Article Text

Abstract
Objectives To identify the components, and assess the reporting quality, of exercise training interventions for people living with pulmonary hypertension.
Design Systematic review with analysis of intervention reporting quality using the Consensus on Exercise Reporting Template (CERT).
Data sources Eligible studies in the Cochrane Systematic Review of exercise-based rehabilitation for pulmonary hypertension, updated with a new search of relevant databases from 1 August 2016 to 15 January 2018.
Eligibility criteria Peer-reviewed journal articles of randomised and non-randomised controlled trials, and non-controlled prospective observational studies, investigating dynamic exercise training interventions in adult humans with diagnosed pulmonary hypertension, reporting on at least one physiological and/or psychosocial outcome.
Results Interventions typically involved cycle ergometry and walking. They were delivered as 3-week inpatient, or outpatient and/or home-based programmes, lasting for 4–15 weeks. Components relating specifically to exercise prescription were described satisfactorily and in more detail than motivational/behavioural change strategies, adherence and fidelity. Mean CERT score was 13.1 (range 8–17) out of a possible maximum score of 19. No studies fully reported every aspect of an exercise intervention to the standard recommended by CERT.
Summary/conclusion Considerable variability was evident in the components and reporting quality of interventions for exercise rehabilitation studies in pulmonary hypertension. Interventional studies using exercise training should pay greater attention to describing motivational/behavioural change strategies, adherence and fidelity. Detailed description of these parameters is essential for the safe and effective replication of exercise rehabilitation interventions for pulmonary hypertension in clinical practice.
Trial registration number CRD42018085558.
- Consensus on Exercise Reporting Template (CERT)
- exercise rehabilitation
- pulmonary hypertension
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary
The reporting of exercise intervention components in clinical populations is often inadequate.
The Consensus on Exercise Reporting Template (CERT) is a useful tool with which exercise intervention reporting can be standardised.
Exercise prescription for people living with pulmonary hypertension is relatively well reported although no studies reported adequately on all CERT criteria.
Motivational strategies, exercise adherence and intervention fidelity are poorly reported in pulmonary hypertension studies.
Introduction
Pulmonary hypertension is a debilitating long-term condition characterised by severe exercise intolerance.1 Pulmonary arterial pressure is abnormally raised due to dysfunctional endothelial cells and vascular smooth muscle, leading to maladaptive pulmonary vascular remodelling and increased right ventricular afterload.2 3 Pulmonary and cardiovascular haemodynamics are progressively compromised, often during minimal physical exertion.4 5 Consequently, exertional dyspnoea, fatigue and syncope are the most common symptoms, impacting profoundly on quality of life (QoL), morbidity and mortality.6 Guidance from the World Symposium on Pulmonary Hypertension7 identified five distinct subgroups: group 1—pulmonary arterial hypertension (PAH), group 2— pulmonary hypertension due to left heart disease, group 3—pulmonary hypertension due to lung diseases or hypoxia, or both, group 4—chronic thromboembolic pulmonary hypertension (CTEPH), and group 5—pulmonary hypertension with unclear multifactorial mechanisms.
There are many similarities between pulmonary hypertension and conditions like chronic obstructive pulmonary disease and chronic heart failure; indeed, they often coexist.6 Exercise therapy improves exercise tolerance and QoL for people living with these conditions; therefore, it is plausible that it will also help people living with pulmonary hypertension. Specific exercise therapy guidelines to maximise physiological and psychosocial gains, while ensuring safe participation, are available for some clinical conditions; for example, post-myocardial infarction8 or chronic obstructive pulmonary disease.9 Such robust recommendations are not available for pulmonary hypertension. Nevertheless, a 2017 Cochrane Review and meta-analysis found a meaningful short-term improvement in exercise capacity from participation in partly supervised, exercise-based, rehabilitation for people with moderately severe pulmonary hypertension; although from low-quality evidence.10 QoL (SF-36) also improved, but the authors concluded that the magnitude of change may be insufficient to be clinically important.
To develop appropriate exercise training guidance for people with pulmonary hypertension, an understanding of exercise intervention components is essential. Systematic reviews commonly pool data from heterogeneous exercise training protocols, which may dilute the relevance and applicability of findings. Recent Cochrane Reviews of exercise-based rehabilitation in cardiac and pulmonary disease, while indicating the potential for benefit, were limited by the quality and diversity of exercise training interventions.11 12 Replication of safe and effective clinical exercise therapy is reliant on access to detailed description of exercise intervention components. Information on important aspects of an exercise intervention, for example, setting, facility, equipment, frequency, intensity, duration, modality, adherence, fidelity and safety, is required for subsequent implementation. Such reporting is often poor, which may question the validity of published exercise protocols and prevent safe and effective adoption of successful interventions. The Consensus on Exercise Reporting Template (CERT), recently developed and endorsed by an international panel of experts, allows standardised appraisal of published exercise rehabilitation interventions.13 14 This document provides guidance on the minimum reporting standard considered necessary to allow replication of exercise interventions. Not only can this tool be used to retrospectively assess reporting quality, it can also help with protocol development. While it is not intended to assess the scientific and methodological quality of studies per se, it should facilitate standardised reporting of exercise interventions and aid translation of research findings into everyday clinical practice
The aim of this review was to assess both the components and reporting quality of studies investigating exercise-based rehabilitation in pulmonary hypertension. To ensure a standardised appraisal, we used the CERT. Collating the components of published exercise interventions also allowed us to make inferences as to future clinical research priorities in the field of exercise programming and prescription for people with pulmonary hypertension.
Methods
We first examined the included and excluded studies of the 2017 Cochrane Systematic Review of exercise-based rehabilitation in pulmonary hypertension.10 We replicated this search, with some amendments, searching for original research published in academic journals as full-length, independently peer reviewed, randomised controlled trials (RCTs) and non-randomised controlled trials, and non-controlled prospective observational studies investigating exercise training interventions in adults with pulmonary hypertension. Inspiratory/respiratory muscle training was only included where it formed part of an intervention which also employed dynamic exercise training. The included studies must have tested the effect of a dynamic exercise training (aerobic or strength) intervention on at least one physiological and/or psychosocial parameter. We did not place any restriction on publication language or study design, other than excluding case reports. We also excluded abstracts and conference proceedings as they do not qualify as full-length original articles, which the CERT checklist was designed to appraise. Shorter communications, such as abstracts, do not contain sufficient detail to enable scoring with CERT. The identified literature was hand-searched for additional publications. Subsequently, we updated the search to cover the period 1 August 2016 to 15 January 2018 using the following databases (online supplementary appendix 1):
Supplemental material
The Cochrane Airways Register of Trials.
Cochrane Central Register of Controlled Trials (CENTRAL) via the Cochrane Register of Studies.
Medline (Ovid).
Embase (Ovid).
Physiotherapy Evidence Database (PEDro).
Two reviewers (GM and RP) determined eligibility by independently screening titles and abstracts. Where discrepancy relating to study inclusion existed, a consensus was reached through discussion and consultation with a third reviewer (SF). All eligible full-text articles were acquired to allow assessment with the CERT. Two reviewers (GM and RP) extracted all intervention component data to summarise each study in a standardised fashion (1).
Two assessors (GM and SF) independently reviewed each extracted manuscript using the 16-item CERT checklist.13 Each item was scored ‘1’ (adequately reported) or ‘0’ (not adequately reported), and a score out of a total of 19 was calculated. Where studies cited methodology from previous work, information from the cited paper was also included in the score. We referred to the CERT examples of ‘good reporting’ to ensure scoring was standardised. Together, both assessors reviewed each of the 16 items for each of the extracted manuscripts to compare scores. Discrepancies were resolved through discussion between the two reviewers and further reference to the CERT Explanation and Elaboration Statement.13 The review was conducted in accordance with PRISMA guidelines and was registered with PROSPERO (2018 CRD42018085558).
Results
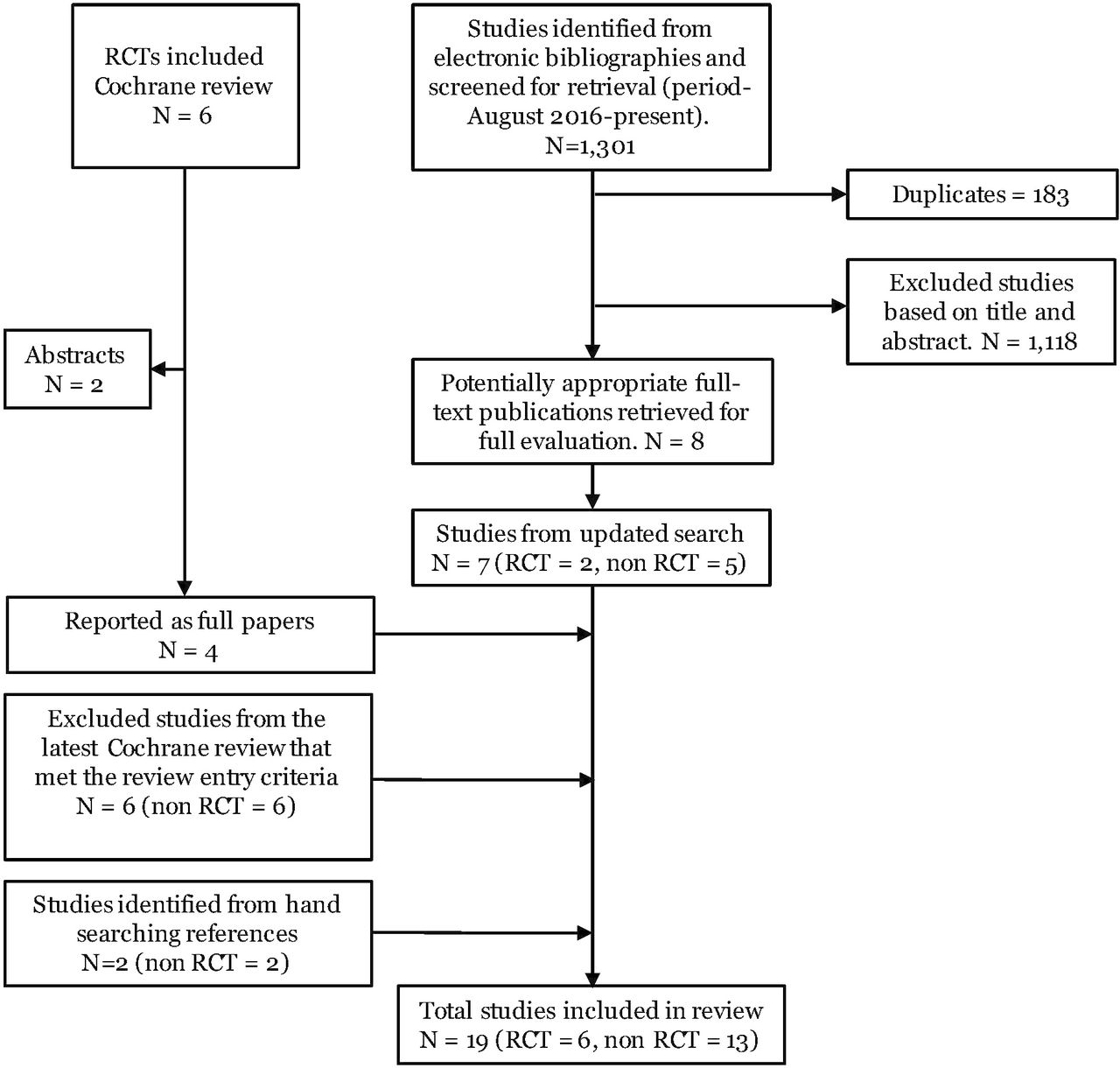
We included 19 studies, 6 of which were RCTs,15–20 3 non-RCTs21–23 and 10 non-controlled, prospective observational studies24–33 (figure 1). Mean sample size was 35 (range 5–183) participants. Pulmonary hypertension aetiology classification was varied: eight studies exclusively enrolled group 1,15 ,20 23 26 28 29 31 32 none groups 2 and 3 only, three group 4 only,22 24 30 two group 5 only,25 27 five groups 1 and 4, and one was mixed.33 Intervention content (online supplementary table 1) was heterogeneous. In total, 2 studies (2/19; 11%) prescribed dynamic exercise training only,15 20 5 studies (5/19; 26%) dynamic exercise training in combination with resistance training21–23 25 27 and 12 studies (12/19; 63%) a multimodality intervention consisting of dynamic exercise training, resistance training and respiratory muscle training.16–19 24 26 28–33 All studies delivered an intervention that was supervised in an inpatient or outpatient setting, with 10 incorporating an inpatient phase. Eleven studies (11/19; 58%) combined unsupervised home-based exercise training with supervised sessions or used home-based as a continuation beyond centre-based exercise.16 18 19 22 24 28–33 Most studies (16/19; 84%) used cycle ergometry as the main modality of dynamic exercise, delivered alone or in combination with walking and/or step climbing. Three studies used walking as the predominant modality of training.15 20 24 There was considerable variation in the duration of the exercise intervention. Programmes lasted 4,26 8,17 10,15 20 1221–25 27 or 1516 18 19 28–33 weeks. Session duration, frequency and intensity were well described in all studies. Most studies detailed the methods of progression, and the use of heart rate, oxygen saturation and subjective measures (perceived dyspnoea and physical exertion) to adjust training intensity. All but four studies, which used exercise training as a stand-alone intervention,17 19 25 27 adopted a multidisciplinary approach, combining exercise training with additional educational and psychosocial components (15/19; 79%).
Supplemental material

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. RCT, randomised controlled trials.
CERT scores ranged from 8 to 17 (mean 13.1) out of a possible maximum score of 19 points (figure 2). No studies adequately described all aspects of exercise interventions in accordance with CERT (figure 3). We detail the standard of reporting for each criteria below.

Consensus on Exercise Reporting Template (CERT) score by paper.

{kind=link}
{kind=link}
{kind=link}
Quality of exercise intervention reporting as assessed with the Consensus on Exercise Reporting Template (CERT).
Question 1: detailed description of the type of exercise equipment
While it was common to describe the mode of activity for example, cycle ergometry or walking, only one study included the make and model of the exercise equipment used.17
Question 2: detailed description of the qualifications, expertise and/or training
Fifteen studies (79%) identified the specific discipline delivering the exercise intervention, for example, physiotherapist, and the presence/nature of medical supervision, for example, respiratory physician. Other than stating ‘experienced’ or ‘specialist’, only three studies described any additional postgraduate training or relevant continued professional development, undertaken by staff, or the extent of the experience required.
Question 3: describe whether exercises are performed individually or in a group
This was poorly described, but in most studies the description of the intervention was sufficient to imply the format, hence 14 studies (74%) met this criterion.
Question 4: describe whether exercises are supervised or unsupervised; how they are delivered
Eighteen studies (94%) reported the presence or absence of supervision but limited detail was provided. As these studies reported face-to-face supervision, there was less need to provide additional detail.
Question 5: detailed description of how adherence to exercise is measured and reported
The methodology for measuring adherence was not well described, as was the case for the level of adherence achieved in the studies. Only six studies (32%) reported this adequately, by first describing a priori how adherence would be assessed, and second, confirming the level of participant adherence in absolute or relative terms.
Question 6: detailed description of motivation strategies
Only one study provided adequate information relating to any motivational strategies and behavioural change interventions used to complement exercise training.26 In this study, while not exhaustive, sufficient detail was included to allow informed assessment of effective motivational strategies in this population.
Question 7a: detailed description of the decision rule(s) for determining exercise progression; 7b: detailed description of how the exercise programme was progressed
The decision rule(s) for progression were defined in 17 studies (90%). Nevertheless, six studies (32%) did not provide sufficient information regarding how exercise programmes were actually progressed in practice.
Question 8: detailed description of each exercise to enable replication
All programmes consisted of walking and/or cycling, requiring very little detailed instruction. Where additional exercise such as resistance training, respiratory muscle training or yoga was prescribed, this was generally well defined. Information regarding dumbbell weight (kg), lifting technique and/or a specific respiratory muscle training protocol was often thorough and detailed.
Question 9: detailed description of any home programme component
Home exercise programmes were secondary components of centre-based interventions in all but one study which primarily tested home-based rehabilitation in pulmonary hypertension, with a secondary centre-based component.24 As such, reporting was generally of a low standard.
Question 10: describe whether there are any non-exercise components
Overall, a clear description of non-exercise components was provided. Sixteen studies (84%) contained a structured educational, physical and psychological disease self-management programme alongside the exercise intervention.
Question 11: describe the type and number of adverse events that occurred during exercise
Sixteen studies (84%) described this aspect well, using predefined criteria, and relating adverse events to clinical outcome and the impact on participant completion of the exercise intervention. Most also made reference to whether or not adverse events were related to the intervention itself.
Question 12: describe the setting in which the exercises are performed
Clearly and concisely reported in 18 studies (95%).
Questions 13: detailed description of the exercise intervention; 14a: describe whether the exercises are generic (one-size-fits-all) or tailored; 14b: detailed description of how exercises are tailored to the individual
All studies provided adequate detail of the exercise intervention. Within this criterion there was considerable variability in the level of detail, but all were deemed adequate in line with CERT recommendations. The intended method of exercise tailoring (individualisation) was also well described in all studies.
Question 15: describe the decision rule for determining the starting level
Primarily from cardiopulmonary exercise testing (a common and informative test in the pulmonary hypertension population), 18 studies (95%) indicated methods for initial exercise prescription.
Question 16a: describe how adherence or fidelity is assessed/measured; 16b: describe the extent to which the intervention was delivered as planned
No studies adequately reported how therapist adherence to appropriate protocol delivery would be measured; however, 12 studies (63%) referred to issues experienced by therapists which in practice could have led to suboptimal intervention deliver
Discussion
Using the CERT, we assessed the quality of exercise intervention reporting in 19 studies investigating the effect of exercise-based rehabilitation in people with pulmonary hypertension. Our main findings were (1) exercise prescription components in pulmonary hypertension rehabilitation were, overall, relatively well defined, and (2) motivational and behavioural change strategies, adherence and intervention fidelity were inadequately described. Formal analysis of data relating to efficacy, safety or clinical outcomes was not within the scope of this review. However, our appraisal of the literature did allow us to make broad recommendations for future clinical research priorities investigating exercise-based rehabilitation for people with pulmonary hypertension.
A striking observation was that 10/19 studies reported a 1-week to 3-week inpatient rehabilitation period prior to an outpatient and/or home-based programme. Due to differences in healthcare provision, this is unlikely to be a plausible treatment option for most people with pulmonary hypertension. As an alternative, outpatient programmes provided at local facilities, offering an hour of exercise, two to three times weekly, are likely to be more feasible. However, the efficacy of this approach is yet to be confirmed. It is reassuring that no studies reported serious adverse events such as death.
The complexity of pulmonary hypertension and its management, and the potential for harm to result from exercise training, means that researchers and clinicians wishing to replicate published pulmonary hypertension rehabilitation programmes require a detailed description of every aspect of intervention delivery. In the translation of robust research findings to clinical practice, practitioners and healthcare commissioners need assurance that comprehensive replication of trial protocols is possible. For this to happen, there is a need for standardised and detailed reporting of exercise intervention components. Currently, throughout the clinical exercise literature, inadequate reporting is the norm.
All studies adequately described the intended protocol for frequency, intensity, time, type, progression, individualisation and starting level. This is a surprising finding given the results of other reviews. A quality assessment of exercise training principles in breast cancer survivors, while not using CERT, identified that only 29% of studies appropriately applied and explained exercise progression, 67% starting values and 38% physiological overload.34 Likewise, an appraisal of exercise intervention quality in subacute and chronic stroke survivors identified only 1 of 37 RCTs which adequately described all principles of physical exercise training.35 Both reviews concluded that incomplete and inconsistent reporting of exercise prescription components would prevent the utility and reproducibility of exercise interventions in these populations. The conflicting finding of adequate exercise intervention description in pulmonary hypertension studies may well reflect the explicit need for highly individualised prescription and clinical safety in pulmonary hypertension patients with a potentially high risk of exercise-induced complications.
While exercise prescription reporting was relatively well defined in the included studies, other components, also considered important, were not. For example, psychological and motivational strategies were poorly described in all but 1 of 19 studies. Most studies provided a brief overview of patient educational programmes covering disease-specific pathophysiology and management by way of generalised group information sessions. Good compliance and adherence to exercise is primarily achieved through effective behavioural change interventions. Regular goal setting combined with motivational interviewing, patient activation, exercise diaries, positive feedback and reinforcement, ‘patient contracts’ and theoretical models are known to enhance short-term and long-term exercise adherence.36–38 These strategies are perhaps most important in clinical populations in which disease-specific symptoms and psychological burden commonly prevent participation in physical activity.
In people living with pulmonary hypertension, exercise can be a very uncomfortable experience, which reinforces negative perceptions and fear of harm. Breathlessness on exertion naturally leads to short-term and longer-term anxiety and depression, resulting in exercise avoidance and an inability to undertake even the simplest of physical tasks. Most of the reviewed studies incorporated management of breathlessness, but there was no detail as to how this would form part of a motivational, behavioural change strategy to enhance compliance and adherence. Clear and detailed reporting of this aspect of exercise programming is essential and is a major weakness of the identified literature.
The methodology for recording and reporting adherence was identified as inadequate in this review. In approximately two-thirds of studies, it was not possible to determine the strategy for measuring adherence and/or the actual level of adherence achieved. As such, a sufficient understanding of the volume or minimum dose of exercise which may lead to benefit in pulmonary hypertension was not attainable. This is a critical flaw in these studies. Equally as important as the demonstration of physiological and psychosocial efficacy is the ability to determine the appropriate dose of exercise required to facilitate meaningful change. This is essential knowledge for practitioners wishing to assess the feasibility of exercise training for people with pulmonary hypertension in clinical practice. Adherence, which has numerous confounding factors including patient motivation, can be recorded accurately as absolute or relative attendance, frequency, intensity and duration. It is unclear why this would not be well defined, as it is simple to monitor, particularly in supervised programme. To ensure adequate information in this area, transparency of reporting should become the norm, regardless of the methodological shortcomings it may expose.
Only one study reported any fidelity strategies. Twelve (63%) reported how accurately and successfully interventions were delivered in line with their protocols. The strategies employed to ensure that practitioners deliver interventions as per the protocol, and the level of precision with which they were delivered, are both critical factors to confirm adequate training stimulus and individualisation. Fidelity is an important component of protocol development and implementation, and should be considered a reporting priority in future studies.
Seventeen studies (90%) were concise and accurate in reporting the rule(s) for determining exercise progression. Methods for monitoring the intensity of exercise, and participant response, were presented in considerable detail, in addition to providing an understanding of how these responses would translate to the progression of exercise prescription. However, implementation of intervention progression in practice was incompletely defined in a third of studies, consistent with the literature in other clinical conditions.34 39 40 This practice may relate to poor recording, reluctance to report inefficiencies or a lack of understanding of the importance of this parameter. Regardless, as with adherence and fidelity, this information supports the successful replication of interventions. Lack of exercise progression can lead to suboptimal exercise prescription and may negatively impact outcomes. Awareness of participant tolerance, and the best strategies by which exercise can be progressed, is vital for safe and effective delivery.
As a general observation, even those parameters deemed to be adequately reported as per CERT may benefit from additional detail. While qualifications/expertise, and supervision were adequately described in 79% and 94% of studies respectively, reporting in both categories could be strengthened. Specific reference to qualifications, expertise and experience, rather than simply detailing staff specialty (with implied knowledge and competence) would be advantageous. Likewise, more thorough explanation of the nature and level of supervision would be beneficial, particularly in cases where face-to-face supervision was limited, that is, home programmes. Three areas in which reporting was considered extensive and appropriate were (1) additional exercise components, for example, respiratory muscle training, resistance training and yoga; (2) non-exercise components such as disease-specific education and (3) adverse events.
Future research should prioritise the assessment of pulmonary hypertension exercise training interventions in the context of clinical service models currently known to be physiologically/psychosocially beneficial and cost-effective in other diseases. It may be possible to seamlessly integrate patients with all subgroups of pulmonary hypertension into existing cardiovascular and pulmonary rehabilitation programmes. Trials should ensure provision of additional expert supervision to manage the potential risk of exercise-induced complications in this population.41 42
Strengths and limitations
We conducted a systematic literature search and objectively summarised results using the CERT. Our search strategy was inclusive, incorporating not only RCTs, but also non-randomised controlled studies and prospective observational studies. We believe the findings have relevance to the clinical exercise community, both academics and clinicians. They also advance the knowledge of exercise prescription and intervention reporting. However, some limitations should be acknowledged. While it was possible to assess the quality of intervention reporting and recommend future research priorities, we did not formally assess the efficacy of exercise interventions in pulmonary hypertension, nor the methodological quality of the studies included. Further, our conclusions are primarily based on group 1 pulmonary arterial hypertension, and mostly reflect exercise provision with an inpatient component.
Conclusion
We did not find any studies that adequately reported all aspects of exercise training interventions in pulmonary hypertension. We did, however, identify some areas in which sufficient information was provided. Exercise prescription was often detailed and well reported, as were non-exercise components and adverse events. Conversely, adherence, fidelity and motivational strategies were poorly described. We encourage the detailed reporting of interventions in future studies, with particular attention to these parameters. The adoption of exercise rehabilitation for pulmonary hypertension may be unnecessarily restricted due to poor reporting. To allow fuller descriptions of interventions, we recommend the publication of trial protocols or intervention development papers, and the use of supplementary online material. Much of the current data are based on a 3-week residential programme in relatively fit people with an average baseline 6 min walking distance of over 400 m. Thus, while it appears that exercise training may be beneficial, there are presently insufficient data to allow practitioners to universally replicate effective exercise-based interventions for people living with pulmonary hypertension.
References
Footnotes
Contributors MU and GM were jointly responsible for the concept of the review. All authors jointly developed the protocol. RP and GM conducted the literature search, and screened and assessed the articles. GM and SF undertook intervention reporting assessment using CERT. GM drafted the manuscript. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MU has received multiple research grants as chief investigator or co-investigator from the National Institute of Health Research and Arthritis Research UK. He is a shareholder and director in Clinvivo Ltd. He is co-investigator on an NIHR funded trial in which ORTHOSPACE Ltd is providing training and surgical implants. He is part of an academic partnership involving Serco Ltd. GM is a director of Atrium Health Ltd.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.