Article Text

Abstract
Background In sport, concussion is assessed using the Sports Concussion Assessment Tool (SCAT) 5 and managed with return to play guidelines. Similar, user-friendly tools are rarely, if ever, used in the emergency department (ED).
Objectives To evaluate a modified concussion assessment tool designed for the ED (ED-CAT) in patients presenting with a head injury and to identify variables that predict 30-day reattendance.
Methods A preliminary, prospective, evaluation in a quality improvement project was conducted in one hospital in South Wales. Patients were recruited if they were over 13 years, and either did not have an ED-CT head scan or had a scan with no acute changes. The primary outcome was 30-day reattendance.
Results 40 patients were recruited, 18 of whom had a CT scan. 37 were discharged on the same day with advice, two discharged the next day and one was admitted. Three (7.5%) patients reattended the department. Predictors of reattendance were headache score (median 3.0 vs 5.0; p<0.05), pressure in head score (2.0 vs 5.0; p<0.05), nausea/vomiting score (1.0 vs 3.0; p<0.05), dizziness score (1.0 vs 4.0; p<0.05), blurred vision score (0 vs 4.0; p<0.01), balance problems score (0 vs 4.0; p<0.05), sensitivity to light and confusion score (0 vs 4.0; p<0.01), orientation score (1. 0 vs 0; p<0.05) and immediate memory score (5.0 vs 4.0; p<0.05).
Conclusions Key symptoms and signs predicted 30-day reattendance. The ED-CAT requires validation and refinement in a larger population to produce a short, practical, user-friendly, relevant tool for ED head injury assessment.
- concussion
- head
- diagnosis
- sporting injuries
- study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
A tool designed for concussion assessment within the emergency department (ED) was able to be developed by modifying the Sports Concussion Assessment Tool 5.
Key symptoms and traits on the tool were able to identify reattenders to the ED.
How might it impact on clinical practice in the near future
With further development, this tool may be used in the ED to identify those suffering a more severe concussive episode.
Introduction
Concussion is one of the complications of a head injury, a common presentation to the emergency department (ED).1 Evidence in the UK is lacking, but the presentations of concussion to the ED in America has been estimated to be over 150 000 annually.2 Another study reports that around 100 000 patients per year present to the ED in just the 8–19 age group in America.3 In sport, where there is more evidence, incidence is highest in rugby and ice hockey.4
The operational definition of concussion as the ‘immediate and transient symptoms of mild traumatic brain injury’ but this has drawn criticism due to a lack of accuracy.5 The Concussion in Sport Group (CISG)6 defines concussion as a ‘complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces’. This may be due to a blow to the head or body that leads to the rapid development of neurological impairment that does not last long and resolves of its own accord.6 The acute symptoms are less likely to be due to structural injury and therefore are associated with grossly normal neuroimaging. However, concussion may cause neuropathological changes.6 The clinical and cognitive symptoms (of which loss of consciousness may be included) of concussion and its sequelae typically resolve gradually.6 The initial effects of concussion cover a large spectrum of symptoms.7 The CISG7 list these over certain ‘clinical domains’. These include somatic/cognitive/emotional symptoms, physical signs such as loss of consciousness, balance impairment, behavioural changes, cognitive impairment and sleep/wake disturbance.7 The CISG advise that concussion should be suspected if any of the symptoms are present, but acknowledge that they are non-specific.7
In sport, concussion is routinely assessed using the Sports Concussion Assessment Tool (SCAT) 58 which has been adopted by many sporting bodies.9 The SCAT requires a clinical judgement to be made by the examining clinician based on the scores from each section of the assessment; it does not simply identify those who are concussed.9 Recommendations for sports-related concussion management have been summarised by the CISG in the graduated Return to Play guidelines (see online supplementary appendix 2).7
Supplemental material
The National Institute of Clinical Excellence (NICE)10 in 2014 published detailed recommendations for patients presenting to the ED with a head injury. However, concussion receives little attention. The main assessment in the ED is to identify if the patient needs a CT head scan according to the Canadian CT head rule.11 There is no routinely used, formal assessment for concussion. The mainstay of management for concussion is discharge with advice regarding red flag symptoms, head injury leaflets and no follow-up.12 13 Concussion advice in the ED is minimal compared with Return to Play guidance for athletes.7 This may partly be due to time pressure and partly due to prioritisation perspective, as the priority for ED is to rule out life-threatening events.13
It is important not to miss concussion. Athletes who have had a concussive episode are at higher risk of re-injury, further concussive episodes in the same season,14 second impact syndrome, postconcussion syndrome and long-term neuropsychological effects.15 Repeated concussions can lead to neurodegenerative changes, a disease process known as chronic traumatic encephalopathy.16 17 Those that return to normal activities too early are at risk of these complications.15
There is little evidence about concussion in the general public or in recreational sport, which also means it is often poorly managed in these populations.18 Data collection systems need improving in the community and in the ED.19 This could be achieved by introducing the SCAT into the ED as an adjunct to the clinical diagnosis of concussion.12 20 However, the SCAT is long and cumbersome and unlikely to be adopted in busy EDs. However, a shorter, simpler, evidence-based assessment tool could be adopted.
There is currently no generally well-accepted, objective tool for recognising concussion in the ED. Tools have been developed, such as the Acute Concussion Evaluation form,21 but these have not been adopted in the ED setting. The objectives of this study, in patients presenting to the ED with a head injury, are to evaluate a potential ED concussion assessment tool investigating which variables predicted 30-day reattendance. This tool may help identify those patients with a more severe concussion who may benefit from follow-up
Methods
Design, setting and participants
As part of a quality improvement programme to improve head injury and concussion assessment in the ED, we have conducted a preliminary, prospective, single-centre study to assess concussion in the ED. Participants were recruited if presenting to the ED of a major teaching hospital in South Wales with a head injury from 25th November 2017 to 22nd January 2018. To be recruited, patients had to present between 08:00 and 17:00 Monday–Friday, when the primary researcher was present. Patients were eligible if aged ≥13 years and either not requiring a CT head scan or with a negative CT scan. Patients were excluded if they had acute changes on CT scan. The methodology of the study is demonstrated in figure 1. The model and cycle specific for this project is shown in online supplementary appendix 4.
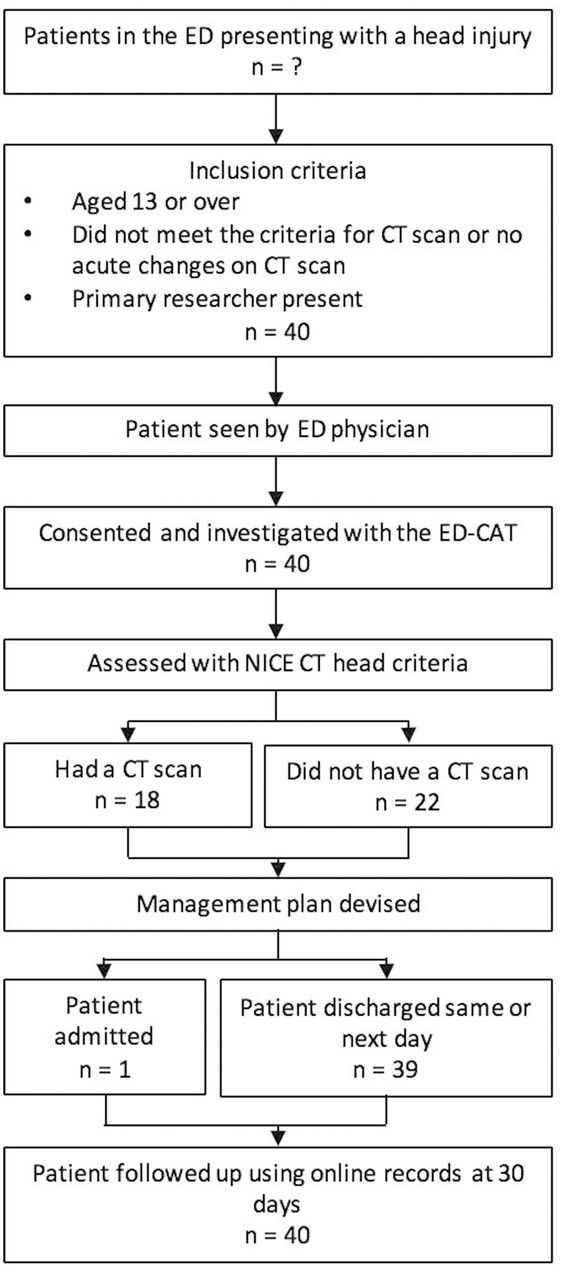
Flow chart showing the methodology of the study.
The assessment tool and data collection
The SCAT5 form was modified in order to produce a suitable form for use in the ED—the Emergency Department Concussion Assessment Tool (ED-CAT; see online supplementary appendix 3). The sections used for immediate/on field assessment from SCAT5 were removed and some sections were shortened. It still retains several sections, which include patient details, orientation, immediate memory, symptom screen, balance examination and delayed recall. The SCAT5 is restricted to those over the age of 13, hence why the age cut-off for this study was the same. A summary of each section can be found in table 1.
Summary of each section of the Emergency Department Concussion Assessment Tool
After the patients were clerked and assessed by an emergency physician, they were verbally consented for the study and assessed using the ED-CAT. The original attending emergency physician then made decisions about whether the patient required a CT scan and about further management. Patients were encouraged to return to the ED if symptoms had not resolved in 3–4 weeks.
Outcomes and follow up
The primary outcome for this study was 30-day reattendance to the ED. This was achieved by scanning the online patient records. Correlations were also analysed between the ED-CAT scores and likelihood of requiring a CT scan.
Statistical analysis
The data collected was analysed using the Mann-Whitney U test, a univariate non-parametric analysis. IBM SPSS Statistics (IBM Corp. Released 2015. IBM SPSS Statistics for Mac, V.23.0. Armonk, New York: IBM Corp.) and MedCalc (MedCalc Software, V.15.8, Ostend, Belgium) were used.
Results
A total of 40 patients were recruited for the study. All 40 were followed up using online patient records. Patient flow through the study is demonstrated in figure 1.
Baseline characteristics, scores on ED-CAT and hospital management
The baseline characteristics of all 40 participants are shown in table 2, as well as the total scores for each section on the ED-CAT form.
Participant’s characteristics*
Primary outcome—30-day reattendance
Of the 40 patients, three (7.5%) reattended the ED within 30 days of their initial assessment. Two patients reattended once and one reattended twice. This patient first reattended the same day due to vomiting and returned 28 days later due to dizziness. The reason for the other two participants reattending was because of worsening symptoms and the other started to develop dysphagia and right lower limb paresis and paraesthesia. This patient did not have a CT head scan initially but did so on their second attendance (as well as a CT cervical spine scan) but it showed no acute changes. They were admitted to hospital for 7 days before their symptoms cleared and they were discharged with concussive trauma.
Participant demographics, total scores for each section on the ED-CAT and management in the ED is shown in table 3 and the individual breakdown of each section on the ED-CAT is shown in table 4, compared with whether they reattended within 30 days.
Summary of patient demographics, scores on Emergency Department Concussion Assessment Tool and management in the emergency department*
The individual breakdown of participant scores on the Emergency Department Concussion Assessment Tool*
The sections on the ED-CAT, which showed a significant difference in medians between reattenders and non-reattenders, were the orientation total score (step 2), orientation to date and time, one of the immediate memory trials, eight of the 22 symptoms and the sum of symptoms severity in step 4. The eight symptoms were headache, pressure in head, nausea or vomiting, dizziness, blurred vision, balance problems, sensitivity to light and confusion.
Correlations between variables—ED-CAT scores and CT scan
Of the 40 patients, 18 were investigated with a CT scan in the ED as per the NICE criteria, none of which had acute changes. When comparing total scores on each section of the ED-CAT and whether or not the patient had the scan showed only one significant result, the balance examination score (step 5). This showed that those who met the criteria scored significantly lower and therefore demonstrated worse balance (median scores of 14.00 vs 35.00).
Management in the ED
Thirty-seven patients were discharged from the ED the same day with head injury advice and a leaflet. Two patients were discharged the next day from the ED. One patient was admitted for 2 weeks due to frailty. Six patients were unable to perform the balance examinations (step 5), either due to unsteadiness or dizziness, and one patient had sustained an undisplaced ankle fracture as well as a head injury in a motor vehicle collision. These patients scored 0 on the balance examinations as a result.
Discussion
This prospective preliminary quality improvement project is one of the first studies looking into concussion assessment in an ED setting using an appropriate tool (the ED-CAT) modified from the SCAT5. This study has demonstrated that scores on certain sections of the ED-CAT were more likely to correlate to a reattendance to the department within 30 days of the original presentation. This may suggest that the concussion experienced by these patients was more severe.
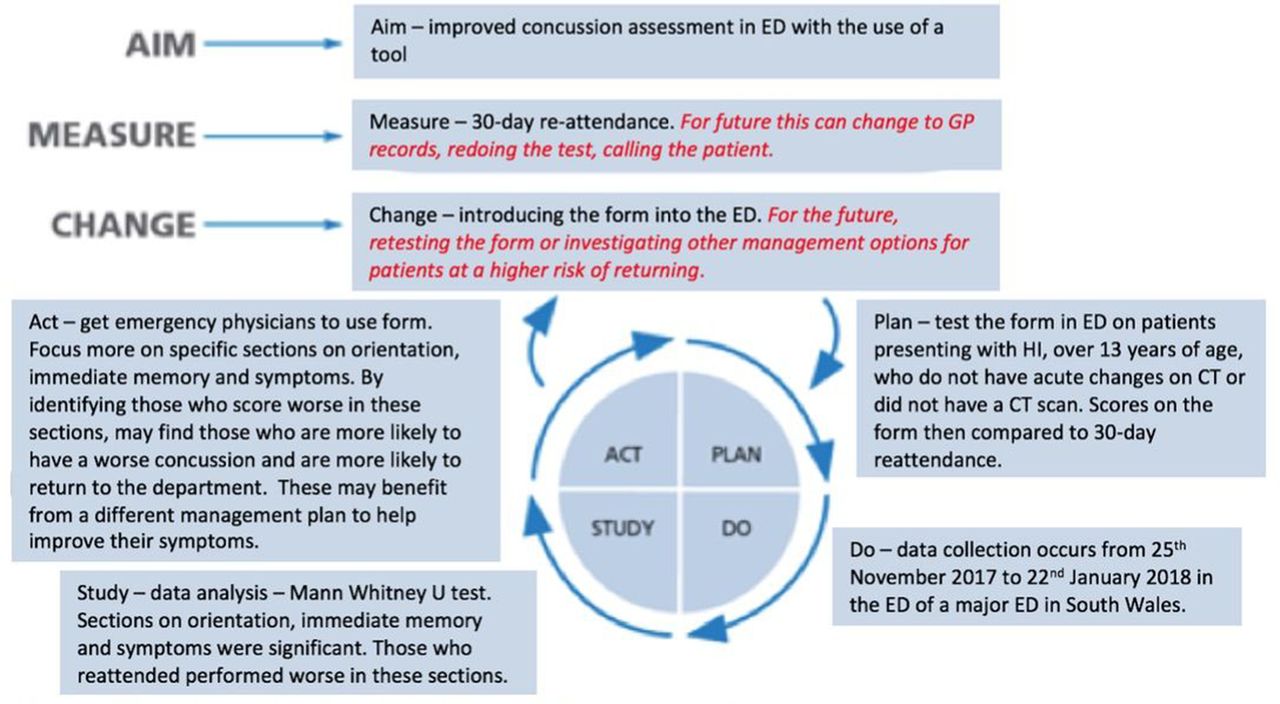
Quality improvement projects are continuously improving processes used to achieve high quality care.22 They involve several elements which are summarised by the model of improvement and plan, do, study, act cycle. They tend to be more effective than traditional audits as a series of interventions and adaptations can be assessed quickly. This project is the first initiative in the quality improvement process aiming to improve concussion assessment in the ED. The cycle (see online supplementary appendix 4) allows for further improvement to be made specifically, to validate the form and test the form using other clinical outcomes (figure 2).

{kind=link}
{kind=link}
Plan, do, study, act cycle for this quality improvement project.7
The ED-CAT is one of the first forms to aid the assessment of concussion in the ED. It does not include the immediate acute tests that are present in the SCAT5 such as the ‘on field assessment’. This makes it suitable to use when patients have self-presented to an ED sometime after their original injury. Some sections of the SCAT5 were shortened, so that ED-CAT was suitable to use in a busy ED where assessing patients efficiently and safely discharging them is critical. The ED-CAT consists of five scoring sections which are orientation, immediate memory, symptom screen (which is split into number of symptoms and symptoms severity score), balance examination and delayed recall. As each section is scored differently (which may cause some confusion), the tool cannot produce a total score to sum up how the patient performed on the assessment. The orientation, immediate memory, balance examination and delayed recall sections are scored such that a higher score means the patient has performed better on this section. Whereas for the number of symptoms and symptom severity scores, a higher score indicates worse symptoms. The scores should be considered together as part of the overall clinical picture (as is advised by the CISG when using the SCAT59). It must be noted that the balance examination was changed from the modified Balance Error Scoring System (mBESS) on the SCAT5 from 20 s to 10 s and the scoring system was reversed. This is not validated; however, the SCAT5’s methodology and scoring system is. It is recommended for future studies to revert back to modified BESS employed by the SCAT5.
Our study has showed that the orientation score, symptom severity score and parts of the symptom and immediate memory sections were able to predict worse outcomes. Patients who reattended the ED within 30 days were significantly more likely to have worse orientation overall as well as worse scores for orientation to date and time; remember less words on the third trial of the immediate memory test (4 words vs 5); be experiencing more severe symptoms of headache, pressure in head, nausea or vomiting, dizziness, blurred vision, balance problems, sensitivity to light and confusion and have a worse overall symptom severity score (67 compared with 26). As these sections were able to predict 30-day reattendance, they may be able to predict worse concussive syndromes. Emergency physicians may be able to use the form to identify these patients and modify their management plan to reduce the chance of them reattending.
In a previous systematic review on concussion assessment involving 33 studies and 2416 athletes, it was found that a symptoms-based approach is best when trying to identify sports-related concussion.23 Symptoms most frequently reported were ‘headache’, ‘fatigue’, ‘difficulty concentrating’ and ‘dizziness’; two of these symptoms predicted reattendance in our study. They concluded that acute assessment of sports-related concussion should involve neurological, vestibular, ocular motor, visual, neurocognitive, psychological and cervical aspects,23 which the ED-CAT attempts to do in conjunction with a history and full examination. Hänninen et al,24 in a prospective cohort study of 27 professional ice hockey players, investigated the validity of the SCAT3. They reported that the symptom section of the SCAT3 was the most sensitive in identifying concussed athletes immediately post-injury and the most common symptoms reported were ‘don’t feel right’, ‘headache’ and ‘pressure in head’.24 An observational case series into the SCAT3 involving 167 patients found that common symptoms reported by athletes included ‘headache’, ‘balance problems’ and ‘don’t feel right’.25 The symptoms most frequently reported in these three studies show some resemblance to the significant findings in this study, with headache being a common theme. However, some caution must be used as these papers investigated concussion assessment immediately postinjury in athletes. Our study investigated sports and non-sports related concussion with a mean time period between injury and assessment being 45 hours; so, these two populations are not completely comparable. It is worth noting that only five of the 40 cases in this study were sports related.
Our secondary analysis interestingly showed a significant correlation between poor balance and meeting the criteria for a CT head scan. However, it is unlikely that this is going to affect practice as there is already a well-accepted criteria in place for assessing the need for a CT scan post head injury.10 11
Strengths and limitations
The primary strength of this quality improvement project is the development of a form that aids concussion management, suitable for patients over the age of 13 who present to an ED with a head injury that can predict reattenders. This is the first step to improving the assessment and management of concussion within the ED. Another strength is that one examiner was used and therefore the assessment of each patient was consistent throughout the study.
There are several limitations to this study. Apart from the small sample size, it relies on the assumption that 30-day reattendance to the ED correlates with worse symptoms or a more severe concussion. There were a limited number of positive results, and we were unable to perform multivariate analysis. Unfortunately, other forms of patient follow-up could not be performed due to ethical implications. Future studies should seek to follow-up patients by contacting them 30 days after initial assessment, checking their general practitioner records or reassessing them using the ED-CAT. The time period for follow-up could also be extended beyond 30 days. Convenience sampling was employed during this study, which meant a large section of patients may have been missed out who attended outside the hours when the data collector was not present. Further, this study was performed in a single centre. Future studies should include other hospitals and healthcare systems.
Another limitation of this study, which makes concussion assessment in the ED very difficult, is that we could not compare the postinjury scores of these patients to baseline scores (preinjury).24 25 One of the findings by Hänninen et al 24 was that there was no statistical difference between comparing baseline scores or normative reference scores (devised by the professional league) with the athlete’s scores from the day of the injury. Use of reference scores would be useful in the ED, where there is no or little chance of using baseline scores. However, these normative reference scores should take into account age, sex, mechanism of injury and risk factors as a minimum. It may take a while to develop these, but this could be a source of future research to aid ED concussion assessment.
Improvements and studies for the future
Future research should involve expanding this study on a much larger scale. This would ideally be multicentre, not use convenience sampling, have a larger sample size and would need more positive cases. This would therefore enable a more advanced analysis to occur. Power sample size calculations were performed for this study (see online supplementary appendix 5) to show how large a sample size is required if this study was to be repeated. These were performed for each individual section of the ED-CAT and as a result, a range of sample sizes were produced. These ranged from 76 to 1514 for the main sections of the ED-CAT. For future studies, over 400 patients would be required for the study to be powerful enough to validate four of the five sections on the ED-CAT.
It is likely that the current ED-CAT is still too long for implementation in most EDs. Larger studies will confirm those variables that contribute little to concussion assessment in the ED, which can be removed.
Another simple initiative the ED can employ is better discharge advice for those suspected with concussion on top of a head injury leaflet. As we explored earlier, discharge advice for concussion is minimal.12 13 26 A specific concussion leaflet to be given out in the ED explaining what is it and how to effectively manage the symptoms including return to work or study guidance, similar to the Return to Play guidelines for athletes,7 may help standardise discharge advice.
Conclusion
This quality improvement project has shown that key symptoms, signs and traits highlighted by the ED-CAT were more sensitive to 30-day reattendance in patients over the age of 13 presenting to the ED with a head injury. These sections showed reattenders to have worse orientation, immediate memory and symptoms. These sections therefore may help identify those suffering from a more severe concussion to emergency physicians assessing them in the ED. These patients could then benefit from an altered management plan to aid their recovery from concussion.
Acknowledgments
The authors would like to thank Dr Bethan Nicholas for her help and advice, and the staff in the ED at one of the major teaching hospitals in South Wales for their cooperation during the study. This work was previously presented at the AWSEM 2018 Academic Conference in Wrexham.
References
Footnotes
Contributors DAM contributed to the acquisition of data and manuscript writing. THR contributed to the supervision and advice. DAM and THR contributed to the study design, data analysis and interpretation, project administration and statistical analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethics was waived as this was part of a quality improvement project, which does not require consent in our institution. All patients were anonymised and no personal or telephone follow-up was employed.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no unpublished data from this study. Only the authors have access to the data. To obtain the data please contact the corresponding author.