Article Text

Abstract
Background Concussion occurs when biomechanical forces transmitted to the head result in neurological deficits. Personality may affect the balance between safe and dangerous play potentially influencing concussion risk. Dopamine receptor D2 (DRD2) and dopamine receptor D4 (DRD4) genetic polymorphisms were previously associated with personality traits.
Objectives This case–control genetic association study investigated the associations of (1) DRD2 and DRD4 genotypes with concussion susceptibility and personality, (2) personality with concussion susceptibility and (3) the statistical model of genotype, personality and concussion susceptibility.
Methods In total, 138 non-concussed controls and 163 previously concussed cases were recruited from high school (n=135, junior), club and professional rugby teams (n=166, senior). Participants were genotyped for DRD2 rs12364283 (A>G), DRD2 rs1076560 (C>A) and DRD4 rs1800955 (T>C) genetic variants. Statistical analyses including structural equation modelling were performed using the R environment and STATA.
Results The rs1800955 CC genotype (p=0.014) and inferred DRD2 (rs12364283–rs1076560)–DRD4 (rs1800955) A–C–C allele combination (p=0.019) were associated with decreased concussion susceptibility in juniors. The rs1800955 TT and CT genotypes were associated with low reward dependence in juniors (p<0.001) and seniors (p=0.010), respectively. High harm avoidance was associated with decreased concussion susceptibility in juniors (p=0.009) and increased susceptibility in seniors (p=0.001). The model showed that a genetic variant was associated with personality while personality was associated with concussion susceptibility.
Conclusion These findings highlight the linear relationship between genetics, personality and concussion susceptibility. Identifying a genetic profile of ‘high risk’ behaviour, together with the development of personalised behavioural training, can potentially reduce concussion risk.
- dopamine receptor genes
- concussion history
- reward dependence
- behaviour
- rugby
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
The C allele of rs1800955 variant within the dopamine receptor encoding gene, DRD4, was correlated with a reduction in concussion susceptibility as noted in junior rugby players.
The DRD4 rs1800955 T allele was associated with socially detached behaviour in both junior and senior players.
A risk model of genetic, personality and injury profiles showed that the DRD4 rs1800955 variant was associated with personality, while personality was associated with concussion susceptibility.
Introduction
Concussions are brain injuries resulting from biomechanical forces transmitting to the head and causing altered neurological function.1 Concussions are common in rugby with an incidence of 3.9 concussions/1000 player-hours reported.2
An individual’s personality traits have been implicated in modulating sport concussion susceptibility.3–5 Specifically, high impulsivity scores were reported in rugby players with an increased concussion risk.3 Both impulsivity and aggression were associated with a concussion history in former athletes4; however, aggression was not associated with concussion susceptibility in soldiers.5 Theoretically, unchecked aggressive behaviour can exacerbate pre-existing concussion symptoms and increase the likelihood of severe concussions.
High novelty-seeking (NS) or a ‘risk-taking’ personality trait was previously correlated with genetic variants within genes encoding dopamine receptors.6 7 These dopamine receptors, including D2 and D4 receptor subtypes, are involved in dopamine neurotransmission and may modulate memory, behaviour and executive functions.8 9 The DRD2 gene encodes for the dopamine D2 receptor, and several functional genetic variants within the DRD2 gene were previously associated with personality traits.7 10 11 The DRD2 promoter rs12364283 (−844 A>G) variant was associated with D2 receptor transcription and density in postmortem brain tissue.11 The rs12364283 AA genotype was associated with personality changes including improved avoidance-based decisions, poorer behavioural inhibition and increased impulsivity.7 10 Furthermore, the DRD2 intronic rs1076560 (C>A) variant was shown to be associated with splicing and mRNA expression of the D2 receptor,11 while the A allele was associated with impaired avoidance learning behaviour.10
The DRD4 gene encodes the dopamine D4 receptor and is expressed in the cognitive and emotional areas of the limbic system.12 13 The functional DRD4 promoter rs1800955 (−521 T>C) variant was shown to influence DRD4 transcriptional activity14; however, this was not reproduced in two independent studies.15 16 The CC genotype was associated with high NS trait, while the C allele was previously over-represented in schizophrenia sufferers.6 14 Collectively, the supporting evidence from expression studies and associations with personality implicates the DRD2 rs12364283, DRD2 rs1076560 and DRD4 rs1800955 variants in modifying personality possibly via inhibition of neurotransmission. Therefore, the investigation of the underlying physiology involved in personality-associated pathways may explain the role of personality in concussion susceptibility. To the authors’ knowledge, no studies have investigated all three functional dopamine receptor variants (DRD2 rs12364283, DRD2 rs1076560 and DRD4 rs1800955) independently and collectively, in a haplotype, with concussion susceptibility and personality.
The aims of this novel, case–control genetic association study were to independently investigate the associations of (1) DRD2 (rs12364283: A>G, rs1076560: C>A) and DRD4 (rs1800955: T>C) genotypes with concussion susceptibility, (2) DRD2 and DRD4 genotypes with personality and (3) personality with concussion susceptibility. An additional aim was to statistically model the collective interaction of concussion susceptibility, personality dimensions and genotype profile.
Methods
Participant recruitment
This case–control genetic association study was conducted according to the STrengthening the REporting of Genetic Association Studies guidelines17 and Declaration of Helsinki. Details on concussion definition, participant recruitment, concussion history and sports participation for this cohort were previously described.18 Concussions were defined according to the Concussion in Sport Group1 and symptoms were selected from the validated list in the Sports Concussion Assessment Tool V.2, which was the latest version in use at the time of diagnosis as participants were recruited during 2013–2015.19 Briefly, concussed cases were defined as individuals who sustained a concussion while playing rugby, with one or more of the following inclusion criteria: (1) diagnosis confirmed by a medical professional (physicians, physiotherapists, paramedics regardless of concussion diagnosis/management training), (2) sustained one or more symptoms and (3) the diagnosis may have included scores from computerised cognitive tests (eg, ImPACT). A ‘diagnosed concussion’ was categorised as concussions diagnosed by a medical professional with one or more concussion symptoms reported; while a ‘self-reported concussion’ was categorised as concussions not diagnosed by a medical professional but self-reporting one or more symptoms.
In total, 420 participants were included in this study after completing the consent and study questionnaire. Participants were excluded based on self-reporting ancestry, sporting activity and brain-related disorders (online supplementary figure S1). After all exclusions, a final total of 301 white, male Rugby Union players (aged 12–39 years) were analysed, with 138 participants self-reporting no concussion history (control group) and 163 participants with a history of clinically diagnosed and self-reported concussions (all cases group). A subgroup, of the all cases group, comprised participants with a history of clinically diagnosed concussions and separately analysed as clinically diagnosed subgroup (n=140). Participants were collectively analysed and stratified by playing level into juniors (n=135, high school/youth rugby players aged 12–18 years) and seniors (19–39 years; amateur-level club, n=116, and professional rugby players, n=50), and independently analysed. The participants were analysed by playing level to identify potential differences in genetic susceptibility. For example, junior players are vulnerable to adverse complications following concussion20 21 while senior players have a higher exposure to potentially pathology-induced, repetitive head impacts.22 23 In addition, the differences in life experience and intellect development between juniors and seniors may also influence personality scores.24 25 All participants completed a study questionnaire detailing their concussion, sporting and medical histories, as well as a psychometric personality questionnaire.
Supplemental material
DNA extraction and genotyping
DNA was extracted from either a buccal swab26 27 or venous blood sample.28 The selected variants, rs12364283 (−844 A>G) and rs1076560 (C>A) within the DRD2 gene (online supplementary figure S2) and rs1800955 (−521 T>C) within the DRD4 gene (online supplementary figure S2), had minor allele frequencies >5% in the white population (NCBI, https://www.ncbi.nlm.nih.gov/). The rs12364283, rs1076560 and rs1800955 variants were genotyped as previously described,18 at the Division of Exercise Science and Sports Medicine biochemistry laboratory, using fluorescence-based TaqMan real-time PCR assays and the StepOnePlus real-time PCR machine with software V.2.2.2 (Applied Biosystems, USA).
Personality questionnaire
Cloninger’s 96-item true/false, validated Tri-dimensional Questionnaire (TPQ) was used to measure the three personality dimensions.29 The personality dimensions evaluated were NS, which responds to novelty and reward, harm avoidance (HA), which responds to aversive stimulus, and reward dependence (RD) for reward anticipation and reinforced behaviour.29 30 True and false answers were scored with one and zero, respectively, and a total was determined for each personality dimension and subscale. Individuals with a higher score would have a heightened behavioural response while the inverse for a lower score (online supplementary table S1).
Statistical analysis
Statistical analysis was performed using STATA statistical software release V.14 (College Station) and the R language and environment for statistical computing.31 A logistic regression model was fitted on concussion history (case–control) as a function of personality traits (NS, HA and RD) as well as a separate analysis where personality was tested as a function of genotypes (rs12364283, rs1076560, rs1800955) using genetics, SNPassoc and haplo.stats packages, and Fisher’s exact test in R.32 33 These analyses were adjusted for age as a confounding covariate. Generalised structural equation modelling was performed using STATA to collectively investigate the interactions between concussion history, personality and genotypes. Concussion history was coded within the model with the all cases group and clinically diagnosed subgroup compared relative to the control group, and the major homozygous genotype used as the reference genotype for each variant (rs12364283: A/A, rs1076560: C/C, rs1800955: T/T). Concussion history was compared between personality and genotypes, while personality was compared between genotypes. A hypothesis-driven approach was adopted with three biologically relevant variants (two of which were positioned on a single gene, DRD2 rs12364283 and rs1076560; D′=0.030, r2=0.0004), thus correcting for multiple testing would be too conservative for this study.34 Statistical significance was set at p<0.05.
Results
Participant characteristics
Only the findings for junior and senior groups will be discussed while the findings for all participants collectively can be found in the online supplementary material 1 (online supplementary tables S2, S3, S4, S5 and S6, and figure S3).
When only the juniors were analysed, no significant differences were noted between groups for age, height, weight, body mass index, rugby exposure and non-rugby collision sport exposure (online supplementary table S2). When only the seniors were analysed, the control group (n=66) was significantly younger than the all cases group (n=100) (p=0.038; control: 21.7±3.3 years; all cases: 22.9±3.9 years).
DRD2 rs12364283, DRD2 rs1076560 and DRD4 rs1800955 genotype and allele frequency distribution
For juniors (figure 1C), the rs1800955 CC genotype was significantly over-represented in the control group (n=11) compared with the all cases group (n=2) and the clinically diagnosed subgroup (n=0) (CC vs TT+CT; control vs all cases: p=0.014, control, 19% and all cases, 4%; OR 0.18, 95% CI 0.04 to 0.87; control vs clinically diagnosed: p=0.003, clinically diagnosed, 0%). All three variants (rs12364283, rs1076560 and rs1800955) were in Hardy-Weinberg equilibrium (HWE) for the control and case groups (p>0.05), with the exception of the rs1800955 variant which was not in HWE for the clinically diagnosed subgroup (p=0.016; figure 1).

The genotypes frequencies of DRD2 rs12364283, rs1076560 and DRD4 rs1800955. The genotype frequencies (%) between the control group (controls), all clinically diagnosed and self-reported concussed cases (all cases) and clinically diagnosed concussed cases only (clinically diagnosed); for the (A) DRD2 rs12364283 (A>G), (B) rs1076560 (C>A) and (C) DRD4 rs1800955 (T>C) variants in juniors (left panel, n=125) and seniors (right panel, n=165). Significant differences between groups are indicated (p<0.05). The rs12364283 GG genotype is missing in seniors.
For seniors, the rs12364283, rs1076560 and rs1800955 genotypes (figure 1) and allele frequency distributions (online supplementary table S4) were not significantly different between groups. All three variants were in HWE for the control and case groups (p>0.05; figure 1).
Inferred DRD2 rs12364283-rs1076560-DRD4 rs1800955 allele combination distribution
The inferred DRD2 and DRD4 allele combination was constructed using the genotype data [DRD2 rs12364283 (A>G), DRD2 rs1076560 (C>A), DRD4 rs1800955 (T>C)]. In total, four inferred allele combinations, above a frequency of 4%, were identified (figure 2). The A–C–C and A–C–T allele combinations were noted as the most frequent (25%–51%), while the A–A–C and A–A–T were the least frequent (3%–11%) for the control and case groups (figure 2). No significant differences were noted for the inferred DRD2 rs12364283–rs1076560–DRD4 rs1800955 allele combination between groups, when only seniors were analysed (figure 2B).

The frequencies of the inferred DRD2 rs12364283–rs1076560–DRD4 rs1800955 allele combination. The frequencies (%) between the control group (controls), all clinically diagnosed and self-reported concussed cases (all cases) and clinically diagnosed concussed cases only (clinically diagnosed) for the inferred DRD2 rs12364283 (A>G), DRD2 rs1076560 (C>A) and DRD4 rs1800955 (T>C) allele combinations; in (A) juniors (n=107) and (B) seniors (n=163). Significant differences between groups are indicated (p<0.05, recessive model).
For juniors (figure 2A), the A–C–C allele combination was significantly over-represented in the control group (n=19, 32%) compared with the all cases group (n=12, 25%) and compared with the clinically diagnosed subgroup (n=11, 28%) (recessive model, control vs all cases: p=0.019, hap.score=−2.34; control vs clinically diagnosed: p=0.039, hap.score=−2.06).
Genotype and personality dimensions
For juniors (table 1), the mean RD score was significantly lower in individuals with the rs1800955 TT genotype (n=24) compared with the combined CC and CT genotypes (n=39) (TT vs CC+CT: p<0.001, TT, 15.5±4.2; CC+CT, 20.0±3.5). Furthermore, the RD1, RD3 and RD4 subscales were significantly lower in individuals with the TT genotype (TT vs CC+CT, RD1: p<0.001, TT, 2.8±1.0, n=27; CC+CT, 3.9±1.0, n=41; RD3: p =0.002, TT, 5.4±2.5, n=24; CC+CT, 7.3±2.2, n=42; RD4: p=0.002, TT, 2.0±1.1, n=27; CC+CT, 2.8±1.1, n=42).
The mean scores for the Tri-dimensional Personality Questionnaire (TPQ) dimensions; novelty seeking (NS), harm avoidance (HA) and reward dependence (RD), between the DRD2 rs12364283 (A>G), DRD2 rs1076560 (C>A) and DRD4 rs1800955 (T>C) genotypes
For seniors (table 1), the mean RD score was significantly lower in individuals with the rs1800955 CT genotype (n=73) compared with the combined TT and CC genotypes (n=66) (CT vs TT+CC: p=0.010, CT, 18.4±3.9; TT+CC, 20.2±4.2). However, none of the RD subscales were significantly different between the rs1800955 genotypes (RD1: p=0.122, RD2: p=0.053, RD3: p=0.499, RD4: p=0.237).
Concussion history and personality dimensions
For juniors (table 2), the HA dimension was significantly higher in the control group (n=44) compared with all cases group (n=40) and clinically diagnosed subgroup (n=33) (control vs all cases: p=0.009, control, 12.9±5.9, all cases, 9.7±5.0; control vs clinically diagnosed: p=0.006, clinically diagnosed, 9.5±4.8). Furthermore, HA1 and HA2 of the four HA subscales were significantly higher in the control group compared with the concussed groups (HA1: control vs all cases, p=0.024; control, 4.1±2.2, n=47, all cases, 3.0±1.9, n=41; control vs clinically diagnosed, p=0.012; clinically diagnosed, 2.9±1.7, n=33; HA2: control vs all cases, p=0.017; control, 3.0±2.0, n=46, all cases, 2.1±1.5, n=40; control vs clinically diagnosed, p=0.009; clinically diagnosed, 1.9±1.4, n=32).
The mean scores of the Tri-dimensional Personality Questionnaire (TPQ) dimensions; novelty seeking (NS), harm avoidance (HA) and reward dependence (RD), between the control group (controls) and all clinically diagnosed and self-reported concussed cases (all cases) and clinically diagnosed concussed cases only (clinically diagnosed)
For seniors (table 2), the HA dimension was significantly lower in the control group (n=56) compared with all cases group (n=86) and clinically diagnosed subgroup (n=74) (control vs all cases: p=0.001, control, 8.1±4.9, all cases, 11.2±6.1; control vs clinically diagnosed: p=0.002, clinically diagnosed, 11.1±6.0). Furthermore, HA1, HA3 and HA4 of the four HA subscales were significantly lower in the control group compared with the concussed groups (HA1: control vs all cases, p=0.003; control, 2.1±1.7, n=57, all cases, 3.1±2.1, n=89; control vs clinically diagnosed, p=0.004; clinically diagnosed, 3.1±2.1, n=76; HA3: control vs all cases, p=0.018; control, 1.8±1.7, n=59, all cases, 2.6±2.1, n=89; control vs clinically diagnosed, p=0.038; clinically diagnosed, 2.6±2.1, n=77; HA4: control vs all cases, p=0.004; control, 2.1±2.1, n=58, all cases, 3.0±2.4, n=90; control vs clinically diagnosed, p=0.004; clinically diagnosed, 3.1±2.3, n=77).
Modelling the collective relationship between concussion history, personality and genotype scores
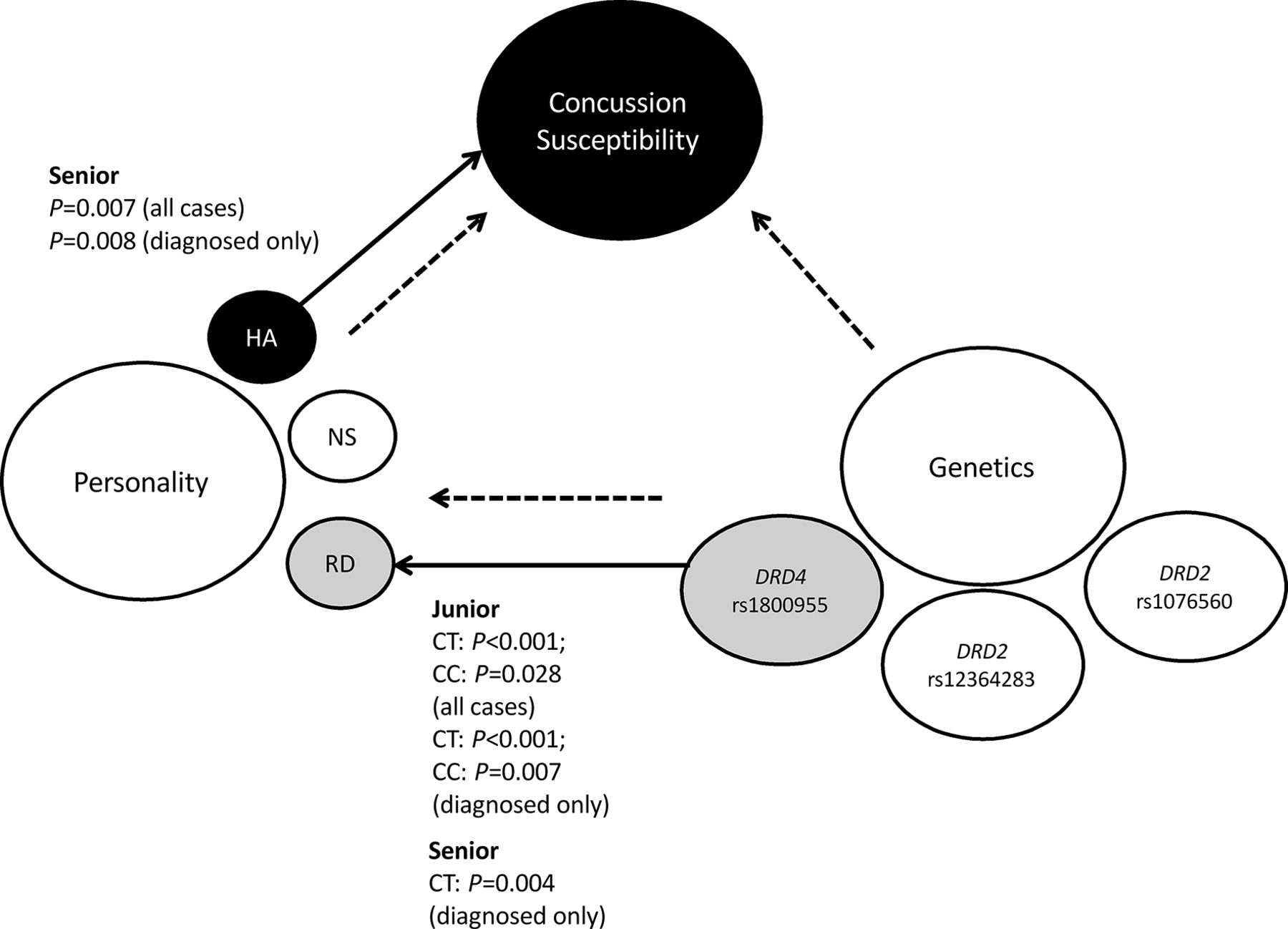
The interplay between concussion susceptibility, personality dimensions and DRD2 and DRD4 genotypes was investigated using a generalised structural equation model (figure 3, online supplementary table S7). When the juniors were evaluated (figure 3), personality and genotype were collectively correlated and specifically the RD score was significantly associated with the rs1800955 genotype for the all cases group (TT vs CT: p<0.0001, coefficient=4.45, SE=1.04; TT vs CC: p=0.028, coefficient=3.06, SE=1.39), and the clinically diagnosed subgroup (TT vs CT: p<0.0001, coefficient=5.01, SE=1.05; TT vs CC: p=0.007, coefficient=3.95, SE=1.46).
{kind=link}
{kind=link}
{kind=link}
The generalised structural equation model of concussion susceptibility, personality traits and genetic variants. The circles represent concussion susceptibility, consisting of non-concussed control and concussed case groups, as the grouping variable, and personality (novelty seeking (NS), harm avoidance (HA), reward dependence (RD)) and genetics (DRD2 rs12364283: A>G, DRD2 rs1076560: C>A and DRD4 rs1800955: T>C) as the predictor variables. The dotted arrows indicate the proposed relationship between variables. the solid arrows, connecting the black and grey coloured circles, indicate the specific significant associations displayed for junior and senior groups, where relevant (p<0.05).
When seniors were evaluated (figure 3), the personality dimensions were found to be significantly correlated with concussion susceptibility. In particular, the HA score was significantly different between control and all cases groups (p=0.007, coefficient=0.10, SE=0.04), as well as between control and clinically diagnosed subgroup (p=0.008, coefficient=0.11, SE=0.04). When the clinically diagnosed subgroup was analysed, personality and genotype were significantly correlated, with the RD score significantly associated with the rs1800955 genotype (TT vs CT: p=0.004, coefficient=−2.30, SE=0.80).
Discussion
The main findings of this study were (1) the independent DRD4 rs1800955 genotype and inferred DRD2 (rs12364283–rs1076560)–DRD4 (rs1800955) allele combination were associated with concussion susceptibility in juniors, (2) the rs1800955 variant was associated with RD scores in both junior and senior groups, (3) HA scores were associated with concussion susceptibility in both junior and senior groups and (4) the model showed that a genetic variant was associated with personality while personality was associated with concussion susceptibility in white male rugby players.
Distribution of the DRD2 rs12364283, DRD2 rs1076560 and DRD4 rs1800955 genotype, allele and inferred allele combination
In this study, the DRD4 rs1800955 CC genotype and the inferred DRD2 (rs12364283–rs1076560)-DRD4 (rs1800955) A–C–C allele combination were over-represented in the control group. These findings implicate the rs1800955 C allele in reduced concussion susceptibility. The C allele, compared with the T allele, was previously associated with higher DRD4 expression.14 The preferential binding of dopamine to D4 receptors inhibits adenylyl cyclase,8 thereby suppressing neurotransmission, particularly modulating decision-making and cognitive behaviour.35 36 We hypothesise that the C allele may stimulate DRD4 expression, increasing the D4 receptor availability to dopamine and directing the dopaminergic activity towards an overall inhibition of decision-making and cognitive behaviour. Tentatively, therefore, the C allele acts as a neuro-protective response against concussion injury by inhibiting ‘risk-taking’ behaviour (online supplementary figure S4).
Genotype and personality dimensions
The rs1800955 TT and CT genotypes were associated with a low RD score in juniors and seniors, respectively. In this study, juniors with the TT genotype presented with socially detached behaviour (low RD).29 37 In seniors, socially detached behaviour was associated with the CT genotype. The theory proposed is that in response to a reward stimulus the TT genotype, in juniors, and the CT genotype, in seniors, may elicit a change in D4 receptor expression and availability thereby increasing excitatory nerve signals and stimulating socially indifferent behaviour. This indifferent behaviour may promote callousness leading to dangerously tackling another player and increase a rugby player’s risk of injuring themselves or others. Reckless tackling techniques are cited as common mechanisms of rugby-related concussions.38 39 Furthermore, in seniors, the C or T allele may act on different biological pathways and both still contribute to eliciting a low RD behaviour. It is possible that the heterozygosity (or heterosis) observed may be due to (1) participant selection or (2) a true effect of heterosis. First, all participant demographics were normally distributed. Second, heterosis of a genetic marker was previously shown to associate with increased risk for neurodegenerative diseases40 and may be a plausible genotype–personality association in seniors in this study.
Concussion history and personality dimensions
In juniors, apprehensive and cautious behaviour (high HA) was observed in the control group compared with the case groups. Anticipatory worry and fear of uncertainty (high HA1 and HA2 scores) were also noted in the controls. These avoidant behavioural traits imply a tendency to avoid dangerous playing techniques which may result in reduced concussion susceptibility.41 In seniors, however, the inverse relationship was observed with carefree and confident behaviour (low HA) in the controls. This contradictory relationship in seniors could be explained by the fact that amateur club and professional rugby players (senior group) have a greater skill level and a higher self-confidence in their playing ability.42 43 A greater self-confidence at the senior level could lead to reduced concussion susceptibility, while a less confident player may make more mistakes and increase their susceptibility to concussion.
Concussion history, personality and genotype modelling
When investigating the collective effect of genetic variants and personality traits on concussion susceptibility using a structural equation model, similar findings were observed to the independent analyses performed. The rs1800955 variant was associated with RD in both juniors and seniors, while HA was associated with concussion susceptibility in seniors only. The model highlighted that genetics (rs1800955) explained personality changes (RD dimension) while personality changes (HA dimension) explained concussion susceptibility, without the direct effect of genetics (figure 3).
This cohort represents a very narrow sample population of white, young male rugby players and, therefore, these results only provide a finite perspective of the population and require investigation in a broader population group. This study is also limited by the concussion diagnosis as not all medical professionals were trained in concussion diagnosis/management and the inclusion of self-reported concussion, which could result in misreporting of concussions.
In summary, these findings highlight that genetic and personality pathways influence concussion risk differently between juniors and seniors. In addition, the findings highlight a linear relationship between genetics, personality and concussion susceptibility in rugby players. Future studies should compare junior and senior groups in larger cohorts to further explore the possible age effect on the relationship between genetics, personality and concussion susceptibility. A future clinical implication of these results is the identification of a genetic profile which could highlight athletes susceptible to ‘high concussion-risk’ behaviour.
Acknowledgments
The authors thank all the participants and respective authorities from the high schools, clubs, professional teams and medical practices for their time, effort and participation in this study.
References
Footnotes
Funding This study and authors were funded by the South African National Research Foundation (grant numbers: 90942, 93416, 85534), the Deutscher Akademischer Austauschdienst (DAAD) and the University of Cape Town. Funders had no involvement in the paper.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the Human Research Ethics Committee of the University of Cape Town.
Provenance and peer review Not commissioned; externally peer reviewed.