Article Text

Abstract
Background Asthma is a frequent diagnosis in competitive sports, and inhaled β2-agonists are commonly used by athletes. Although inhaled β2-agonists do not seem to improve performance in athletes, it has remained uncertain whether they can increase exercise performance in non-athletes.
Objective To investigate the effect of inhaled β2-agonists on exercise performance in healthy non-athlete individuals.
Methods In a double-blinded, placebo-controlled, cross-over trial, healthy, non-asthmatic, non-athlete individuals were randomised to inhalation of either 900 µg of salbutamol or placebo. Cardiopulmonary exercise testing, dynamic spirometry and impulse oscillometry were performed. The primary outcome was the effect from salbutamol on peak oxygen uptake, whereas secondary outcomes were breathing reserve and ventilation efficiency, and workload, heart rate, breath rate and minute ventilation at peak exercise under influence of salbutamol.
Results A total of 36 healthy subjects with a mean age of 26±5 years were included. Salbutamol had no effect on peak oxygen uptake compared with placebo, 46.8±1.3 mL/kg/min versus 46.6±1.2 mL/kg/min, p=0.64. Salbutamol had no effect on workload, p=0.20, heart rate, p=0.23, breath rate, p=0.10, or minute ventilation, p=0.26, at peak exercise compared with placebo. Salbutamol lowered oxygen uptake, p=0.04, and workload, p=0.04, at anaerobic threshold compared with placebo. Forced expiratory volume in 1 s, 116%±13% of predicted, and peak expiratory flow, 122%±16% of predicted, increased after inhalation of salbutamol compared with placebo; 109%±13% and 117%±17%, respectively, p<0.01. Breathing reserve was found to be higher, 22%±2%, after salbutamol inhalation than after placebo, 16%±2%, p<0.01.
Conclusion Inhaled salbutamol did not improve peak oxygen uptake in healthy, non-asthmatic, non-athlete individuals compared with placebo.
Trial registration number NCT02914652.
- performance
- randomised controlled trial
- Sports & exercise medicine
- doping
- endurance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
Salbutamol inhalations do not increase peak exercise performance in non-asthmatic, non-athlete individuals.
Ventilation during exercise is unaffected by salbutamol inhalations despite improved dynamic spirometry, impulse oscillometry and breathing reserve capacity.
Our data emphasise that inhaled salbutamol is not ergogenic, thus strengthening current WADA guidelines regarding its use in competitive sports.
Introduction
The prevalence of asthma in competitive athletes is higher than in the background population,1 and the use of β2-agonists among competitive athletes has gradually increased since the Olympic Games in 1984.2–4 It could be questioned whether this increase in inhaled β2-agonists is related to an increase in prevalence of exercise-induced bronchoconstriction. Based on the assumption that systemic β2-agonists might increase exercise performance, all systemic β2-agonists are prohibited in and out of competition.5 However, inhaled formoterol, salbutamol and salmeterol are permitted if the prescribed maximal dosage is obeyed. The ergogenic potential of these drugs has been subject to intense debate in recent decades. Although the available literature does not point towards an ergogenic effect of inhaled β2-agonists,6 7 systemically administered β2-agonists have been found to improve endurance time,8–10 peak power11–14 and muscle strength.10 15 One may speculate on whether β2-agonists could affect individuals differently depending on their baseline physical performance level. van Baak et al 16 demonstrated an ergogenic effect on endurance time after inhalation of salbutamol, where the largest improvements were seen in the subjects with poorest baseline performances, suggesting that the ergogenic effect may depend on baseline physical performance level. In the literature, studies have almost exclusively been conducted on highly trained athletes in relatively small sample sizes and do not show any ergogenic effect.17–25 Whether inhaled β2-agonists increase exercise performance in non-asthmatic, non-athlete individuals needs to be elucidated in order to entirely cover β2-agonists’ possible ergogenic potential. Therefore, the aim of this study was to investigate the effect of an inhaled β2-agonist on exercise performance in non-athlete, non-asthmatic, healthy individuals.
Methods
Study design
In a double-blinded, placebo-controlled, cross-over trial, participants were randomised to inhalation of either 900 µg of salbutamol (Ventoline) or placebo (Evohaler). Investigations were performed on two separate occasions with 2–14 days of interval at Aarhus University Hospital, Denmark. A block randomisation sequence with six participants in each block was made by the Hospital Pharmacy of Region Midtjylland. Each participant received an identification number, which was linked to the participant’s intervention containers. Allocation information was concealed for all involved personnel until completion of the data analyses. The participants were requested not to perform exhausting exercise within 24 hours prior to each visit and they were asked to abstain from large meals, coffee and tobacco smoking for at least 2 hours before the visit. The International Physical Activity Questionnaire was handed out and bioelectrical impedance measurements were performed using the ImpediMed Model SFB7 (ImpediMed, Brisbane, Queensland, Australia) prior to interventions at first visit. Each participant performed pulmonary reversibility tests and a cardiopulmonary exercise test at both visits.
Study population
Participants were healthy, non-athlete individuals aged 18–40 years, approached through flyers and announcements on official web pages. Exclusion criteria were cardiac abnormalities, pulmonary disease, syndromes (eg, Down’s), pregnancy or current breast feeding, and metabolic disorders (eg, hyperthyroidism).
Interventional protocol
A metered dose inhaler containing either salbutamol or placebo was used for administration of intervention. To ensure correct and systematic administration, an official, governmental instruction video was shown at both visits. Approximately 10–15 min prior to the pulmonary reversibility test, eight doses of either 100 µg Ventoline or Placebo Evohaler were administered. An additional dose of 100 µg Ventoline or Placebo Evohaler was given approximately 60 min before the cardiopulmonary exercise test to ensure maximal effect during the test. Hence, the cumulative dose of salbutamol was 900 µg.
Pulmonary function tests
Dynamic spirometry
For dynamic spirometry measurements an IntraMedic Jaeger MasterScreen PFT pro Diffusion System and a BodyBox from CareFusion (IntraMedic, Gentofte, Denmark) were used. Tests were performed in accordance with established guidelines.26
Impulse oscillometry
A CareFusion Vyntus Impulse Oscillometry using SentrySuite Software and a Vyntus Spirometer (IntraMedic) using Lab Manager V.4.67.0.1 (CareFusion Germany, Hoechberg, Germany) were used and measurements were performed per current guidelines.27
Cardiopulmonary exercise testing
Cardiopulmonary exercise testing was performed on an upright ViaSprint 150P ergometer cycle (Ergoline, Bitz, Germany) by trained experienced personnel following current international guidelines.28 All participants were instructed to hold a pedalling speed between 60 and 70 rounds/min throughout the test without standing, talking or releasing the handlebars. Investigators chose an individual workload protocol for each participant based on the participant’s body mass, gender and habitual activity level. Each protocol had an initial rest period of 2 min followed by a start workload of 25 or 100 W, increasing with 10, 15 or 25 W/min. Participants were encouraged to pedal until complete exhaustion, defined as inability to maintain the instructed pace.
Gas exchange was measured breath by breath using a Jaegers MasterScreen CPX system (IntraMedic) from onset of the test until 1 min after exhaustion. Heart rate, 12-lead ECG and arterial oxygenation were continuously monitored, while arterial blood pressure was measured at rest and every second minute during active pedalling. A test was considered valid if the respiratory exchange ratio reached a value of 1.1 or above. Anaerobic threshold was calculated using the V-slope method.29 Maximal voluntary ventilation was estimated using the forced expiratory volume in 1 s (FEV1) multiplied by 40, from which the breathing reserve index at maximum exercise was calculated as 100 × (maximal voluntary ventilation − maximum ventilation at peak exercise)/maximal voluntary.30 VE/VCO2 slope was calculated as the slope from onset of exercise until exhaustion.
Outcomes
The primary outcome was the effect of salbutamol on peak oxygen uptake. Secondary outcomes were the effects from salbutamol on workload, heart rate, breath rate, minute ventilation, breathing reserve and ventilation efficiency, defined as VE/VCO2.
Statistical analyses
Continuous data are reported as mean with SD or median with total range and, if appropriate, binary data are presented as absolute numbers and percentage of participants. For continuous data, differences between interventions are analysed using paired Student’s t-tests or two-way analyses of variance. Χ2 tests are used for binary data. Level of significance was set to p values <0.05 for the primary outcome and p values <0.01 for secondary outcomes. Descriptive data were stored in Microsoft Excel 2016 (Microsoft, CA, USA) and data analysis was performed using STATA/IC V.12.1 for Mac (StataCorp, Texas, USA). Graphical illustration was made with GraphPad Prism V.6 (GraphPad Software, La Jolla, CA, USA).
Results
Participant characteristics
Between October 2016 and June 2017, a total of 36 non-asthmatic, healthy individuals were included at Aarhus University Hospital, Denmark (figure 1). All enrolled participants completed both study visits and no serious adverse events were observed. Demographics and clinical characteristics, including the International Physical Activity Questionnaire, are displayed in table 1. None of the included participants were competitive endurance athletes. One participant performed more than 2 hours of high-intensity exercise per day, three participants performed more than 1 hour/day whereas the rest performed less than 1 hour/day. None of our participants performed competitive high-intensity sports (eg, cycling, long-distance running or swimming). Four participants were smokers, of which three smoked less than 20 cigarettes per week, and one smoked more than 20 cigarettes per week. Twelve participants received prescribed drugs: attention deficit hyperactivity disorder medication (n=1), psoriasis medication (n=1), antidepressants (n=1), migraine medication (n=1), contraceptives (n=6) and acne medication (n=2).

Flow chart of investigations performed at first and second visits. The red and blue lines represent the randomisation order.
Demographics and clinical characteristics of non-asthmatic, healthy individuals
The effect of salbutamol on physical performance
All tests were considered valid according to above-mentioned criteria with no premature test terminations. Exercise outcomes are shown in table 2. Oxygen uptake at peak exercise after salbutamol inhalation did not differ from the peak oxygen uptake after inhalation of placebo, 46.8±1.3 mL/kg/min versus 46.6±1.2 mL/kg/min, p=0.64. Salbutamol did not affect workload, p=0.20, heart rate, p=0.23, breath rate, p=0.10, or minute ventilation, p=0.26, at peak exercise differently compared with placebo. Breathing reserve was found to be higher, 22%±2%, after salbutamol inhalation than after placebo, 16%±2%, p<0.01, while ventilatory efficiency was comparable between interventions, p=0.74.
Exercise outcomes during intervention with salbutamol and placebo in non-asthmatic, healthy individuals
Salbutamol had a significant impact on anaerobic threshold parameters, resulting in lower oxygen uptake, 31.9±1.6 mL/kg/min, p=0.04, and lower workload, 2.62±0.17 W/kg, p=0.04, after salbutamol inhalation compared with placebo; 34.6±1.2 mL/kg/min and 2.91±0.11 W/kg, respectively. A tendency towards lower heart rate, 153±4 beats/min, p=0.05, was observed with salbutamol intervention compared with placebo, 161±2 beats/min.
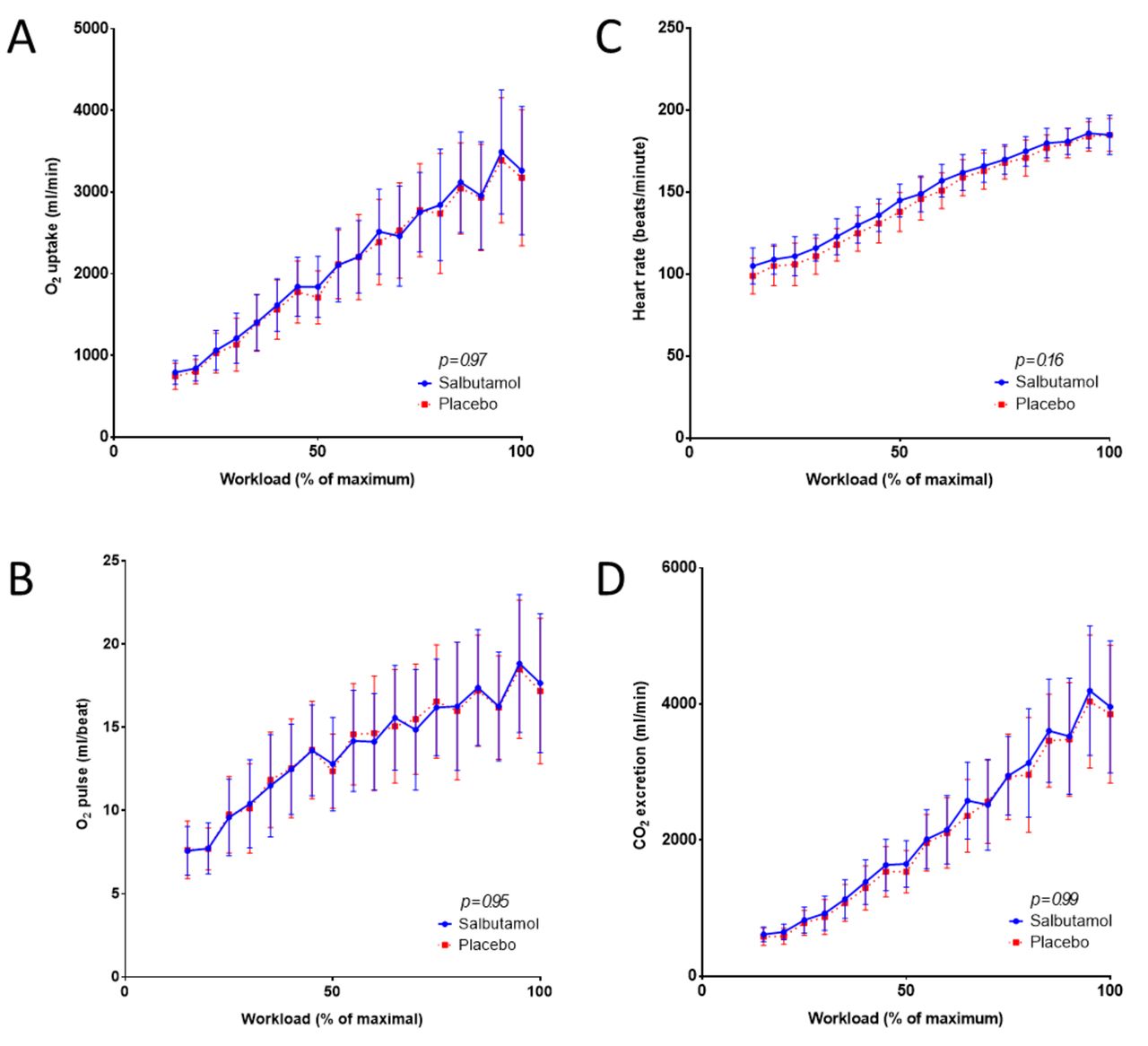
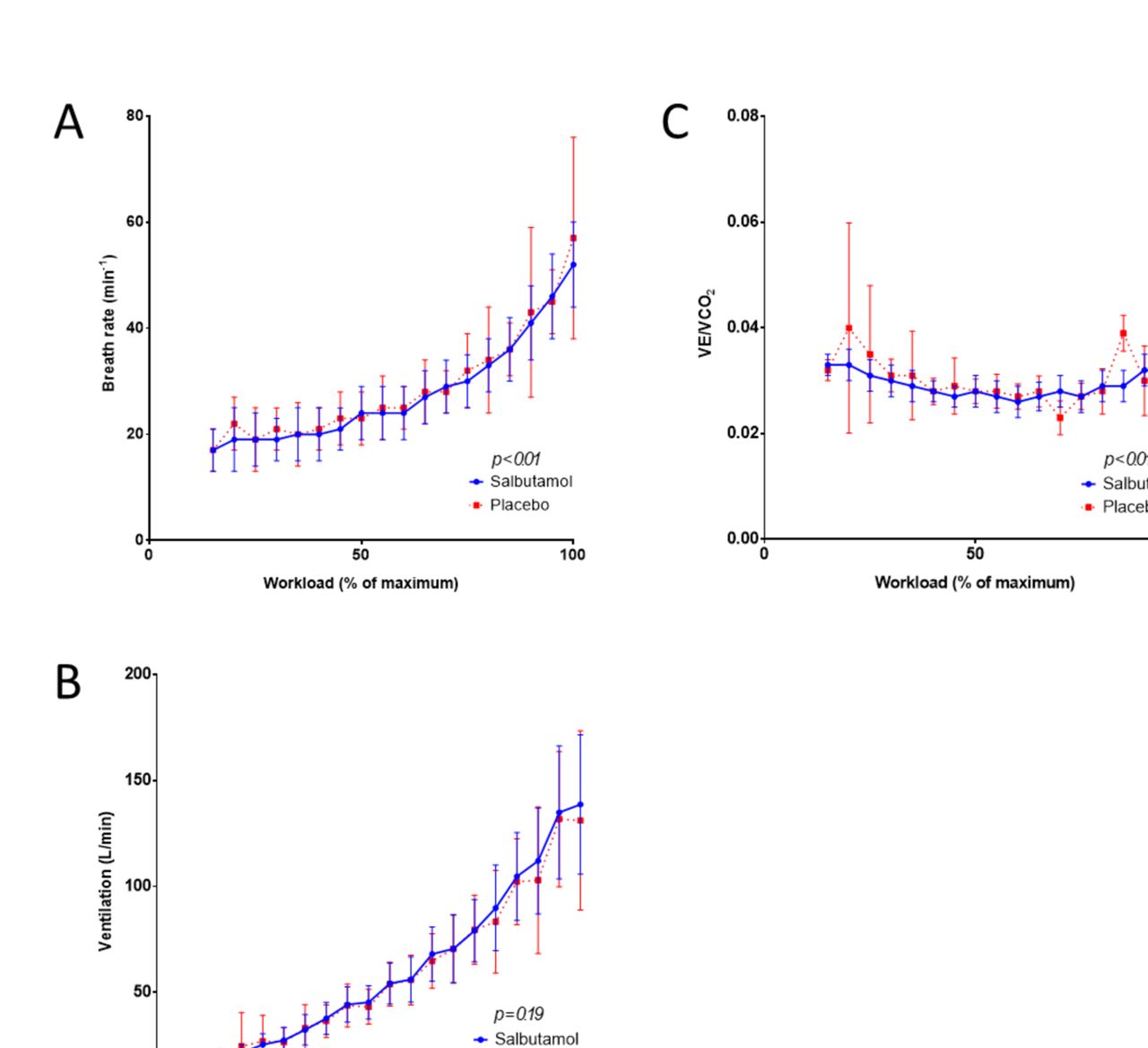
Exercise parameters related to workload after salbutamol and after placebo intervention are illustrated in figures 2 and 3. Breath rate decreased with salbutamol compared with placebo, but minute ventilation was comparable between treatments. Ventilatory efficiency decreased after salbutamol intervention compared with placebo.

Exercise parameters related to workload during bicycle ergometry after salbutamol and placebo intervention in healthy, non-asthmatic individuals. (A) Oxygen uptake. (B) Oxygen pulse. (C) Heart rate. (D) Carbon dioxide excretion.

{kind=link}
{kind=link}
{kind=link}
Exercise parameters related to workload during bicycle ergometry after salbutamol and placebo intervention in healthy, non-asthmatic individuals. (A) Breath rate. (B) Ventilation. (C) Ventilatory efficiency.
The effect of salbutamol on pulmonary function
Pulmonary function after salbutamol and placebo intervention is outlined in table 3. None of the participants had clinical undiagnosed asthma. FEV1, 116%±13% of predicted, and peak expiratory flow, 122%±16%, increased after inhalation of salbutamol compared with placebo, 109%±13% and 117%±17%, respectively, p<0.01. We did not observe an effect from salbutamol on forced vital capacity. Salbutamol lowered the resistance in the conducting airways, 89%±26% of predicted compared with placebo, 102%±28%, p<0.01, where the bronchodilation could be localised to the large conducting airways, 96%±24% versus 112%±27%, p<0.01.
Pulmonary function during placebo and salbutamol intervention in non-asthmatic, healthy individuals
Discussion
Our main finding in this double-blinded, randomised, cross-over study on non-asthmatic, untrained, healthy individuals was that inhaled salbutamol did not increase peak oxygen uptake compared with placebo. Furthermore, inhaled salbutamol and placebo administration were comparable in terms of workload, heart rate and breath rate at peak exercise. We did not observe any difference between treatments on minute ventilation or ventilation efficiency. Lastly, inhalation of salbutamol had a divergent effect on anaerobic threshold parameters, where we observed a decreased workload, oxygen uptake and heart rate during salbutamol condition compared with placebo.
This is the first study investigating the effect of supratherapeutic doses of inhaled salbutamol on exercise performance and pulmonary function in healthy non-athletes. Our findings are in line with those which have previously been reported in highly trained athletes.17–25 During exercise, salbutamol increases plasma lactate due to a β2-stimulated shift in glucose metabolism, from aerobic to anaerobic metabolic pathways, and a following accentuation of lactic acid production.11 31–33 Our study population responded, as described in literature, when administered salbutamol with increased carbon dioxide excretion as a measure of increased lactic acid production, significantly shifting the ventilatory anaerobic threshold downwards, for example, reaching the threshold earlier during the exercise test compared with placebo. The VE/VCO2 curve as a function of workload further elucidates this physiological mechanism, as the curve is shifted downwards during salbutamol intervention compared with placebo. This implies that inhalations with salbutamol decrease the amount of aerobic work performed and increase the amount of anaerobic work, without increasing maximal performance. In competitive endurance sports requiring a high anaerobic threshold this would be detrimental. Our observations contradict the findings of Carlsen et al 17 who found unaffected anaerobic threshold in highly trained athletes after inhalation with 800 µg salbutamol or 50 µg salmeterol compared with placebo. Hence, either athletes are not as affected by the β2-stimulated increase in glucose metabolism as untrained individuals, or our sample size was not large enough to detect a significant difference.
Inhalation of salbutamol increased dynamic pulmonary function and lowered the resistance of the conducting airways, however, without an analogous increase in exercise ventilation. However, our cohort of non-athletes had a breathing reserve capacity of 15% after placebo inhalation, and a breathing reserve capacity below 20% may indicate that the pulmonary function is the limiting factor at peak performance.30 Salbutamol inhalations in supratherapeutic doses lowered the resistance of the conducting airways, increased dynamic pulmonary function and increased the breathing reserve capacity to 22%. Despite these improvements, inhalation of salbutamol does not seem to improve exercise ventilation in healthy individuals, thus suggesting that the potential ergogenic effect must lie within another possible physiological mechanism, beyond the respiratory system. These observations mimic the results previously found in highly trained athletes,17–21 34 where maximal performance was unaffected after salbutamol inhalations despite increased resting pulmonary function. Altogether, our data support the consensus that pulmonary function is not a limiting factor for exercise performance in healthy individuals. Improved lung function at rest cannot be interpreted as ergogenic in an exercising setting.
In the literature, only two studies have demonstrated an ergogenic effect after inhalation of β2-agonists. Signorile and colleagues35 performed a 15 s Wingate test on healthy men and women, and observed a gain in sprint capacity after inhalations with 180 µg albuterol compared with placebo. van Baak et al 10 demonstrated a 2% increase in performance during an ergometer time trial in 16 non-asthmatic male athletes after 800 µg salbutamol inhalations. The most significant improvement was seen in subjects with poorest test times, raising the question whether the potential ergogenic effect from inhaled salbutamol could depend on baseline physical performance level. However, our data showed that there is no ergogenic effect of salbutamol inhalations in non-athletes either. On the other hand, the ergogenic effect after systemic administration seems to be explained by delivery route and subsequently plasma concentration.8–15 36 It seems conceivable to assume that the explanation for the potential ergogenic effect of salbutamol lies within the pharmacokinetics and, subsequently, the pharmacodynamics as systemic administration of β2-agonists is known to mediate, directly and indirectly, increase plasma glucose,37 38 increase availability of free fatty acids8 37 39 40 and stimulate insulin secretion and glycolysis,9 37 with increased lactate and pyruvate release from muscle.
Plasma concentrations are significantly lower after inhalation than after oral administration. Nevertheless, studies have demonstrated changes in free fatty acids, glycerol, lactate and potassium after salbutamol inhalations,16 41 42 suggesting its capability to reach peripheral organs and affect its metabolism, but this effect might be of poor clinical relevance in the light of the negligible effects on exercise performance.7
A potential way to reach higher plasma concentration through inhalations is chronic administration. In a placebo-controlled trial, Dickinson et al 43 investigated whether 1600 µg of inhaled salbutamol for 6 weeks improved endurance, strength and power performance in a group of healthy athletes of mixed sports. They found no significant increase in performance outcomes, further supporting the statement that inhaled salbutamol does not possess an ergogenic potential.
Given the nature of the drug, and what have been reported in literature on no improvement in exercise performance after inhalation with a β2-agonist, one might assume that athletes with exercise-induced bronchoconstriction would derive no ergogenic benefit in terms of maximal performance. Therefore, the debate regarding inhaled β2-agonist as a possible ergogenic agent seems to be inappropriate. Consequently, these drugs should be allowed as treatment for exercise-induced bronchoconstriction in athletes according to same guidelines as in non-athletes and patients with asthma as long as the WADA guidelines5 are obeyed.
A possible limitation to our study worth mentioning is the fact that we performed the exercise performance measurements on an ergometer bicycle without giving our participants the opportunity to try the bicycle and the protocol prior to the test. Since the participants were non-athletes, one can claim that unfamiliarity with using an ergometer bike could have affected the outcome. However, with the cross-over design this possible source of error can be ruled out. Another limitation is that we did not perform a bronchodilation test prior to inclusion; however, none of the participants had any asthmatic symptoms, neither at rest nor in relation to exercise.
In conclusion, acute supratherapeutic inhalation of salbutamol does not have an ergogenic effect on exercise performance compared with placebo in healthy, non-athlete individuals. Improved lung function at rest cannot be interpreted as ergogenic in an exercising setting since neither minute ventilation nor peak oxygen uptake was increased. Our data support the consensus that pulmonary function is not a limiting factor for exercise performance in healthy adults. Furthermore, this study encourages that inhaled β2-agonists can be used as an acceptable treatment option for exercise-induced bronchoconstriction in athletes.
Acknowledgments
The nurses from the Department of Paediatrics are warmly acknowledged for their contribution to data collection.
References
Footnotes
FE and CER are joint first authors.
Contributor All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content. All authors have made substantial contribution to the work in the manuscript including participation in the concept, design, analysis, writing, or revision of the manuscript.
Funding The project was supported with aid from the following funds: Aarhus University, Aase and Ejnar Danielsen’s Fund, Children’s Heart Foundation and Dagmar Marshall’s Fund.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by the Danish (chart: 2016061269) and the European (EudraCT No 2015-005507-89) Medicines Agency, and the Committee on Biomedical Research Ethics of the Central Denmark Region (chart: 1-10-72-153-16). Further, approval was obtained from the Danish Data Protection Agency (chart: 1-16-02-315-16). The trial was conducted in accordance with Danish law and the Helsinki Declaration of 1975, revised in 2008, for research involving human subjects, and is listed on ClinicalTrials.gov (identifier: NCT02914652). The Good Clinical Practice (GCP) Unit at Aalborg and Aarhus University continuously monitored the trial.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.