Article Text

Abstract
Objective It has been suggested that the mechanism behind cardiac troponin elevation after strenuous exercise is passage through a cell membrane with changed permeability rather than myocardial cell death. We hypothesised that an increase of cardiac specific myosin heavy chain-alpha (MHC-α; 224 kDa compared with cardiac troponin T’s (cTnT) 37 kDa) could hardly be explained by passage through a cell membrane.
Methods Blood samples were collected from 56 athletes (15 female, age 42.5±9.7, range 24–70 years) before, directly after and on days 1–8 after an Ironman. Biomarkers (C reactive protein (CRP), cTnT, creatine kinase (CK), MHC-α, myoglobin (MG), creatinine (C) and N-terminal prohormone of brain natriuretic peptide (NT-proBNP) were measured.
Results The course of MHC-α concentration (µg/L) was 1.33±0.53 (before), 2.57±0.78 (directly after), 1.51±0.53 (day 1), 2.74±0.55 (day 4) and 1.83±0.76 (day 6). Other biomarkers showed a one-peaked increase with maximal values either directly after the race or at day 1: cTnT 76 ± 80 ng/L (12–440; reference<15), NT-proBNP 776±684 ng/L (92–4700; ref.<300), CK 68±55 µkat/L (5–280; ref.<1.9), MG 2088±2350 µg/L (130–17 000; ref.<72) and creatinine 100±20 µmol/L (74–161; ref.<100), CRP 49±23 mg/L (15–119; ref.<5).
Conclusion MHC-α exhibited a two-peaked increase which could represent a first release from the cytosolic pool and later from cell necrosis. This is the first investigation of MHC-α plasma concentration after exercise.
- cardiovascular medicine
- sports and exercise medicine
- physiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the findings?
A full distance Ironman triathlon leads to temporal muscle injury, inflammation activity, worsening of kidney function and cardiac strain.
In 98% of participants, cardiac troponin T was above the cut-off value for myocardial infarction.
Myosin heavy chain-alpha (MHC-α) exhibited a two-peaked increase which is not compatible with the changed cellular wall permeability hypothesis but rather reflects myocardial cell death.
How might it impact on clinical practice in the future?
This is the first report on MHC-α increase after exercise and the results do not give a final answer as to the mechanism of increase of cardiac biomarkers under these circumstances.
Further research into MHC-α and other cardiac biomarkers has to be done.
Introduction
High volumes of endurance exercise have been found to be associated with right ventricular dilatation,1 inflammation,2 atrial fibrillation,3 myocardial fibrosis1 and accelerated coronary artery calcification.4 The terms ‘cardiac overuse injury’,5 ‘extreme exercise hypothesis’6 and ‘cardiotoxic effects of exercise’7 have been coined to describe the possible negative effects of very high level endurance exercise. However, most questions regarding the possible repetitive injury to the heart through high volume endurance exercise and their clinical consequences are unanswered and the different observations have yet to be put together to a fitting theory.8 9 One of the vexing observations which has been known for several decades is the phenomenon of troponin elevations after exercise,10 namely after marathon,11 triathlon12 13 or ultrarunning.14 Troponin elevation after exercise marathon has been reported since at least the 1990s to varying extent.10 Some authors have tried to explain troponin rise with temporal changes of the permeability of the heart muscle cell membrane and subsequent release of free troponin molecules into the bloodstream rather than heart muscle cell death.9 15 Several other explanations for troponin appearance in plasma have been suggested without succeeding in giving a clear cut answer to the question whether troponin leakage is a benign or malign phenomenon in this setting.16 Despite the intensity of this troponin debate, the answer seems as far away as when the phenomenon was first described.17
Cardiac TnT is a small molecule (37 kDa) while cardiac-specific myosin heavy chain-alpha (MHC-α) is much larger (224 kDa). MHC-α is occurring predominantly in atrial muscle but as well in ventricular muscle.18 An increase of MHC-α after exercise could, as we hypothesise, hardly be explained by passage through an intact cardiac cell membrane. Therefore, we measured MHC-α before and after a full distance Ironman.
Methods
Study population
The Kalmar Ironman 2016 had about 2500 participants and is a full distance triathlon consisting of 3.86 km open water swimming, 180 km cycling and 42.2 km running. A volunteer sample of 56 apparently healthy non-elite athletes was included in the study. Since we did not have a statistical hypothesis, we chose the number of volunteers based on convenience and the results of the Kalmar Ironman 2015 and the selection on willingness to come for blood samples a week before and up to 1 week after the race.13 All participants underwent anamnesis, blood pressure measurement and ECG. Written informed consent was obtained from all participants.
Biomarkers
Biomarkers (high sensitive C reactive protein (hs-CRP); cTnT, creatine kinase (CK), myoglobin (MG), creatinine (C) and N-terminal prohormone of brain natriuretic peptide (NT-proBNP) were measured by accredited laboratory methods 5–7 days before, directly after (within 15 min of passing the finish line), as well as day 1 (8–12 hours after the race) and day 5–8 after the race. In n=12 participants, additional blood samples for MHC-α and cTnT were taken on days 2, 3 and 4. MHC-α concentration was measured with a commercially available ELISA (Cloud-Clone, Houston, Texas, USA) with no reported cross reactivity with other myosins.
Runners gave a resting prerace venous blood sample 5–7 days prior to the triathlon. Postrace blood samples were taken within 15 min of runners completing the race by escorting the runners into the investigators tent (50 m after finish line). For both prerace and postrace samples, 10 mL of blood was extracted from the antecubital vein. Whole blood was then stored in Gel (SST gel) BD vacutainers and analysed within 4 hours of collection. For MHC-α, serum was frozen at −80°C and analysis was done within 2 months from collection. CTnT was analysed using an electrochemiluminescence assay (Roche; Basel, Switzerland). This had a limit of blank of 3 ng/L, limit of detection of 5 ng/L, upper reference limit (URL) based on the 99th percentile of 14 ng/L and coefficient of variation at URL of <8%.
Statistical analysis
All continuous variables are presented as the mean (SD) and range, and categorical variables as counts (%). Analyses were performed using Statistica software, V.12 (Statsoft, Tulsa, USA). P<0.05 were considered to indicate statistical significance.
Results
Of the 56 non-elite athletes (15 female, 41 male; age 42.5±9.7, range 24–70 years), 52 finished the race (14 female, 38 male; age 42.1±9.7; range 24–70) and were included in the final analysis. The main laboratory findings are summarised in table 1.
Biochemical parameters, 5–8 days before, directly after, 1 day after and 5–8 days after the race (n=52)
A full distance Ironman triathlon leads to disturbances in several biomarkers indicating temporal muscle injury, inflammation activity, worsening of kidney function and cardiac strain. Almost all participants had pathological values in CK and myoglobin directly after the race and on the day after, with CK values as high as 280 µkat/L and myoglobin up to 17 000 µg/L, thus more than 40 times the upper limit of CK and more than 200 times the upper limit of myoglobin. Rhabdomyolysis was accompanied by a decrease in renal function: the glomerular filtration rate (GFR) was reduced from 83.8±8.1 mL/min/1.73 m2 (creatinine-based) before the race to 71.0±13.2 mL/min/1.73 m2 directly after the race. The GFR had returned to normal in all but one athlete on days 5–8. The same was observed when using a cystatin-C-based GFR estimate: The values went from 91.0±0.4 mL/min/1.73 m2 before the race to 84.8±10.0 mL/min/1.73 m2 directly after the race. Values had returned to normal in all athletes at days 5–8. We have earlier published data on Kalmar Ironman 2015 where significant differences between men and women were observed in several biomarkers including myoglobin, CK and creatinine.13 These differences were confirmed in the 2016 Ironman (data not shown).
The longest lasting effect of the race on biomarkers was observed for hs-CRP which was normal in all but one athlete before the triathlon, peaked at day 1 after the competition (up to 60 times the upper normal range) and was still elevated above the upper reference level in 25 (48%) of participants at days 5–8 (table 1).
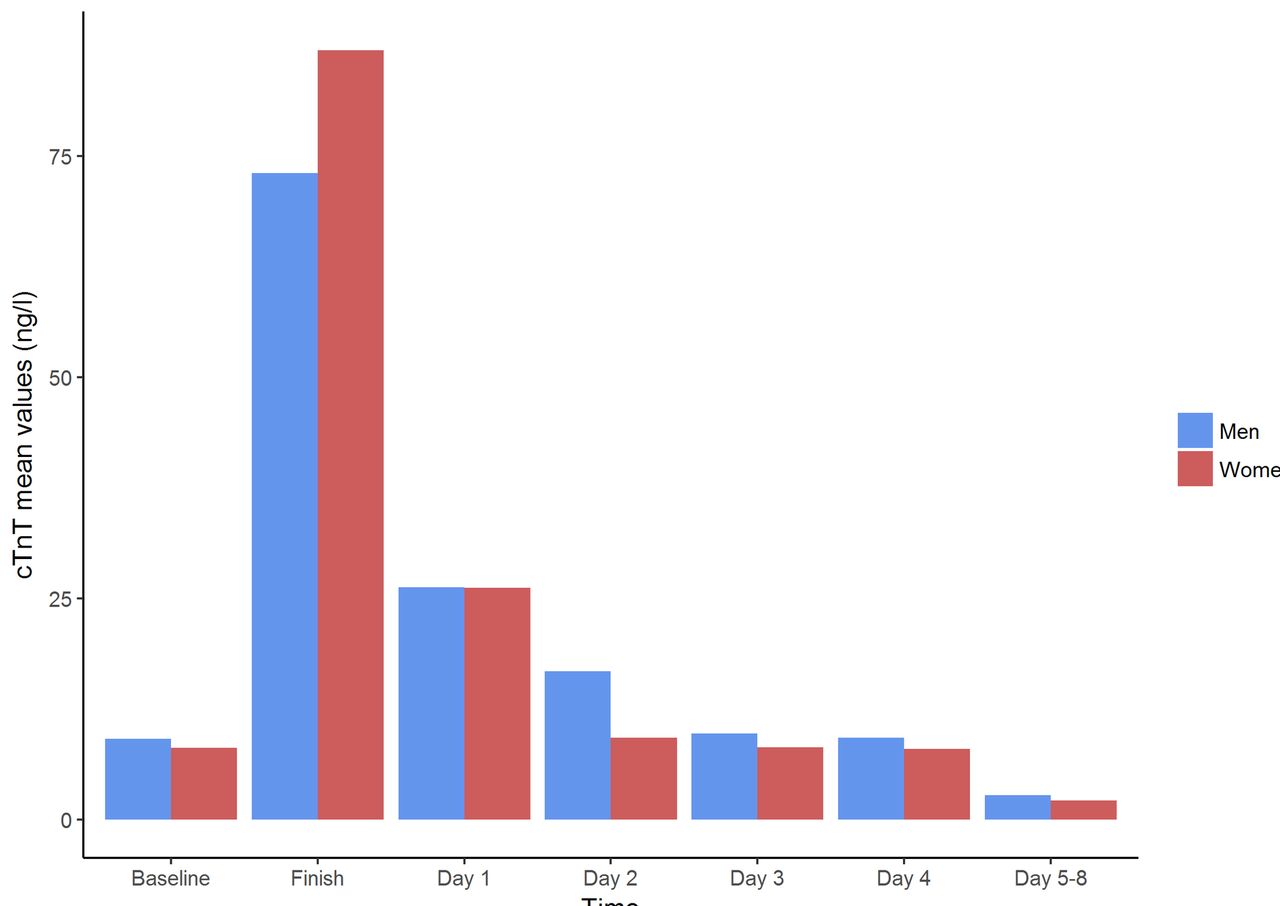
Cardiac troponin T was above the cut-off value in seven participants (15–28 ng/L) already before the competition. It increased to pathological values in all but one participant (51/52; 98%) reaching a maximum value of 440 ng/L in one athlete. It had returned to <15 ng/L in 13 athletes on day 1 after the race and in 51/52 on days 5–8 (figure 1). The data for NT-proBNP showed normal values in all participants at baseline (49–130 ng/L) and a peak directly after the race when 46/52 (88.5%) participants had abnormal levels up to 4700 ng/L. The NT-proBNP level had returned to normal in all participants at days 5–8 after the competition.
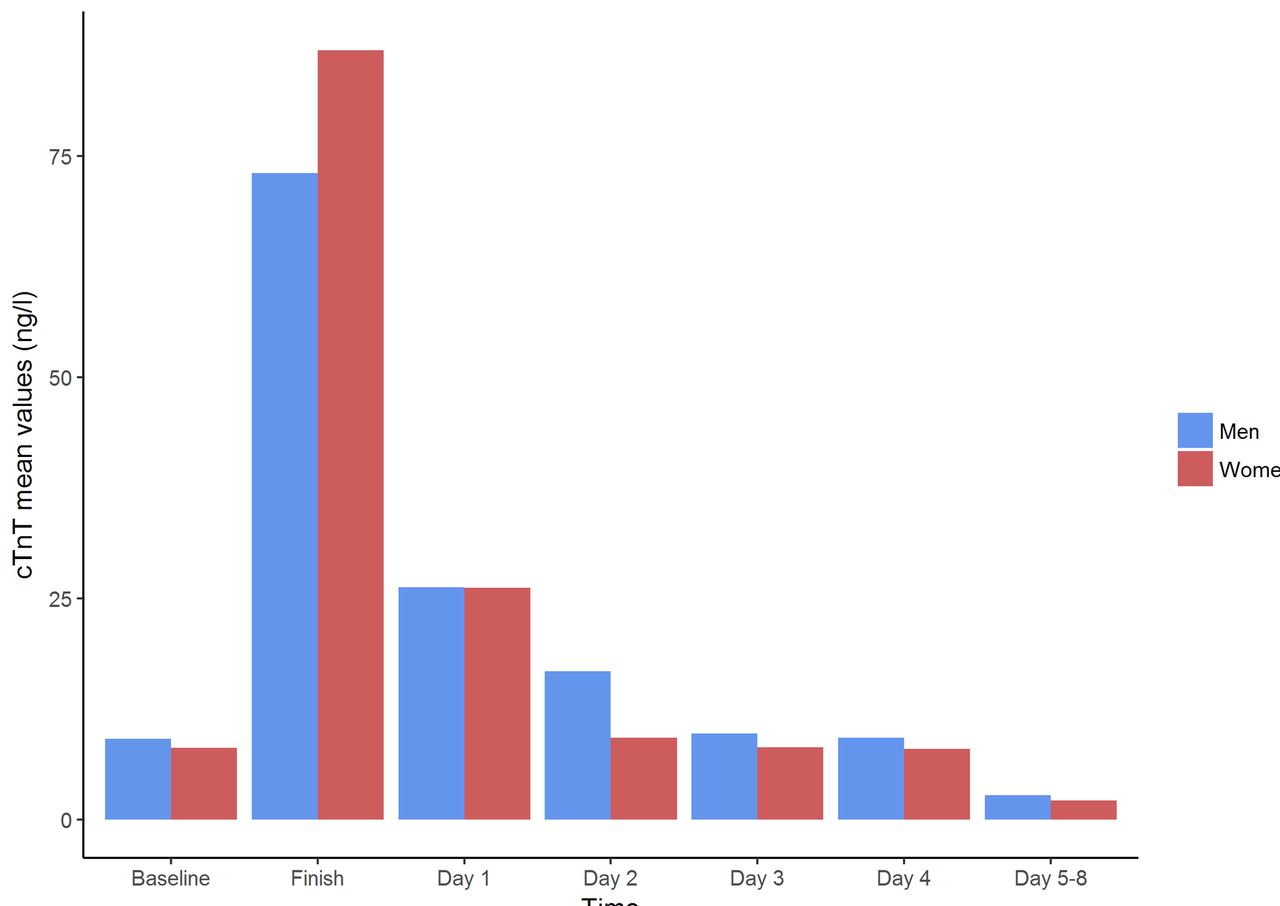
Cardiac TnT course (ng/L), mean values. Values for male participants in blue, female in red. cTnT, cardiac troponin-T.
The main purpose of this investigation was to investigate changes in plasma concentration of the MHC-α. There are no established normal values in the literature. The values before the race exhibited a wide range from 0.51 to 3.13 µg/L. The parameter then showed a two-peaked time course (figure 2). There were significant differences between male and female participants with women having higher values (all in μg/L): at baseline 1.15±0.4 vs 1.71±0.6; directly after the race 2.29±0.7 vs 3.13±0.8; 1.38±0.5 vs 1.89±0.7 on day 1 after the race (all p<0.01). However, the last measured MHC-α at days 5–8 had not returned yet to baseline levels and the difference between male and female participants was not significant by then (1.77±0.7 vs 1.88±0.8).

{kind=link}
{kind=link}
MHC-α course (μg/L), mean values. Values for male participants in blue, female in red. MHC-α, myosin heavy chain-alpha.
There was a significant correlation between the plasma concentrations of MHC-α and NT-proBNP (R=0.48; p<0.001) but neither between MHC-α and cTnT (R=0.13; p=0.36) nor MHC-α and myoglobin (R=0.18; p=0.2). Other correlations, for example, between CK and myoglobin and creatinine are well known and have earlier been described and discussed, not at least in our publication from Ironman 2015.13
Discussion
Non-cardiac biomarkers after exercise
The results concerning skeletal muscle damage, temporary decline of kidney function and inflammation markers after the Kalmar Ironman 2016 are in line with previous research in athletes engaging in either triathlon12 13 or other types of endurance sports such as marathon11 19 or ultradistance running.20 Given the amount of exercise, the results are neither surprising nor do they lead to any debate about long-term consequences.
Cardiac troponins after exercise
Long-term consequences of endurance sports have only been discussed for the heart. And here the question of a possible pathophysiological sequence—repeated myocardial injury as demonstrated by troponin release leads to patchy areas of myocardial fibrosis which, in turn leads to electrical instability and mainly atrial arrhythmias such as atrial fibrillation.3 Obviously, not every athlete gets atrial fibrillation in the long run and, as shown in the present and in earlier investigations, the spectrum of cTnT rise in connection to the race is rather large. The maximum cTnT in the present investigation differed by a factor of 36 while one 37-year-old man participant only went from 4 at baseline to 12 directly after the race and back to 6 the next day (all ng/L). A lot of work has been done on the question of determinants of troponin rise after exercise; however, the results concerning parameters such as exercise intensity, age, absolute racing time, body mass, training status and maximal oxygen uptake were heterogeneous.19 The newest publication found that cTnT rise was related to exercise intensity relative to ventilatory threshold and maximal oxygen uptake in participants of the Brighton Marathon.19 In our own material, aerobic capacity was not related to cTnT rise (paper submitted). The percentage of athletes with cTnT values above the cut-off value for myocardial infarction was even higher than in some earlier publications;21 22 however, it seems that the newer and the more sensitive the assay used the higher this percentage. Richardson et al, using the same fifth generation cTnT assay as we did, reported 100% values above the myocardial infarction cut-off value in 52 marathon runners.19 Very little work has been done on individual data using serial measurements in athletes during repeated races. Cardiac troponins are elevated in a number of acute and chronic conditions and acute coronary syndrome is only one of them. However, the mechanism of cTn elevation in conditions like systemic hypertension or post-tachycardia is poorly understood as it is in endurance exercise.17 White suggested six potential mechanisms for cTn increase in the blood stream: myocyte necrosis (as in myocardial infarction), apoptosis, normal myocyte turnover, cellular release of proteolytic degradation products, increased cell wall permeability and the formation and release of membranous blebs.16 Especially, the increased cell wall permeability hypothesis has gained popularity among researchers who see the release of unbound cTn in connection with exercise as a benign phenomenon with no irreversible cell death.9 However, this hypothesis has never been proven and has been deemed unlikely by others.5 8 17 Even if the mechanism is related to increased myocardial strain than to ischaemic conditions, it appears likely that irreversible cell death is a prerequisite for cTn entering the circulation in higher than baseline amounts.17
Other cardiac proteins
Of more than 10 000 different proteins found in heart tissue,18 different types of cardiac myosin were investigated as a marker of myocardial infarction in the 1980s and 1990s.23–25 Since neither myosin light chain-1 nor myosin heavy chain-β are specific for heart muscle—both are expressed in skeletal muscle as well—there was never a diagnostic use for these markers. In contrast, MHC-α is specific for atrial and ventricular heart muscle.18 Moreover, mutations in the gene encoding MHC-α have been associated with heart disease.26 However, as a diagnostic marker, MHC-α has not been thoroughly studied and there are no, with modern technology, established normal values.24 25
Our hypothesis was rather mechanical and a response to the hypothesis of an increased cell membrane permeability: If a rise and fall of MHC-α with six times higher molecular weight than cTnT can be measured in the bloodstream after endurance exercise, the membrane permeability hypothesis seems appreciably less likely to be correct. The two phase rise of MHC-α concentration that we found in our athletes is a strong argument against the hypothesis. The finding could be more easily interpreted as follows: the first peak can be due to cellular release of myocardial MHC-α which is not incorporated into the thick filaments of the sarcomere. The second peak, on the other hand, may represent the total disintegration of myocardial muscle cells. The fact that there was no correlation between MHC-α and cTnT levels could be ascribed to the fact that MHC-α is mainly found in the atria while the amount of cTnT predominantly originates in the ventricles. The mechanism of cTnT and MHC-α release would rather be myocardial strain and stretch-mediated cardiomyocyte death than ischaemia in these athlete hearts. In this context, the correlation of MHC-α and NT-proBNP would be consistent with high filling pressures and myocardial stretch.
The absence of previous research into MHC-α as a biomarker for myocardial infarction or other cardiac diseases known to lead to abnormal cTnT levels is a limitation of this work and its conclusions. We are not able to exclude other mechanisms of MHC-α release, for example, secretion of myosin or its fragments under oxidative stress, even if they appear unlikely. More work on variability in the MHC-α plasma concentration in health and disease seems important.
Practical aspects for athletes
With more and more people engaging in endurance sports worldwide, the question whether a marathon, triathlon or ultrarunning repeatedly harms the heart by causing heart muscle cell necrosis seems of utmost importance. However, there is only circumstantial evidence on both sides of the debate of physiological versus pathological explanations of troponin leakage. Neither side can so far conclusively prove what the mechanism of troponin rise really is. It seems counterintuitive that just exercise should be the one and only scenario where increased plasma troponin levels are not associated with increased risk of adverse outcomes. In virtually all other clinical and preclinical situations, an elevated troponin level, even within the normal range, indicates an increased risk of death and cardiovascular morbidity. This includes the general population,27 patients post supraventricular tachycardia,28 patients with chronic kidney disease29 and patients undergoing non-cardiac surgery.30 Even a subclinical rise of cTnT from below detection level to below the cut-off value for myocardial infarction indicates a higher incidence of subsequent coronary heart disease, heart failure and death.31 On the other hand, it seems equally unlikely that elite distance runners who maintain a high fitness over decades would have repeatedly sustained small myocardial infarctions.32
Conclusion
The study into MHC-α plasma levels after triathlon was designed to address the question of possible cell membrane permeability changes as mechanism for the rise of myocardial biomarkers after endurance exercise. The results point rather towards myocardial cell death associated with a two-peaked pattern of MHC-α release after triathlon. However, several new questions arose and old ones remain. Possibly, these questions may be better elucidated in long-term follow-up studies of individuals with particularly low and particularly high increases of troponin and MHC-α plasma levels after extreme sport events.
Acknowledgments
Thanks must go to the Kalmar Ironman organisers, the team of nurses who took the blood samples and of course the willing triathletes. We would also like to thank the laboratory team in Kalmar County Hospital and Marlene Norrby and Mohammad Ashikur Rahman from the Department of Chemistry and Biomedical sciences, Linnaeus University.
References
Footnotes
Contributors All authors (TD, HS, HW, TJ, AM, PB and JC) contributed to the conception of the study. JC and PB performed the data analysis. All authors assisted with the interpretation. JC and TD were the principal writers of the manuscript. All authors contributed to the drafting and revision of the final article. All authors approved the final submitted version of the manuscript.
Funding The project was funded by Landstinget Kalmar Län through unrestricted funds to a professorship of public health (JC currently holds that position) at the Linnaeus University Kalmar. The study was undertaken as part of the IronWoMan study group.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Regional Ethics Review Board in Linköping (EPN, Dnr 2016/86-31).
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement All measured data separated by sex can be obtained through contact with the corresponding author.