward healthy lifestyle behaviours,4 5 including verified PA, healthy food purchases, screening for lifestyle risk factors and cancer, vaccination and other prevention activities. The Vitality programme has been demonstrated to increase healthy food purchases as well as reduce hospitalisation, length of hospital stays and overall healthcare costs in a variety of research studies.4 6
PA is a core behaviour incentivised by Vitality, but its impact on other healthy behaviours has not yet been studied. Previous studies in this field have been limited by offering only short-term interventions, being conducted in research rather than real-world settings, relying exclusively on self-reported rather than verified PA data and including inadequate sample sizes. This current study is novel in that it is large-scale, real-world, runs indefinitely and records verified PA.
The objective of the study was to test whether engagement in PA and additional health-promoting behaviours in a real-world setting increased over time.
Methods
This was an observational study of employee members who were enrolled in Vitality’s US-based programme (see online supplementary appendix A, B). We investigated whether earning PA points was followed by improvements in engagement with other health-promoting behaviour and health markers.
Supplemental material
Overall inclusion criteria required that participants had
Joined the Vitality programme before 31 December 2017.
Completed their first verified PA event on the Vitality platform between 1 January 2014 and 31 December 2017 (verified PA refers to any activity that can be verified through attendance at a participating member gym, an endurance event or tracked via a device including, but not limited to, Fitbit, Garmin, Polar, Apple Watch, Map My Fitness, as well as steps logged through one’s mobile telephone).
Completed at least two Vitality Health Reviews (VHRs, see online supplementary appendix B) during the study period: one prior to and one following their first PA event with at least 1 year between measures.
Additional inclusion criteria for analyses on the biological age differential and shifts in health behaviours required that participants had
Been eligible for the Vitality programme for a full programme, rather than calendar, year prior to and following the first PA event. As members have differing dates on which the programme runs, we have used the programme rather than the calendar year to adjust for this difference.
Members were categorised according to self-reported weekly PA at baseline prior to their first PA event as follows:
High PA: 150 min (moderate to vigorous intensity) (n=12 053 (35.4%)).
Moderate PA: 60–149 min (moderate to vigorous intensity) (n=8248 (24.2%)).
Low PA: 0–59 min (moderate to vigorous intensity) or only reporting low-intensity activity (n=13 760 (40.4%)).
Data for other behaviours and measures for the study were derived as follows:
Fruit and vegetable intake: average daily servings, self-reported data in the VHR.
Sleep: average hours per night, self-reported data in the VHR.
Stress score: Kessler Stress scoring undertaken as part of the VHR.
Sedentary time: average daily hours of sedentary activity, self-reported data in the VHR.
Alcohol intake: average weekly drinks, self-reported data in the VHR.
Smoking status: verified from cotinine testing at Vitality Check (in a subset of employers’ programmes).
Point-earning categories included
Education: online Vitality content (including nutrition courses, webcasts and other health-related topics).
Vitality reviews: reviews offered on the Vitality website, including the VHR, Mental Well-being Review and the Physical Activity Review.
Vitality Check: biometric assessment that includes fasting blood glucose, blood pressure, total cholesterol, Body Mass Index (BMI) and cotinine testing for smoking status. (All biometric screenings are conducted by accredited third-party laboratories. Vitality recognises a positive cotinine result as 10 ng/mL for saliva or blood and 50 ng/mL for urine.)
Prevention: includes dental screenings, influenza and other vaccinations, and other preventive health screening (including colorectal screening, mammography and cervical smears).
In order to provide a single composite score of health, a proprietary biological age calculation was used comprising 10 risk factors for BMI, total cholesterol, systolic blood pressure, diastolic blood pressure, fasting blood glucose, nutrition, PA, Kessler Stress Score, smoking and alcohol consumption.7 The biological age differential refers to an individual’s biological age minus their actual age at the time at which the health review is conducted. The lower an individual’s biological age differential, the lower his or her overall risk.
The VHR records self-reported responses on biometric health markers, PA, nutrition and lifestyle habits, mental well-being, and work and home life attributes. Completion of the VHR is optional but is incentivised as a point-earning activity and is typically completed annually. Individual member responses do not accrue points; consequently, regardless of an individual’s answers, the same number of points would be awarded.
Statistical analysis
All analyses were conducted using R V.3.4.3 (2017-11-30).
Dependent variables in the multivariate analysis included PA minutes; points earned for Vitality activities including education, reviews, biometric assessments, prevention; fruit and vegetable consumption; Kessler Stress Score; sleep; and smoking status. Age and sex were adjusted for in all comparative analyses and all reported p values. Data were not available for socioeconomic status (SEC) but as the data included only employed individuals, the variation in SEC was not expected to be considerable.
For all analyses, linear regressions were used. For categorical or binary variables, a random-effects logistic regression was used.
All Vitality members consented to enrolment for use of their data for research purposes in an anonymised format, making them exempt from ethics review.
Results
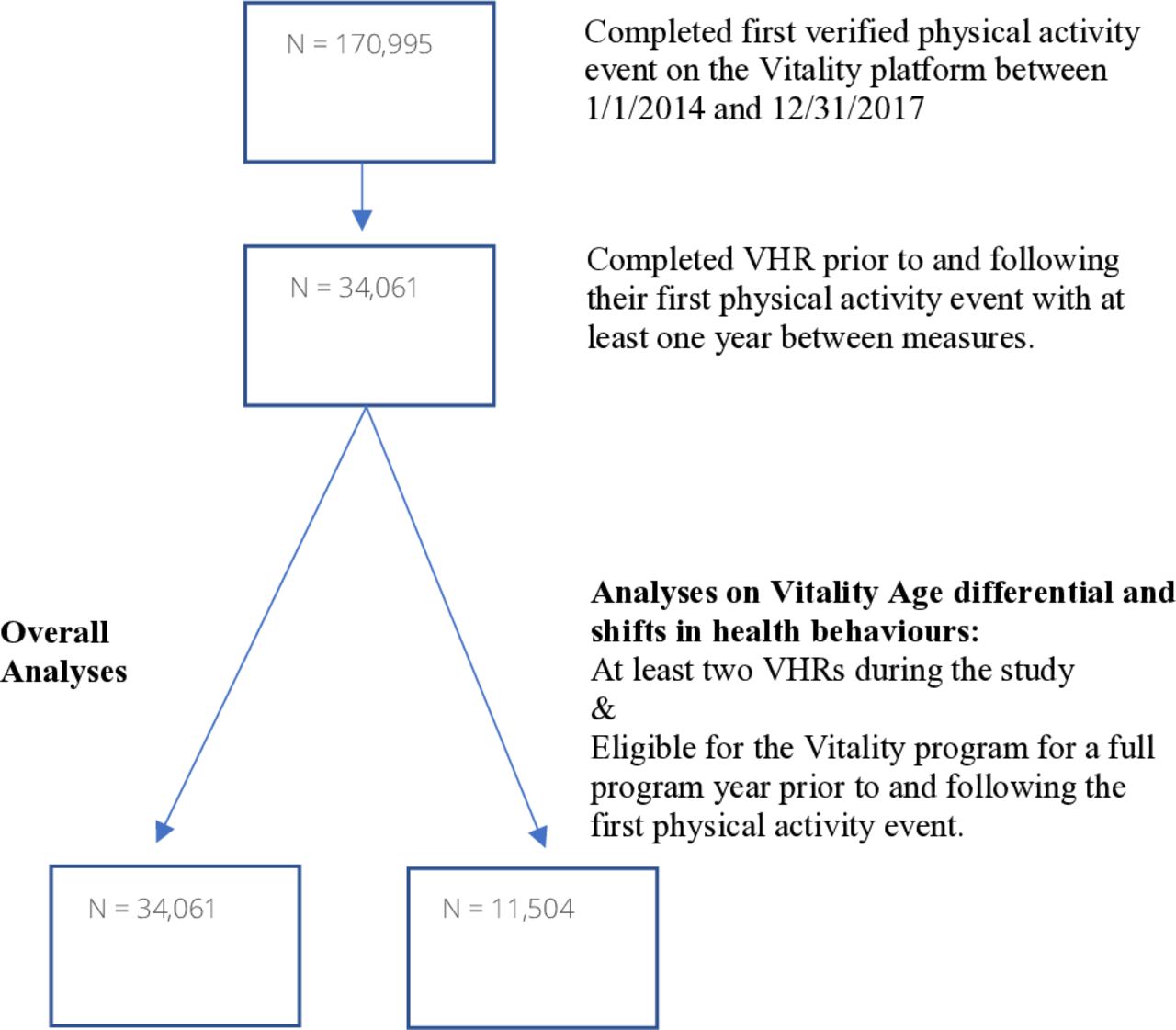
This study included 34 061 participants who met the baseline inclusion criteria; further analysis included subsets for trends in other healthy behaviours of 11 504 participants and cotinine testing of 6110 individuals (see figure 1). The mean duration on the Vitality programme was 40.1 (SD 12.6) months, and the median time until PA initiation was 13.1 (SD 16.6) months. Table 1 shows other baseline characteristics with a mean age of 42 (SD 11.1) years and 14 881 (43.7%) being male. Baseline levels of PA were 63, 98 and 283 min/week for the low, moderate and high activity groups, respectively.

Inclusion criteria. VHR, Vitality Health Review.
Baseline characteristics of partcipants by baseline PA level
Figure 2 reports the shifts in self-reported PA following PA initiation. Low PA members experienced an increase by 157% in weekly active minutes from an average of 39.8 min (95% CI 28.6 to 51.0) to 102 min (95% CI 94.5 to 109.8). The moderate PA saw an increase of 60.1% from 85.0 min (95% CI 76.4 to 93.5) to 136.0 min (95% CI 130.2 to 141.8). The high PA group had no significant change in active minutes. Overall, individuals exhibited an increase of 25.6% in their weekly active minutes from an average of 130.3 min (95% CI 121.2 to 139.4) to 163.7 min (95% CI 157.5 to 169.8).
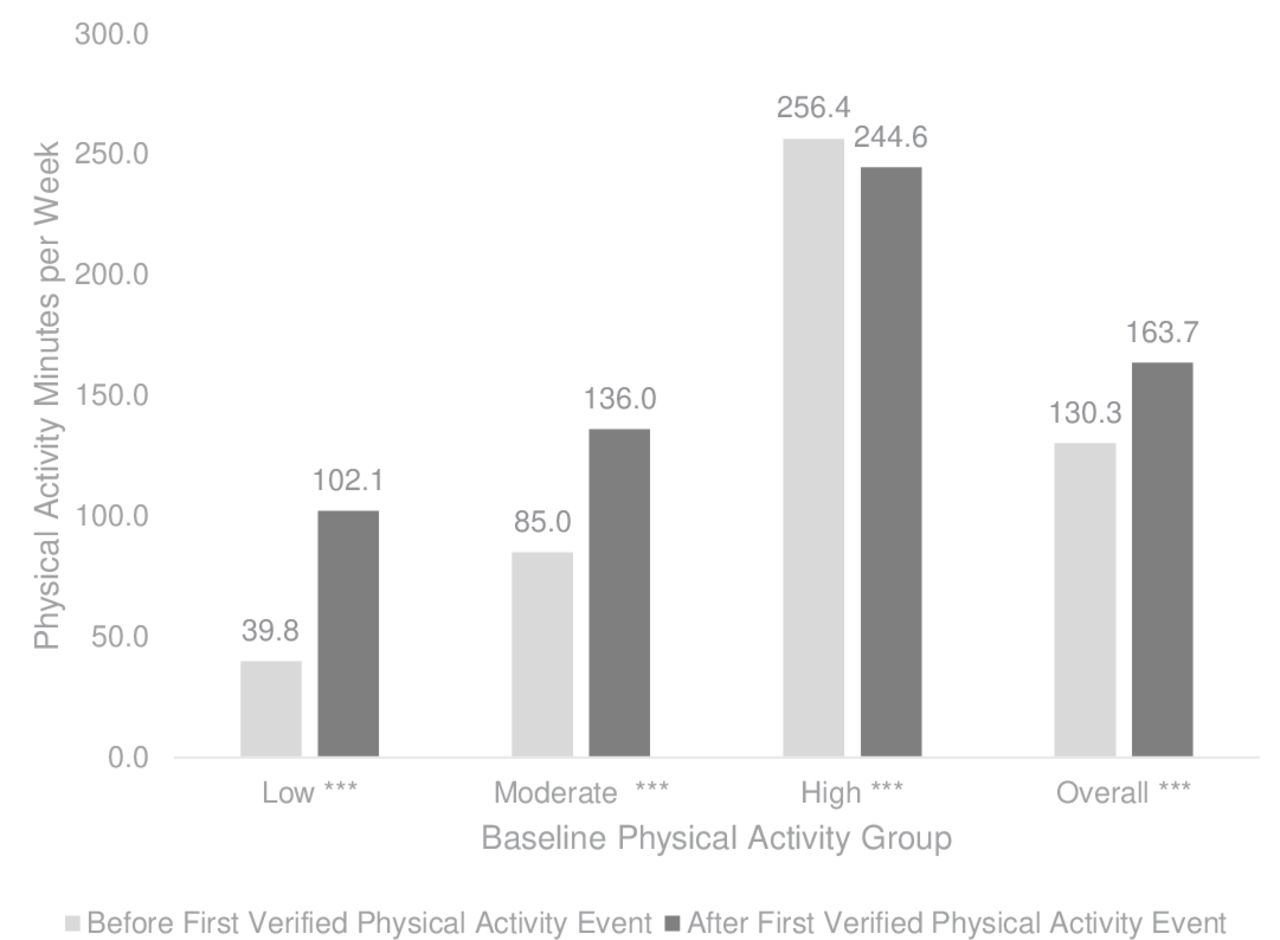
Shifts in weekly minutes of physical activity following physical activity initiation. Note: Adjusted p-values ***p <0.001.
Figure 3 shows that increases occurred in non-PA points earnt following PA initiation in all baseline PA groups, with increases of 55.0% in education points from 881.6 (95% CI 807.0 to 956.1) to 1366.5 (95% CI 1315.1 to 1417.8), 31.5% in review points from 874.0 (95% CI 844.7 to 903.3) to 1149.4 (95% CI 1129.3 to 1169.6), 40.7% in verified biometric health check points from 1605.8 (95% CI 1489.3 to 1722.4) to 2260.0 (95% CI 2179.7 to 2340.3) and 238.4% in prevention points from 25.5 (95% CI 0.3 to 50.8) to 86.4 (95% CI 69.0 to 103.8).
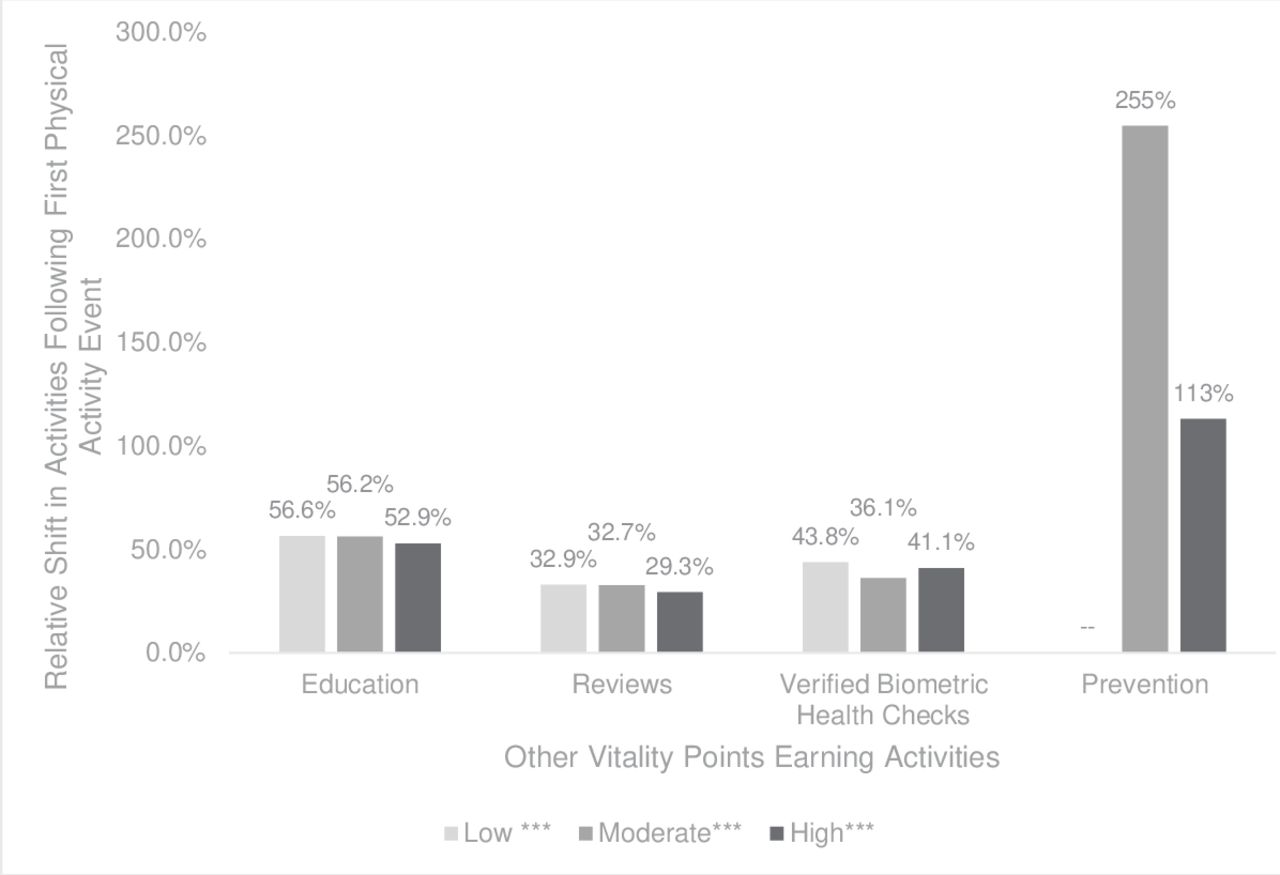
Shift in other point-earning activity following physical activity initiation, by baseline physical activity. Note: ***p <0.001. Improvements for prevention activities amongst the low group have not been included due to the scale but exhibited a shift from 0 to 59.7 Vitality Points.
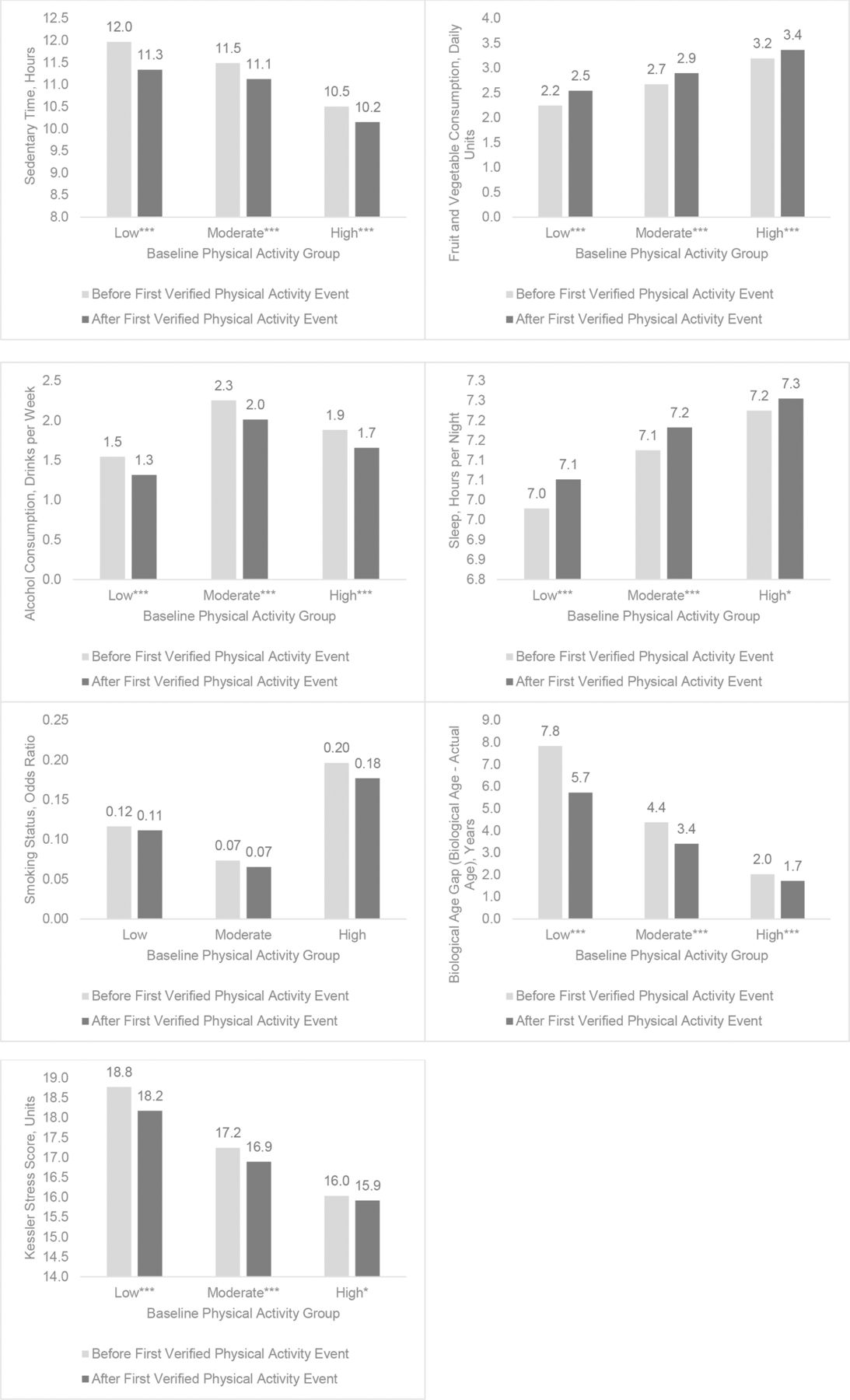
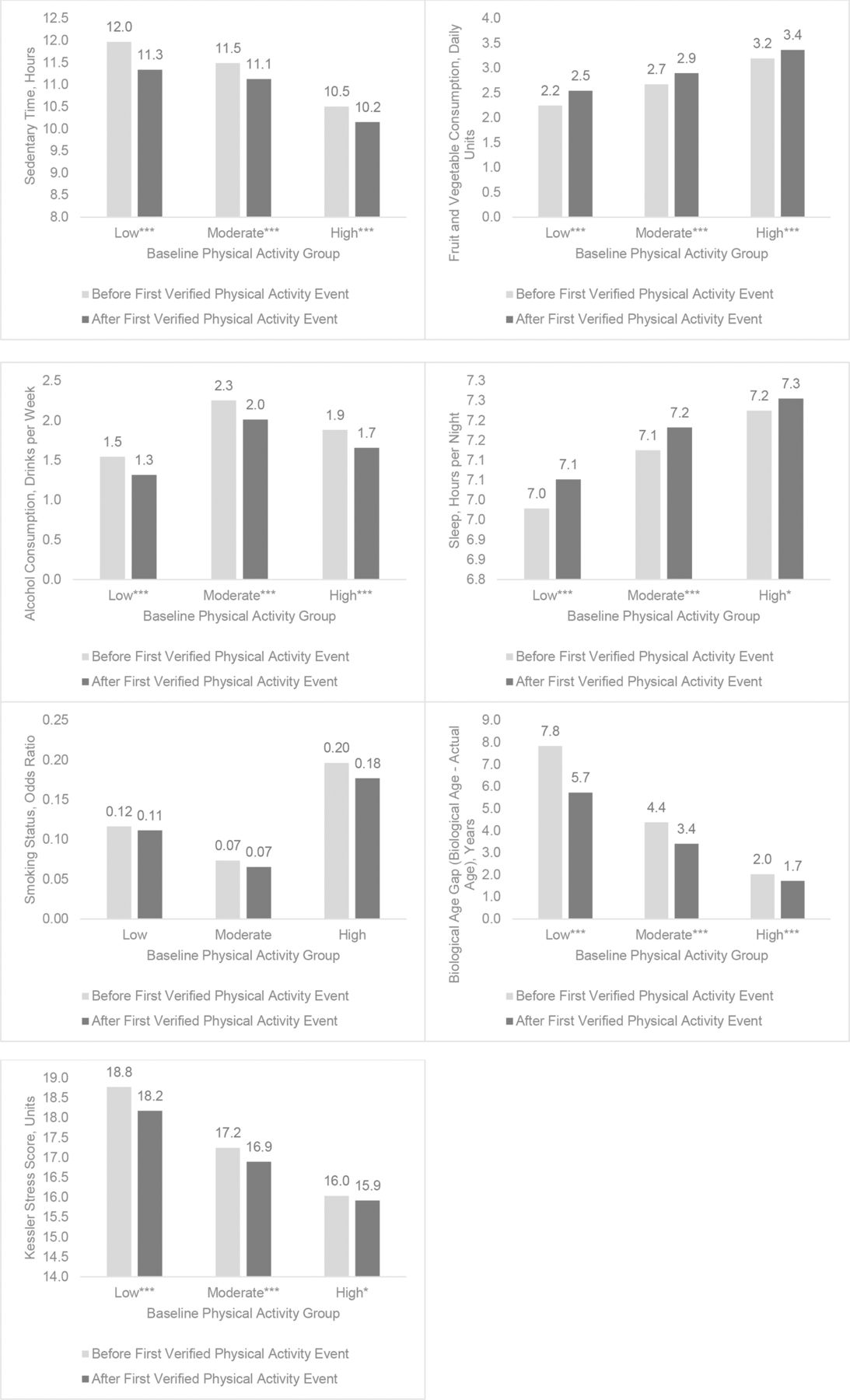
Figure 4 shows the shifts in other health behaviours following PA initiation. Significant improvements were seen for fruit and vegetable intake, increasing from 2.7 (95% CI 2.6 to 2.8) to 2.9 (95% CI 2.9 to 3.0) servings per day; sedentary hours, decreasing from 11.3 (95% CI 11.1 to 11.5) to 10.8 (95% CI 10.7 to 11.0); alcohol consumption, decreasing from 1.8 (95% CI 1.7 to 2.0) to 1.6 (95% CI 1.5 to 1.7) drinks per week; Kessler Stress Scores, decreasing from 17.4 (95% CI 17.2 to 17.6) to 17.0 (95% CI 16.9 to 17.1); and sleep, increasing from 7.1 (95% CI 7.1 to 7.2) to 7.2 (95% CI 7.1 to 7.2) hours. There was no significant shift in smoking status. The low PA group exhibited the greatest normalisation of their biological age differential by 2.1 years with a decrease from 7.8 (95% CI 7.6 to 8.0) to 5.7 (95% CI 5.6 to 5.8) years.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Shifts in biological age and other behaviours following physical activity initiation. Note: All values have been adjusted for age (except for mean vitality age minus actual age) and gender. ***p <0.001, **p <0.01, *p <0.05 (parameters without asterisks are not statistically significant).
Discussion
This study of over 34 000 Vitality members found that following a first PA engagement, participants increased their weekly PA and improved their education, prevention, health reviews and verified biometric health checks. In the year following PA initiation, participants showed a significant improvement in fruit and vegetable intake, sedentary time, alcohol consumption, sleep, stress and overall composite health scores. The improvements were greatest in those with the most to gain, those with low baseline PA levels.
Our study extends previous findings that health behaviours such as PA, healthy eating, and abstaining from alcohol and smoking tend to co-occur in individuals,8 9 and the presence of one healthy behaviour is followed by other healthy behaviours.10 However, the literature is sparse on the temporality of these shared behaviours. One randomised controlled trial found initiating an exercise intervention promotes engagement in fruit and vegetable consumption.11 The relationship may be mediated by changes in the strength of the habit formed towards exercise, suggesting individuals may be more likely to invest further towards healthy behaviours in other domains once they have developed a PA routine. Other research has shown how an exercise intervention can increase self-determination and motivation, which can facilitate subsequent changes in healthy eating behaviours, known as a transfer effect.12 While there are also studies that have found increases in PA cannot directly explain subsequent dietary changes,13 14 existing research suggests engaging in one health behaviour may alter social cognitive beliefs that influence one’s motivation, regulation and perceived mastery related to other health behaviours. To our knowledge, the current study is one of the largest studies to report findings on verified PA being followed by improvements in health markers, such as stress scores, in a real-world setting.
This study is one of few to quantify both PA and sedentary activity simultaneously and has shown that, following PA initiation, sedentary time (eg, time spent in front of a television or computer screen), independent of leisure time PA, is reduced by 4% overall and by 6% in the low PA group. The British Heart Foundation reported that despite a majority of adults being able to meet leisure time PA recommendations, the majority of these same individuals remain sedentary.15 Sedentary behaviour has been shown to be strongly associated with poor health, irrespective of overall PA levels, and conversely, individuals who reduce their sedentary levels have shown tangible modest weight loss.16
Interventions targeting health behaviours have used a wide variety of strategies, including various behaviour-change techniques, informational messaging, social marketing, environmental changes and policies.16 Whether targeting BMI, PA or eating behaviours, most behavioural interventions measure and report the impact on a single health behaviour,17 whereas the findings from the current study suggest improvements in other aspects of health co-occur and should be included in the evaluation of impact from the programme.
Strengths and limitations
This is one of the largest studies, with over 34 000 participants, to report on PA being followed by other healthy behaviours and is the first to report a positive impact on a broader range of other health behaviours. Another strength is that the PA levels are more accurate as they are verified rather than self-reported. Other measures, however, such as fruit and vegetable intake, were self-reported and may have been overestimated. However, this would be partly accounted for by comparison of the self-reported behaviours before and after the first PA event in the same individuals, using the same measurement tools.
As the current study is an observational study design, randomisation being infeasible in such a real-world setting, it is unable to eliminate issues such as selection bias and confounders.
The difference in characteristics and traits according to baseline PA level suggests there may be an inherent bias such that those who are physically active are also more likely to be engaged in other healthy behaviours at the outset, regardless of the Vitality programme initiatives. This study, however, reports on a temporal change in healthy behaviours for the same members before and after their PA event, thus reducing the impact of selection bias.
Conclusions
The impact of PA interventions in organised programmes may also manifest in changes in other healthy behaviour. Given the results of the current study, those who implement PA interventions should consider evaluating broader success measures than PA alone. Multibehavioural interventions may have greater impact by staggering PA to precede interventions for other behaviours.
References
Footnotes
Twitter @cotherhajat
Contributors DY and CH were responsible for conducting the study. DK was responsible for statistical analysis. ES, CH and DK were responsible for manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests At the time of writing, DK and DY were paid employees, CH and ES were paid contractors for the Vitality Group, which provides commercial wellness initiatives. DK has no financial disclosures. ES and CH have received consulting fees from Teva Pharmaceuticals for work on multiple chronic conditions. DY is currently the founder and president at the Foundation for a Smoke Free World, has been a paid employee at PepsiCo, and has provided paid consultancy/advisory services to Mars, PepsiCo, Astra-Zeneca, Novo-Nordisk, AB Inbev, Tesco and Teva Pharmaceuticals.
Patient and public involvement statement The Vitality programme is direct to consumer and regularly takes feedback into account for programme offerings and design. Vitality members are informed and consented for participation in research during their enrolment into the programme.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.