Article Text

Abstract
Objective Health clubs (HC) and personal trainers (PT) are traditional outlets for the promotion of physical activity (PA) and exercise programming. As physicians are increasingly being called on to write exercise prescriptions for their patients, this study sought to investigate the level of integration between the healthcare and fitness systems.
Design An internet study was designed with five domains to understand physicians’: (1) overall perception of HC, (2) appropriateness and recommendation of HC and PT to their patients, (3) attitude regarding specific aspects of HC, (4) support of patient participation in HC sponsored exercise and (5) elements of HC that physicians would like to know for referral.
Methods An electronic survey was sent to members of two mailing lists of primary care and sports medicine specialty physicians during 2011–2012.
Results On a Likert scale of 1–10 412 physicians reported being familiar with HC (8.9±2.1), indicated a favourable view of HC (7.9±2.2), and believe HC to be an appropriate venue for their patients (7.5±2.3). However, physicians only recommend HC to 41%±28% of their patients and PT for only 21%±21.6% of patients. Physicians ranked expense and convenience as the most problematic elements of HC (8.1±2.1 and 6.3±2.5, respectively). 72% of physicians indicated cost as most concerning when recommending a specific HC.
Conclusion HC and PT are a significant implementation system for the promotion of physical activity, yet physicians are concerned with several elements of HC and are not adequately relying on this partnership to promote physical activity to their patients.
- physical activity
- exercise
- physicians
- prescription
- health club
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
Health clubs (HC) and personal trainers (PT) are traditional outlets for the promotion of physical activity and exercise regimens, and physicians are not adequately relying on these partnerships to promote physical activity to their patients.
There has been an increase of patients receiving advice to exercise by physicians; however, results from this study indicate that less than half of physicians familiar with HC would refer their patient to one, and only one-fifth would refer to a PT.
There is a meaningful trust gap between physicians and fitness professionals who may be a partner able to implement exercise and physical activity prescriptions.
Impact on clinical practice
Initiatives and partnerships should be cultivated to bridge the gap between physicians and fitness professionals and, more critically, build trust between the medical institutions prescribing exercise as medicine and the practitioners ‘filling’ these prescriptions in HC and the community at large.
Introduction
Physical activity is an essential component to health and is considered a primary prevention strategy for most non-communicable disease.1 Physicians are often called on to recommend or prescribe exercise to their patients and are an important element in the environmental landscape to encourage increased levels of physical activity in the general population. However, only 30% of patients report receiving this advice from their doctors2 and physicians themselves often cite individual, environmental, policy and organisational barriers to discussing physical activity and exercise with their patients.3–5 Calls have been made for physicians to ‘outsource’ or ‘refer’ their patients to health and fitness professionals that have dedicated time to promote physical activity,6 yet there has been little investigation into the attitude or knowledge of physicians regarding this type of referral process.
Health clubs (HC) and personal trainers (PT) are traditional outlets for the promotion of physical activity and exercise regimens. Globally, the HC industry has approximately 201 000 HC with 162.1 million members.7 Specifically in the USA, there are greater than 36 000 HC with 57.3 million members.7 With regard to healthcare, use of a HC has been shown to benefit health-related outcomes,8 slows the growth of healthcare costs as a population ages9 and may reduce overall healthcare costs long term.10 In addition, individuals who exercise with certified health and exercise professionals tend to see greater levels of physical activity overall as well as increased weight loss and strength and aerobic capacity compared with individuals who are not trained by a fitness professional.11–13 Yet, while several studies have examined the positive impact of participation in HC programming on patient outcomes, no study has yet reported the attitude of physicians regarding referral to such facilities, despite an increasing call to prescribe exercise to their patients.6 14
There are limited reports investigating physician attitudes regarding implementation of physical activity prescriptions with a specific focus on referral. One recent longitudinal qualitative study examined family physicians’ experiences of trying to implement written PA prescriptions into their practice and found that the rate of implementation was lower than anticipated by physician participants with a primary concern being uncertainty of the effectiveness of written exercise prescriptions.15 Another study found that physicians indicated a strong ability to refer patients to affiliated medical fitness centre facilities, but needed education about referral programmes available as well as standard clinical guidelines and protocol for delivery.3
The current study used a global survey of primary care and specialty sports medicine physicians to understand their overall perception of HC, attitude regarding specific aspects of HC and appropriateness and subsequent recommendation of HC and PT to their patients. This study is the first of its kind to attempt to understand the necessary relationship between medical professionals and the rapidly expanding fitness industry.
Methods
To establish an understanding for physician overall perception of HC, attitude regarding specific aspects of HC and appropriateness and subsequent recommendation of HC and PT to their patients, the authors developed an internet-based survey targeted to these domains. The details of the survey have been reported previously.4
The study was stratified into five domains. The first three domains addressed physician opinions about HC in general. In the first domain, physicians were asked on a 1 to 10 scale (1=definitely no; 10=definitely yes) if: (1) HC are an appropriate exercise venue for their patients, (2) from personal experience, if they were familiar with HC, (3) if they had a positive view of HC. The second domain of the survey asked physicians to estimate what percentage of their patients they (1) recommend going to a HC and (2) recommend using a PT (whether in or out of a club). The third domain asked physicians to judge on a 1 to 10 scale (1=no problem; 10=major problem) several aspects of HC including: expense to patients, convenience for patients, safety for patients, effectiveness for patients and liability exposure for self.
In the fourth domain of the study, physicians were asked to comment on how supportive they were of patients participating in a variety of exercise options. Physicians were asked on a 1 to 10 scale (1=Do not Support at All; 10—Support strongly) to rank: strength training (eg, machines, free weights), aerobic oriented (eg, treadmills, aerobic classes, running), PT and group exercise classes (eg, indoor cycling, yoga, pilates).
In the fifth and final domain, physicians were asked what elements of each HC they would be interested in knowing when recommending a specific HC to their patients. Physicians were asked to check all elements that applied and included: certified trainers, wide range of activities, clean and pleasant facility, helpfulness of staff, specific outstanding teachers/trainers, convenience, cost to patient, certified facility, personal experience with the club, reputation and other (fill in the blank). Physicians were then asked to recall and name a specific HC that they thought particularly highly of.
Data that were returned via the online survey was analysed in SPSS V.11.5 (Armonk, New York, USA). Means and SD were calculated for all continuous variables. Descriptive, bivariate t-tests and correlation statistics were computed. P≤0.05 were considered statistically significant.
Results
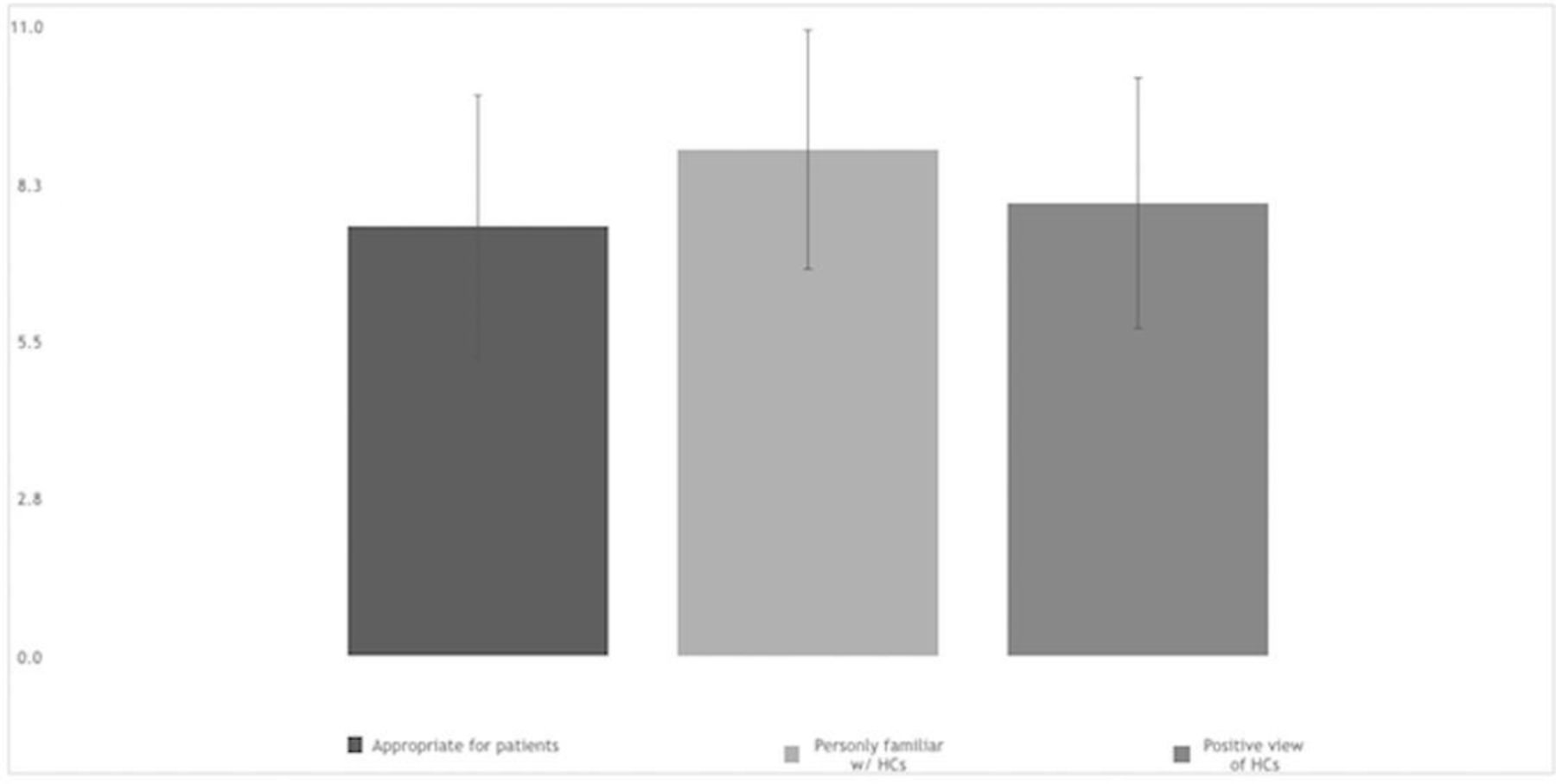
Specific data regarding the sources and response rate of these surveys have been reported elsewhere.4 When asked if physicians were personally familiar with HC, physicians responded overwhelmingly that they were indeed familiar with HC (8.9±2.1). Physicians also indicated that they had a favourable view of HC (7.9±2.2). With regard to whether or not HC were an appropriate venue for their patients, physicians responded a mean of 7.5±2.3 in favour of HC (figure 1). Significant correlations between personal familiarity and a positive view of HC were observed (r=0.4; p<0.05) as well as between a positive view of HC and appropriateness for patients (r=0.6; p<0.05). Physician self-reported minutes of physician activity was also positively correlated with appropriateness of HC for patients (r=0.17, p<0.01), familiarity with HC (r=0.16, p<0.01) and positive view of HC (r=0.24, p<0.01). Physician body mass index (BMI), however, was not associated physician perception of appropriateness of HC for patients (r=−0.03, p=0.63), familiarity with HC (r=−0.02, p=0.755) and positive view of HC (r=−0.03, p=0.60). Physician self-reported minutes of physician activity was negatively correlated with BMI (r=−0.16, p<0.01).
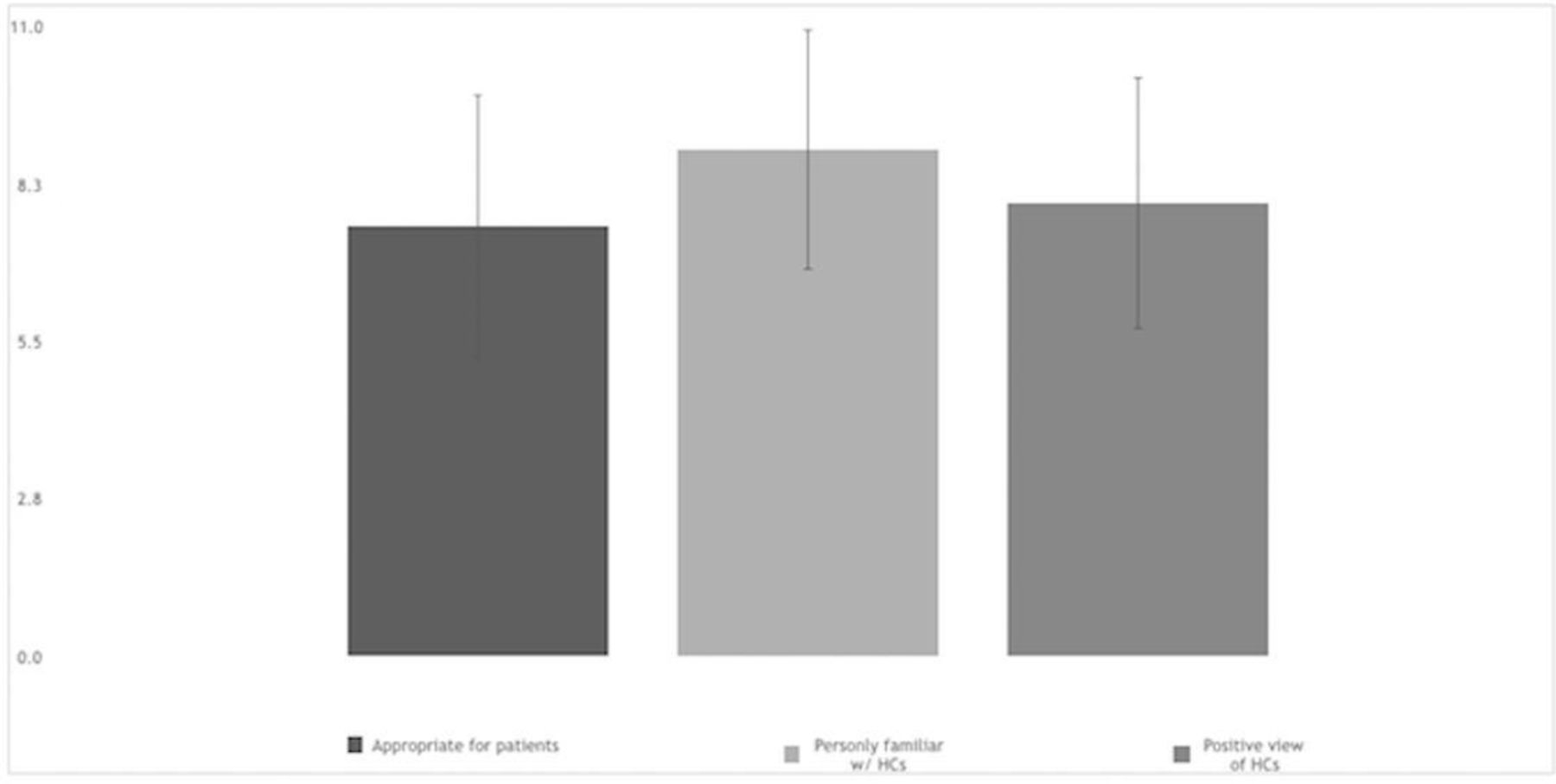
Physicians were asked on a scale of 1–10 (1=Do not Support at All; 10=Support strongly), ‘From personal experience, are you familiar with health clubs (HC)’, ‘Do you have a positive view of health clubs’ and ‘Are health clubs an appropriate exercise venue for your patients’. Overall perception of HC was positive.
When asked to what percentage of their patients physicians were likely to recommend HC, physicians estimated that they recommend HC to 41%±28% of their patients. Yet, physicians recommend PT for only 21%±21.6% of their patients (figure 2). A significant correlation between a positive view of HC and support of PT for their patients (r=0.26, p<0.01) was observed as well as a significant correlation between the belief HC are appropriate for their patients and support of PT for their patients (r=0.17, p<0.01). However, simply being familiar with HC was not associated with support of PT for their patients (r=0.099, p=0.065).
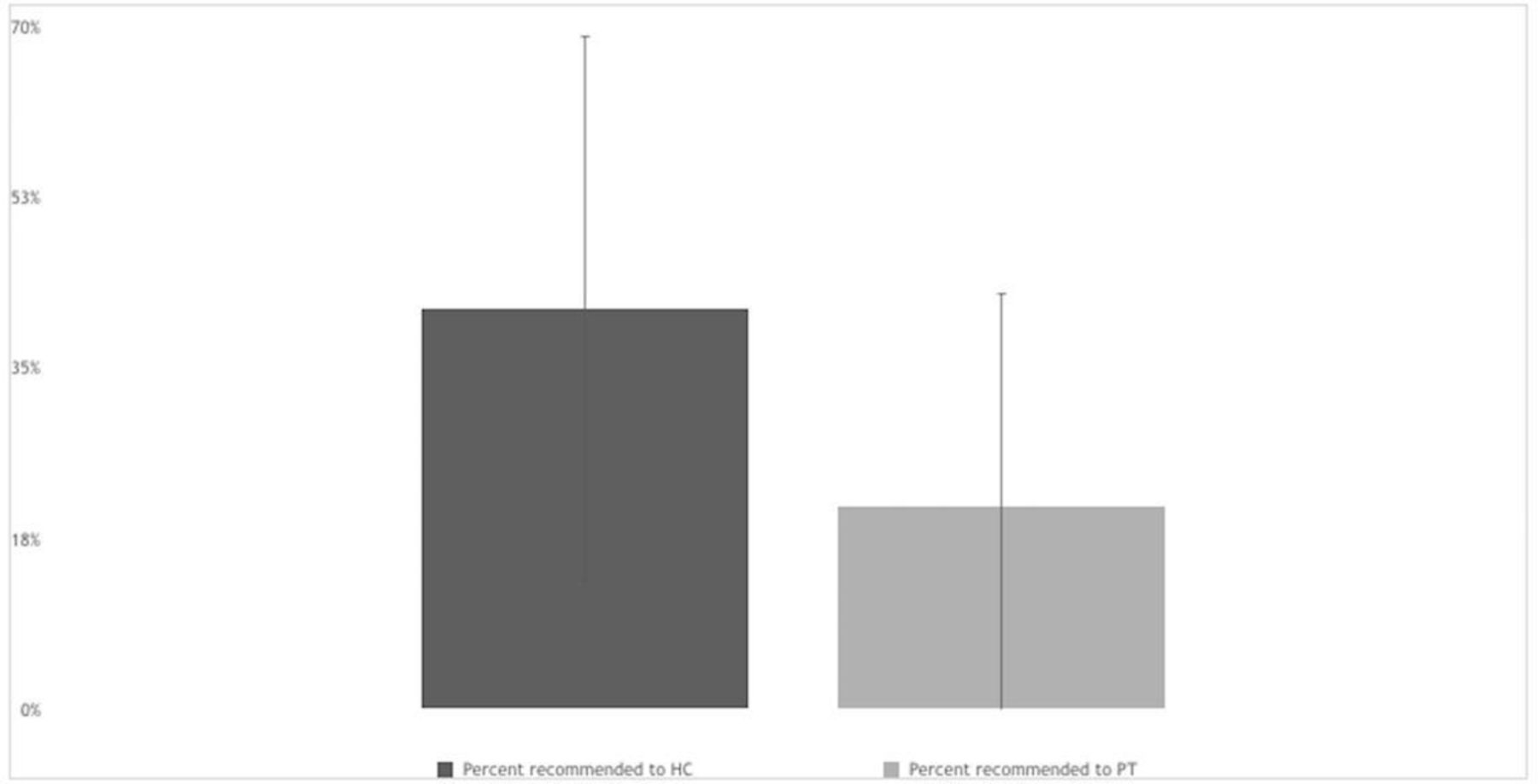
The majority of physicians were not inclined to recommend HC (41%±28%) or PT (21±21.6) to their patients. HC, health clubs; PT, personal trainers.
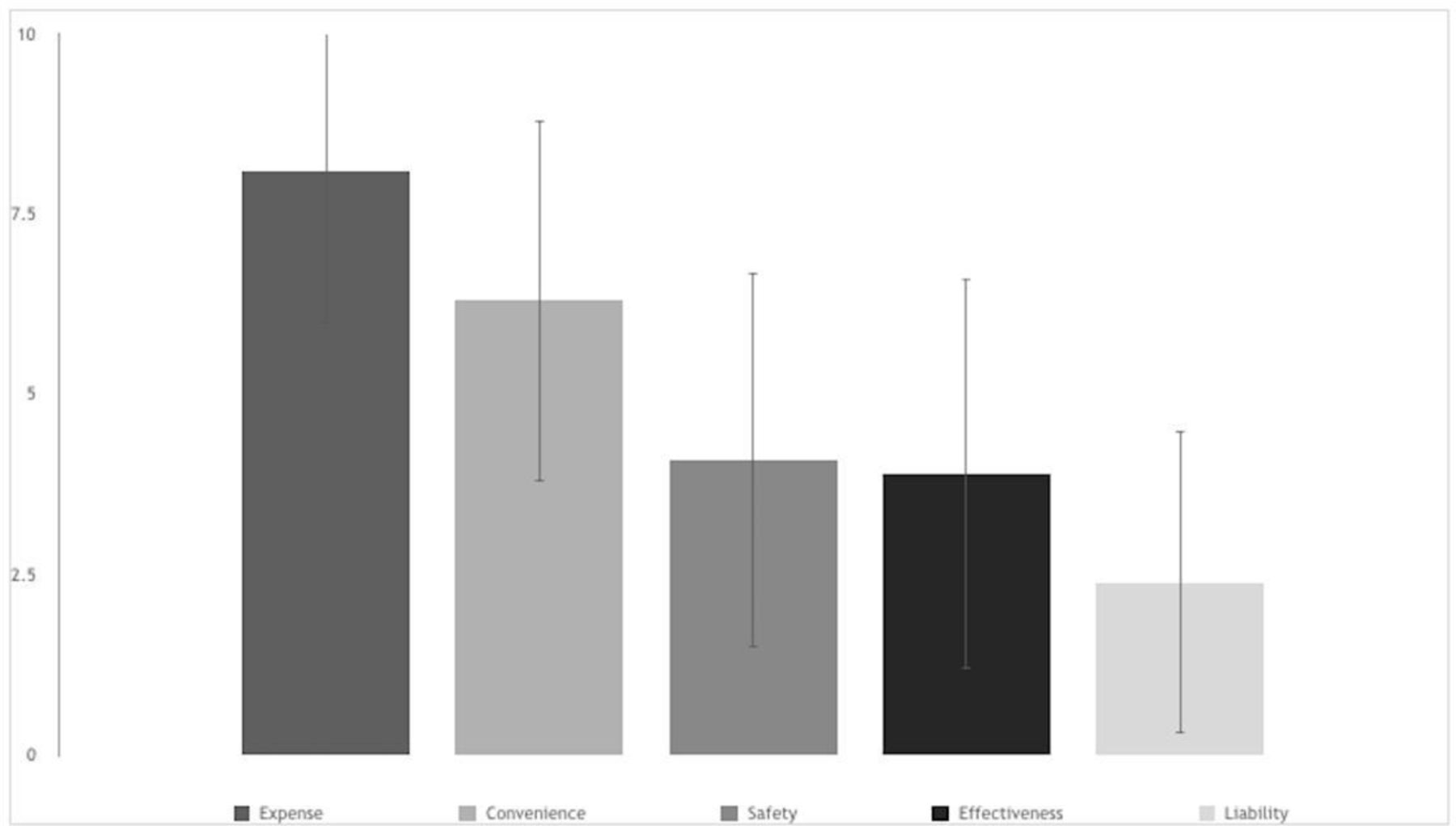
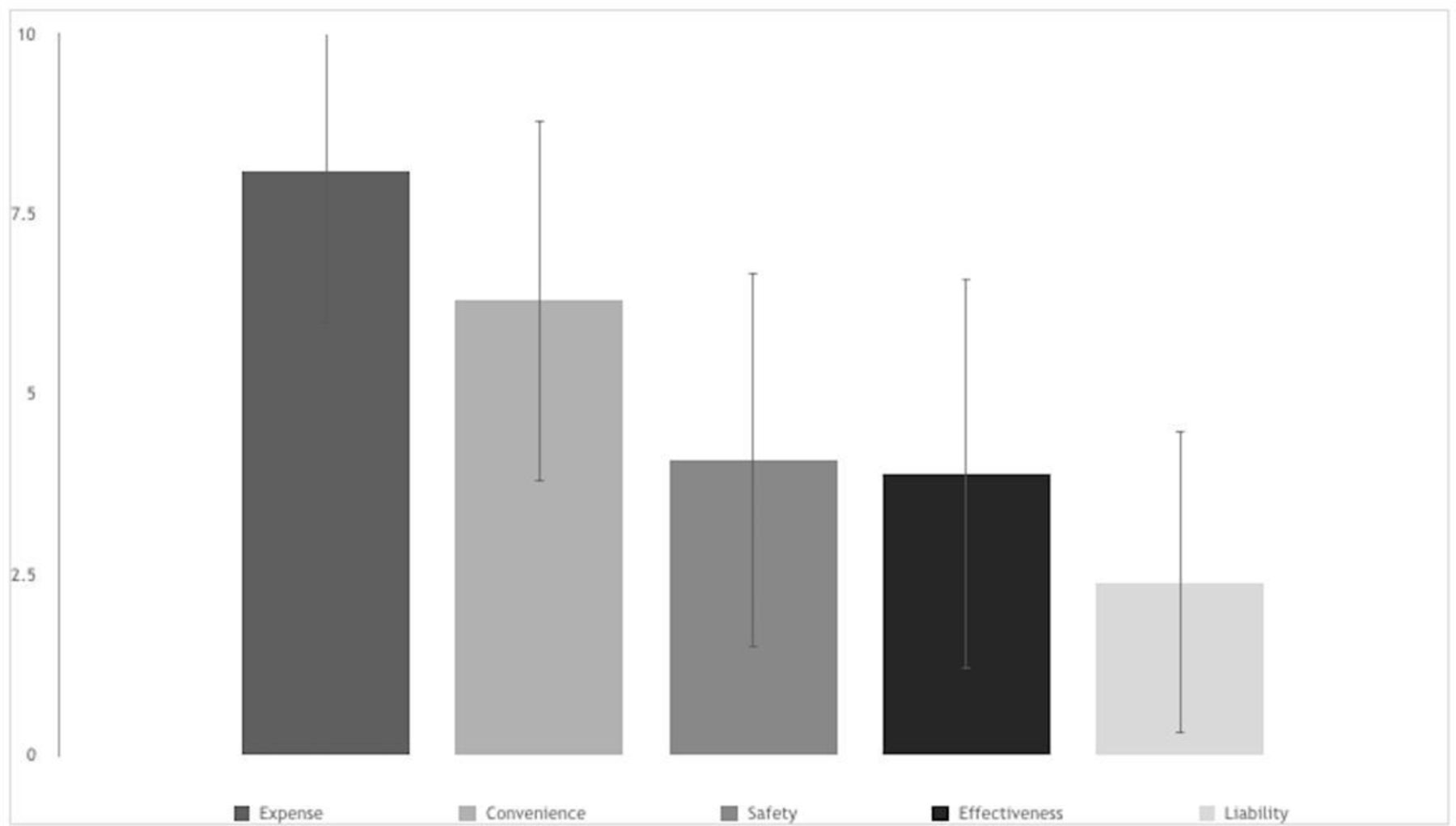
Physicians ranked specific HC attributes (from major problem to no problem) in the order of: expense, convenience, safety, effectiveness and personal liability. Physicians ranked expense as the most problematic of the choices (8.1±2.1) with convenience second (6.3±2.5). Safety (4.1±2.6), effectiveness (3.9±2.7) and personal liability to the physician (2.4±2.1) were seen as much less of a problem than expense and convenience (figure 3).
{kind=link}
{kind=link}
{kind=link}
Physicians were asked ‘How do you judge the following aspects of health clubs in terms of recommending them to your typical patients on a scale of 1–10’ (1=no problem to 10=major problem). Expense and convenience were averaged as the two major problems (8.1±2.1 and 6.3±2.5, respectively) with safety (4.1±2.6), effectiveness (3.9±2.7) and liability (2.4±2.1) as lesser problems.
When asked whether physicians were supportive of a variety of exercise options offered at HC, physicians ranked options (support strongly to do not support at all) as: aerobic activity (8.7±1.8), strength training (8.3±2.1), group exercise (8.2±2.0) and PT (6.5±2.6).
When asked to indicate all elements of what physicians do (or would) look for in recommending a specific HC, 72% of physicians indicated cost to patients was the element that was most concerning. More than half of physicians were concerned about: wide range of activities (66%), convenience (65%), clean and pleasant facility (61%) and helpfulness of staff (52%). Less than half of physicians surveyed indicated that they were concerned with certified trainers (48%), personal experience with the club (32%), specific outstanding teachers/trainers (30%), club reputation (30%) and a facility that was certified (26%).
When asked if there was a specific HC that physicians think highly of, 33% of physicians named a facility that was not a YMCA (”The Y”), 20% of physicians named YMCA specifically, 29% named a facility that was not specified and 20% indicated that there was no HC they thought highly of.
Discussion
This survey sought to investigate the attitude and knowledge of physicians regarding the range and opportunity for a referral process to facilities and trained professionals within the HC and fitness arena. Our results demonstrate that while physicians tend to have a generally positive view of HC, less than 50% refer their patients to HC in order to increase patient levels of physical activity and exercise. Further, only 20% of physicians surveyed refer their patients to a PT. Concurrently, when asked which exercise options offered at HC they are supportive of, physicians ranked aerobic activity highest and working with a PT lowest. While belief that HC are appropriate for their patients and favourable views of HC were associated with support of PT for their patients, less than half of physicians surveyed indicated that they were concerned with certified trainers, specific outstanding teachers/trainers or certification of the facility. This may suggest a lack of knowledge of specific fitness certifications or, potentially, a disregard of these certifications in general. Indeed, in a section on the survey for open comments regarding negative feelings towards HC (data not presented), 13 out of 40 comments (33%) referenced poorly trained PT.
Although 33% of physicians named a variety of separate and distinct HC, the most recognised single HC was YMCA, with 63% open comments (15 out of 24, data not presented) referencing affordability and convenience for patients as a reason for favourability. Interestingly, 20% of physicians could not name any HC they held in high regard. When asked to indicate all elements of what physicians do (or would) look for in recommending a specific HC to their patients, more than half of physicians were concerned about the club offering a wide range of activities, convenience, a clean and pleasant facility and helpfulness of staff. Physicians cited expense and convenience as most problematic for patient referral, with 72% of physicians indicated cost to patients was the element that was most concerning.
This study does have some limitations. Specifically, physicians were not asked to differentiate between generally healthy patients and those with non-communicable chronic disease (ie, cardiovascular disease or type 2 diabetes) that may require specialty supervision. This clarifying point may have affected their recommendation. Moreover, this study did not investigate the global ranges of certification that fitness professionals can pursue and that may limit generalisability, particularly between countries.
Despite the limitations and given the burgeoning market of the health and fitness industry, the observed disconnect in this study between the clinical and fitness practitioner domains is somewhat alarming. The former president of the American College of Sports Medicine recently called for the establishment of a ‘pharmacy’ for exercise prescription, staffed by patient support people with backgrounds in health, fitness and/or nutrition.6 Our results, however, suggest that there is a gap of communication and referral between physicians and HC, with a particular breach regarding PT. Given that physical activity programming has been recommended to be personalised, based on individual habits, preferences, motivation and tolerance,16 and presented in such a way that will ‘…fit more seamlessly into the context of …daily routines’,17 this divide could be seen as problematic for implementation. By dismissing HC, and PT in particular, as viable options for personalised exercise care, physicians may be limiting their patients’ exposure to a critical component of healthy lifestyle behaviour. Moreover, this partnership may attenuate physician uncertainty about the effectiveness of written PA prescription, as recently reported.15
Conclusion
Physicians are uniquely positioned to educate patients regarding the importance of physical activity and to encourage all patients to make exercise a regular part of their lifestyle. In the last decade, there has been a 40% increase in all patients receiving advice to exercise by their primary care physicians, yet still only one in three patients have been so advised.18 Our results suggest that less than half of physicians who are familiar with HC would refer their patients to one, and only 20% would refer to a PT. This could be an unfavourable oversight for patients given results from a recent report that suggest exercise capacity could be a more important indicator of mortality than even BMI.19 It is of the utmost importance that initiatives and partnerships are cultivated to bridge this gap and, more critically, build trust between the medical institutions prescribing exercise as medicine and the practitioners ‘filling’ these prescriptions in HC and the community at large.
Ethics approval
Spaulding Rehabilitation Hospital Institutional Review Board.
Footnotes
Contributors RP was responsible for data interpretation and manuscript preparation. MAK was responsible for planning and conducting the study. FA was responsible for planning and data analysis. AB and EP were responsible for planning and conduct of the study and manuscript preparation.
Funding This study was funded by International Health, Racquet, and Sportsclub Association.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data will be made available upon request.