Article Text

Abstract
Background Evidence concerning the use of vibrotactile feedback for acquiring and learning new motor skills is limited. Although various concepts and applications for tactile feedback have been proposed, little is known about the suitability of this feedback mechanism in sports training.
Aim The goal of this systematic review was to gather knowledge on the efficacy of the use of vibrotactile feedback in improving sports performance skills.
Design Systematic review.
Methods Comprehensively searched databases were: PubMed, Cochrane and Web of Science. Studies investigating the effects of using vibrotactile feedback in sports training in healthy subjects were included in this review.
Results No consensus was found regarding the positive effectiveness on performance using vibrotactile feedback in a sports context. No evidence was found that the addition of tactile feedback is effective for acquiring new motor skills. None of the studies show a significant learning effect.
- Review
- Physiology
- Neuromuscular
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known?
Motor tasks are controlled by intrinsic feedback mechanisms.
Augmented feedback (verbal instructions) in learning new motor tasks is important in sports.
What are the new findings?
The use of vibrotactile feedback in several medical and non-medical areas has well been established.
Vibrotactile feedback as feedback tool in sports has not yet been supported by scientific evidence.
There lies a huge potential for sports science to study feedback mechanisms by using vibrotactile feedback as intervention tool.
Introduction
When an athlete performs a designated movement (motor task), any attempt is neurophysiological evaluated by scanning the information originating from intrinsic feedback (IFB) systems such as visual, auditory, proprioceptive and/or tactile feedback (TFB). Those feedback (FB) systems analyse and adjust extremity position either in real time (concurrent FB) or store the information during post-task evaluation (terminal FB).1 Thus IFB leads to the information regarding the outcome of the motor task (knowledge of results) and provides information of the entire process of a motor task (knowledge of performance).1 2 The only IFB system that is in direct contact with the environment is tactile sensory system, known as TFB. TFB allows us to interact with the environment through specific sensors in the skin. They sense vibration, pressure, touch, texture and so on. TFB is complex and is primarily composed of a skin sensation, enabling subjects to localise and recognise individual tactile cues and collaborates closely with the proprioceptive and kinaesthetic system, that is, body part position recognition.3 Interestingly, TFB is the only FB system that is bidirectional, that is, it interacts with the environment and simultaneously senses and processes such interactions.4–6 Although TFB is essential for movement-controlled actions, it can also be a disturbing factor by creating a kind of sensory overload mainly because it can also be handled consciously.7
In contrast to IFB, augmented feedback (AFB) serves as an add-on to the task-intrinsic information and is exclusively delivered by external cues.2 To date, it is impossible to consider modern sports training, but also rehabilitation of certain patient groups, without the use of AFB. AFB comes from external sources, for example, trainers/coaches, electronic devices (displays, sounds), spectators and recently also haptic systems (robots, vibrotactile (VT) actuators), or a combination thereof.3 AFB has also been shown to play an important role in learning new motor tasks by enhancing the effect of IFB.5 8 This can be provided verbally (a coach provides detailed spoken instructions), visually (a coach demonstrates the specific task) or haptic (a coach guides part of the trajectory of the movement by touching the subject at key parts of the motor task) cues. Mostly, however, AFB is offered after completion of a motor task, as terminal FB. Although it has been shown that terminal FB can play an important role in the learning process of motor tasks, the major drawback of this type of FB is that it only provides information on the outcome of the motor task but not real time on the process as in concurrent FB.5 Nowadays, technological progress allows us to provide information to an athlete in real time. One of such methods is vibrotactile feedback (VTFB). During VTFB, a signal is generated by an actuator that applies vibrational stimuli to the skin guided by information on position of an extremity.9 VTFB is a form of concurrent FB and information can be delivered by varying temporal parameters in frequency, amplitude, waveform and/or duration.10 The tight coupling between motor task and the resulting VTFB stimuli requires a minimal latency.11 Instant and real-time augmented VTFB makes it feasible to provide spatial proprioceptive information during a complex motor task.12 In this sense, VTFB can thus be used to guide a motor task and provide instant FB. VTFB is, from a neurophysiological point of view, an interesting source of FB, since it can bypass the athletes’ visual FB system. The relatively small, low-weight and wireless potential makes it an excellent FB tool.3
Prior to the use of VTFB, consistent metaphors need to be learnt. Amemiya et al suggested that wearable VTFB devices should create realistic sensations.13 In that light, Spelmezan and Ziefle distinguished two types of encoding metaphors: a push and a pull metaphor.14 The pull metaphor means that the extremity of a subject reacts to a signal by moving towards the stimulus, whereas the push metaphor means that it pulls away from the stimulus.
The major aim of this present systematic review is to evaluate the definitions, methodologies and use of FB systems for learning motor tasks in sports. To the best of our knowledge, this is the first systematic review on VTFB systems within sports.
Methods
Design
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, which is an updated statement addressing the conceptual and methodological issues of the original QUOROM (Quality of Reporting of Meta-Analyses) statement.15
Search strategy
PICO(S) components were used to establish the research question. This PICO(S), along with the corresponding eligibility criteria, is shown in table 1.
PICOS and eligibility criteria
To complete this review, three electronic databases were used. PubMed (http://www.ncbi.nlm.nih.gov/pubmed/), Web of Science (WOS; https://webofknowledge.com/) and the Cochrane database (http:// www.cochranelibrary.com) were searched for peer-reviewed articles.
The Cochrane was used to find relevant clinical trials without date restrictions as search option. Using the advanced search option, a selection was made to find clinical trials only. Conference papers were excluded. FB conditions where VTFB is used to only robotically guide someone, that is, the subject playing a passive role, were also excluded from this review, along with FB conditions where VTFB is used as sensory substitution.
In addition, we manually searched for relevant articles based on article citations and reference lists in the PubMed and WOS databases. The articles found were extracted and organised in EndNote Online. Duplicates were removed manually. The first search was performed in October 2015 and the date of the last search was on 30 March 2017.
The search strategy is shown in table 2.
Database search strategy
Study selection
After implementation of the research strategy in all databases and the execution of the manual search, articles were extracted and organised in EndNote Online. Duplicates were deleted by hand. The remaining articles were transferred to an Excel template published by the KCE-Belgian Health Care Knowledge Centre (http://kce.fgov.be/). Two hundred and ninety-six (296) articles from the three used databases, 321 studies selected for screening and 25 records from other sources (30 March 2017) were sequentially included or excluded according to the eligibility criteria. Two reviewers (KW and TP) performed eligibility assessment independently in an unblinded standardised manner.
Thus, the inclusion criteria were:
athletes or healthy subjects who practise sports regularly;
VTFB or haptic FB;
heart rate (HR), joint angles, motor patterns, movement variability;
randomised clinical trials, randomised controlled trials, clinical trial, case reports, cohort study, and so on;
full text written in English, Dutch, German and French;
study subjects are adolescents or adults.
Exclusion criteria were:
non-healthy or pathological population and animals;
children (<10 years of age) and elderly (>65+);
other languages than those mentioned above;
meta-analysis, systematic reviews.
Experiments by Pressley and Ghatala indicated that children younger than 10 years of age are less accurately aware of FB results. Consequently, this set our lower age limit in our search strategy.16 The same goes for the upper limit in adults as has been shown by Rodrigue et al.17
The systematic screening of the articles was carried out in two different phases. First, all search results were screened based on title and abstract in a preliminary screening. If citations were considered potentially eligible and relevant, and if both reviewers (KW and TP) independently had agreed, full-text articles were obtained. In the second phase, full-text articles were evaluated. Detailed evaluation of the full-text publication was necessary for 47 articles. Disagreements between reviewers were resolved by consensus. If no consensus could be reached, a third reviewer (SV) would decide.
Data extraction
Two reviewers (KW and TP) independently performed data extraction by selecting relevant data and integrating it into two databases. The two databases were compared and integrated into a final extraction table. Again, disagreements were resolved through discussion between KW and TP, and in case of disagreement a third author (SV) was asked to make a final judgement. None of the authors were contacted for further information when information was missing or unclearly reported. The reason for the latter was that non-peer-reviewed unpublished information would, among others, hamper the systematic review process and could affect the quality of this paper as such.
Items extracted from the studies were study design, age and number of subjects included, study characteristics (including branch of sports or movement studied, setting and FB conditions), VTFB conditions (including number of vibrotactors, vibrotactor placement, vibrating frequency, stimuli duration, encoding signals and possible bandwidth used), type of outcome measures, and follow-up or retention and finally main results.
Risk of bias assessment
Two independent reviewers (KW and TP) independently assessed all included articles.
Suitability of randomisation and concealment of allocation, blinding of patients, healthcare providers, data collectors, and outcome assessors, and extent of loss to follow-up were determined by the two above-mentioned reviewers using the PEDro (Physiotherapy Evidence Database) scale. According to de Morton,18 the PEDro scale is a valid tool to measure the methodological quality of clinical trials.
The risk of bias was assessed by the same authors (KW and TP) who performed the systematic search of literature. The two authors performed the assessment of methodological quality independently. Findings were compared for agreement but in case of disagreement, a third judgement was in all cases obtained by one of the other coauthors (SV). Agreement between the two reviewers concerning the scoring of methodological quality was determined by the Cohen’s kappa. Cohen's kappa coefficient is a statistic measure for inter-rater agreement for qualitative items. In all cases, disagreements were resolved by discussion.
Scores were assigned based on meeting up with the criteria. A maximum possible score of 10 (low risk of bias) could be reached. Scores 6–10 were regarded as high-quality studies, 4–5 as fair quality and 3 or lower as poor quality. Studies with a risk of bias assessment score of 3 or less were considered poor and their contribution to results was weighted as half.
Evidence was graded according to EBRO (Evidence-Based Richtlijn[guideline]Ontwikkeling[development]) recommendations (table 3).19 EBRO is an initiative of the Dutch Cochrane Centre and the Dutch Institute for Healthcare Improvement (CBO, http://www.cbo.nl), a member of the Guidelines International Network.
EBRO classification of study results and recommendations: classification of the study results according to the level of evidence
Data analysis
Since the average quality of the studies was poor, a quantitative or meta-analysis was not feasible. We tried to analyse the data from the included studies in a fashion as has been proposed by Saw et al.20 However, because of the diversity in outcome parameters and in objective data, we have not been able to perform such analysis. Therefore, the results of the individual studies will be presented qualitatively.
Results
Study selection
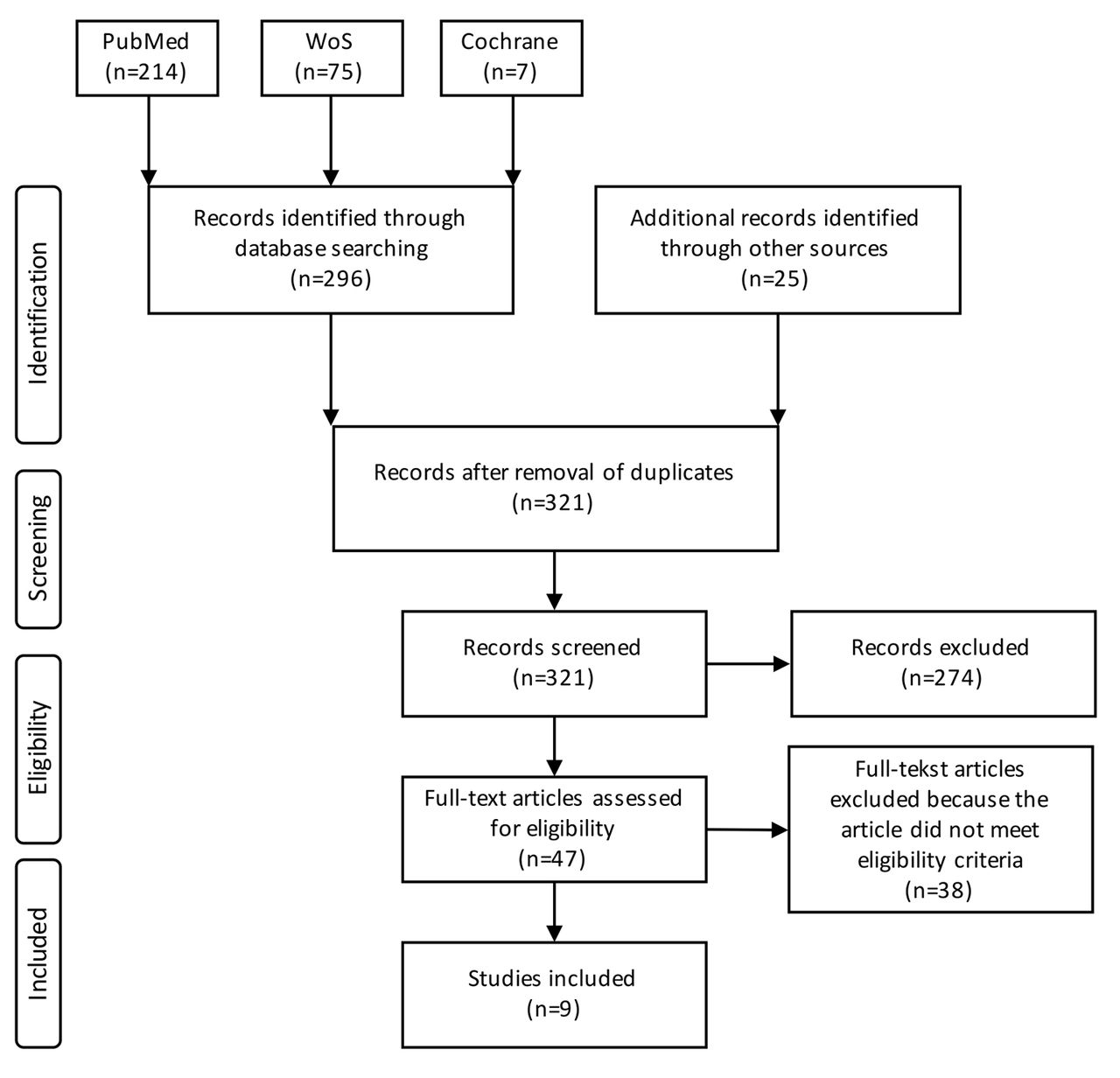
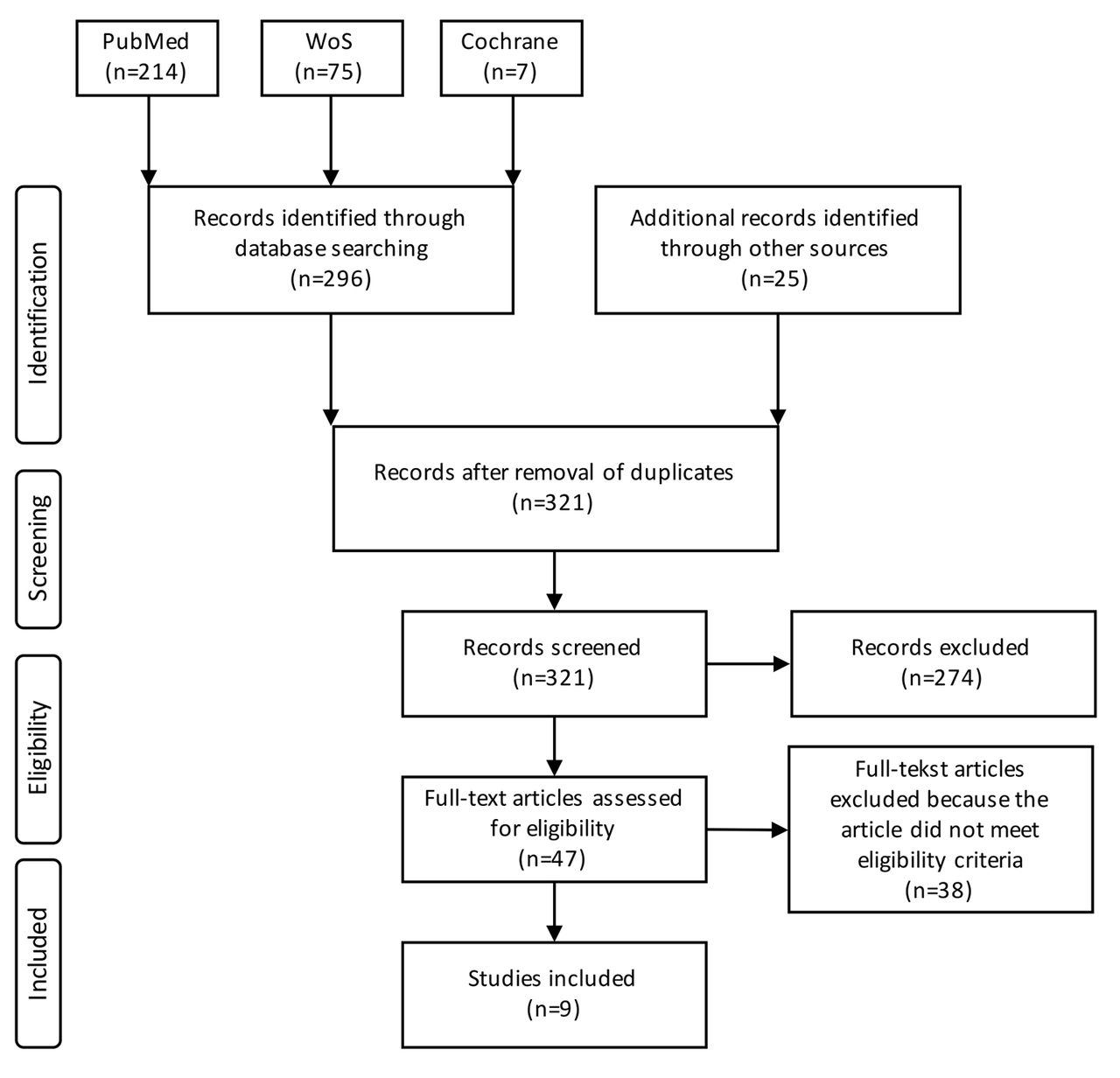
The PRISMA flow diagram (figure 1) summarises our study selection process. The initial search yielded 312 results, of which 16 duplicates were deleted, leaving a total of 296 studies. The manual search and repeated search yielded a total of 25 extra studies, making a total of 321 studies that were selected for screening. From the initial 296 studies, 274 were excluded based on title and abstract. Subsequently, 38 studies were excluded based on full-text screening. Of the 25 studies obtained by the manual and repeated search performed on 30 March 2017, a total of 14 were excluded based on title and abstract, and 6 on the full-text screening. Nine9 studies remained eligible for this review.
{kind=link}
Flow chart of the search strategy and study selection process. WOS, Web of Science.
The majority of the studies were excluded based on intervention and population, 63% and 20%, respectively. Twenty20 studies were excluded based on its study design and 24 based on outcome. Finally, three3 studies were excluded based on subject, eight8 studies on language and four4 studies were excluded based on age of the population. The majority of full-text exclusions were based on intervention.
Study characteristics
For each included study, the characteristics of data extraction are shown in table 4. All nine9 studies were published in English and could be designated as clinical study designs with VTFB as (one of) the intervention(s). The majority of the studies involved simple clinical trials21–25 whereas two studies26 27 involved a randomised controlled trial. Only one study could be designated as a randomised clinical trial.28
Data extraction table
The study of Spelmezan et al29 consists of one exploratory clinical trial with an open response paradigm and two clinical trials, one of which was performed in a reality-based context. Two studies investigated the effects of VTFB during rowing, two during snowboarding, one focused on treadmill running and two during a simple arm movement.26 28 One study investigated the effects of VTFB during an artistic skill.27
In two studies23 27 and in one of the trials of Spelmezan et al,29 the experiments were done in a real rather than a laboratory setting.
VTFB was compared with other FB modalities in the majority of studies, except for the study of Jansen et al24 and in the first two trials of Spelmezan et al.29 In the latter, VTFB was the only intervention. Outcome parameters differed between all studies. The main outcome parameters were joint angle error, root mean square error (RMSE), percentage of correct pattern recognition, reaction time and HR. Secondary and additional outcome parameters included temporal and spatial errors, timing errors and subjective description of perceived FB. In five studies,22 23 25 26 29 participants’ subjective impression on the FB modalities was assessed using a questionnaire or interview. Duration of the intervention, that is, number of training days, ranged from 1 to 4 days. Only four studies included a retention phase ranging from a 1-day retention test to a 1-week26 retention test.
Risk of bias within studies
Table 5 shows the methodological scoring and the assessment of the level of evidence.
Methodological scoring using the PEDro checklist and level of evidence of individual studies according to the CBO guidelines
We found a significant Cohen’s kappa agreement between the two authors who performed the reviewing concerning the scoring of methodological quality (κw=0.983; p<0.001). In 97% of the cases, both reviewers agreed. In all cases, disagreements were resolved by consensus, and if no consensus could be reached by the two authors (KW and TP) a third author was asked (SV). Each item contributes one point to the total PEDro score ranging from 0 to 10 points. Item 1 is not considered for the final score as it relates to external validity. Of the nine included studies, one had a final PEDro score of 1,21 three22 24 27 had a final score of 5, three25 26 28 had a final score of 6 and one23 had a final score of 7. The study of Spelmezan et al29 contains three trials of which one had a final score of 3, one had a final score of 4 and the third had a final score of 5. The overall quality of the included studies was fair to excellent, with the exception of the study of Eid et al (score 1)21 and the first trial of the Spelmezan et al’s study (score 3).29 Most studies were rated with a lower score based on blinding and randomisation.
Results of individual studies
The effects of VTFB in regulating optimal training intensity
Eid et al studied the effectiveness of VT stimuli to adjust exercise intensity.21 A within-subject design was used to compare ‘training with VTFB’ with no device and one with a Nike+ SportBand, using HR as the main outcome parameter. Unfortunately, only one subject was presented, but based on VTFB was shown to be more efficient to regulate HR, showing fewer fluctuations and resulting in a smooth change in method by taking bigger steps and breathing more efficiently. A faster HR recovery was found in the VTFB condition.
VTFB in learning single and multiple degrees of freedom of arm movements and initiating wrist rotations
Lieberman and Breazeal22 and Bark et al25 studied whether VTFB, based on the push protocol and sensory saltation, accelerates learning of single and multiple degrees of freedom (df) arm movements and reduces motion errors. Lieberman22 compared visual FB (n=20) with the combination of visual FB and VTFB (n=20). They found that the addition of VTFB to motor training induces significant change in performance: a reduction in real-time errors by up to 27% and an improvement of learning rate by up to 23%; with a steady state in learning errors by 27% over flexion joints. Subjects with the combination FB showed a significant higher level of correcting their motions in comparison to those without TCB. No significant loss of comfort through the addition of the wearable has been reported by the subjects.
In line with the studies of Lieberman et al,22 Bark et al25 used a within-subject design to compare visual FB with the combination of visual FB and VTFB. They reported that RMSE was significantly lower for the combination group (15.7°±6.5°) in comparison to the visual only group (17.1°±6.4°) for learning 1 df motion, but not for 2 or 3 df motions. In both groups, motion errors decreased over the 4 days of training but no significant effect on joint angle error was found during probe or retention.
Finally, Jansen et al studied whether VTFB was useful in initiating wrist rotations and which stimulus location provided the fastest reaction time.24 They concluded that an extrinsic reference frame in which the vibratory signal ‘pulls’ the hand in the desired direction is most intuitive.
Effectiveness of VTFB in a real sports context
Spelmezan et al conducted a within-subject study in snowboarding in which traditional verbal instructions in combination with VTFB were compared with traditional verbal FB only.23 Verbal instructions in the morning resulted in fewer mistakes compared with VTFB (p=0.044), whereas the opposite was true for trials in the afternoon (p=0.014). Verbal instructions outweighed VTFB when practising new tasks. Such results are in line with another study of Spelmezan et al in which snowboarders were provided with verbal FB instructions with or without VTFB.29 A faster response time has been found for VTFB in comparison with verbal FB (p=0.01).
The effectiveness of VTFB in learning a rowing task was studied by Van Erp et al and Sigrist et al.26 28 Van Erp et al28 compared direct positional VTFB with direct non-positional verbal FB and delayed non-positional verbal feedback. Neither group showed a learning effect. The VT group showed a significant (p<0.02) decrease in HR over tests but no difference was found between groups regarding timing and speed. Sigrist et al26 compared VTFB with verbal FB and auditory FB with a self-controlled terminal FB. Terminal self-controlled FB was found to be superior to all types of concurrent AFB. Furthermore, a significant decrease in RMSE, temporal error and error in velocity ratio was found from baseline to retention indicating that VTFB is effective in enhancing temporal aspects, rather than spatial aspects of movement. Again, a guidance effect could be found, that is, decrease in performance in non-FB conditions.30
Discussion
The aim of the present review was to provide a more detailed insight in the scientific literature concerning VTFB as a tool for sports performance enhancement. Only nine studies, based on the methodological criteria set, were eligible for this review. The quality of the studies was fair but the level of evidence was suboptimal. We conclude that, although VTFB has been shown to be effective under some conditions, evidence for its use as sports performance enhancement remains scarce and challenging.10 11 31
Summary of evidence
VTFB has been used in navigation,32 aviation33 and in automotive.34 It also found its way in virtual reality, gaming and in art.35 36 In healthcare, VTFB has been used as a navigation tool in the visually impaired subjects, as sensory substitution in the rehabilitation of patients with stroke, and in vestibular impaired subjects where it has been used as sensory augmentation.37 To the best of our knowledge, its use in sports practice is very limited. A reason for this is not easy to provide but the limited number of scientific studies in concordance with the broad range of outcome parameters and variability of the results in laboratory setting may be the major cause of the lack of use in sports practice.
Out of the nine studies eligible for final interpretation, only the studies of Spelmezan et al and van der Linden et al23 27 29 addressed VTFB in a reality-based context. For instance, van der Linden et al implemented the use of VTFB in real training situations for artists (violin players) whereas Spelmezan used snowboarders as study population. Subjects in the later study, however, stated that the VTFB instructions hindered normal movement because VT instructions were randomly provided in time and the placement on the body/limbs was reported to be frustrating. This might be one of the major reasons for athletes not to use VTFB devices on their body/limbs even if it might help them to improve performance. These findings are in contrast with the findings of Lieberman et al,22 who reported no loss of comfort during the application of VTFB. The use of devices that differ in size, weight and position could play a major role in the acceptance of VTFB in sports practice. Future studies should therefore be designed such that VTFB does not interfere with normal movement by providing VT instructions on suitable moments of VTFB.
There is some evidence that VTFB is effective in regulating exercise intensity during physical performance by keeping HR within aerobic limits.18 By applying VTFB, athletes could, based on their maximal HR, be guided by tactile information to perform at a less intense level and thus exercise more efficiently. Exercising with VTFB resulted in both short term and long term, in a decrease in HR.22 The athletes in their study who received TFB (ie, direct and positional) showed a decreased HR in the post-test as compared with the pretest whereas the athletes who did not get TFB showed an increase in HR. A plausible explanation for this HR effect was that athletes without VTFB were less efficient in maintaining motor skills and more than necessary adjustments in motor control were necessary. Therefore, it is reasonable to assume that VTFB is effective in improving temporal movement aspects, but not spatial errors.26 These findings support the results of previous studies.38 39 Lastly, there is moderate evidence that VTFB instructions could support the athlete in practising and fine-tuning a previously learnt movement. A second explanation for an over-the-day decrease in HR is that VTFB is less mental demanding.25 To date, no studies are present that support this idea.
Some studies used joint angle errors as the main outcome parameter.19 22 This is somewhat surprising since joint angle is not necessarily the most important outcome parameter for motor performance, and as such, athletic performance. Moreover, during a motor task, several joint angles should be taken into account, that when applying VTFB should provide simultaneous and multiple VTFB signals.23 25 27 The major drawback, however, of some studies using VTFB as error signal is the lack of implementing an order or sequence in signals.22 28 Subjects are continuously provided with FB signals which lead to overcorrection of motor tasks/movements. Only a few scientific studies that used VTFB for motor task correction used more accurate and timed signals.21 25–27
Limitations of the current review
The quality and diversity of the studies made it impossible for us to do quantitative analysis of the results. The risk of bias of individual studies was overall moderate to fair and because randomisation was inadequate or lacking in the majority of trials, level of evidence was moderate to weak. Furthermore, poor and incomplete reporting of study designs, patient populations and interventions made the interpretation and synthesis of the included studies much more difficult and may have contributed to publication bias. Therefore, generalisation of the results to athletes is difficult.
Finally, the main limitation of this study is that the context of VTFB and comparison between different FB modalities and outcome measures for performance were not the same across the studies, making a direct comparison between the outcome of these studies difficult.
Conclusions
Our review suggests that VTFB, which has been used as application in medical and non-medical-based contexts (ie, patient groups, automotive, and so on), lacks scientific support for enhancement of sports performance outcomes. The inconsistency of findings and moderate level of support, as reported in the present study, hardly provide evidence to support the suspected role. More basic and applied studies are necessary to warrant its use in a sports context.
References
Footnotes
Contributors The study was planned by EvB, SV and ST. KW and TP conducted the literature search whereas SV was used as author in case of disagreements during selection. EvB and SV wrote the initial draft of the manuscript. EvB, SV, WS and ST discussed and revised the manuscript together and gave final approval for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.