Article Text

Abstract
The shoulder, specifically the glenohumeral joint, by virtue of its anatomical characteristics and biomechanics confers a large range of movement, which ultimately results in a joint that is inherently prone to becoming unstable. The incidence of acute traumatic shoulder dislocation varies within the sporting environment, commonly occurring following direct trauma. Anterior dislocations account for nearly 90% of all dislocations. While most are referred and managed in the emergency department, pitch-side relocation by experienced clinicians does occur prior to referral. The aim of this study was to delineate a guideline specifically for the pitch-side management of this common injury. A literature search of PubMed and Medline using the keywords ‘prehospital’, ‘pitch-side’, ‘shoulder dislocation’ and ‘reduction’ or ‘relocation technique’ was performed, and the available literature was reviewed and collated. Articles focusing on reduction techniques were then reviewed, with particular consideration on their applicability to a pitch-side setting. While studies exist that compare and contrast examination and reduction techniques, most are based in a hospital setting. To date, there is no standardised management protocol published for the initial management of an anterior dislocated shoulder in a pitch-side setting. This article addresses this discrepancy and proposes a structured, algorithmic approach to the pitch-side management of a shoulder dislocation. The article addresses factors to consider in a pitch-side setting, suitable techniques and postreduction care. While a systematic approach has been delineated in this article, we recommend those pitch-side medical practitioners who provide this form of support should have attended appropriate training and ensure adequate malpractice cover.
- Shoulder
- Injuries
- Sports medicine
- Trauma
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The shoulder, specifically the glenohumeral joint, by virtue of its anatomical characteristics and biomechanics is one of the most unstable joints within the body.1 The bony architecture confers a large range of movement, but ultimately lacks inherent stability. It is therefore one of the most commonly dislocated joints in the body, with an incidence density rate (IDR) estimated to be between 23.9 and 26.9 per 100 000 person-years within the general population.2 3 Research that focused on smaller, high-risk subpopulations such as athletes and military personnel showed a significant variation in the IDR ranging from 8.2 to 26.2 per 100 000 person-years.4 5 Approximately 75% of first-time glenohumeral dislocations are sustained during some form of sporting activity.6
A 3-year review by Cutts et al 7 analysing the age spectrum of patients who sustained shoulder dislocations identified a bimodal distribution, with the bulk of patients being young adults who sustained high-energy injuries to their shoulder. The second cohort of patients was much older, and was injured with a lower level of violence. Interestingly, the risk of recurrence correlated significantly to the mechanism of injury, that is, a higher impact, and the age of the patient at presentation—with the group 16 to 30 years old being at particular high risk.7 8
The incidence of acute traumatic shoulder dislocation varies between different sports. Most occur via direct trauma, such as a collision or a fall onto an outstretched arm. The most common position for an anterior shoulder dislocation to occur is while the arm is held in abduction and external rotation9 resulting in anterior leverage of the humeral head.10 Certain sports such as rugby, gymnastics, swimming, wrestling and basketball often rely on this anatomical orientation of the arm during their active sports participation, and therefore the very nature of these sports predisposes athletes to shoulder dislocations.
While the majority of shoulder dislocations are anterior, accounting for up to 90% of all dislocations,11 it is important to identify patients with multidirectional instability prior to any intervention. Athletes in particular cannot be divided into clear-cut groups, that is, unidirectional versus multidirectional instability.12 This is because they are often lax to begin with and they then subject their shoulder to repetitive microtrauma on a daily basis.12 In the long run, this affects joint congruency. Any trauma sustained after may result in a superimposed injury. Therefore, to manage an athlete pitch-side on the presumption of an anterior dislocation without clinical correlation may lead to unforeseen complications.
Assessing an athlete with a significant limb injury (such as a dislocated shoulder) is quite daunting in a prehospital setting. Often, it would be tempting to immobilise the limb and refer the athlete to the nearest emergency Department. However, the easiest option may not necessarily be the right option at that point, especially if performing an early intervention can prevent complications down the line. For example, in a recent Inter-University football match, a player landed awkwardly on his shoulder following a mid-air collision. Following an uneventful primary survey, the shoulder was examined, revealing loss of normal shoulder contour with the arm held abducted and internally rotated. The humeral head was palpable anteriorly and a diagnosis of an anterior shoulder dislocation was made. The radial pulse was easily palpable and there were no signs of neurovascular compromise. The initial assessment was followed by a myriad of subsequent questions—is relocation appropriate? In the absence of sedation, would Entonox suffice? What technique is appropriate? Is additional assistance required? Is there a fracture that may displace while attempting relocation? A decision was made to attempt relocation and fortunately, using a single-person external rotation method of the Leidelmeyer technique, with the athlete supine, the shoulder was put back into joint.
The authors being both in-hospital and pitch-side emergency medical practitioners recognise the variation in assessment and management of injuries between these two environments. This highlights the need for a designated, systematic protocol while assessing a shoulder dislocation on a pitch-side setting. Doing so would help delineate cases that would be appropriate for pitch-side interventions against those that may require further investigations prior to any intervention. In addition to this, highlighting the most appropriate pitch-side relocation technique to a medical practitioner would maximise their chance of success on the first attempt. Furthermore, delineating an evidence-based guideline that could be safely and systematically applied in a prehospital setting would be a welcomed addition to pitch-side injury protocols.
Discussion
A literature search of PubMed and Medline using keywords ‘prehospital’ or ‘pitch-side’ and ‘shoulder dislocation’ and ‘reduction’ or ‘relocation technique’ was performed. While studies exist that compare examination and reduction techniques, most were based in a hospital setting. The literature search revealed no results encompassing management of shoulder reduction on a pitch-side setting. Similarly, a review of the guidelines derived from the UK National Institute for Health and Care Excellence (NICE), US guidelines through the American College of Sports Medicine (ACSM) and the American Academy of Orthopaedic Surgeons (AAOS) revealed no specific guidelines pertaining to pitch-side management for shoulder dislocations. Therefore, at present, to the best of our knowledge, there are no standardised management protocols for the initial management of this common injury.13–15 This article proposes to address this discrepancy using a structured, systematic approach to the pitch-side management of a shoulder dislocation.
Shoulder stability
It is well established that the humeral head articulates with the glenoid fossa with less than one-third of its surface area normally in contact, thus compromising stability for an increased range of movement. The shoulder therefore relies on a complex array of static and dynamic joint components to provide stability.16–18
Static stabilisation within the shoulder is collectively provided by the bony congruency of the joint surfaces, the glenoid labrum, the joint capsule and ligaments, and the negative intra-articular pressure generated within the joint.1 11 19 The orientation of the articular surface of the scapula relative to the glenohumeral head provides resistance against postero-inferior instability.20 21 Although the glenoid fossa is relatively shallow, the presence of the glenoid labrum increases the humeral contact area from 25% to about 35%.22 This fibrocartilaginous structure also increases the fossa depth and provides an attachment point for the glenohumeral ligaments. In the absence of the labrum, the forces required to dislocate the head are reduced by 20%, substantiating its role as a static stabiliser.18 20 The joint capsule itself exhibits inherent laxity thereby allowing for a wide range of motion. However, in extremes of motion, it becomes taut—allowing it to act as a static stabiliser.17 Several ligaments are involved in static stability including the superior, middle and inferior glenohumeral ligaments as well as the coracohumeral ligament.18 The superior glenohumeral ligament and the coracohumeral ligament have been shown to provide resistance to posterior and inferior instability. This occurs most efficiently when the humerus is adducted and externally rotated. When the arm is held abducted at 45°, the middle glenohumeral ligament acts as the primary restraint to anterior instability.23 When abduction increases to 90°, the anterior band of the inferior glenohumeral ligament takes over this role. The posterior stabilising effect of the posterior band of the inferior glenohumeral ligament also occurs most effectively at this same anatomical orientation of 90° humeral abduction.18 24 The negative intra-articular pressure within the glenohumeral joint generates a ‘vacuum’ effect which acts as a stabiliser, primarily against inferior instability.25
Dynamic stabilisation occurs via the synergistic function of the rotator cuff muscles, the long head of the biceps and the scapular-stabilising muscles. The rotator cuff muscles, that is, teres minor, subscapularis, infraspinatus and supraspinatus are positioned to exert a ‘concavity-compression’ force that provides stability during mid range of motion when the capsule and ligaments are lax.26 These forces press and centralise the head within the fossa resisting translation. Coordinated muscle contraction itself also plays a crucial role in maintaining stability.16 Due to intertwining of the joint capsule with the rotator cuff muscles at their distal insertion, it is thought that the capsule and ligaments are tensioned during active contraction of the muscles—therefore acting as a dynamic musculoskeletal stabiliser.27 The long head of the biceps muscle resists excessive external rotation, thereby contributing to anterior stability.28 Optimal scapula function is critical for glenohumeral joint stability. The scapular-stabilising muscles (trapezius, serratus anterior, pectoralis minor, rhomboids major and minor and latissimus dorsi) stabilise the scapula during joint movement as well as orient the scapula to the glenohumeral head for optimal static and dynamic stability.29 Ligamentous neurological feedback that mediates joint position and muscular reflex feedback is referred to as proprioception. Joint instability is often associated with decreased proprioception, but does appear to be restored following surgical correction of this instability.30
Instability in an athlete may occur from three primary aetiologies: major trauma, chronic repetitive microtrauma or an underlying congenital abnormality.31 Anterior instability may result from either a tear in the anteroinferior portion of the joint capsule (involving the anterior static stabilisers) or more commonly from anteroinferior labral detachment—known as a Bankart lesion. A Bankart lesion is the most commonly recognised traumatic pathological lesion of anterior instability.32 Concomitant fracture of the posterolateral aspect of the head (Hill-Sachs defect) may also occur during an anterior dislocation. Other factors that may contribute to anterior instability include superior-labral-anterior-posterior lesions, tear to the rotator cuff muscles or humeral avulsion of the ligamentous stabilisers.18
While the factors that affect posterior and inferior instability are indeed important, they exceed the scope of this article and have thus not been included. Additionally, posterior dislocation (identified by an inability to externally rotate the shoulder combined with posterior fullness just below the scapular spine) usually results in a reverse Hill-Sachs lesion.1 The extent of this injury is best assessed prior to closed reduction and this can only be done via radiological imaging. Therefore, in this case, early referral to an emergency department would be deemed most appropriate. Unlike anterior or posterior instability, inferior instability does not occur in isolation.
Multidirectional instability, however, encompasses anterior instability and is by definition symptomatic instability in two or more directions. It arises when static and dynamic stabilisers become incompetent due to congenital means (eg, Marfan or Ehlers-Danlos syndromes) or acquired means (unidirectional instability that progresses to multidirectional instability).33 It commonly occurs bilaterally and is associated with generalised joint laxity17 and, most commonly occurs in swimmers—particularly those using the butterfly stroke.34
Prehospital management
There are currently no set guidelines for the ‘pitch-side’ management of a dislocated shoulder,13–15 including the absence of validated UK NICE guidelines, or US Guidelines through the ACSM or the AAOS.
The available literature pertaining to prehospital management refers to a statement made by the Wilderness Medical Society, which dates back to 1989 and was revised in 2013: ‘The common anterior dislocation can usually be reduced [in a pre-hospital setting] without too much difficulty and the sooner it is attempted, the easier it will be’.35 While this statement offers no systematic approach to managing a patient pitch-side, it accepts prehospital shoulder reduction on the assumption of an anterior dislocation.
This statement leads onto several follow-up questions, in particular.
How do we confirm absence or presence of a fracture?
How can we clinically assume that a force large enough to result in a dislocated shoulder would not result in a concomitant fracture, in the absence of X-ray confirmation?
Objectively, there is probably no right answer to this question/these questions and in reality, it therefore places a heavier burden on our clinical judgement. Fragments of information pieced together from an athlete’s mechanism of injury, prior history and pitch-side examination can help differentiate which athletes are suitable for pitch-side management and those who require immediate referral to the nearest emergency department.
Factors to consider
Mechanism of injury
Anterior shoulder dislocations may occur via a direct or indirect mechanism. Knowing the anatomical orientation of the shoulder predislocation will help delineate the direction of the dislocation. Indirect mechanisms usually result from anterior leverage of the glenohumeral head out of the glenoid fossa when the shoulder is abducted and externally rotated. There are many sport-specific examples such as rugby, wresting, gymnastics and throwing sports with overhead activity, for example, cricket and baseball that rely on this positioning, subsequently predisposing them to a shoulder dislocation. It may also occur while blocking high shots in games such as netball and basketball or even goalkeepers in football.36 The resultant position of the follow-through during a miss–hit in a boxer also predisposes them to an anterior dislocation.36 Swimmers undergo repetitive microtrauma through their shoulder joint resulting in laxity, and leverage of the head inevitably occurs at various stages of a swimming stroke.
A direct mechanism of injury can result in any contact sport, and usually occurs when a violent anteriorly directed force occurs on the posterior aspect of the shoulder.36
Past medical history
Certain athletes are predisposed to recurrent shoulder instability, because of a previous acute dislocation, making them vulnerable to repeat episodes. In the event of a shoulder dislocation in this subset of athletes, asking the patient whether prior pitch-side attempts were successful or whether they had to be transferred to hospital for analgesia and sedation is crucial. Doing so negates unnecessary attempts, which may result in more harm to the athlete. Recurrent dislocation affects men three times more often than women, with the dominant extremity involved in 60% of cases.37 It is also worth noting that many athletes with a history of prior dislocation often successfully self-relocate.38
Clinical examination
Following a primary survey, it is normally appropriate to extract the player from the field of play before continuing. This is dependent on the sporting activity and availability of resources. If this is the case, the arm should then be supported in the most comfortable position, often found by the athletes themselves. Once the player is comfortable, a thorough examination using the ‘look-feel-move’ model should be carried out. The examiner must always have a high index of suspicion for a concomitant fracture, and this must be correlated with the clinical presentation and mechanism of injury and in particular the sensation or sound of cracking or grinding. Any athletes with a suspected fracture must be referred to hospital for an x-ray without attempting reduction. Athletes usually present with a loss of the normal shoulder contour and with a limitation in their range of internal rotation. In thin patients, the glenohumeral head may be palpated anteriorly.
A careful assessment of the neurovascular status must be performed prior to attempting relocation as approximately 10% of primary anterior dislocations in athletes are also associated with an axillary nerve neuropraxia.39 An isolated vascular injury is a relatively infrequent complication (1%–2%), but demands immediate intervention. The pathognomonic triad for an axillary artery injury consists of an anteriorly dislocated shoulder, diminished (or absent) radial pulse and palpable axillary haematoma.40 Any clinical examination that reveals diminished pulse pressure over the radial or brachial pulse or even transient coolness of the limb should be referred to hospital via ambulance for an urgent angiography.7 Posterior dislocations are more difficult to diagnose and manage pitch side. They are easily missed, as the arm is held adducted and internally rotated. The two most important clinical findings are limitation of external rotation beyond neutral and a fullness, rather than a hollow, just inferior to the lateral scapular spine. This is the hard humeral head which may be palpable posteriorly and radiological confirmation, usually XR or CT, is required.41 This would help delineate any defects on the humeral head and subsequent glenoid changes after which a decision or either non-operative or operative treatment can be made.42
Only once a thorough clinical examination has been performed coupled with a low index of suspicion for a fracture, can we ask, ‘should reduction be attempted?’
Suitable methods for prehospital relocation
If a decision is made to relocate the shoulder, prompt reduction is always necessary as the procedure becomes more difficult with time. This is partly due to the difficulty experienced in overcoming muscle spasm the longer the shoulder remains out of joint. Although opioid analgesics have been proven effective prior to reduction,13 Entonox may be more readily available on a pitch-side setting, being used on the assumption that there is no associated head or chest injury. In the absence of a fracture, pain usually occurs due to stretching and the subsequent tension on the encompassing muscles and ligaments. Therefore, an early successful reduction significantly alleviates pain and may negate the need for further analgesia. However, pain may persist despite reduction if the mechanism of injury resulted in damage to other underlying structures. Often, clinical experience and the availability of medical facilities dictate the decision to relocate the shoulder on-site within the confines on a medical room setting. In an ideal setting, clinicians with prior experience at attempting shoulder relocation should do so. In its absence, it may be more appropriate to refer the athlete to the nearest emergency department. Athletes with a dislocated shoulder generally ambulate off the field with minimal support. If medical rooms are in close proximity, often the transfer time lost to attempt relocation does not have a negative effect on spasm development. This time may also allow prior analgesics to take effect. However, if these facilities are not within easy reach, it may be more appropriate to relocate pitch-side to avoid overcoming muscle spasm. A variety of non-sedating techniques have been described with successful outcomes.43–46
Relocation procedures
Several methods are not applicable on pitch-side or medical room setting, either due to the requirement of more than one medical person (which is not always guaranteed at sporting events), athlete elevation on a bed (stable plinths are not always available in pitch-side medical first aid rooms) or the use of additional adjuncts such at sheets or straps. Thus, the modification of simpler one-on-one techniques has proven more reliable.43
The single-operator Spaso technique allows the athlete to remain supine on the ground or plinth (if available) while the arm is held vertically at the wrist or forearm. Gentle vertical traction is then applied (figure 1), and while doing so, the shoulder is externally rotated (figure 2). If the athlete experiences any pain or discomfort, they tend to lift their shoulder off the bed. If this occurs, stop any further movement, but maintain traction.45 46 If any difficulty is experienced, the humeral head is palpated through the axilla and gently pushed posteriorly with the free hand while maintaining traction.45 This technique works on the principle that in the vertical position, all shoulder stabilising muscles are directed upwards on to the humerus, thereby assisting reduction to the anatomical state.45 Prospective studies evaluating the clinical efficacy of the Spaso technique for anterior dislocations have been performed in several emergency departments. They report an 83%–87.5% success rate, without any procedural complications.44 46 Ugras et al concluded that the Spaso technique was indeed an effective reduction method without anaesthesia or assistance.44

Spaso technique—vertical traction.

Spaso technique—external rotation.
The Stimson technique, first described in 1900, 47 is a relatively simple technique requiring minimal clinician input. The patient is placed prone with the arm hanging off the edge of a plinth pointing towards the ground. This position results in shoulder flexion. Subsequent downward traction is applied to the athlete’s wrist by either the clinician or by the athlete holding a weighted object (figure 3). Following muscle relaxation, the shoulder should painlessly relocate.43

The Stimson technique.
Alternatively, if the athlete is supine or sitting, the external rotation method of Leidelmeyer can be used. The affected arm is adducted against the torso with the elbow flexed at 90° (figure 4). Using the forearm as a lever, the upper arm is gently, and slowly, externally rotated (figures 5 and 6). Importantly, no significant force is required during the external rotation, and the shoulder is usually reduced by the time the arm is in the coronal plane. This method avoids the unnecessary torque applied during a previously advocated Kocher’s technique, thus avoiding its complications.43 Use of these techniques pitch-side often depends on familiarity, and ideally the pitch-side medical professional should be proficient with more than one technique.48

External-rotation method—arm adducted against torso with the elbow flexed at 90°.

External-rotation method—using the forearm as a lever the upper arm is externally rotated.

External-rotation method—external rotation.
In the event of a failed attempt at reduction, it may be deemed more clinically appropriate for a re-attempt at reduction to occur in a more secure environment with the availability of sedatives and stronger analgesics. Additionally, It would be inappropriate to have a second attempt with a different pitch-side technique. In this case, the shoulder should be immobilised using a sling or shoulder immobilizer. The athlete usually holds their arm in a position that they find most comfortable, and can subsequently be referred to the nearest emergency department.
If an attempt at relocation increases pain, it is likely that a concomitant fracture exists and therefore should be immediately ceased. Once again, the arm should be immobilised and then referred to the nearest emergency department for imaging.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
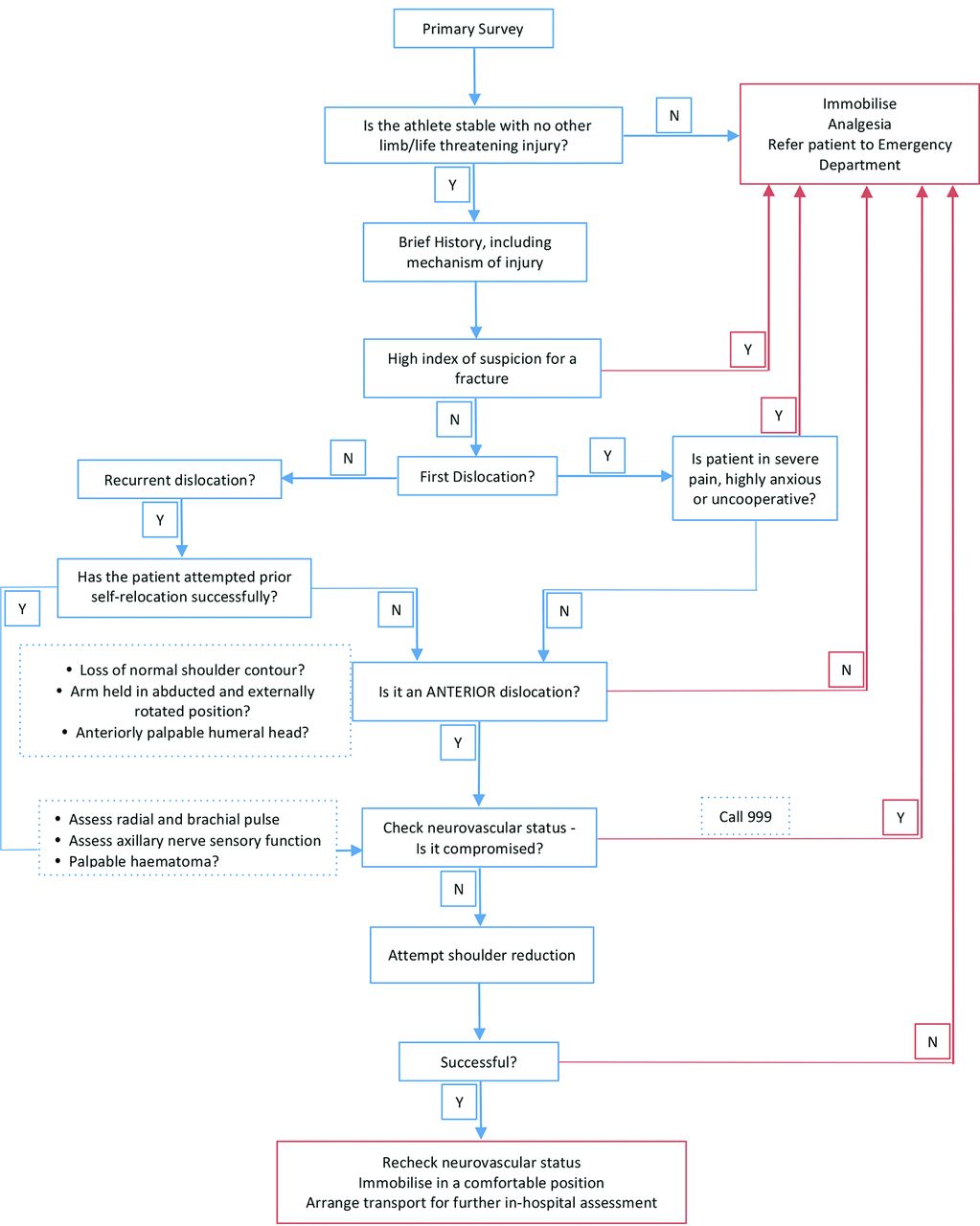
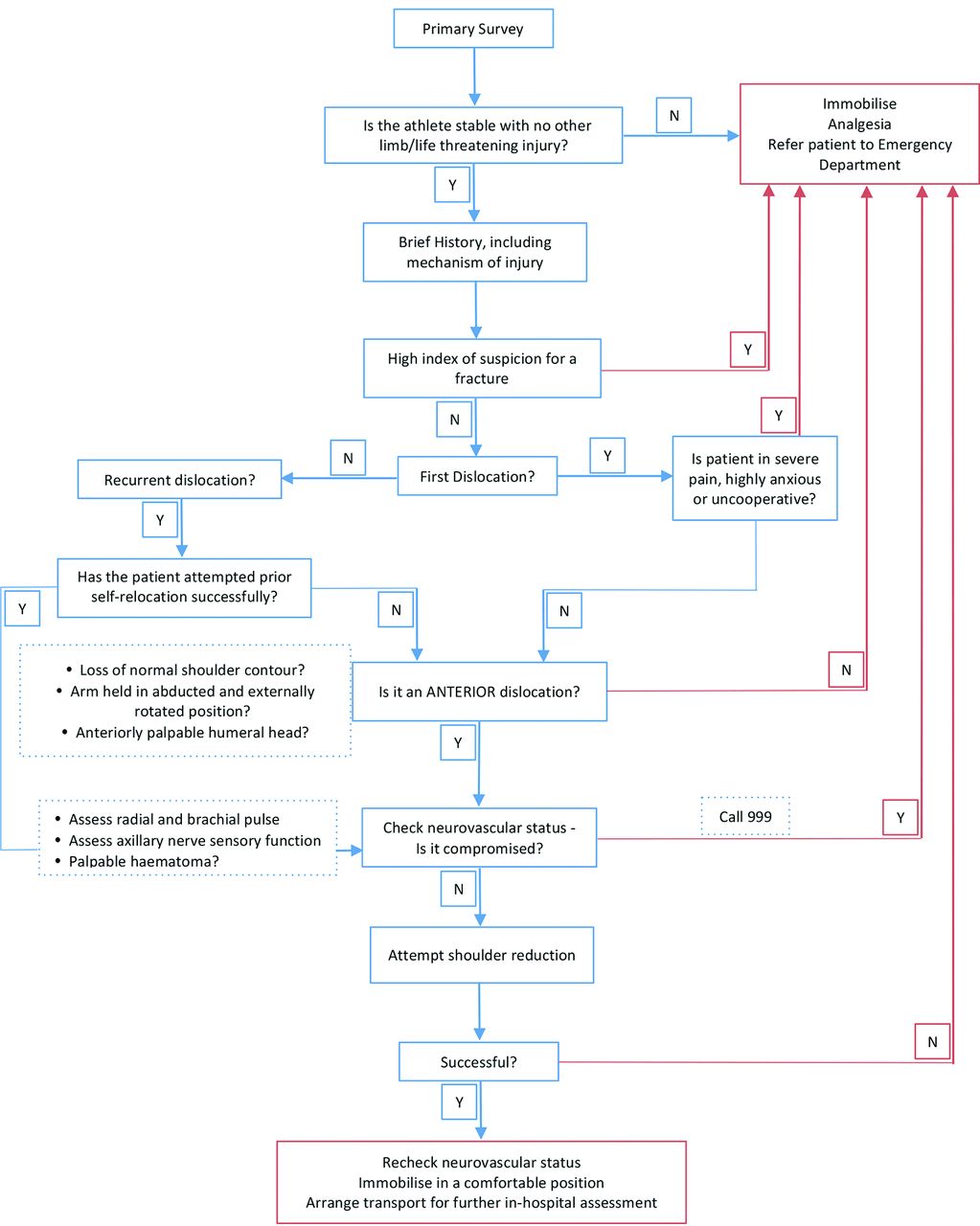
A systematic approach to the pitch-side management of a dislocated shoulder.
A ‘clunk’ is often felt on successful relocation with the shoulder contour appearing normalised and often with almost immediate relief of symptoms. Irrespective of the outcome of the attempted relocation, all athletes should be re-examined for any compromise to their neurovascular status.
Postreduction care
Figure 7 demonstrates a systematic approach to the pitch-side management of a dislocated shoulder. In the event of a successful pitch-side relocation, the athlete should be referred to a hospital for further orthopaedic assessment with the arm should be immobilised in a sling. The position of the sling has been a topic well debated, with cadaveric and MRI studies showing optimal reduction of the torn labrum to bone in the externally rotated position49–51 compared with the internally rotated position. Conversely, Liavaag et al showed that having the arm in the internally rotated position in a sling had no impact on rates of recurrence in comparison to the externally rotated position.52 For the purposes of pitch-side management, immobilising the arm in an arm sling in the most comfortable either position should suffice prior to referral.
Conclusion
Shoulder dislocations are relatively common sporting injuries and even in the absence of clinically validated guidelines, pitch-side reduction of an ‘uncomplicated’ anterior dislocation is common practice. A good history and through clinical examination would help discern the potentially limb-threatening injuries that require urgent referral to hospital or those that may require radiographic confirmation of fracture exclusion. However, there is no substitute for sound clinical judgement. When a decision is made to reduce an anteriorly dislocated shoulder, do so at the earliest opportunity to avoid overcoming increasing resistance due to muscle spasm using techniques that you are familiar with. Once reduced, the shoulder should be immobilised in the most comfortable position and referred for an expert opinion. However, we recommend those ‘pitch-side’ medical practitioners who provide this form of support should have attended appropriate training and ensure adequate malpractice cover.
Finally, hope for the best, but prepare for the worst; a patient will always thank you for a successful reduction!
Learning points
Anterior dislocations account for up to 90% of all shoulder dislocations.
Athletes with a high index of suspicion for a fracture should be referred to the nearest hospital without any attempts at reduction
Prior to attempting reduction, confirm that the shoulder is anteriorly dislocated:
Loss of normal shoulder contour?
Arm held in abducted and externally rotated position?
Anteriorly palpable humeral head?
Always assess the neurovascular status of the limb, prior to and after reduction.
What are the new findings?
In the absence of a standardised management protocol published for the initial management of an anterior dislocated shoulder in a pitch-side setting, this article proposes a structured, systematic approach to the pitch-side management of a shoulder dislocation.
Despite the availability of different reduction techniques, few are applicable in a pitch-side setting. The Stimson and Spaso techniques are simple and effective for pitch-side reduction with the external rotation method being an effective alternative.
With regard to postreduction care, immobilise the limb in the most comfortable position prior to referral to hospital.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.