Article Text

Abstract
Background A thorough knowledge of the epidemiology and severity of injuries and illness in youth female elite sports is lacking due to the methodological challenges involved in recording them. In this study, the prevalence and incidence of injuries and illness are assessed among youth female elite athletes. Instead of solely focusing on time-loss injuries, our study included all substantial and non-substantial health problems (ie, injuries, mental problems and illnesses).
Methods Sixty young elite Dutch female athletes (age: 16.6 years (SD: 2.3), weight: 58.3 kg (SD: 15.1), height: 154.1 cm (SD: 44.2)) participating in soccer (n=23), basketball (n=22) and gymnastic (n=15) talent development programmes were prospectively followed during one season (September 2014 to April 2015). To collect health problem data, all athletes completed the Oslo Sports Trauma Research Center Questionnaire on Health Problems every other week. Main outcome measures were average prevalence of injury and incidence density of injury.
Results At any given time, 47.9% of the athletes reported an injury (95% CI 43.6% to 52.6%) and 9.1% reported an illness (95% CI 5.1 to 19.0). The average injury incidence density was 8.6 per 1000 hours of athlete exposure. The average number of self-reported injuries per athlete per season was significantly higher in soccer athletes (4.3±2.7) than in basketball athletes (2.6±2.0) (p=0.03) and not significantly higher than in the gymnastic squad. The knee and the ankle were two of the most common injury locations for all squads. Knee injuries in basketball and soccer and heel injuries in the gymnastic squad had the highest impact on sports participation.
Conclusion High prevalence of self-reported injuries among talented female athletes suggests that future efforts towards their prevention are warranted.
- Young
- Female
- Athlete
- Injuries
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
This paper reports an injury incidence of 8.6 per 1000 hours of athlete exposure, an injury prevalence of 48%, using a new injury recording method.
The new injury recording method captures a complete picture of the burden of health complaints in young female elite athletes.
The knee and the ankle were two of the three most common injury locations for all squads.
Introduction
Overuse injuries, defined as injuries without a specific, identifiable event responsible for onset, may be a substantial problem in sports.1 Young athletes involved in elite talent development programmes are thought to have a particularly high risk of both overuse2 3 and acute injuries.4 In this group, high training volumes and overscheduling have been suggested to represent risk factors for overuse injury.5–7 A thorough knowledge of the epidemiology of overuse injuries in youth sports is needed to target injury risk factors, and thereby prevent injury-related talent development stagnation and increase the return on investment in elite youth sports programmes.8 Baxter-Jones et al studied 64 elite young soccer and 119 elite young gymnast athletes and found a prevalence of overuse injuries of 15% for soccer and 33% for gymnasts.9 Yang et al found an overuse injury incidence of 2.0 per 1000 hours of athlete exposure among National Collegiate Athletic Association Division I basketball athletes.10 Although these studies indicate that overuse injuries in young athletes are common, they may underestimate the full extent of the problem. This is because most studies define injury as time loss from participation, whereas many athletes with overuse injuries continue to participate despite pain and reduced performance.1 11 When time loss definitions are used, about 90% of overuse injuries appear to be missed.
Clarsen et al 1 proposed a new surveillance method designed to address the methodological challenges involved in overuse injury registration,1 which was later adapted to record all types of health problems, including overuse injuries, acute injuries and illnesses.12 Using this method, athletes periodically report injury and illness symptoms and consequences using an electronic questionnaire. In comparison with standard methods of injury registration, this approach may provide greater information on true consequences of injury over time.1 7 13 Although some athletic groups have been investigated using this new method, little is known about young talented female athletes, who are suggested to be a high-risk population.6 The aim of this study was to use this new method and gain more insight into the injuries and illnesses of young elite female athletes by recording injury and illness prospectively throughout a full season.
Materials and methods
Subjects
We invited all athletes (n=60, mean age: 16.6, SD=2.3 years) involved in the soccer (n=23), basketball (n=22) and gymnastics (n=15) squads of the Dutch national high-performance programme of the Centre for Top Sport and Education (CTO) Amsterdam, the Netherlands. To qualify for the programme, athletes must be nominated by their national federations and be competing at the national or international level in their sport. About 180 athletes in eight different sports are currently supported by CTO Amsterdam. The teams included in the study were a convenience sample, and all athletes and their parents were informed about the procedure and provided written informed consent. The study was approved by the Medical Ethics Committee of the Academic Medical Centre Amsterdam.
Procedures
During the preseason period (August 2014), the baseline characteristics were recorded by the medical staff of the CTO Amsterdam, including age, height and body weight. All athletes were prospectively followed during the entire 2014/2015 competitive season. The season runs from August 18 until April 26 for the soccer team (36 weeks) and from September 28 until April 26 (30 weeks) for the basketball and gymnastic teams. Every other week, all athletes were asked to complete questionnaires by using a web-based system (Monitoring Athletes, Trainers, Coaches and Health (MATCH) professionals). MATCH is developed by the Amsterdam University of Applied Sciences and used to monitor stress and recovery. This system consists of different questionnaires, including a Dutch translation of the Oslo Sports Trauma Research Center Questionnaire on Health Problems.12 This version was a forward–backwards translation from the original Norwegian version.7 Every fortnight on Sunday, athletes automatically received a link to the questionnaire by e-mail. If the athlete did not respond to the questionnaire within 3 days, a reminder by e-mail was sent. After 5 days of non-response, the coach was notified by the research team about uncompleted questionnaires. Subsequently, the coach asked the athletes personally to complete the questionnaire.
Illness and injury registration
The questionnaire consisted of four key questions on the consequences of health problems on sport participation, training volume and sport performance, as well as the degree to which the athlete perceived symptoms. Each item is scored with a 4-point or 5-point scale, ranging from 0 (no problem, no reduction, no effect and no symptoms, respectively) to 25 (cannot participate at all or severe symptoms). The severity of a health problem was calculated on a scale of 0–100 by summing the score of the four key questions, according to the method proposed by Clarsen et al.1 If the severity score was 0, the questionnaire was finished for that 2-week period. However, if the severity score was higher than 0, a health problem was registered, and if the athlete selected option 2 or 3 in either key question 2 or 3, a substantial health problem was registered.12 Next, the athlete was asked whether she was referring to an injury or an illness. In case of an illness, no further information about the illness was registered. In case of an injury, the athlete was automatically directed to an injury registration form based on an international consensus statement on injury surveillance methodology for football14 to collect further details (eg, location, history and acute or overuse onset). At the end of this injury form, the athlete was asked if the injury was mentioned in the questionnaire of the previous biweekly period. If the athlete stated that the injury was previously mentioned, the severity score was added to the severity score of the previously mentioned injury to calculate the cumulative severity score for each case. Only one injury or illness could be registered. Finally, the athlete reported her training and match exposure minutes over the last 2 weeks.
Statistical analysis
All statistical procedures were performed using SPSS V.22. Baseline characteristics, measured as continuous variables, were expressed as mean and SD. Body mass index was calculated from athletes' baseline height and weight. The prevalence of all health problems (eg, illness, overuse injuries and acute injuries) was calculated for each biweekly period by dividing the number of reported problems by the number of respondents for that specific period. The prevalence of substantial problems (ie, a moderate or major reduction in sport activity and/or performance) was calculated separately.12 Injury incidence density (IID) was calculated as the number of new injuries per 1000 hours of sport participation. Injuries that were present at the start of the study were not taken into account. A Poisson model was used to obtain 95% CI around the IID.
To calculate differences in injury characteristics between sports, independent samples t-tests were applied for the normally distributed continuous parameter (eg, reported injuries per athlete). p Values were two-tailed, and significance level was set at p<0.05. To calculate the relative impact of injuries between the various sporting groups, a cumulative severity score was calculated for each anatomical area for each sporting group by summing athletes’ severity score over the total season, adjusted for differing group sizes and response rate.15 An assessment of scores of the relative impact of injuries was used to compare each anatomical area within and between sports.
Results
Response and baseline characteristics
Fifty-nine of the 60 athletes enrolled in the study completed the entire follow-up period. The baseline characteristics of these athletes are shown in table 1. One athlete dropped out the talent development programme during the season. In total, 970 questionnaires were sent to the athletes and 919 were completed, resulting in a response rate of 95%.
Baseline characteristics shown as mean (±SD)
Prevalence of health problems
During the season, a health problem was reported in 556 of the 919 (60.5%) questionnaires. Of these, 440 were caused by an injury (79.1%), 84 by an illness (15.1%) and 32 were unclassified (5.8%). Of all reported health problems, a total of 282 (30.7%) were classified as substantial. A majority of the substantial health problems were injury-related (n=232, 82.3%). As shown in table 2, the average biweekly prevalence of substantial injury problems in the gymnastic squad is significantly lower than in both the soccer and basketball squads.
Average biweekly prevalence of all health problems and of substantial problems, prevalence given as the biweekly per cent of injured players in the entire population (95% CI)
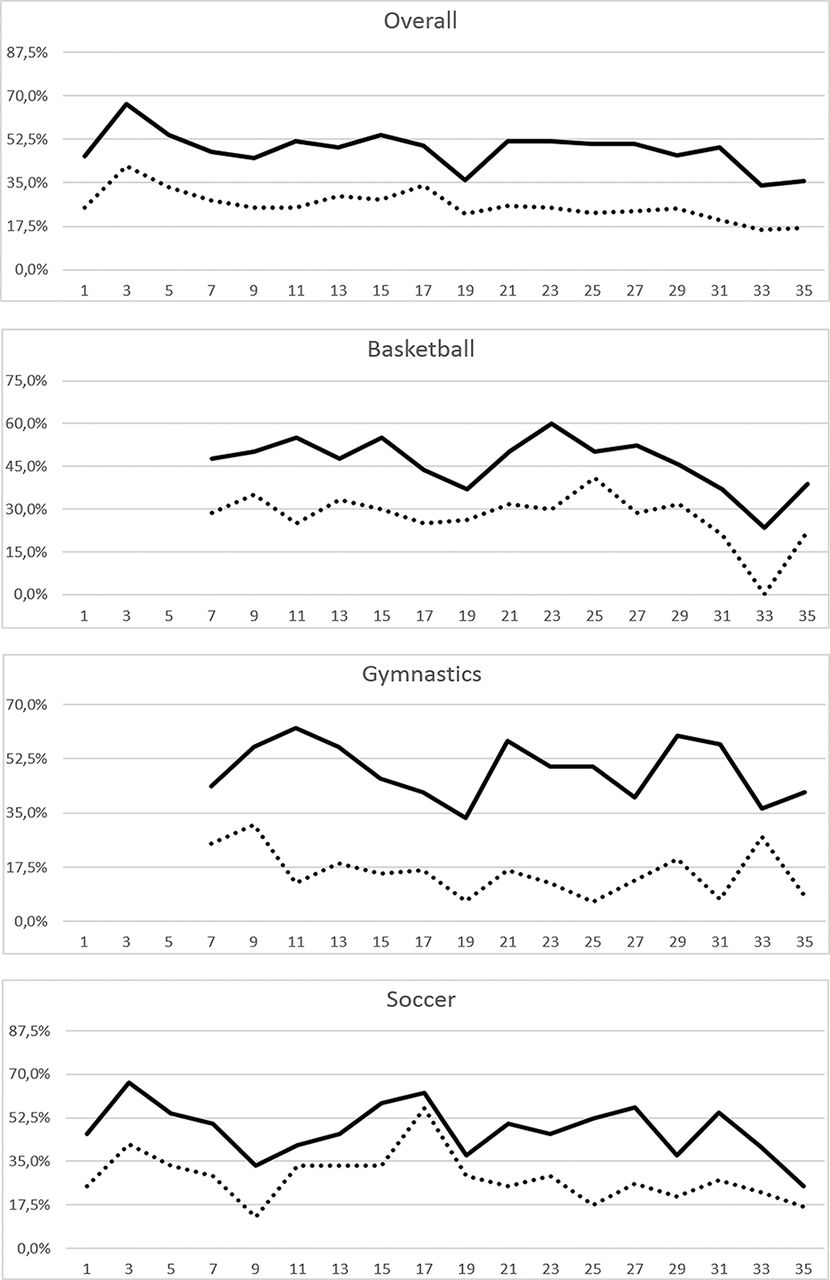
There was no significant difference on the prevalence of injuries between the biweekly periods. Figure 1 shows that there may be a trend indicating that the injury prevalence was higher at the start of the season and during the winter break (weeks 17–19).

Biweekly prevalence of injuries during the 36-week follow-up period. Full line represents all reported injuries, whereas dotted line represents substantial injuries.
Characteristics of health problems
Of all 556 reported health problems, 308 were unique (eg, not mentioned in the previous questionnaire). Of these, 192 were classified as an injury (62.3%), 84 as illness (27.3%) and 32 were unclassified health problems (10.4%).
Illnesses
A total of 84 illnesses were reported by 44 athletes (27% of all health problems), which equates to an average number of reported illnesses per athlete of 1.4 during the season (soccer: 1.6, basketball: 1.5 and gymnastics: 1.0).
Injuries
Sixty-two per cent of all health problems were injuries (n=192). Four athletes (6.7%) did not report any injury during the season, 10 athletes (16.7%) reported one injury, 12 athletes (20%) reported two injuries and 46 athletes (76.7%) reported three or more injuries. The average biweekly severity score of injuries was 32.0±20.3, with a range of 86.4 and a median of 28. No significant differences of the average biweekly severity score were found between sports (table 3).
Average, mean and range of the biweekly severity score of injuries per sport
As shown in figure 2, the average number of reported injuries per athlete was significantly higher in soccer athletes (4.3±2.7) than in basketball (2.6±2.0) (p=0.03) athletes. Furthermore, a total of 22 425 hours of athletic exposures were reported during the entire season (19 903 training hours and 2523 competition hours). This equates to an overall IID of 8.6 injuries per 1000 hours (95% CI 7.4 to 9.9). Injury incidence in the soccer squad (17.1 injuries per 1000 hours; 95% CI 14.0 to 21.0) was significantly higher than in the basketball squad (6.3 injuries per 1000 hours; 95% CI 4.9 to 8.2) and the gymnastic squad (5.2 injuries per 1000 hours; 95% CI 3.9 to 7.1) (table 4).

The average number of injuries reported per player. *Significantly different from the basketball squad (p< 0.05%).
Injury incidence density characteristics per sport, % (95% CI)
The most common acute injury locations were the ankle (n=36; 18.8%), knee (n=31; 16.1%) and the posterior upper leg (n=24; 12.5%), whereas the most common overuse injury locations were the knee (n=12; 20.3%), posterior upper leg (n=7; 11.9%), lower back (n=5; 8.5%) and the heel (n=5; 8.5%). Table 5 shows the most common injury locations for each sport.
Total number of injuries and acute injuries per location overall and per sport (%)
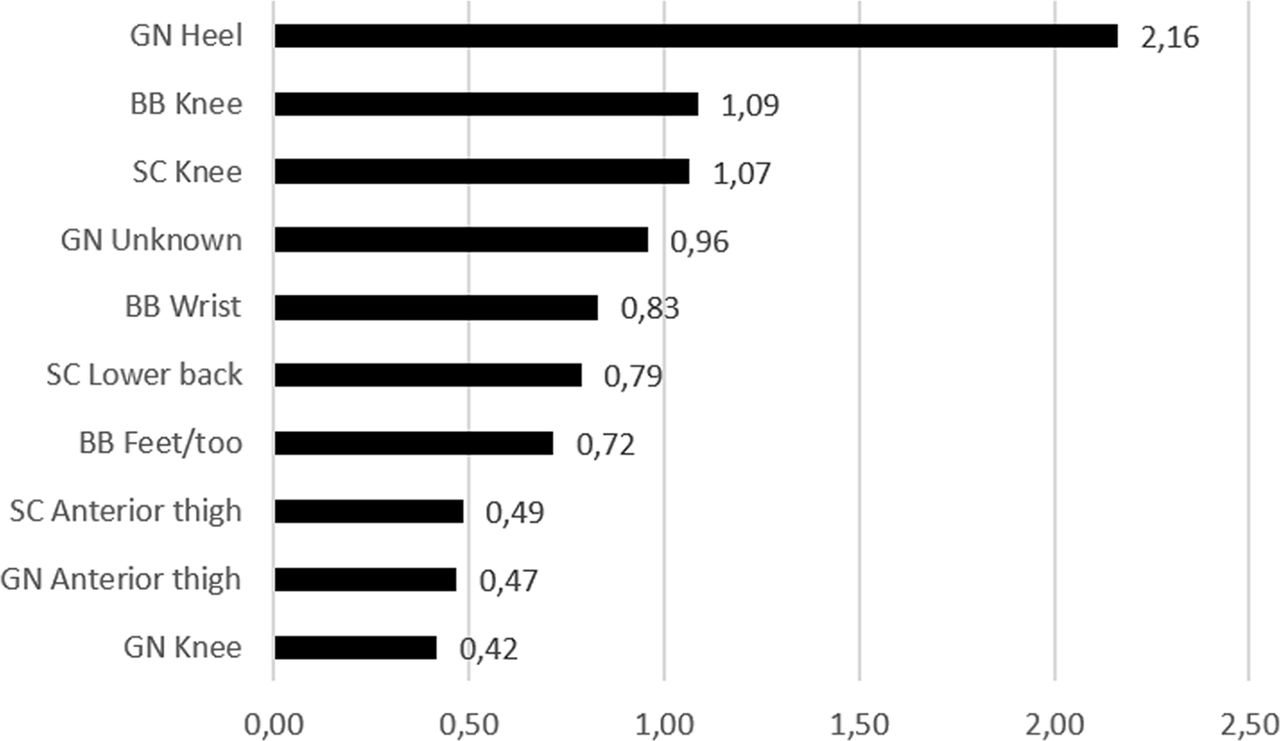
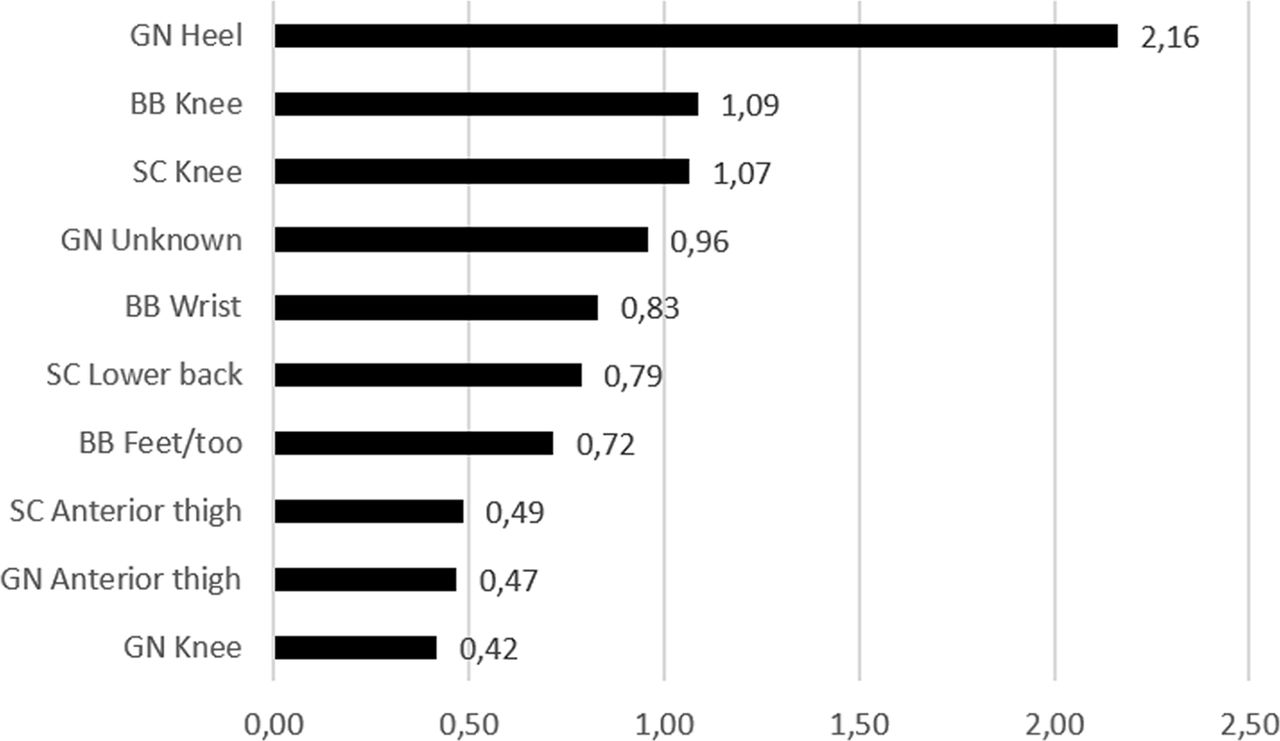
Relative impact of injuries
Figure 3 shows the top 10 of the relative impact of injuries in each anatomical area for each sport, based on the adjusted cumulative severity score over the total season. As shown in the figure, heel injuries among gymnasts, knee injuries among basketball athletes and knee injuries among soccer athletes had the greatest impact on athletes’ performance and participation.
{kind=link}
{kind=link}
{kind=link}
Top 10 of the relative impact of injuries shown as the adjusted cumulative severity score for each group (arbitrary units). BB, basketball; GN, gymnastics; SC, soccer.
Discussion
The main finding of this study was that the average biweekly prevalence of health problems was 60.5% (95% CI 55.7 to 65.7). Furthermore, injuries are the main problem, with an average biweekly prevalence of 47.9% (95% CI 43.6 to 52.6). This is higher than the prevalence of injuries found in Norwegian Olympic and Paralympic adult athletes using similar data collection methods.12 This might be explained by several factors. First, the athletes in our study are adolescents. The musculoskeletal system of adolescents is not fully developed, which may increase the risk of injuries.16–18 This is underlined by the adolescent growth sport-induced alterations in limb length, body mass and moments of inertia, which may affect coordination and movement patterns. These physical alterations may play a role in the increased risk of injuries.17 19–24 Second, our participants are all female. It is well documented that women are at higher injury risk compared with men for many injury types.25–28 Some studies attribute the increased injury rate to gender-based anatomical differences, such as joint laxity, bone structures and limb alignment.27 Other studies have suggested that female hormones are directly involved in female injury rates.29–31 Especially after the onset of maturation, differences in circadian sex hormones are attributable to imbalances in neuromuscular control, which may cause an increased injury risk in pubertal women.32–34
In the soccer squad, we found an incidence of 17.1 injuries per 1000 athletic exposure (95% CI 14.0 to 21.0), which is significantly higher than the incidence found in the study of young elite female soccer players (6.4; 95% CI 5.9 to 6.9).35 Furthermore, we found an incidence of 5.2 (95% CI 3.9 to 7.1) injuries per 1000 athletic exposure in the gymnastic squad, which is higher than the injury incidence of 2.9 found in the study of young elite female gymnasts.36 In the basketball squad, we found an injury incidence of 6.3 (95% CI 4.9 to 8.2), which is significantly lower than the injury incidence of 13.9 (95% CI 11.2 to 16.7) in the study of female basketball players in Flanders’ national and regional competition.37 The differences in the injury incidence in the soccer and gymnastic squads can be explained by the use of different injury definitions. Both studies used the consensus statement for injury surveillance methods in football.14 Our results substantiate this suggestion. The differences in injury incidence may be even greater, as it is not clear whether the studies excluded injuries that were present at the start of the study. Clarsen et al showed that 44% of identified injuries in their study would have been excluded in incidence calculation for this reason.1 Furthermore, as suggested by Clarsen et al, the injury registration method used in our study can identify more than 10 times as many cases than this standard method.1 Apart from a possible overestimation of injury incidence, the lower injury incidence in the basketball squad may be explained by the different competing levels the subjects were involved in. There is some scientific evidence that athletes performing at international levels are at lower injury risk than athletes performing at the national level.38 39 Internationals have more sports medicine and sports science and coaching resources working in a coordinated fashion, resulting in a better understanding of injury risks and injury prevention, which may result in a lower injury risk. Furthermore, the higher injury incidence found by Cumps et al is also a result of the injury definition that was used, as it included serious, moderate and minor injuries. This definition is similar to the definition used in this study.
Although injury incidence differed from other studies, the majority of injury locations in our study were in agreement with other studies. The majority of injuries were located at the ankle and knee for all squads. Thigh injuries supplemented the top three injury list in the soccer and basketball squads, whereas it was the foot in the gymnastic squad. These results are similar to other studies on adult 26 40–42and young35 36 female elite athletes. The relatively high average prevalence of heel injuries in gymnastics and knee injuries in soccer and basketball supports the fact that the foot (gymnastics) and the knee (soccer and basketball) are the most commonly affected areas.26 35 36 40–42 The relative average prevalence of heel injuries in the gymnastic squad was at least double of the prevalence of all injuries in the other squads. This indicates that gymnastic prevention programmes should focus on heel injuries. Soccer and basketball squads should focus on the prevention of knee problems, for example with the 11+ injury prevention programme43 and the ankle prevention programme, freely available as an interactive app (‘Strengthen Your Ankle’ translated in Dutch as: ‘Versterk je enkel’; available for iOS and Android).44
One major strength of this study is the response rate of the biweekly questionnaire of 95%. There are several reasons that might explain the high response rate. For example, we used adequate guidance during the season to increase the involvement of athletes and coaches. In addition, we used MATCH to give coaches visual feedback of the collected data to improve their commitment to this study. We recommend to use this approach when using similar registration methods.
A unique aspect of this study is that all participants were active in a professional sports talented programme for female athletes. A thorough investigation on the severity and magnitude of self-reported health problems in this group is missing. Although the sample size is relatively small, the presented data are accurately measured and can be seen as a thorough representation of the real life.
In this study, we used athlete-reported outcomes. This methodology exposes a potential limitation. Most talented athletes lack medical expertise. Therefore, we were unable to record specific diagnoses for the reported injuries and profound onset mechanisms. We recommend that future studies include a follow-up from the medical staff during the data collection period to gain more insight in the injury type and aetiology. As the focus of this study was to reveal the magnitude and severity of self-reported health problems, we chose to restrict athletes to report only injury locations. However, future studies may better target a specific injury prevention programme for common injuries, when specific medical data of injuries are available.45 Moreover, training and match exposure may be difficult to be defined by the athletes as time on the pitch may not equal exposure time. Future studies can include coaches in defining training and match exposure.
The second limitation is that athletes recorded a questionnaire every other week, instead of every week, as proposed by Clarsen et al.1 This may have led to a slight underestimation of health problems, as athletes may forget a health problem that occurred 2 weeks earlier. In addition, the used methodology implies that the problem’s severity is constant between two recordings. It is, therefore, unclear at what specific day the severity of the health problem was the highest. However, due to this method, the athletes were not overloaded with questionnaires every week, leading to a very high compliance. Furthermore, we believe that athletes are able to provide reliable information about a health problem from prior to 2 weeks. Clarsen et al showed that the average prevalence and severity of health problems were not affected by the sampling frequency of up to a frequency of one sample every 4 weeks.1
Third, the injury definition is very broad. Therefore, some normal aches and pains being part of the sport (eg, delayed onset muscle soreness) may be recorded as an injury. To prevent overestimation of injury prevalence, substantial health problems (ie, reduction in activity and sports performance) were included in this study, which were also very high. Nevertheless, monitoring the severity of normal aches and pains over time may reveal worsening problems. Adequate preventive interventions targeting these problems may prevent athletes to cease participation in training and competition.
Moreover, the data in this study are based on single teams. These teams are not necessarily representative of all young elite female athletes in these sports. Nevertheless, the results in this study identify the extent and severity of the sports injury problem, which can be used to identify risk factors and reduce future risks of these particular injuries in general.
Finally, in this study, only basic data were collected, but as the focus of this study was injury, no attempt was made to record illness symptoms or classify illness types. Nevertheless, our data are sufficient to conclude that illness rates were low in these athletes (normal population estimates of 2–3 respiratory tract infections per year) and injuries represent the major burden.
References
Footnotes
Funding This work was supported by National Association of Applied Sciences SIA Grant Number 2013-15-12P.
Competing interests None declared.
Ethics approval The Medical Ethics Committee of the Academic Medical Centre (AMC) Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed