Article Text

Abstract
Objective To review existing biomechanical and clinical evidence regarding postoperative weight-bearing and range of motion restrictions for patients following meniscal repair surgery.
Methods and data sources Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline, we searched MEDLINE using following search strategy: ((((“Weight-Bearing/physiology”[Mesh]) OR “Range of Motion, Articular”[Mesh]) OR “Rehabilitation”[Mesh])) AND (“Menisci, Tibial”[Mesh]). Additional articles were derived from previous reviews. Eligible studies were published in English and reported a rehabilitation protocol following meniscal repair on human. We summarised rehabilitation protocols and patients’ outcome among original studies.
Results Seventeen clinical studies were included in this systematic review. There was wide variation in rehabilitation protocols among clinical studies. Biomechanical evidence from small cadaveric studies suggests that higher degrees of knee flexion and weight-bearing may be safe following meniscal repair and may not compromise the repair. An accelerated protocol with immediate weight-bearing at tolerance and early motion to non-weight-bearing with immobilising up to 6 weeks postoperatively is reported. Accelerated rehabilitation protocols are not associated with higher failure rates following meniscal repair.
Conclusions There is a lack of consensus regarding the optimal postoperative protocol following meniscal repair. Small clinical studies support rehabilitation protocols that allow early motion. Additional studies are needed to better clarify the interplay between tear type, repair method and optimal rehabilitation protocol.
- arthroscopy
- knee surgery
- knee injuries
- sporting injuries
- rehabilitation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known?
The menisci reduce stress by increasing the contact area between the femur and tibia.
Meniscal repair is becoming a more appealing treatment for meniscal injuries.
There is a wide variation between postoperative rehabilitation protocols following meniscal repair.
What are the new findings?
There is no consensus regarding postoperative rehabilitation protocol for meniscal repair.
The quality of existing evidence is low.
An accelerated rehabilitation protocol may be safely implemented for appropriate patients.
Further studies are needed to determine an optimal rehabilitation protocol.
Introduction
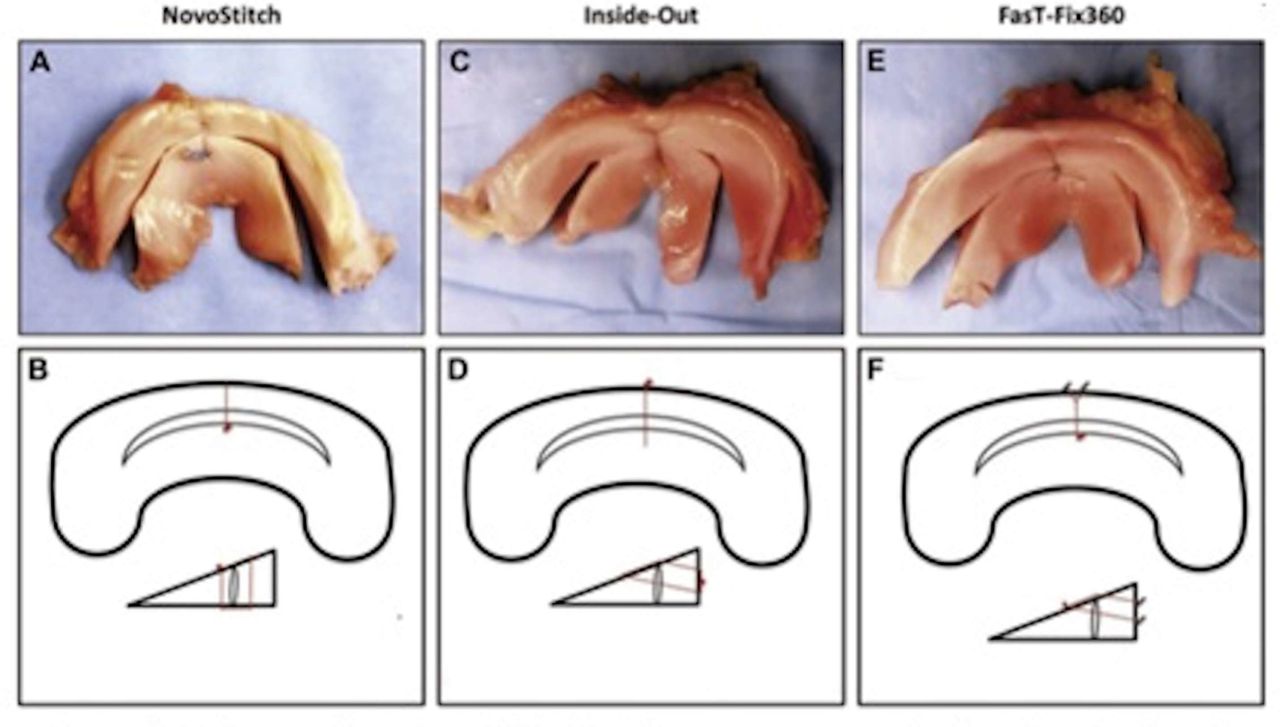
The menisci reduce stress by increasing the contact area between the femur and tibia. They buffer against axial, rotational and shearing forces about the knee during motion.1 The loss of meniscal tissue localises tibiofemoral contact and leads to progressive arthrosis2 3 and functional decline in the long term.4 To prevent these degenerative changes, meniscal repair has become more common.5 Kim et al6 documented a 25% increase in medial and lateral meniscal repairs between 1996 and 2006. Even though the majority of surgeries on the meniscus remain meniscectomies, Abrams et al7 found that between 2005 and 2011 more isolated meniscal repairs were performed in the USA without an increase in the number of meniscectomies. Meniscal repairs may be performed more frequently because there has been a significant advance in surgical techniques and repair devices (figure 1A–E). Historically, the gold standard for meniscal repair has been the inside-out technique (figure 1C,D). Long flexible needles are used to pass sutures through the tissue under arthroscopic guidance.8 The sutures are then retrieved using a separate incision and are tied over the joint capsule. This technique may place neurovascular structures at risk and requires an additional incision.9 To avoid the morbidity associated with an inside-out repair, ‘all-inside’ arthroscopic techniques have been developed (figure 1A,B). These include anchor-based repairs and suture-based repairs. The most popular of these designs employ pre-tied sutures between non-absorbable anchors. The anchors are deployed when an introducer is passed through the meniscal tear and the joint capsule (figure 1E,F). In a study of porcine meniscal repairs,10 the inside-out technique was significantly stronger compared with recent all-inside repair devices. A study on fresh-frozen human menisci11 showed no difference. Although potentially less invasive than the inside-out technique, all-inside repairs can result in neurovascular injury, irritation from anchors and implant failure.12

(A, B) All-inside suture-based repair, (C, D) inside-out suture repair and (E, F) anchor-based repair techniques.
Several factors may influence meniscal healing. The most important may be the meniscal blood supply. Scapinelli13 in 1968 and Arnoczky and Warren14 in 1982 described the limited peripheral blood supply to the outer one-third to one-quarter of the meniscus. From this finding, peripheral meniscal tears (ie, tears in the ‘red-red’ zone) are felt to have better healing potential (figure 2A).
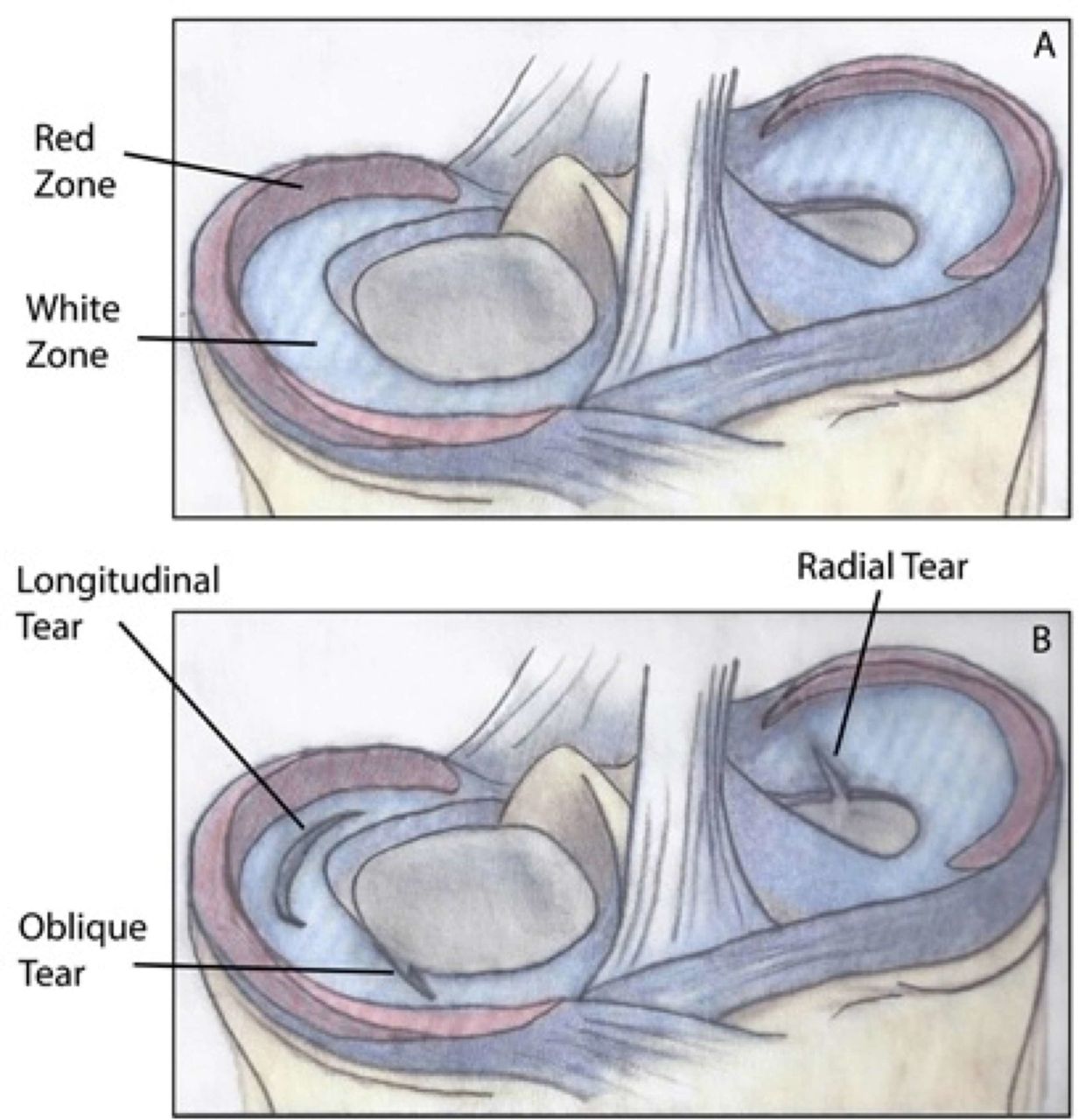
(A) Outer red zones receive blood supply; (B) longitudinal tears have a higher likelihood of being vascularized.
The timing and type of meniscal tear may also impact healing. Acute, traumatic tears tend to have higher healing rates than chronic, atraumatic tears.15 Longitudinal tears are more amenable to repair due to their vertical orientation (figure 2B), whereas radial tears extending to the central relatively avascular ‘white-white’ zone are more challenging. Some surgeons have reported success when repairing bucket-handle tears extending to the white-white zone.16
Age is another topic for consideration. Preserving meniscal tissue is particularly important for the long-term health of young athletes, and younger patients may have a higher healing potential. In one study of 26 patients aged 17 years or younger, none required a repeat surgery at an average of 5 years of follow-up.17 In another report on two very young cases, meniscal repair for traumatic tears followed by limited weight-bearing rehabilitation resulted in a positive outcome.18 When age is not a factor, a meta-analysis investigating outcomes at least 5 years after meniscal repair showed a pooled failure rate of 23.1%.19
As biomechanical factors, postoperative range of motion (ROM) and weight-bearing status can impact meniscal healing after repair. The interplay between tear type and knee biomechanics can help define the most appropriate postoperative plan.
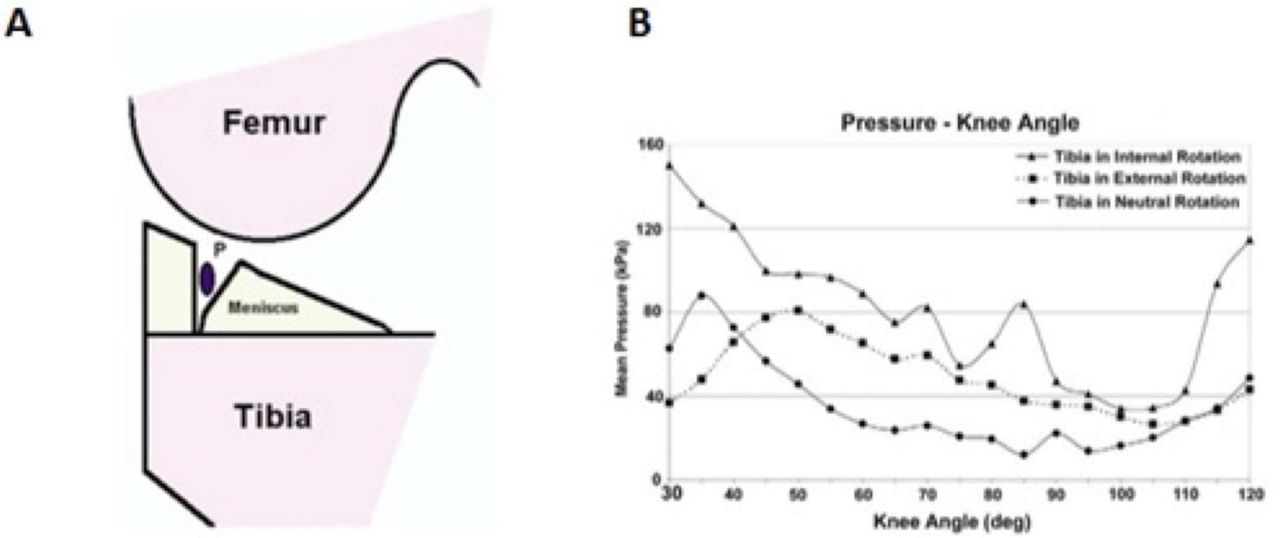
Restricting a patient’s postoperative ROM intends to limit the risk of re-tear. Cadaveric studies have shown that femorotibial contact pressures increase with knee flexion.20 If the ROM is restricted, the meniscal repair may be protected from increased mechanical stress.21 However, Richards et al22investigated the effects of compressive loads in porcine longitudinal lateral meniscus repairs and found that weight-bearing reduced the meniscus and stabilised the repair. The highest compressive force occurred at full extension and the lowest was at 90° of flexion. Beyond 100° of flexion, it increased steadily (figure 3). Higher pressures were seen with internal rotation of the tibia, suggesting torsional forces may be different than axial loads. Conversely, for radial tears, axial loading might displace, rather than reduce, the injury.22 Of note, cadaveric investigations are limited in their ability to recreate the biomechanics of the knee in vivo and are not able to predict how specific rehabilitation protocols impact a meniscal repair. For this reason, rehabilitation following a meniscal repair is particularly conservative in an effort to protect the repaired meniscus.
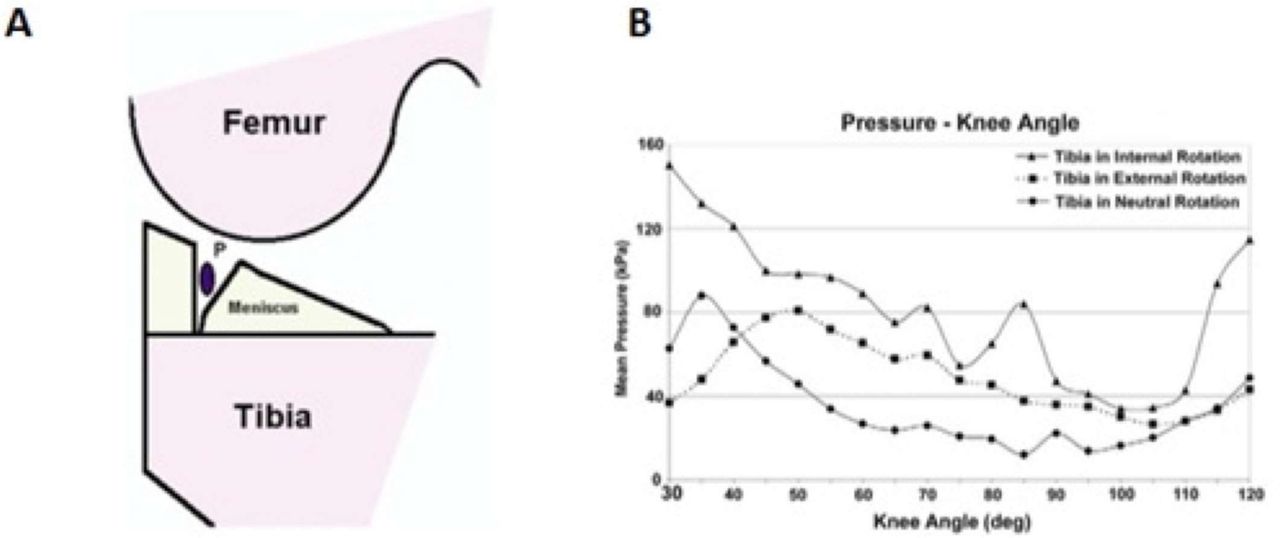
(A) The pressure transducer ‘P’ was placed in the lateral meniscal cut and the knee was cycled into flexion and extension. (B) Intrameniscal pressures were reflected in neutral, internal, and external rotation.
Postoperative rehabilitation aims to foster healing after meniscal repair and facilitate the patient’s return to full function. Generally, these programmes are initially focused on protecting the repair while regaining ROM and gradually introducing progressive strengthening en route to a return to preinjury activity level. At present, there is a paucity of evidence to support one best practice and there is a high degree of variability among postoperative rehabilitation programmes. Considering the increased frequency and evolution of meniscal repairs, this review intends to summarise the best-available evidence and practices regarding the postoperative care and rehabilitation of patients undergoing a meniscal repair.
Methods
Search strategy and data sources
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline, on 15 June 2017 we conducted an electronic search on MEDLINE with the following search strategy: ((((“Weight-Bearing/physiology”[Mesh]) OR “Range of Motion, Articular”[Mesh]) OR “Rehabilitation”[Mesh])) AND (“Menisci, Tibial”[Mesh]). Additional sources included references of previous reviews.19 23 24
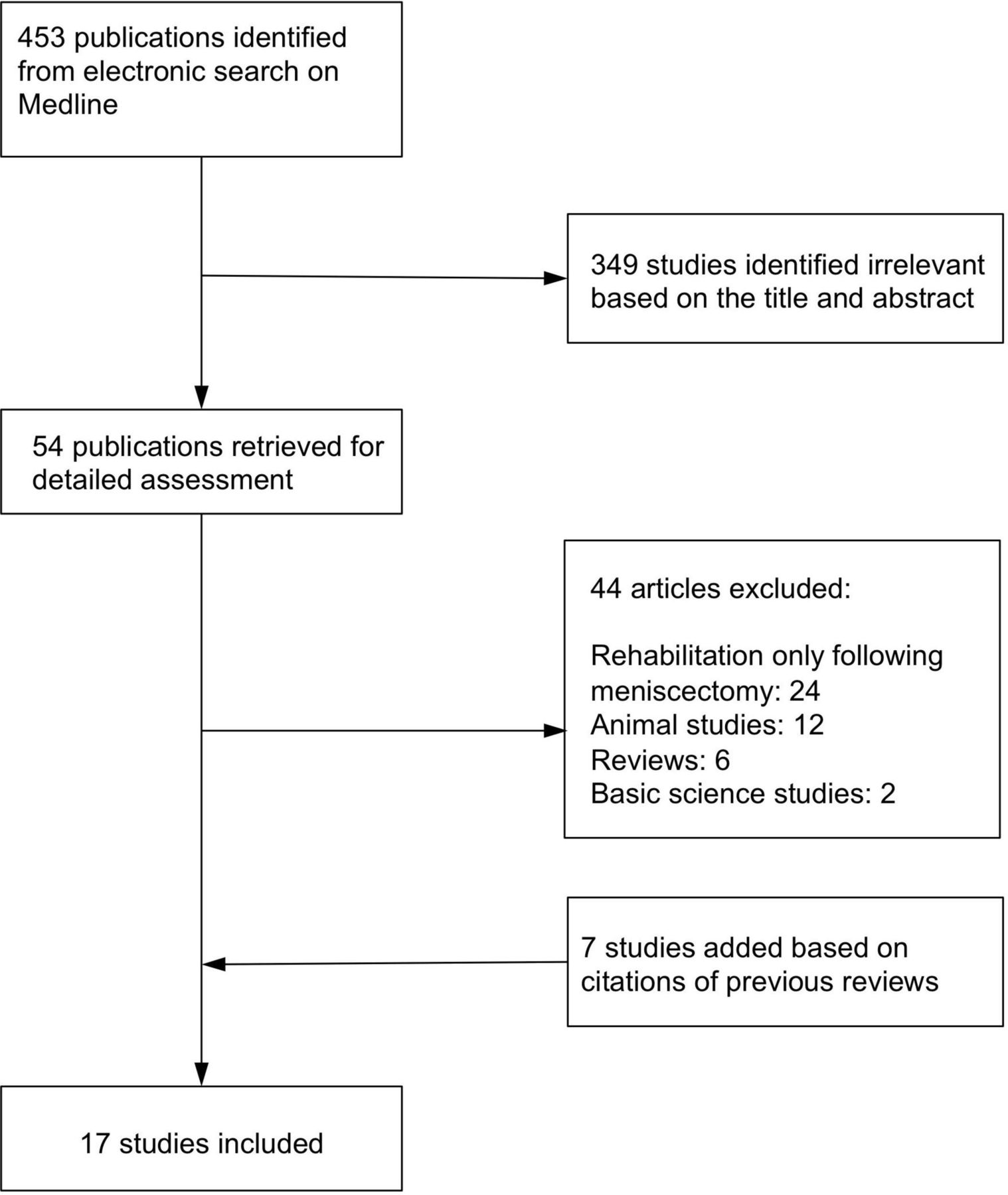
A total of 453 studies were screened for eligibility. Only studies published in the English language in peer-reviewed journals were considered. Review papers, commentaries and studies on rehabilitation protocol following meniscectomy were excluded. Finally, 17 studies were included in the review (figure 4).

Flow chart of the systematic review.
Bibliographic data, patients’ characteristics, rehabilitation protocol and clinical outcome were recorded. Patient’s outcome included meniscal healing, return to activities and clinical assessments based on the original studies. We did not confirm collected data by authors. The level of evidence for original studies is reported for each study.25
Cochrane tool for evaluating risk of bias was used for assessing the methodological quality of the included studies.
Results
Seventeen clinical studies including 798 patients were reviewed in this systematic review. There was wide variation in methodological quality of clinical studies. The majority of studies had considerable risk of bias (table 1).
Assessment of risk of bias using Cochrane tool
A restricted rehabilitation protocol was used for 438 patients. An accelerated protocol with immediate weight-bearing at tolerance was used in 360 patients. Three studies compared restricted and accelerated protocol, which did not show any significant difference in complication rate or functional assessment (table 2).
Previously published rehabilitation protocols
Although a meta-analysis was not possible, it seems accelerated rehabilitation protocols are not associated with higher failure rates following meniscal repair.
Discussion
Many rehabilitation programmes propose avoiding weight-bearing forces as an important goal in the immediate postoperative period to protect the repair from high compressive and shear forces. An MRI study of weight-bearing and non-weight-bearing knees found that the relative tibiofemoral movements of the loaded knee were similar to those in the unloaded knee. However, the medial femoral condyle moves approximately 4 mm anterior when the knee bends from full extension to 10° of flexion while bearing weight. In the unloaded knee, the position of the medial femoral condyle did not change from extension to flexion. Laterally, the femoral condyle rolls forward 13 mm from 110° to 60° of flexion and 1 mm from 60° to 0° in the unloaded knee.26 In isolation, this pattern of motion suggests that non-weight-bearing knee flexion would be safe to 110° for medial meniscal repairs and to 60° for lateral meniscal repairs. However, this finding has not been validated clinically.
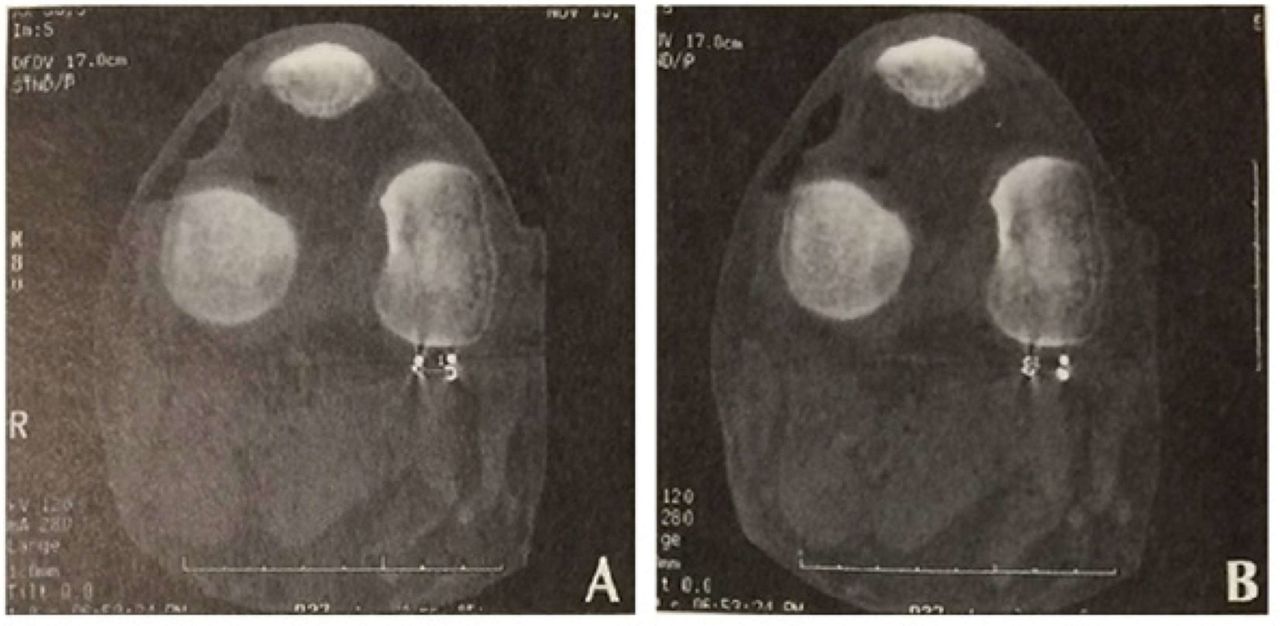
Becker et al20 investigated changes in the meniscofemoral contact pressure after meniscal repair. Knees were loaded to approximately 50% of body weight, and meniscofemoral contact pressure was measured (Tekscan, Boston, Massachusetts, USA) while cycling the knee from extension to 90° of flexion. They found that meniscofemoral pressures increased in both compartments as the knee flexed and that meniscal repair had no impact. Their study did not investigate the effect of this pressure difference on the meniscal repair, nor did they include torsional forces or higher impact loading. Ganley et al27 sought to further investigate knee flexion and loading on meniscal healing in a cadaveric model. They produced full-thickness posteromedial meniscal tears in cadaveric knees and imbedded metal markers into the tear following repair. Using CT scans, the marker position was assessed at 30°, 60° and 90° of knee flexion after loading of 100 lbs to simulate partial weight-bearing. They determined that neither flexion angle, loading nor suture had a significant impact (figures 5 and 6). In this way, accelerated rehabilitation programme with partial weight-bearing may be appropriate. Torsional forces, higher degrees of flexion and loads larger than 100 lbs were not assessed.

Transverse section of a cadaver knee under 100 lbs of load at 60°. (A) Longitudinaland (B) transverse measurements are depicted between the markers.
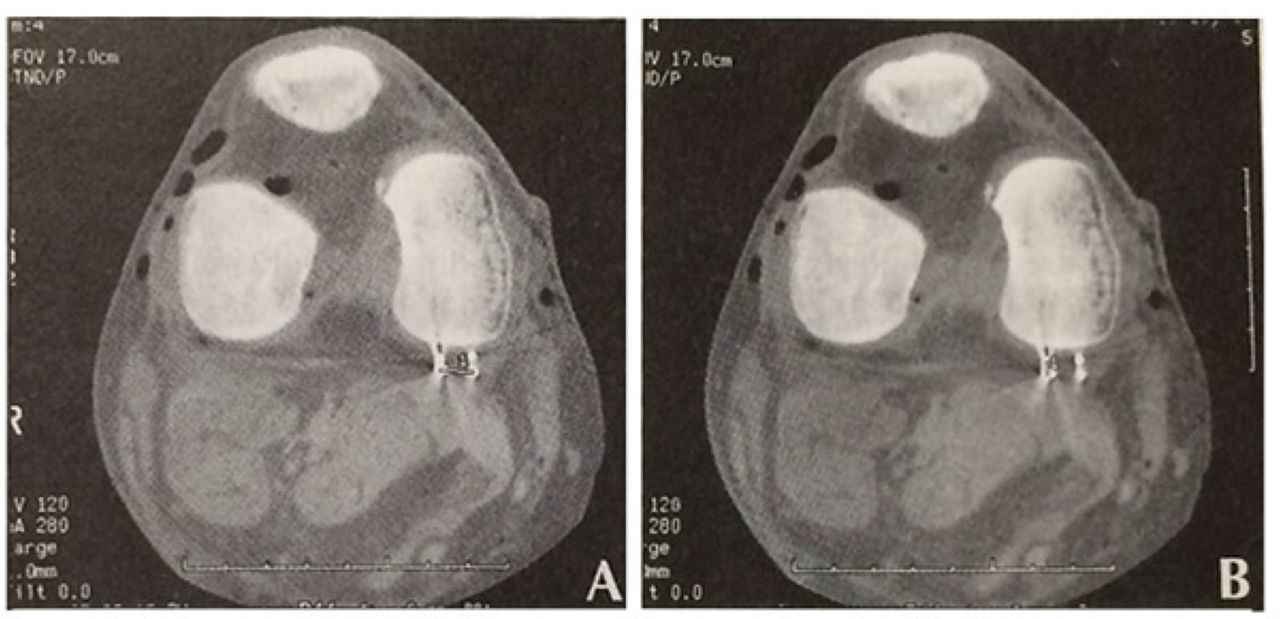
Transverse section of a cadaver knee without load at 60°. (A) Longitudinal and (B) transverse) measurements are depicted between the markers.
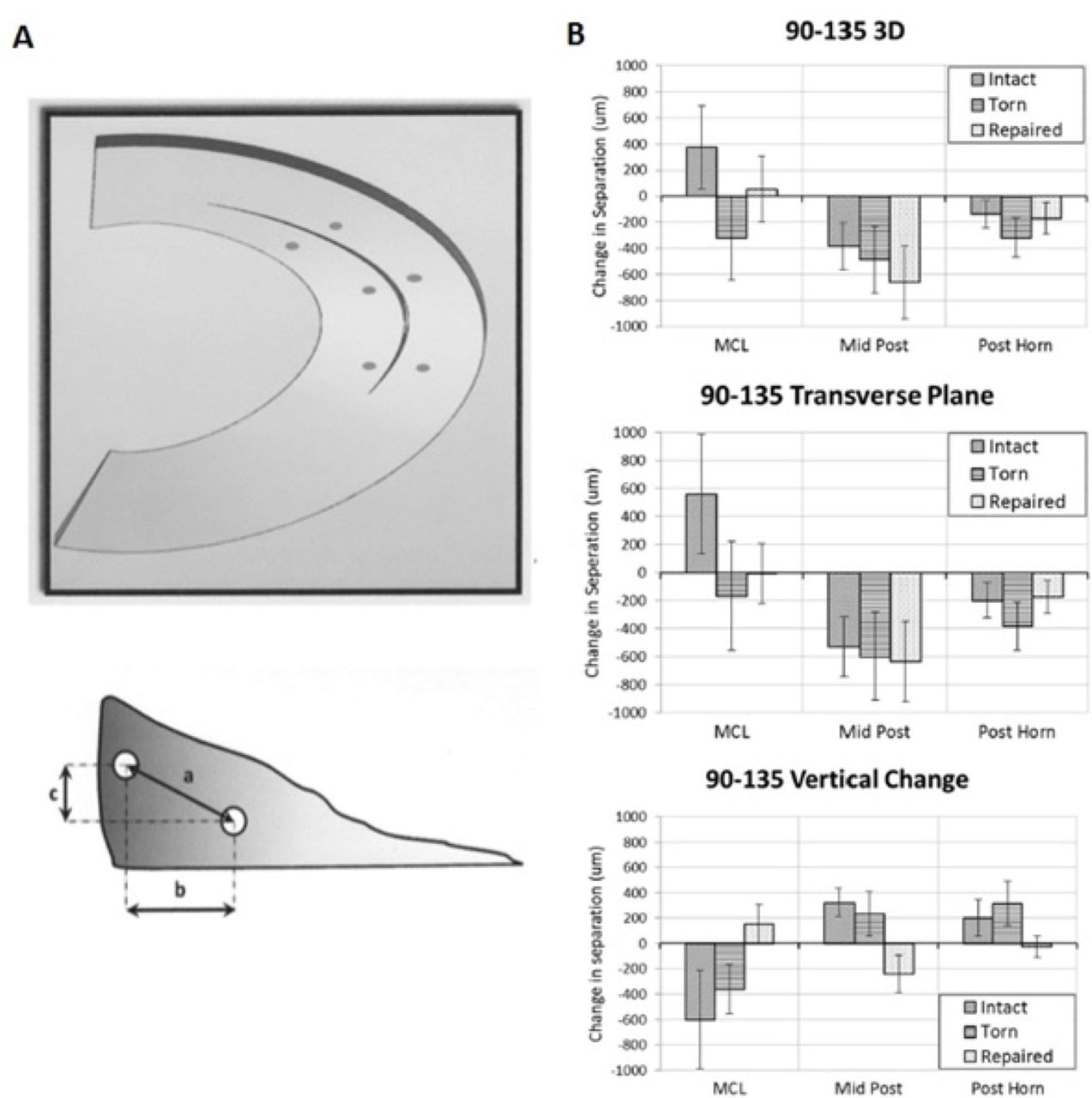
Lin et al28 sought to assess the effect of postoperative ROM following meniscal repair using a cadaveric model. They created a 2.5 cm posteromedial meniscal tear and repaired it with inside-out vertical mattress sutures (figure 7A). They measured the displacement at high degrees of flexion (90°, 110° and 135°) when loaded (figure 7B). Specimens were subjected to simulated open-chain flexion and extension with a load of 29 N applied to the hamstrings and 150 N to the quadriceps, exceeding the normal joint reactive force encountered during active knee flexion.28 In accordance with the findings of Richards et al22 and Ganley et al,27 they found that neither the meniscal tear nor the meniscal repair demonstrated significant gapping. Rather they compressed in the transverse plane when flexed from 90° to 135°s while subjected to physiologic loads. They conclude that ‘non-restrictive un-resisted open chain ROM protocols do not place undue stress on meniscal repairs’.

(A) Schematic of roentgen stereophotogrammetric analysis bead pair placement in relation to tear. Distances measured by vectors: a—absolute, b—transverse and c—vertical. (B) Changes in separation for each vector. Positive values indicate widening. Negative values indicate compression. MCL, medial collateral ligament region of posterior horn of medial meniscus; mid post, middle of posterior horn; post root, posterior root area of medial meniscus.
Early weight-bearing might enhance the mechanical environment promoting healing and allowing earlier functional recovery and return to sport.22 It has been shown that early weight-bearing as tolerated and limited ROM resulted in acceptable outcomes (ie, Lysholm score of 71.5) at 17 month follow-up.29 While Becker’s cadaveric findings may alleviate concern over iatrogenic cartilage damage from implants, the hypothetical danger of increased meniscofemoral pressures with knee flexion after meniscal repair has not been shown to impact clinical outcomes.20
Some authors recommend immobilisation in full extension, reportedly due to the observation that peripheral posterior horn tears move away from the capsule in flexion and reduce in extension.18 30–32 This recommendation stems from direct viewing of peripheral posterior horn tears using a 70° arthroscope and observing the reduction of these tears during passive knee extension. However, this observation and the subsequent practice of immobilising meniscal repairs in extension has not been shown to be beneficial clinically and may not be relevant to other tear types. Some investigators recommend immobilisation in various degrees of flexion,32–34 and others still advocate for limited early motion. Despite more aggressive protocols allowing for free ROM immediately postoperatively, 90° of flexion appears to be a comfortable restriction for surgeons.35 Up to 85% of the load travels through the menisci with the knee in 90° of flexion, while less (50%) of the load passes through the meniscus in extension.36
Additionally, meniscal dynamics using MRI three-dimensional reconstructions show that during knee flexion, the posterior excursion of the medial meniscus is 5.1 mm and the lateral meniscus is 11.2 mm.37 However, a more recent study by Lin suggests that higher degrees of flexion may be safe.28 There is no clinical evidence that limiting weight-bearing and/or knee flexion improves healing rates. Long-term outcome studies are lacking.
Accelerated rehabilitation protocols
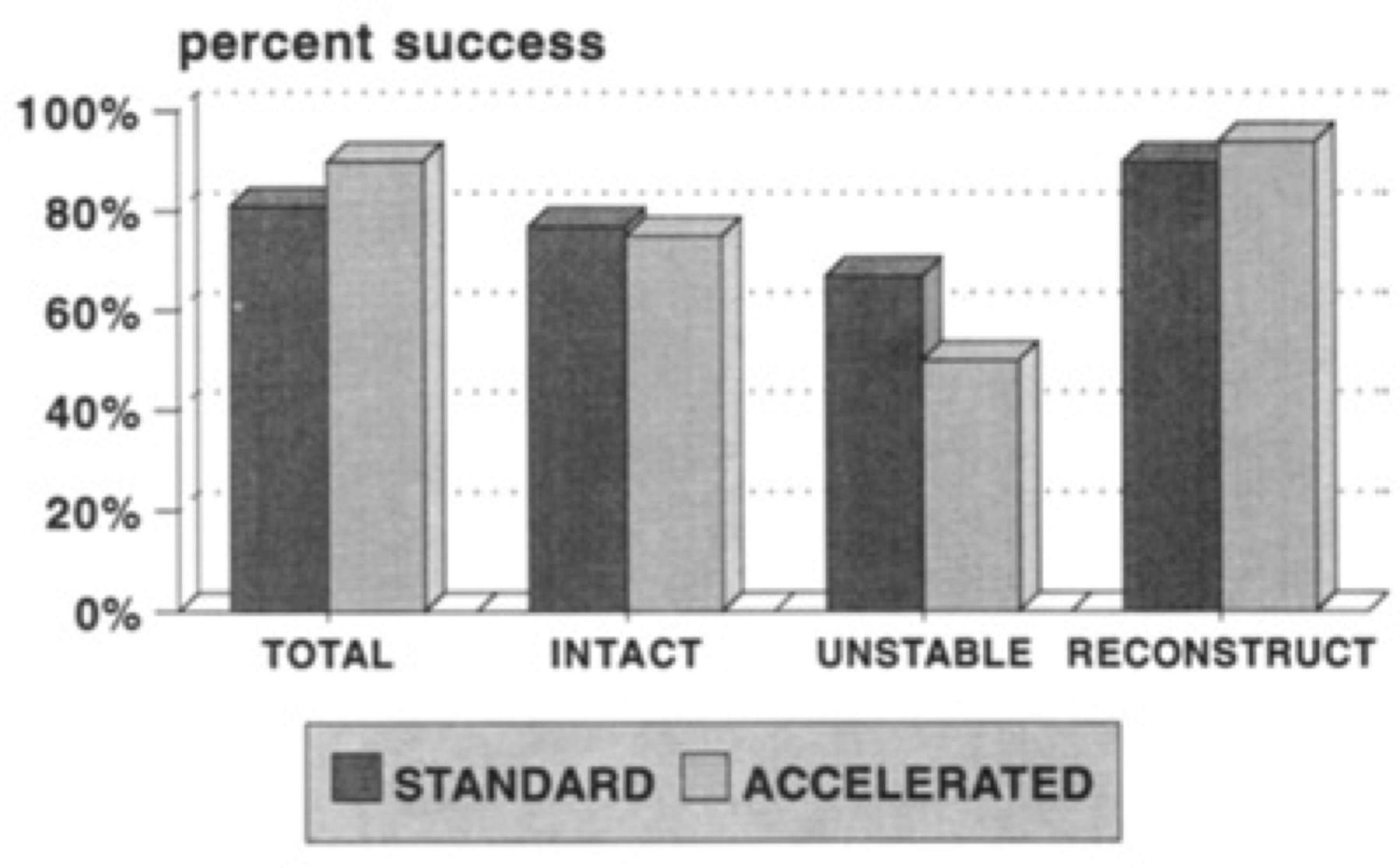
A number of investigators have advocated for accelerated rehabilitation protocols (figure 8).38–41 In a prospective randomised trial, Lind et al28 compared the impact of a ‘free rehabilitation’ regimen versus ‘restricted rehabilitation’.35 Sixty patients underwent isolated repair of a vertical meniscal lesion using an all-inside technique. They were randomised by rehabilitation regimens. The ‘free’ group was allowed to range the knee 0°–90° immediately while maintaining the knee in touch-down weight-bearing for 2 weeks, and weight-bearing as tolerated thereafter. They were allowed to return to contact sports at 4 months. The ‘restricted’ group wore a hinged brace for 6 weeks and gradually increased their ROM to 90°. They were touch-down weight-bearing for 6 weeks, followed by eventual return to sport at 6 months. The authors found no difference in the healing rate. At second-look arthroscopy, there were 9 and 10 failures in the free and restricted rehabilitation groups, respectively. There was no difference in functional outcome scores at 2 years. From this experience, the authors concluded that free rehabilitation was safe without a higher failure rate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meniscus repair success: standard versus accelerated. No difference in success rates exists between the standard accelerated rehabilitation groups.
Kocabey et al42 reported excellent results using rehabilitation guidelines specific to the tear’s characteristics. For anterior-posterior longitudinal tears less than 3 cm, they promoted weight-bearing as tolerated without a brace. ROM progressed to 125° between 3 and 6 weeks. For tears greater than 3 cm, weight-bearing was allowed in a locked brace. ROM was limited to 0°–125° until 6 or 8 weeks. Return to sport was allowed after 3 months. For complex and radial tears, patients were required to wear a brace in which they were weight-bearing as tolerated ranging from 0° to 125° for 6 to 8 weeks. They returned to sport between 4 and 5 months.
Mariani et al40 followed 22 patients who underwent an outside-in meniscal repair. They were allowed to bear weight immediately without ROM restrictions. On re-examination with an MRI at an average of 28 months after surgery, only 3 of 22 patients showed signs of re-tear with greater than 1 mm of gapping. Based on this experience, they advocated for more aggressive rehabilitation regimens.36
There remains a concern regarding the safety of accelerated rehabilitation in the setting of a radial meniscal tear. Most studies investigating rehabilitation after meniscal repair have included patients with a longitudinal tear. However, since radial tears experience distraction forces and increased strain with axial loading, it is thought that a more conservative postoperative rehabilitation approach may be prudent in this setting.43 Choi et al44 and Haklar et al45 reported on their experiences repairing isolated radial tears of the lateral meniscus. Choi et al44 used a weight restriction protocol, whereas Haklar used a dual restriction protocol.
Overall, there is considerable variability in the rehabilitation following a meniscal repair. There is no clear consensus regarding the ideal programme (table 2). On the one hand, Noyes limited weight-bearing initially for 4–6 weeks, with ROM progressively advanced to 135° of flexion over 6 weeks.46 At the other end of the spectrum, O’Shea and Shelbourne 47 published favourable results after unrestricted ROM with weight-bearing as tolerated beginning 3 days after surgery. Similarly, Bryant et al48 allowed weight-bearing to tolerance with the knee locked in extension for 3 weeks, then WBAT with unlimited ROM thereafter. The impact of weight-bearing combined with twisting or pivoting movements on the repaired meniscus has not been adequately investigated. Furthermore, rehabilitation protocols with respect to meniscal repair with or without augmentation have not been evaluated.
Return to sport
The decision to repair a meniscus influences both the long-term health of the knee as well as the more immediate ability to return to activity. The postoperative treatment is an important consideration that should be discussed with the patient when considering a meniscus repair. Meniscal preservation offers long-term benefits. However, because the recovery requires a longer period of immobilisation with restrictions and delays the return to sport, some athletes might not want to have a meniscal repair. In one study of 45 meniscal repairs in elite athletes, 81% returned to sports, with the vast majority back to their prior sporting level.49 The mean return to sport was 5.6 months (range 3–8 months) for an isolated meniscal tear, compared with 11.8 months for ACL reconstruction with meniscal repair.
Meniscal repair in association with ACL reconstruction
Accelerated, or aggressive, rehabilitation is important following ACL reconstruction to improve ROM.41 Several studies have shown that accelerated rehabilitation is safe following ACL reconstruction with meniscal repair.40 50 In a series of 63 consecutive patients, 58 meniscal tears were repaired arthroscopically using an inside-out technique at the time of ACL reconstruction. Barber et al50 promoted a rapid return to full function. Patients were aggressively rehabilitated to playing non-contact pivoting sports at 10–12 weeks, with unlimited activity using a derotational brace as early as 3–4 months once adequate motion (0°–120°), good strength and no effusion were achieved. With regards to meniscal repairs, the authors noted a lack of consensus regarding rehabilitation protocols and called restrictions into question.
Many surgeons do not restrict patients after meniscal repair in the setting of concurrent ACL reconstructions. It has been hypothesised that meniscal repairs benefit from an abundance of healing factors due to the intra-articular bleeding present during an ACL reconstruction. In a matched cohort study by Wasserstein et al,51the patient cohort with concomitant ACL reconstruction was found to have a meniscal reoperation rate of 9.7% compared with 16.7% in the meniscus repair alone cohort. Conversely, in an ACL-deficient knee, meniscal repairs are prone to failure due to the persistent mechanical stress on the tissue.31 52 53
Conclusion
Meniscal repair is an important procedure that aims to preserve tissue and prevent future arthrosis. While treatment may alleviate symptoms and allow for a timely return to activity, there is a lack of consensus regarding the optimal postoperative rehabilitation protocol. Moreover, there is scarce evidence supporting many current practices. Biomechanical evidence suggests that high degrees of knee flexion may be safe, but these data are limited to a few cadaveric studies. The impact of rotation and torsion forces has not been determined, but have implications for the return to sport and work. It is unclear whether larger joint forces associated with running or jumping threaten the meniscal repair.
An accelerated rehabilitation protocol may be safely implemented for appropriate patients, but it is unclear how the type of meniscal tear and the repair technique should affect the postoperative programme. Additional biomechanical studies are needed to better clarify the interplay between tear type, repair method, knee loading, knee positioning and torsional forces. Clinical studies investigating these specific elements will help to optimise patient outcomes.
Acknowledgements
The authors would like to acknowledge the generosity of Mr. Joseph Fallon for providing funding for this project.
References
Footnotes
JPD, AN and AJR are joint senior authors.
JPD, AN and AJR contributed equally.
Contributors RCS, MCN, AM, JPD, AN and AJR developed the idea of the study. RCS, MCN and AM collected the data. JPD, AN and AJR approved the accuracy of the collected data. RCS, MCN and AM prepared first draft of the manuscript. JPD, AN and AJR provided clinical and biomechanical insight to the study. All authors approved final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Not required.
Data sharing statement This is a systematic review of previously published studies. All studies are available to the public.