Article Text

Abstract
Objectives The aim of this study was to establish quantitative values for asymptomatic and symptomatic Achilles tendons.
Design Cohort study with a single (cross-sectional) time point of patients diagnosed with unilateral Achilles tendinopathy and an asymptomatic group with comparative homogeneity.
Methods A sample of 50 participants: 25 diagnosed with symptomatic unilateral Achilles tendinopathy (AT group) and 25 with asymptomatic Achilles tendons (control group 2). The asymptomatic side of the AT group was used as a control (control group 1). Measurements at 2 cm intervals on the tendon from its insertion at the calcaneum up to the musculotendinous junction were taken non-weight bearing (NWB) and weight bearing (WB) using the MyotonPRO.
Results There was a significant (p<0.005) decrease in natural oscillation frequency (F) at points 2, 3 and 4 of the AT group (NWB condition) and points 2 and 3 for the WB condition. There was a significant (p<0.005) increase in logarithmic decrement (D) at points 2 and 3 signifying a decrease in elasticity. Dynamic stiffness (S) was significantly (p<0.005) reduced in the AT group at points 2 and 3 WB and point 3 WB. There was no significant difference in creep (C) observed between the symptomatic and asymptomatic tendons. There was a significant (p<0.005) increase in mechanical stress relaxation time (R) at point 2 NWB.
There was a correlation between body weight and gender on tendon mechanics, with the symptomatic tendons. No significant differences were observed between the control group 1 and control group 2.
Conclusions The MyotonPRO measured decreased stiffness over a section of the tendon corresponding clinically with Achilles tendinopathy. This may have potential in identifying risk of injury and informing rehabilitation, however further extensive research is required to generate baseline data for specific population groups monitoring variables over time. Age, gender and body mass index appear to have some bearing on the mechanical properties of the tendon but mainly in the tendinopathy group.
- tendinopathy
- diagnosis
- sports & exercise medicine
- sports rehabilitation programs
- achilles
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
There was a significant decrease in the stiffness of symptomatic tendons.
Measurable differences in tendon mechanics were observed over the tendinopathic region.
Weight bearing and non-weight bearing measurements demonstrated measurable differences between symptomatic and asymptomatic tendons.
The data observed may assist the clinician in identifying risk of injury and informing rehabilitation.group.
Introduction
Achilles tendinopathy, a prevalent condition among athletes, has an incidence rate of 8.3 per 1000, 1 and non-athletes 2.35 per 1000.2 Achilles tendinopathy has a detrimental effect on physical and mental well-being,.3 There is no single beneficial treatment and a poor prognosis,4 with a high incidence of chronicity and reoccurrence, particularly if tendinopathy is not detected early on. It is thought that therapeutic interventions demonstrate improved outcomes if implemented early in the tendinopathic process.5 6 Screening for injury prevention in the sporting population is a common practice with aims of early diagnosis and detection and is widely debated.7 The concept of screening therefore, to detect early changes in health, is a clear goal for practitioners managing the athletic population.7 However the current predictive models for tendinopathy pain remain inconclusive.8
The diagnosis of Achilles tendinopathy has been traditionally based on patients' symptoms of pain, focal swelling of the tendon and decreased physical function.9 A systematic review of the diagnostic accuracy of subjective and objective orthopaedic clinical tests suggest that clinical tests can demonstrate a significant diagnostic capability for Achilles tendinopathy.10 Ultrasound imaging of tendons can reveal structural changes, particularly tendon swelling and collagen disorganisation. However, ultrasound findings, particularly in patellar tendons, are not well correlated with clinical symptoms.11 12
The functional mechanical changes associated with tendinopathy are often poorly understood in sports medicine. An important mechanical property of tendon is stiffness, determining the function of the tendon and its effect on muscle power and locomotive efficiency.13 An optimal level of stiffness is required for optimal function. The stiffness and elastic properties of the tendon affect its ability to return to its previous shape following deformation and assist the clinician in understanding how the tendon functions as part of the kinetic system.14 For example, slower recovery of muscle/tendon length can directly affect myofascial force transmission through loss of energy and inefficiency.15 It has been previously suggested that there is an optimum stiffness of tissues for injury prevention.16
In order to determine components of stiffness, this study used a novel handheld myotonometer (MyotonPRO, myoton.com) to measure the quantitative mechanical parameters of the Achilles tendon in vivo. The MyotonPRO is a non-invasive handheld device which generates an oscillation in soft tissues resulting in a calculation of the mechanical properties of the tissues. Soft tissue measurements taken with the MyotonPRO are captured simultaneously by its accelerometer, and can be altered with underlying pathology.17 These mechanical properties are components of tissue biomechanics and stiffness, that is, natural oscillation frequency (Hz) (F), characterising tone; logarithmic decrement (D) of natural oscillation, characterising elasticity; dynamic stiffness (N/m)(S), creep-(C), mechanical stress relaxation time (ms) (R) (Myoton.com). The MyotonPro has been deemed a reliable measure for the mechanical properties of tendon and muscle tissue,18 19 and provides a quantitative measurement of mechanical soft tissue data with low user-level skill required. The quantitative mechanical measurements generated by the MyotonPRO provide the clinician with information about the pathological nature of the tissues under question.20 Other clinical measures previously used to achieve this have been shear wave elastography (SWE). SWE uses focused ultrasound waves travelling horizontal to the soft tissues to measure tissue mechanical properties. SWE has been established as a reliable method to measure soft tissue parameters,21 with a significant correlation between measurements generated using MyotonPRO and those from the SWE.22 This association would support the use of the MyotonPRO as a clinical tool to measure soft tissue mechanics. In addition, the intrarater and inter-rater reliability of the MyotonPRO is excellent and reliable when compared with SWE used on tissues such as the gastrocnemius muscle.22 In addition to this, intraday measurements of the Achilles tendon were found to be repeatable with the MyotonPro.23 The effect of skin on the MyotonPRO output has been previously tested for validity.24 In this study the skin had a statistically significant effect on the device measurements, however it did not interfere with the ability of the device to measure physiological variation or trend. In addition to this the MyotonPRO was tested for consistency with known material parameters and was shown to provide a very small margin of error.
This study aims to establish quantitative values for asymptomatic and symptomatic Achilles tendons to provide reference values for developing an understanding of presymptomatic detection and further research.
Methodology
Trial design
This is a cohort study with a single (cross-sectional) time point of 50 participants. The Achilles tendon (AT) group consisted of 25 participants from Cwm Taf University Health Board diagnosed clinically (with symptoms of pain, focal swelling of the tendon and decreased physical function) with symptomatic unilateral Achilles tendinopathy. The AT group was identified via existing paper-based triage from consecutive service user referrals. These patients were booked into a foot and ankle clinic at an orthopaedic outpatient department. A within-subjects control was also used with the asymptomatic side of the symptomatic group, that is, control group 1. Control group 2 consisted of 25 participants with asymptomatic Achilles tendons with comparative homogeneity, recruited from staff volunteers within the outpatients department via an invitation letter and staff information sheet on local clinical notice boards. The null hypothesis stipulated that there would be no measurable mechanical changes with the MyotonPRO in patients with Achilles tendinopathy compared with participants that were asymptomatic and not diagnosed with Achilles tendinopathy. Participant data were age-matched and gender-matched.
Pilot data sourced from clinical activity were used to compare the tonal properties of the control groups and AT group data. At the time of study design, there were no published comparative analyses to use for the calculation. A two-sided t-test was used with a mean symptomatic score of 33 for F, a mean asymptomatic score of 57 for F and a common SD of 8, and assuming a standard 5% significance threshold, a requirement of four Achilles tendon measurements (eight in total) would be required to demonstrate a statistically significant difference with 90% power.
The soft tissue mechanical data collected from each group using the MyotonPRO were used to compare each set of data. Each point marked on the Achilles tendon (ie, 1–8) was compared with its corresponding point in each group, for example, point 1 AT gas compared with point 1 control group 1. MyotonPRO is a class 1 medical device according to European Medical Device Directive 93/42/CEE+2007/47/CE. There are five steps in the MyotonPRO measurement process: application of prepressure (0.18 N), a mechanical impulse with quick release (0.4N), recording of oscillations (200 ms), processing of raw signal (10 ms) and computation of parameters (5 ms): F (Hz), characterising tone; D, characterising elasticity; S (N/m) (S), creep-ability (C) (Deborah number), mechanical stress relaxation time (ms) (R) (Myoton.com). The mechanical impulse exerted on the tendon does not cause residual mechanical deformation or neurological reaction of the muscle or tissue being evaluated. Therefore repeatability following initial non-weight bearing (NWB) measurement is of no concern for the subsequent weight bearing (WB) measurements.
The inclusion criteria for the AT group consisted of unilateral Achilles tendinopathy diagnosed clinically by symptoms of focal or generalised swelling and pain of the Achilles tendon; age restriction of 18–70 years to eliminate possible growth variations in younger participants and possible degeneration variation in older participants. Criteria for exclusion from the study included previous surgical repair or rupture of the Achilles tendon; patients prescribed quinolone antibiotics; a body mass index (BMI) of >35; history or symptoms of below knee soft tissue or joint pain; known rheumatological disease, diabetes or connective tissue disease and participants should not be actively receiving or proceeding through an existing treatment plan for their condition.
Procedure
Measurements were taken NWB (participant lying prone on a couch) and WB (participant standing), both with the feet and legs exposed. The MyotonPRO measured points at 2 cm intervals along the Achilles tendon with the first point 6 cm from the plantar aspect of the heel up to the proximal component of the musculotendinous junction for both groups of participants(figure 6).

Procedure figure: MyotonPRO measurements of participant non-weight bearing (left), participant weight bearing with points 1–8 (right).
The measurements correspond to previous anatomical studies of the Achilles tendon complex.25 A multiscan (comprising five measurements) was taken with the MyotonPRO. The median measurement was recorded at each point. In accordance with Myoton.com a measurement with a coefficient of variation less than 3% was accepted and any measurement above this recommendation was measured again. This was carried out to ensure reliability of data.
Data were imported from the MyotonPRO into Microsoft Excel and analysed using Minitab V.17 statistical software package and were found to be normally distributed using the Anderson-Darling method. Multiple comparisons between MyotonPRO measurement points were compared using the general linear model with adjustment for BMI, age and gender.
Results
Statistical analysis
General linear analysis demonstrated that age and gender affected stiffness values in the AT group only. Women presented with significantly lower F(Hz) value in the symptomatic group.
A two-sided t-test between points 1 and 8 of the AT group and the control group 1 demonstrated significant differences between the two data sets.
Natural oscillation frequency (Hz) (F)
The differences were significant (p<0.005) at NWB points f2, f3 and f4 (figure 1A) and WB points f2 and f3 of F (figure 1B), characterising the tonal properties of the tissues. There was a significant decrease in tone measured at these sites, representing 6 cm in length of the tendon.
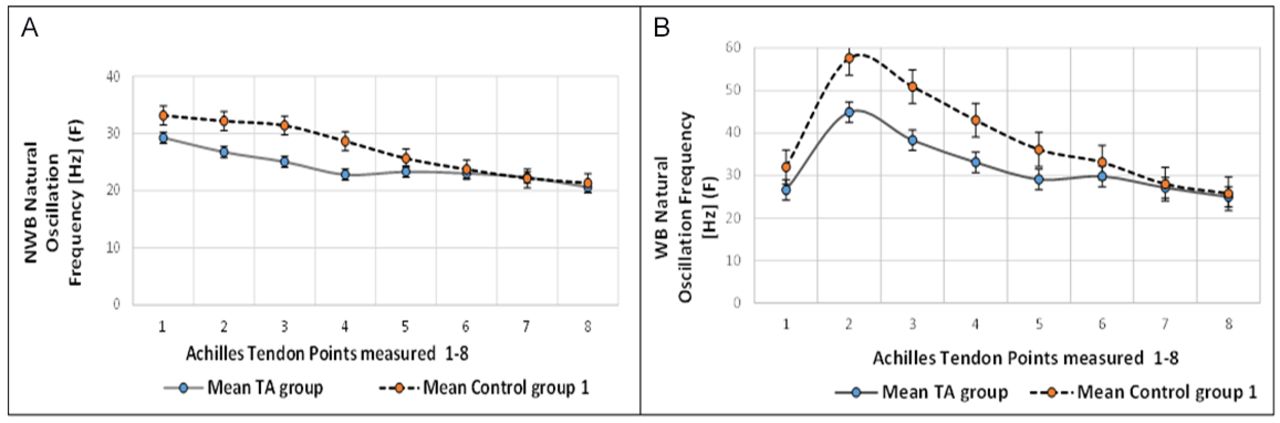
(A) Summary of points 1 to 8 for the natural oscillation frequency (F) measurement within subjects non-weight bearing (NWB). (B) Summary of points 1 to 8 for the F measurement within subjects weight bearing (WB).
A one-way analysis of variance of the symptomatic and asymptomatic data indicates a highly significant difference in the F scores, suggesting a significant reduction in the tonal properties (F) of the Achilles tendon along its course from its insertion in the calcaneum (point 1) to its musculotendinous junction (point 8). The mean tone (F) scores were higher in the WB group compared with the NWB group.
Logarithmic decrement (D)
The AT group WB demonstrated significantly increased points D 2 and 3 (figure 2B) corresponding to the tendinopathic site clinically. An increase in the D of tissues was observed in the AT group NWB signifying a decrease in elasticity. Figure 2A demonstrates the NWB symptomatic and asymptomatic data where D is increasing at each point measured. This suggests that the Achilles tendon becomes less elastic along its course.
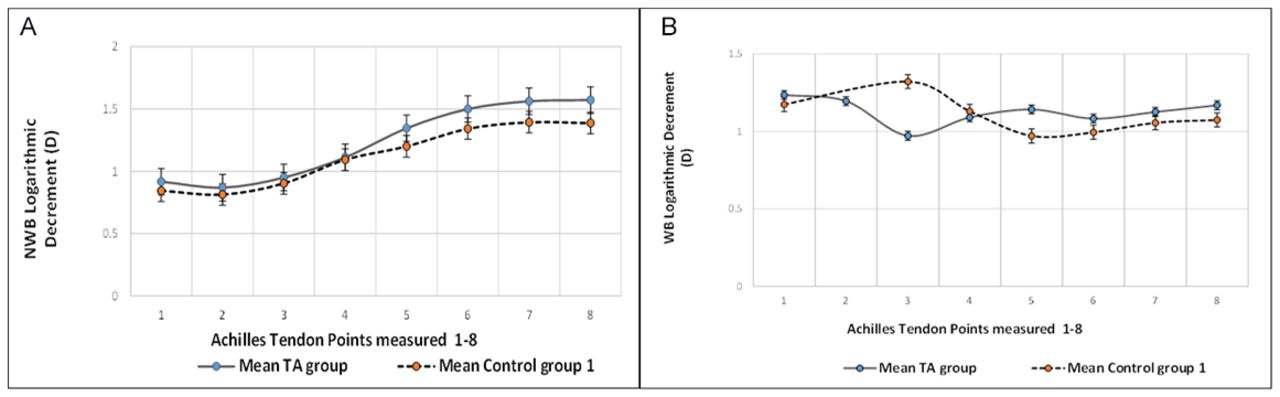
Summary of points 1 to 8 for the logarithmic decrement (D) measurement within subjects non-weight bearing (NWB) (A) and weight bearing (WB) (B).
Dynamic stiffness (N/m)(S)
The WB AT group presented with significantly decreased points S2 and S3 (figure 3B) and NWB S3 (figure 3A) and therefore decreased S of the tendon.

Summary of points 1 to 8 for the dynamic stiffness (S) measurement within subjects non-weight bearing (NWB) (A) and weight bearing (WB) (B).
Creep-ability (C)
Both WB and NWB conditions demonstrated decreased C scores along the course of the tendon from its insertion into the calcaneus at C1 to its musculotendinous junction at C8. There was an incremental increase in the points C1 to C8 NWB (figure 4A) and a decrease in points C1 to C5 WB suggesting a reduction in the creep (C) of tissues (figure 4B).

Summary of points 1 to 8 for the C measurement within subjects non-weight bearing (NWB) (A) and weight bearing (WB) (B).
Mechanical stress relaxation time (R)
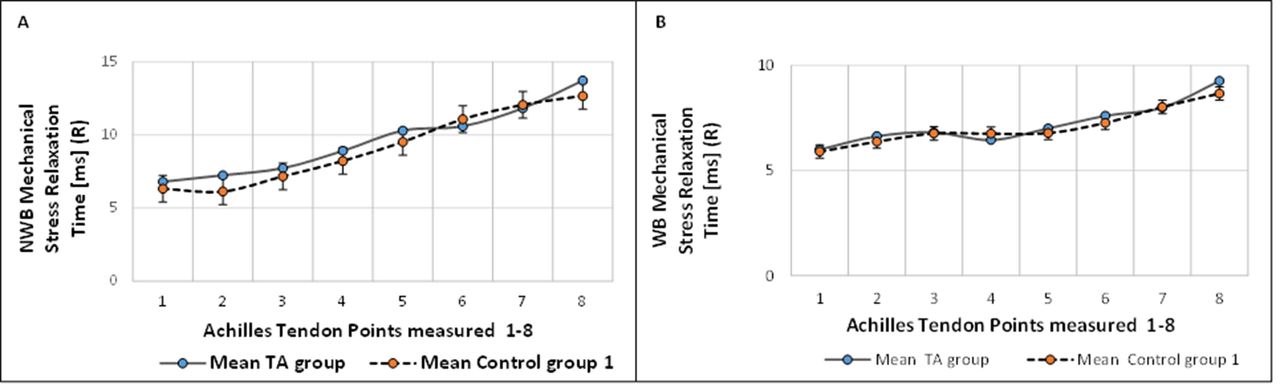
The NWB AT group demonstrated significantly (p<0.005) increased mechanical stress relaxation time (R) of point R2 (figure 5A), suggesting an increase in time taken by the tendon to return to normal shape following deformation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of points 1 to 8 for the R measurement within subjects non-weight bearing (NWB) (A) and weight bearing (WB) (B).
Effects of age, gender and BMI
Both age, gender and BMI were adjusted for their expected affects. Gender or age did not significantly affect scores in the control groups. However age and gender were significant covariates in the AT group. The mean BMI of the AT Group was 25.5 (range=14.5) and control group 2: 25.8 (range=14.8). The mean age of the AT group was 45.2 (range=49) years and control group 2: 39.6 (range=35) years. There were 17 women to 8 men in the AT group with 18 women to 7 men in the control group.
Control data
A two-sample t-test of the 25 participants in the control group 2 indicated that there were no significant differences (p<0.005) between left and right tendons within the group (WB and NWB). In addition to this, a two-sided t-test of control group 1 and control group 2 did not indicate any significant differences (p<0.005). This strongly suggests that the significant differences observed in the AT group between the symptomatic tendon and the asymptomatic tendon are as a result of the tendinopathic changes.
Discussion
Key findings
To our knowledge this is the first study to establish normative baseline values along eight points on the Achilles tendon WB and NWB using the MyotonPro in patients with Achilles tendinopathy and an asymptomatic control. A previous study demonstrating increased stiffness postkarate fight in the Achilles tendon, used one measurement point only on the soleus muscle and Achilles tendon 5 cm from its insertion.26 Another study using the MyotonPro to calculate normal values on healthy Achilles tendons and plantar fascia also only used one measurement point on the Achilles tendon and plantar fascia.18
The initial null hypothesis proposed that there would be no measurable mechanical changes with the MyotonPRO in patients with Achilles tendinopathy compared with participants that were asymptomatic and not diagnosed with Achilles tendinopathy. The experimental data do not support this hypothesis, as significant differences in the mechanical data were measured along the tendon. Across all five mechanical parameters measured with the MyotonPRO, seven WB points and four NWB points demonstrated measurable differences across points 2–4. These points correspond to a region of the tendon approximately 6 cm in length, which correlates with the focal tendinopathic swelling stated in the literature.9
The MyotonPRO measures components of tendon stiffness and viscoelasticity that is tone (F), logarithmic decrement (D)(characterising elasticity), dynamic stiffness (S), creep (C) and mechanical stress relaxation time (R) (Myoton.com). This study demonstrated that there was a significant decrease in Tone (F) along points 2, 3 and 4 NWB and 3 and 4 WB, of the symptomatic tendons within subjects of the AT group. It also demonstrated that two points measured in the AT group indicated an increase in logarithmic decrement and therefore a decrease in elasticity.27 Logarithmic decrement was measured to determine the damping (conversion of mechanical energy into thermal energy over the course of an oscillation cycle) of a structure.27 The damped oscillations characterising elasticity, reduce over time to achieve this. In addition, there was a decrease in the Dynamic Stiffness of the tendon in the AT group. Therefore, the measurements demonstrated a significant decrease in stiffness of the tendinopathic tendons. This supports a study using dynamometry and real time ultrasound on tendinopathic Achilles tendons which suggested that tendinopathy alters the mechanical properties and weakens the Achilles tendon.19 A degenerative tendon demonstrated lower stiffness and Young’s Modulus compared with healthy tendons. There is very little evidence for the characteristics of tendon viscoelasticity in the literature. However it is thought that the viscoelastic nature of soft tissue is likely to be due to the fluid flow and structural interactions within the extracellular matrix of tissue during loading.18 29 One further study which compared the viscoelastic properties of Achilles tendons with unilateral tendinopathy measured electromechanical delay, normalised rate of force development and hopping distance.28 This study concluded that the decreased viscoelastic properties of the affected tendon reduced explosive tendon performance in athletes.A component of viscoelastic behaviour measured in our study was creep, which is the deformation of tendon over time under a constant force.30 This is an important mechanical parameter which can predict tendon behaviour under transient loading and therefore the ability of the body to efficiently convert muscle contraction into movement.28 A review of existing literature reports testing of creep longitudinally in tendon.30 31 The measurement of creep carried out by the MyotonPRO is determined transversely. This does overcome some of the problems associated with in-vitro studies of longitudinal tendon loading, where positioning the axial loading of the tendon can often be problematic due to variability within tendon anatomy.31 However, likewise the measurement of transverse creep in the Achilles tendon, as with the MyotonPRO must also be brought into question. Particularly as we found no significant differences between the Control and AT Group for this parameter. In our study Achilles tendon Creep decreased from Point one until Point 8 of the NWB condition whereas the WB condition demonstrated an initial decrease in creep. A previous study which investigated the effects of creep and cyclic loading on the Achilles tendon (with the tendon longitudinally loaded) suggested that with increasing initial strain on the tendon there was an exponential decrease in creep.33 Suggesting strain as a primary mechanical parameter of tendon damage.
It has been hypothesised that the more elastic energy stored in muscle the less energy is lost at contraction or relaxation.13 The elastic tendon should recover its initial shape efficiently and in addition to this the elastic energy stored in muscle is used for dynamic movement. This demonstrates an important factor that a decrease in tendon stiffness results in higher strain, greater tendon elongation under a given muscle force and possible further damage to the collagen fibres through microtrauma.17 32 In contrast to this, excess tendon stiffness reduces tendon elongation in muscle contraction and impairs the elastic strain energy storage and release in tendons.33 These mechanical changes may reflect a loss of type 1 collagen fibres, loss of transverse bands of collagen fibres, increased crimping of collagen, loss of continuity of collagen fibres and production of mechanically weaker type 3 collagen.17
Age, gender and weight
This study suggests a correlation between body weight and gender on tendon mechanical properties, mainly in the AT group. There is some suggestion that the stiffness of the Achilles tendon is not correlated to body weight.32 Furthermore, it is noted that the difference in the Achilles tendon mechanical properties between men and women seems to be correlated to the difference in muscle strength, rather than gender.34 We believe that this is an important factor which should be considered in future research. A review of Achilles tendon and aponeurosis function in vivo has suggested there is a reduction in tendon stiffness with disuse.35 Although this may be reflected by the age variation of the study, no measure of exercise frequency was used in this study to validate this. Our study only found age as a covariance.
Asymptomatic data
Some studies have suggested that asymptomatic tendons may present with subclinical tendinopathic changes not perceived by the patient,4 therefore the asymptomatic control group 2 was introduced in our study. There were no significant differences in the measurements between control group 1 and control group 2.
Conclusion
We concluded that the Achilles tendinopathy reduces stiffness of the tendon body over a section of the tendon which correlates clinically with tendinopathy, supporting the concept that tissue mechanical properties are a marker for disease. The MyotonPRO is a useful clinical tool to quantitatively assess the tendon WB and NWB. Measuring the whole tendon complex rather than one site generated useful mechanical data which varied along its course. Age, gender and BMI appear to have some bearing on the mechanical properties of the tendon but only in the AT group.
This may have potential in identifying risk of injury and informing rehabilitation, however, further extensive research is required to generate baseline data for specific population groups monitoring variables over time.
Acknowledgments
The authors thank all subjects who participated in this research, the Research & Development Department, J Morgan for proof reading and all who supported this research project in Cwm Taf University Health Board.
References
Footnotes
Twitter @CwmTafPodiatry
Contributors GEM: chief investigator/lead author. RM: coauthor. LW: coauthor. OP: contributed to data collection. KM: statistical advice.
Funding This project was supported by Research & Development at Cwm Taf University Health Board.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was conducted according to the Helsinki Statement and was approved by local and national ethics committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data can be obtained from the corresponding author.