Article Text

Abstract
Introduction Hip arthroscopy is increasingly adopted for the treatment of intra-articular and extra-articular pathologies. Studies from USA demonstrate a 365% increase in the number of procedures performed between 2004 and 2009 and 250% increase between 2007 and 2011. There is limited evidence of long-term efficacy for this procedure and hip arthroscopy is not universally funded across England. The aim of this study is to describe temporal trends in the adoption of hip arthroscopy in England between 2002 and 2013 and to forecast trends for the next 10 years.
Methods A search of the Hospital Episodes Database was performed for all codes describing arthroscopic hip procedures with patient age, sex and area of residence.
Results 11 329 hip arthroscopies were performed in National Health Service hospitals in England between 2002 and 2013. The number of hip arthroscopies performed increased by 727% (p<0.0001) during this period and is forecast to increase by 1388% in 2023. Females represent 60% of all patients undergoing hip arthroscopy (p<0.001). Median age category is 40–44 for females and 35–39 for males and average age decreased during the study period (p<0.0001). There is significant regional variation in procedure incidence. In the final year of this study the highest incidence was in the Southwest (8.63/100 000 population) and lowest in East Midlands (1.29/100 000 population).
Conclusions The increase in number of hip arthroscopies performed in England reflects trends in USA and continued increases are forecast. Evidence from robust clinical trials is required to justify the increasing number of procedures performed and regional variation suggests potential inequality in the provision of this intervention.
- Arthroscopy
- Hip
- Orthopaedics
- Surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
Our study demonstrates a 727% increase in the number of arthroscopic hip procedures performed in England between 2002 and 2013 and a forecast increase of 1388% by 2023, despite limited evidence of long-term efficacy. Hip arthroscopy is most commonly performed in females and average patient age is decreasing. There is significant regional variation with a 6.69-fold difference in procedure incidence between regions suggesting potential inequality in healthcare provision.
Introduction
Arthroscopic intervention is adopted for an increasing number of hip pathologies. In an acute setting, joint irrigation can be performed arthroscopically for the management of septic arthritis.1 Fixation of femoral head fractures is also possible arthroscopically.2 In an elective setting, hip arthroscopy is used in the treatment of a range of intracapsular conditions including femoroacetabular impingement (FAI),3 labral pathology,4 chondral lesions,5 instability,6 synovial chondromatosis7 and ligamentum teres injuries.8 Applications continue to expand and hip arthroscopy is also used to facilitate hip reduction in infants with development dysplasia of the hip9 and for the treatment of extracapsular pathology including iliopsoas tendon and iliotibial band pathology.10
Hip arthroscopy was first described in 1931,11 although implementation has only been possible more recently after technical advances were made that allow adequate distraction of the femoral head from the acetabulum and joint instrumentation with arthroscopic devices.12 The arthroscopic approach confers potential benefits over open surgery and most studies report lower complication rates and outcomes that are equal to or better than open approaches.13
An increasing number of arthroscopic hip procedures are performed each year worldwide. In Korea, there was a twofold increase between 2007 and 2010.14 In the USA there was an increase of 365% between 2004 and 200915 and 250% between 2007 and 2011,16 where an estimated 70 000 procedures are performed annually.17 The number of hip arthroscopy procedures performed by orthopaedic trainees in the USA increased 18-fold between 1999 and 2009.11 Despite the rapid uptake, there are very few studies reporting long-term outcomes for arthroscopic hip surgery and these are limited to cohort studies. This is particularly salient given the increasing questions raised over the efficacy of arthroscopic knee surgery.18 Randomised controlled trials are required to compare the efficacy of arthroscopic hip surgery with non-operative interventions,19 and such studies are currently recruiting patients.20
The adoption of hip arthroscopy in the UK has not been described. It is not universally funded by Clinical Commissioning Groups, which may give rise to geographical variation in practice. The aim of this study is to describe temporal trends in the adoption of hip arthroscopy since 2002 and to project trends for the next 10 years. The publication of temporal trends may aid decision-making by surgeons and commissioning bodies. Regional variation is of particular interest given the perceived inequalities in the commissioning landscape.
How might it impact on clinical practice in the near future?
The increasing number of arthroscopic hip procedures performed each year in England highlights the requirement for robust evidence of procedure-specific effectiveness from clinical trials. Large regional variation in the provision of hip arthroscopy suggests uncertainty among clinicians and healthcare commissioners over clinical effectiveness. The decreasing age of patients is consistent with cohort studies demonstrating good outcomes in active young adults and worse outcomes with advancing age.
Methods
Data was collected from the Hospital Episode Statistics (HES) database.21 The HES database contains data on patients attending National Health Service (NHS) hospitals in England for treatment. Each entry represents a single episode of care and codes are assigned to diagnoses and procedures during that episode. Anonymised data was requested using Operating Procedure Codes (OPCS-4) specific to hip arthroscopy and included patient age and gender and area of residence between the years 2002 and 2013. The search included all arthroscopic procedures that were combined with joint-specific codes for the hip (see online supplementary data for full search details). The generic nature of these codes and their modification through different iterations of OPCS-4 codes within the period of this search meant it was not possible to analyse trends in individual procedures. Several procedures may be performed within the same joint during arthroscopic hip surgery, for example, chondroplasty and labral repair. When several codes were encountered within the same patient episode, only the primary code was counted to prevent duplication. To aid data analysis, the Health and Social Care Information Centre geographical regions in England were grouped as the North (North East (q30), North West (q31), Yorkshire and the Humber (q32)), Midlands (East Midlands (q33), West Midlands (q34), East of England (q35)), South East (South East Coast (q37), South Central (q38)), South West (q39) and London (q36). The number of procedures performed in each region was calculated per 100 000 population. Projections were made using the Drift method and are provided with 95% prediction intervals. Forecasts are equal to the last value plus the average change seen in historical data, so that the forecast for time T+h is given by:
Supplemental material
All statistical tests were performed using STATA V.13.1 (StataCorp, College Station, Texas, USA). Relationships between variables were explored using a χ2 test. Statistical analysis of trends was performed using simple linear regression for continuous variables and Wilcoxon Rank-Sum methodology for categorical variables. A p value less than 0.05 was taken as the threshold for significance.
Results
Total number of procedures
A total of 11 329 hip arthroscopies were performed in NHS hospitals in England between 2002 and 2013. There was a statistically significant increase of 727% (p<0.0001) during this period and there is a projected increase of 1388% by 2023 (table 1 and figure 1).
Observed and forecast total number of hip arthroscopies (with 95% prediction intervals (PI))
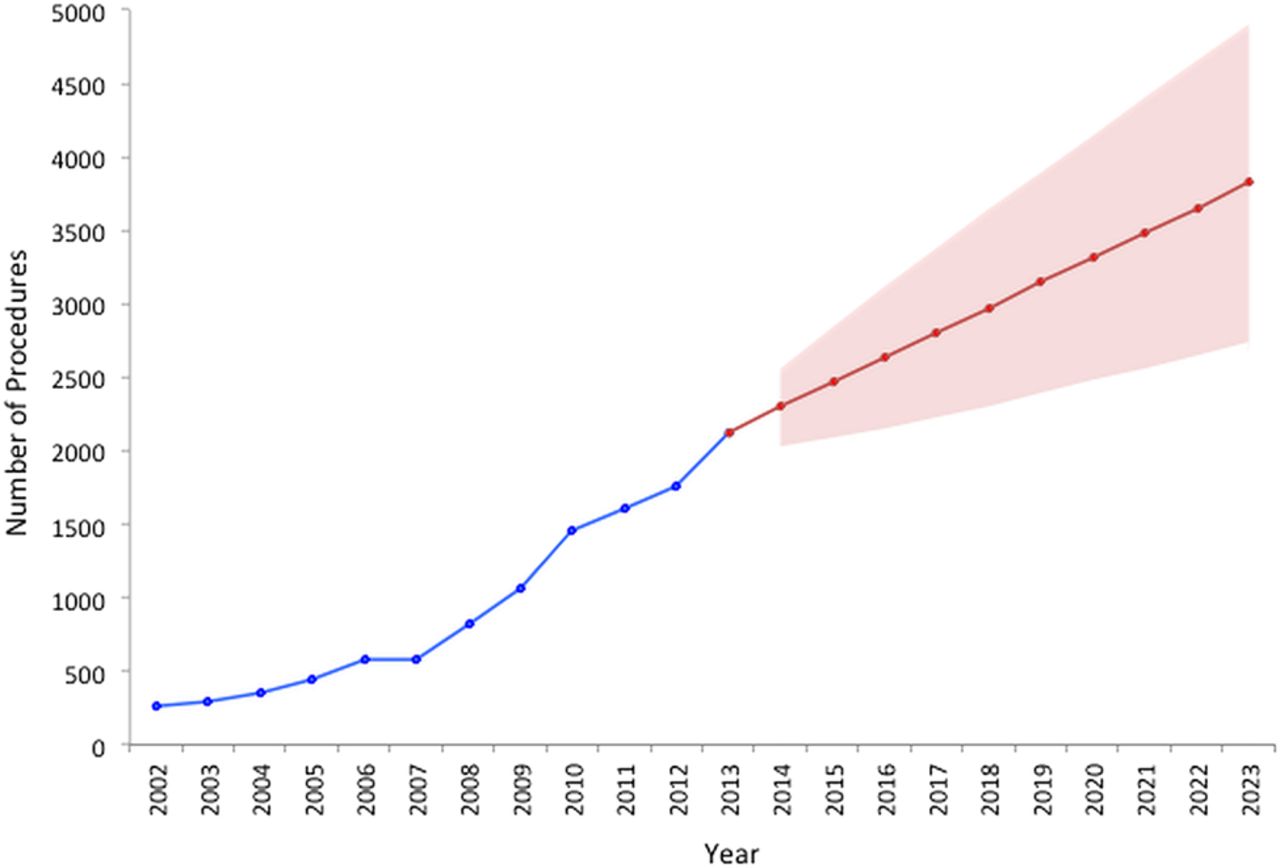
Observed and forecast total number of hip arthroscopies (with 95% prediction intervals).
Patient demographics
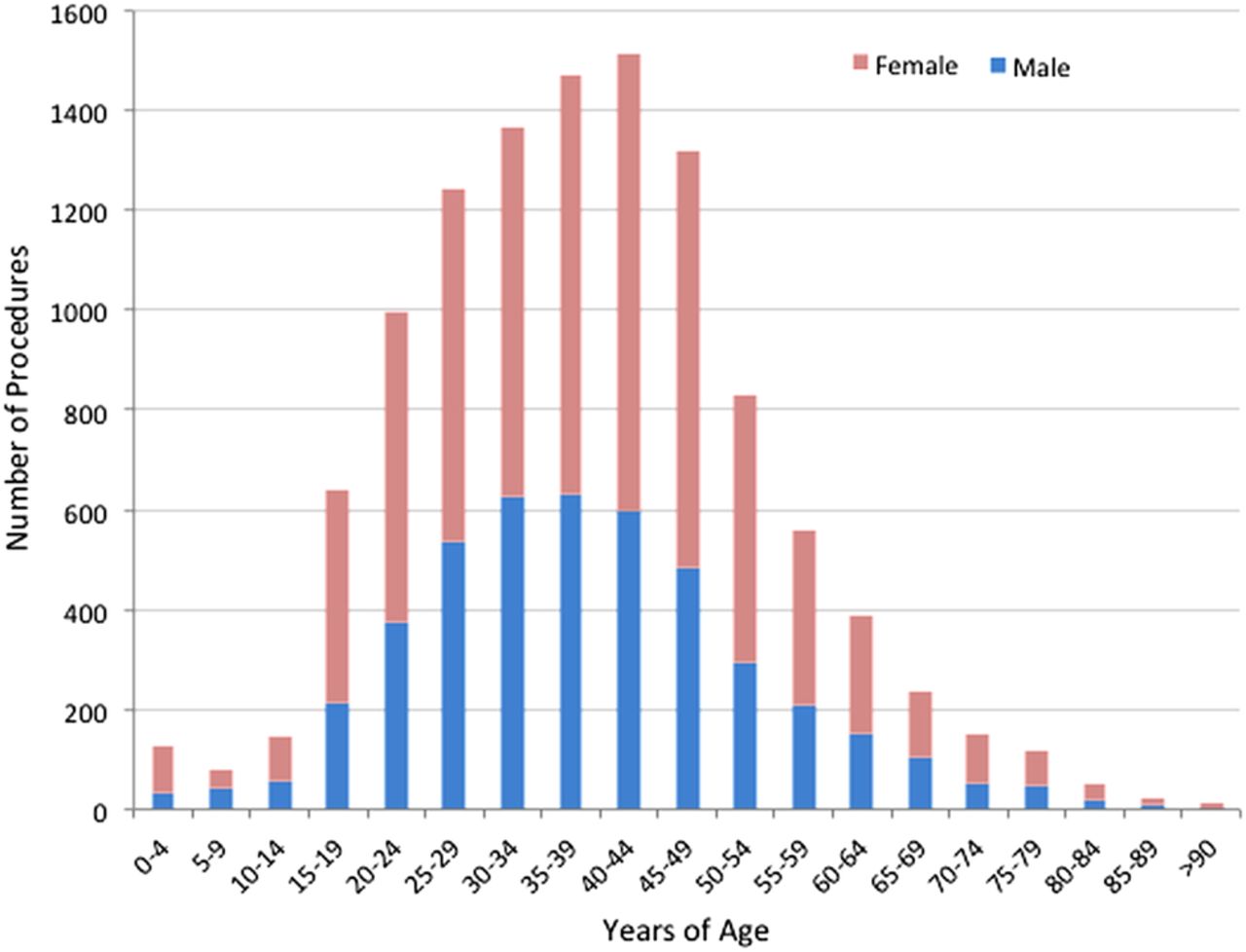
Arthroscopic hip procedures are performed more frequently in females (60.3%) than males (39.7%) (p<0.001; table 2 and figure 2). Females accounted for between 56.3% and 64.1% of cases throughout all years of the study and there was no statistically significant change in these proportions with time (p=0.289; table 2).
Observed number of hip arthroscopies for males and females
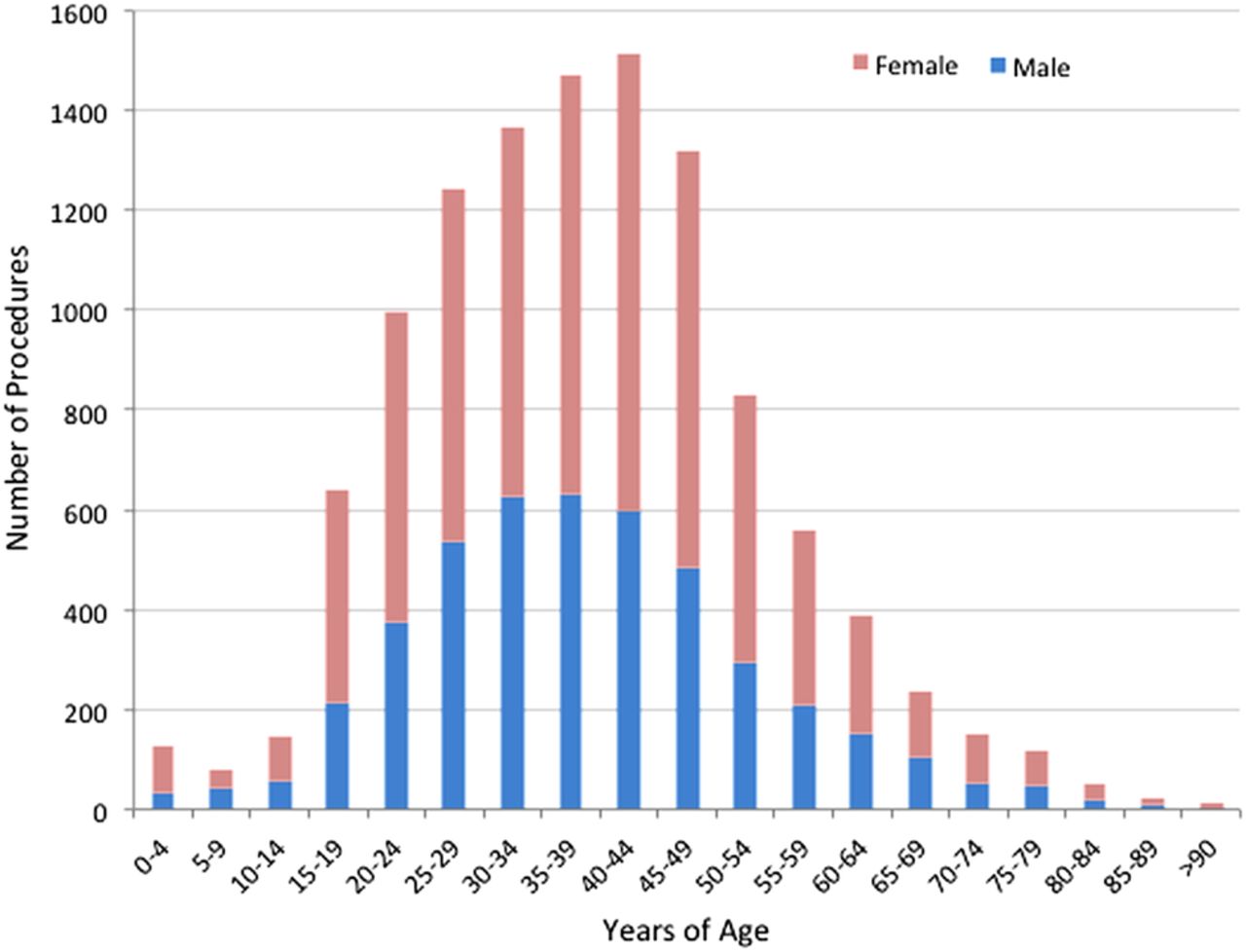
Histogram illustrating number of arthroscopic hip procedures 2002–2013 by age and sex.
Females were older at the time of surgery with a median age range 40–44 years compared with 35–39 for males (table 2) although this was not statistically significant (p=0.075). The age of patients undergoing surgery is decreasing (p<0.0001 z=−0.544) and this trend is present for males (p<0.0001 z=−3.96) and females (p<0.0001 z=−3.83). The age group with the greatest increase in procedure rate is 20–24 years.
Regional variation
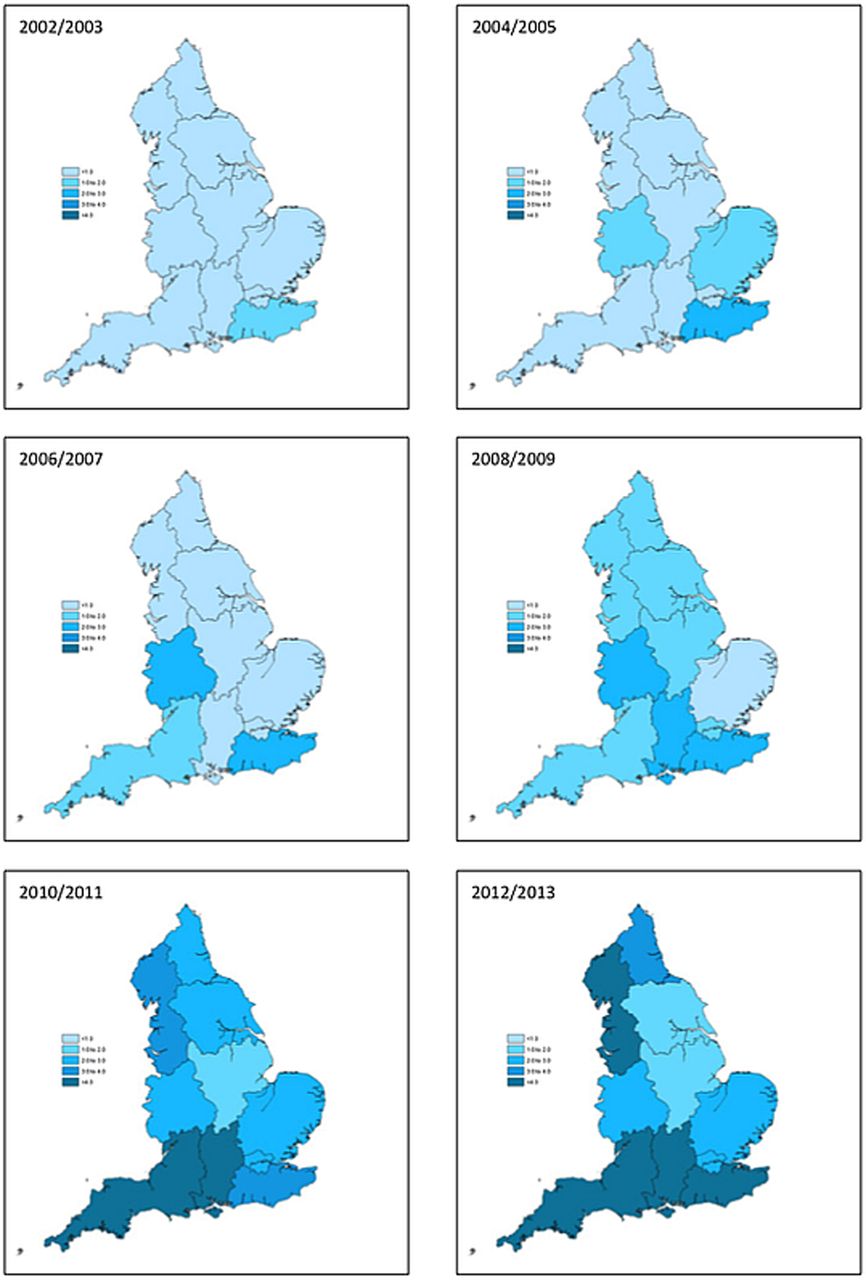
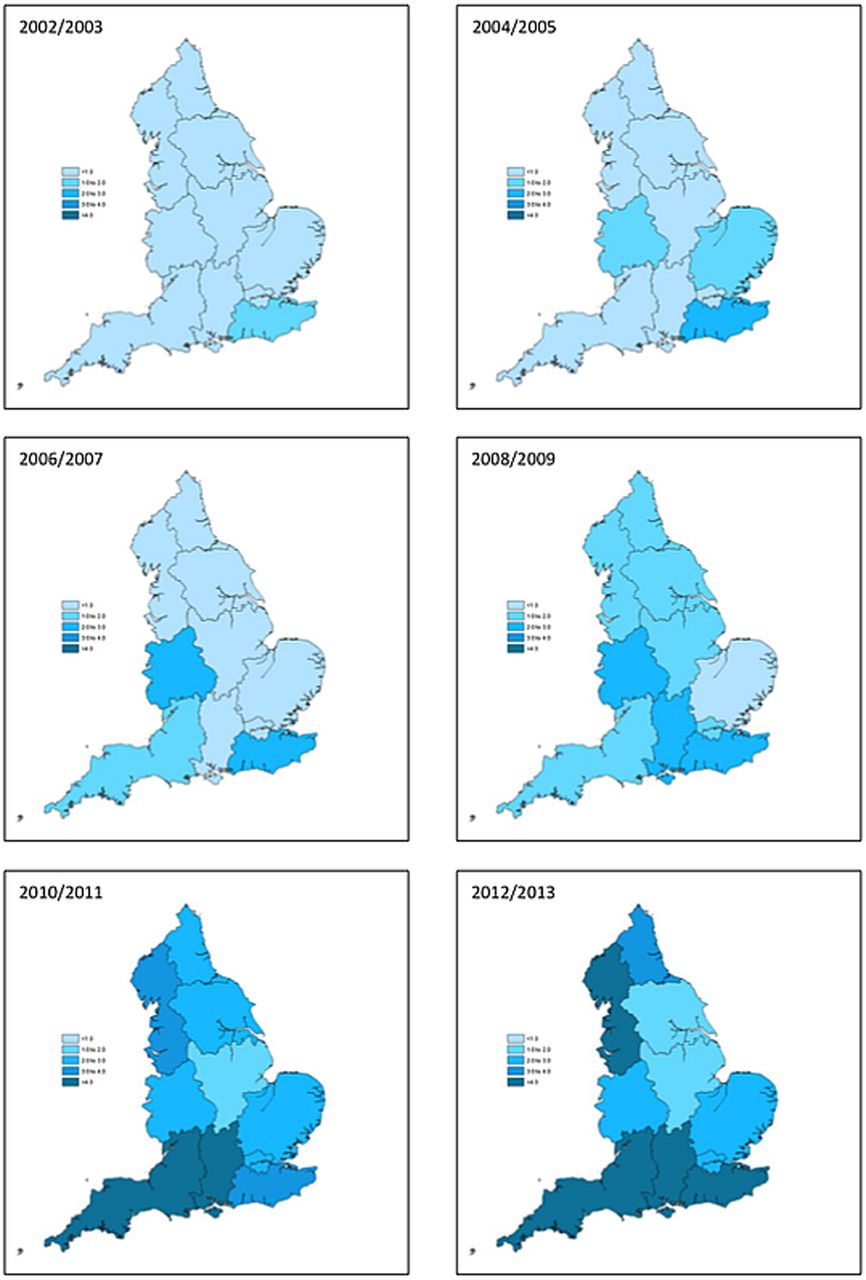
There has been a statistically significant increase in the number of arthroscopic hip procedures performed in all regions of England since 2002 (p<0.0001) with a concurrent change in the relative number of procedures performed between regions (p<0.0001) trending towards the Southwest and Southeast (table 3). Nationwide, the incidence of hip arthroscopy procedures has risen from 0.51 to 4.09 per 100 000 population (table 3). The greatest growth has taken place in the Southwest (1640%) and the smallest in the Midlands (355%). Considering all regions, the most rapid rate of increase took place between 2006 and 2009, beyond which there has been continued divergence in the number of procedures performed per capita in each region (figure 3). An increase in the number of procedures continues in the Southwest, Southeast and North of England, whereas there is evidence of plateau in the Midlands and London (figure 3). In the final year of this study, the highest number of procedures per capita was performed in the Southwest (8.63 per 100 000 population) and lowest in the East Midlands (1.29 per 100 000 population) Strategic Health Authority Region (figure 4). This represents a 6.69-fold difference between regions.
Regional variation in arthroscopic hip procedures in England per 100 000 population

Regional variation in arthroscopic hip procedures in England per 100 000 population represented as a non-weighted moving average over 2 years.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Regional variation in number of hip arthroscopy procedures per 100 000 population in each strategic health authority region 2002–2013.
Discussion
The aim of this study was to describe temporal trends in the adoption of hip arthroscopy since 2002 and to project trends for the next 10 years. The number of arthroscopic hip procedures performed in England has risen by 727% since 2002 and this trend is projected to continue over the next 10 years despite limited evidence of long-term efficacy or superiority over non-operative measures. These trends mirror those of subacromial decompression and rotator cuff repair of the shoulder, again in the absence of robust evidence to demonstrate clinical effectiveness.22 Increasing questions are also being raised over the efficacy of arthroscopic knee surgery.18
The rate of increase in the number of arthroscopic hip procedures is broadly in line with that reported in the USA where a 365% increase was reported between 2004 and 200915 and a 250% increase between 2007 and 2011.16 The incidence of hip arthroscopy reported in Korea is comparable to that in England at 5.17 per 100 000 in 2010.14 Studies from the USA have calculated procedure incidence using the PearlDiver Patient Records Database and hence are not representative of the general population. Our study underestimates the number of hip arthroscopy procedures performed in England since it does not include those undertaken in private healthcare.
Several factors are likely to be driving the increasing number of hip arthroscopies. Conditions such as femoracetabular impingement and labral tears are increasingly recognised as a source of pain and future osteoarthritis23 by both clinicians and patients. Demands are buoyed by outcomes from cohort studies, which report good short-term and medium-term outcomes for a wide range of arthroscopic hip procedures.24 ,25 Guidance from the National Institute for Health and Clinical Excellence (NICE) may have played a role. In 2007, NICE highlighted the uncertain efficacy of hip arthroscopy for the treatment of femoracetabular impingement, whereas in 2011, they concluded that there was adequate evidence of symptom improvement in the short and medium term. There is no strong inflection of the trend line at these time points and it is not possible to say with any certainty that they influenced practice. In the USA, there was an 18-fold increase in the number of hip arthroscopies performed by candidates of the American Board of Orthopaedic Surgery between 1999 and 200911 and a 600% increase between 2006 and 2010.26 Hip arthroscopy is now an established procedure within training programmes.
Hip arthroscopy is more frequently performed in females (60.3%) than in males (39.7%) in England and this has not changed during the period of study. The same gender ratio was reported in the USA where 63% patients are female.16 Additional studies from the USA and Korea have reported more equal gender distributions with females representing 52.9%15 and 51.9%,14 respectively. The higher number of procedures in females is an interesting finding given FAI, one of the most frequent indications for hip arthroscopy,16 has a higher prevalence in males.27 The HES database does not utilise sufficiently specific codes to explore the indications for surgery or the nature of procedure performed, and this is an area for future research. There are likely to be gender-specific indications for arthroscopic hip surgery.
Median age at hip arthroscopy is 40–44 years for females and 35–39 years for males, although there is no statistically significant difference in age. These ages are comparable to studies in the USA,15 ,16 and slightly younger than a study from Korea.14 In the USA, the greatest increase in the number of procedures was seen in patients <30 years of age,16 as is the case in our study. This may relate to the publication of good outcomes in active young adults who are able to return to high level sporting activities.28 Conversely, outcomes are worse in older patients.29
There is significant regional variation in the incidence of hip arthroscopy in England with continuing divergence. The highest incidence is seen in the Southwest and the lowest is in East Midlands. Regional variation is also seen in the USA, albeit less pronounced with a 2.05-fold difference between regions15 compared with the 6.69-fold difference in this study. Key factors are likely to be local expertise in hip arthroscopy and the local commissioning of services in England. Hip arthroscopy is not funded by the NHS in many regions given the limited evidence of efficacy available for many arthroscopic hip procedures. Indeed, equipoise is present within surgeon and patient communities for the arthroscopic treatment of FAI.19 Results from robust clinical trials will inform decision makers and may give rise to more standardised care.
Our forecast rise in the number of arthroscopic hip procedures of 1388% between 2002 and 2023 will accentuate challenging funding decisions within the NHS. It is difficult to quantify the cost of hip arthroscopy procedures due to their heterogeneous nature. A study from America estimated an average direct cost of $11 850 for arthroscopic treatment of femoroacetabular impingement and concluded that this was cost-effective in patients without evidence of osteoarthritis at $21 700 per Quality Adjusted Life Year (QALY).30 These results were replicated in a study from Scotland with an estimated a cost of £19 335 per QALY, meeting the NICE threshold for cost-effective inventions.31 Cost-analysis is required for the diverse spectrum of hip conditions treated arthroscopically.
There are several limitations to this study. As already discussed, limitations of the HES database are the exclusion of procedures performed within private healthcare sector and the limited codes available to determine the precise indication and nature of procedure performed. Inclusion of new OPCS-4 codes for specific diagnoses and arthroscopic hip procedures would greatly facilitate the study of clinical activities. At present it is not possible to accurately code the array of different procedures performed. The three most frequently used codes in the final year of this study were ‘endoscopic excision of articular cartilage’, ‘endoscopic decompression of joint’ and ‘other endoscopic therapeutic procedure’.
It is clear that the number of arthroscopic procedures continues to increase in line with observations from the USA and Korea. Robust evidence of efficacy is required from clinical studies and research priorities should reflect the changing nature of healthcare provision. An increasing demand for hip arthroscopy may also have implications for physiotherapy rehabilitation and orthopaedic training, and this is particularly salient given the procedure has a very steep learning curve.32
Acknowledgments
The authors would like to acknowledge support from the National Institute for Health Research (NIHR) Oxford Musculoskeletal Biomedical Research Unit.
References
Footnotes
Contributors AJRP was responsible for study conception and design, acquisition of data, analysis and interpretation of data, drafting and critical revision of manuscript. TTM and JB were responsible for analysis and interpretation of data, drafting and critical revision of manuscript. JH, LM and KW were responsible for acquisition of data, analysis and interpretation of data. GERT, AT and AJA were responsible for drafting and critical revision of manuscript. GC was responsible for analysis, interpretation of data and statistical support. AJC was responsible for study conception and design, analysis and interpretation of data, drafting and critical revision of manuscript. SG-J was responsible for study conception and design, analysis and interpretation of data, drafting and critical revision of manuscript.
Funding AJRP received funding from a Joint Royal College of Surgeons of England and Dunhill Medical Trust Research Fellowship. JB received funding from a Royal College of Surgeons of England Research Fellowship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.