Article Text

Abstract
Background Scrummaging is unique to rugby union and involves 2 ‘packs’ of 8 players competing to regain ball possession. Intending to serve as a quick and safe method to restart the game, injury prevalence during scrummaging necessitates further evaluation of this environment.
Aims The aim of this study was to determine the effect of scrummage engagement sequences on spinal kinematics of the hooker. The conditions investigated were: (1) live competitive scrummaging using the new ‘crouch, bind, set’ sequence; (2) live competitive scrummaging using the old ‘crouch touch pause engage’ sequence and (3) training scrummaging using a scrum machine.
Methods Inertial sensors provided three-dimensional kinematic data across 5 spinal regions. Participants (n=29) were adult, male community club and university-level hookers.
Results Engagement sequence had no effect on resultant kinematics of any spinal region. Machine scrummaging resulted in lesser magnitudes of motion in the upper spinal regions. Around two-thirds of the total available cervical motion was utilised during live scrummaging.
Conclusions This study indicates that the most recent laws do not influence the spinal kinematics of the hooker during live scrummaging; however, there may be other benefits from these law changes that fall outside the scope of this investigation.
- Rugby
- Spine
- Biomechanics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
There are no spinal kinematic differences between the two competitive scrummaging scenarios indicating neither a positive nor negative effect of the law change.
Large magnitudes of thoracic and lumbar spine motion may put these spinal regions at an increased risk of injury.
Machine scrummaging is a much more constrained kinematic environment.
Modest amount of cervical flexion may be owing to a large amount of ‘stabilising’ muscle forces in order to minimise head displacement.
Introduction
Rugby union players are consistently exposed to a relatively high risk of injury across all playing levels.1–12 While the high level of participation suggests that players accept this risk of injury, specific elements within the game remain the target for reduction strategies. The scrummage (hereafter termed the ‘scrum’), involves eight players from each team attempting, en masse, to push their opponents backwards and regain ball possession. This represents the contact event with the highest risk of injury within the sport.13 World Rugby, the game's governing body, has recently evolved the laws in an attempt to reduce this risk of injury; hence, as of the 2013/2014 playing season, the scrum followed the referee's command ‘crouch-bind-set’ (CBS), as opposed to ‘crouch-touch-pause-engage’ (CTPE).14
Scrum injuries can be either acute, chronic or degenerative in nature,15–17 with longer term exposure to this demanding biomechanical environment associated with disc narrowing (35–71% incidence), osteophyte formation (83%), apophyseal joint degeneration (74%), and degeneration of the vertebral endplates (77%).18 ,19 Given the time spent scrummaging compared with other contact events during a game, it is associated with a disproportionately high percentage (6–13%) of all spinal injuries within the sport.20–25 These spinal injuries predominantly happen to players of the front row. Front-row players (ie, the three players from each team, who directly oppose each other) are at particular risk of both chronic and acute injuries, accounting for 78% of all scrum-based acute cervical spine injuries.21 ,26 While it is acknowledged that risk of injury is multifactorial, the biomechanical demands of the scrum are unique and are likely to significantly contribute to the risk of injury. The scrum consists primarily of the ‘hit/impact’, followed by a sustained attempt to ‘shove’. The ‘hit’ is where the two packs initially engage, immediately after the referee's instruction. Both packs then produce a sustained shove, aiming to push the opposition away from the ball. As the packs engage, the shoulders of the front-row players of each team collide, their heads become interlocked and are forced underneath the chest of their opposing player. The impact force of this interaction has previously been reported, varying from 4.4–16.5 kN,27–31 measured by instrumenting either the scrum machine or shoulder pads (point of impact) of front-row players, during live scrummaging.31
Recent kinematic studies have additionally focused on investigating neuromuscular activation patterns during simulated, live and machine-based scrummaging.31 ,32 While no significant differences were observed between engagement sequences for body kinematics, it does appear that the ‘crouch-bind-set’ engagement sequence may prepare the cervical spine by stiffening the joints prior to impact. Furthermore, it was reported that machine scrummaging does not accurately replicate live scrummaging, suggesting the need for future studies to focus on investigations of live scrummaging.
As the scrum has been identified as being specifically associated with injury, a greater understanding of spinal kinematics will further aid in the quest for injury reduction. To date, while studies have considered machine-based and simulated live scrummaging,33 ,34 technical challenges have prevented studies from acquiring spinal kinematics during competitive scrummaging. Given the association between scrummaging and the potential for spinal injury, it is critical that these challenges are met to enable data acquisition in the most relevant physical environment.
This study aimed to determine the resultant spinal kinematics of the hooker during competitive scrummaging using two different sequences (CBS and CTPE), and using CBS when performing machine-based scrummaging. This study focused on the most injury-prone player, the hooker,21 ,23–25 generating the first data sets that allow direct comparison of spinal kinematics between the new and old scrum sequences. It was hypothesised that the hooker's spinal kinematics will be more constrained during the new (CBS), as opposed to the older (CTPE), engagement sequence.
Materials and methods
A repeated-measures design was employed to evaluate the effect of the scrum engagement sequence (within-group factor) on three-dimensional spinal kinematics. The methodology replicated the scrum law evolution in both training and competitive scenarios.
Participants
Hookers were recruited from a convenience sample of local community club and university rugby union teams. Data were collected from all participants during team versus team interactions (hereafter described as competitive scrummaging), using both the old and new scrum sequences. Some of these hookers were also analysed when their eight players (the ‘pack’) were using a scrum machine within a typical training scenario. All participants were deemed by their qualified coach to have the requisite skill and knowledge of playing in this position, and had been appropriately trained, according to World Rugby guidelines.14 Potential participants were excluded if they had inadequate front-row experience, a history of any major spinal injury, or any indication of current neuromusculoskeletal neck problems (eg, pain). The study was approved by the Cardiff School of Engineering Ethics Committee, with all volunteers providing written informed consent.
Equipment
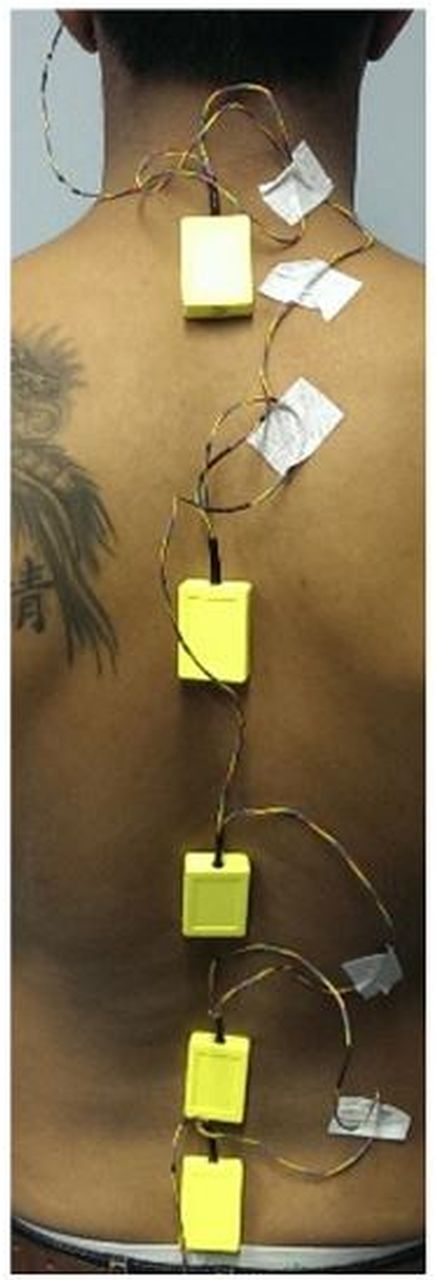
Participants were instrumented with a string of inertial sensors (THETAMetrix, Waterlooville, UK) adhered to the skin on the forehead and overlying the spinous processes of C7, T7, T12, L3 and S1 (figure 1). Each sensor was comprised of a triaxial accelerometer, gyroscope and magnetometer, and sampled at 40 Hz/sensor. The sensors had previously been validated for reliability and accuracy during factory calibration, with errors typically <1°. The sensors’ fusion algorithm, incorporating Kalman filtering, provided drift-free computation of absolute orientation. Similar sensors have been widely used for spinal motion analysis,35 ,36 and such an experimental set has been used previously during rugby scrummaging.37 Each sensor was adhered directly to the skin using double-sided hypoallergenic tape.
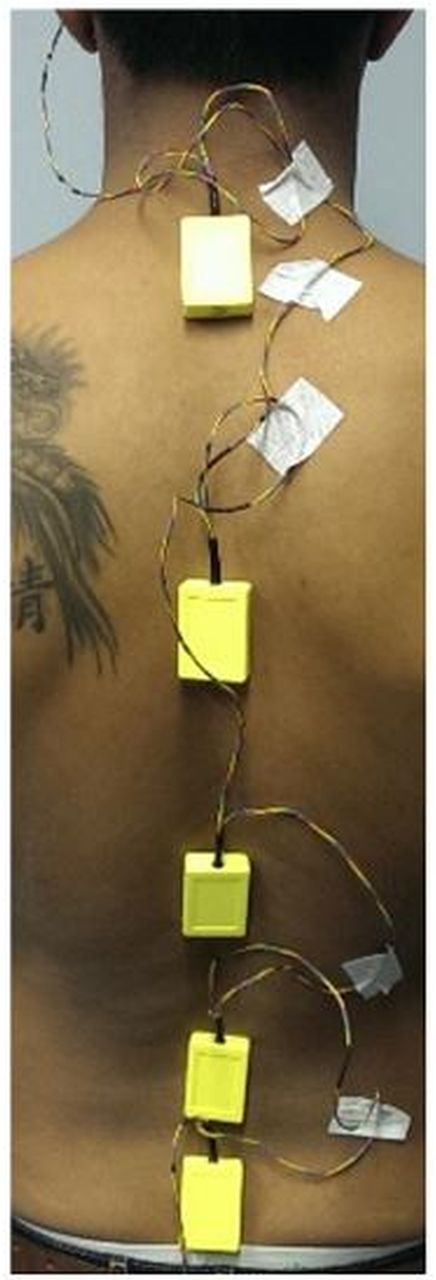
Inertial sensor placements over the spinous processes of C7, T7, T12, L3 and S1.
This created five spinal ‘segments’ (ie, the spinal region between these 6 specific locations), which were defined as the cervical (C), upper thoracic (UTx), lower thoracic (LTx), upper lumbar (ULx) and lower lumbar (LLx) regions. A modified scrum cap was used to reinforce the attachment of the forehead sensor. Absolute orientations, expressed as Euler angles, were determined for each sensor and stored on a PC.
Procedures
Data collection was integrated within scheduled training sessions, such that all players were familiar with the facilities and environment. All participants completed their club's standard warm-up routine before being instrumented with the inertial sensors and taking part in their trial. Each trial lasted approximately 15 min. Prior to scrummaging, each player completed range of motion (ROM) trials to characterise their normal, active, spinal ROM. This was performed for the full spine, while additional cervical spine ROM data was collected in a position of hip flexion (similar to that of scrummaging). Each uniplanar motion was performed three times in a predefined order (flexion/extension, lateral bending and rotation), with a short pause in between each motion. The participant always resumed a neutral position between movements. For the cervical segment, normalisation was performed from the hip flexion ROM trial. For all other segments, normalisation was performed from the standing ROM trial. The peak ROM was calculated for each motion and each spinal segment. All participants then performed three trials of the new (CBS) and old (CTPE) sequences, within a competitive environment, with scrums being performed on either grass or synthetic (3G) turf, depending on their training facilities. The sequence of scrums was randomised, with players instructed to replicate their ‘in-game’ scrum performance. Prior to testing, participants were assigned a value, via a table of randomised numbers, as to the order they would perform the two engagement sequences. All trials for one engagement sequence were completed before moving onto the next sequence. Players were allowed 2 min for full physiological recovery between each trial,38 ,39 to minimise the effect of fatigue.40 ,41 Additionally, where a scrum machine was available, the pack also performed the CBS sequence to replicate a typical training scenario.
Data processing
Absolute orientations of the sensors, described as Euler angles, were converted to rotation matrices, and resultant angles between two adjacent sensors were calculated through matrix multiplication. This process is commonplace in three-dimensional kinematic analysis, with the resultant angles describing the ROM of each spinal segment. ROM computation was completed using custom Matlab (Mathworks, 2012a) scripts.35 ,37 ,42 The rotation order corresponded to motion describing flexion-extension, lateral bending and rotation. This resulted in six motions for each spinal segment described as flexion, extension, left and right lateral bending, and left and right rotation.
ROM values were used to determine the spinal ROM relative to each participant's maximal ROM, defined in the earlier ROM trials, as it is increasingly acknowledged that end-range postures have the potential to increase risk of injury.43–46 Data were time-normalised according to event duration. All kinematic data were filtered using a zero lag 4th order low-pass Butterworth filter, with a 6 Hz cut-off frequency.47 Sensor-skin adhesion was confirmed before and after each trial, with data discounted in cases where there appeared to have been sensor displacement.
Participants and environment
Table 1 describes the 29 hookers analysed during the competitive scrum scenarios. Fourteen of these hookers were also analysed within a training scenario, with their pack scrummaging against a machine on a grass surface.
Data describing the 29 hookers analysed within a competitive scrum
Statistical analysis
Normality and sphericity were checked using Shapiro-Wilk and Mauchly's test, respectively. A one-way repeated measures ANOVA, with scrum condition as the within-group factor (ie, competitive (CBS), competitive (CTPE), training), was applied to test for differences across the variables, with post-hoc Bonferroni comparisons where appropriate. Significance was set at p<0.05. All tests were performed with SPSS V.22 (SPSS Inc, Chicago, USA).
Results
Kinematic analysis
There were no significant differences in kinematics for any spinal region between the two engagement sequences during competitive scrummaging (p>0.05). Table 2 presents the mean peak motion data for the two scrum engagement sequences.
Mean (SD) data describing the ROM for each sequence
Significantly greater ROM was identified in the upper three spinal segments in both competitive sequences, versus the training (machine scrummaging) scenario. No significant differences (ie, p>0.05) were evident in the two lowest spinal regions.
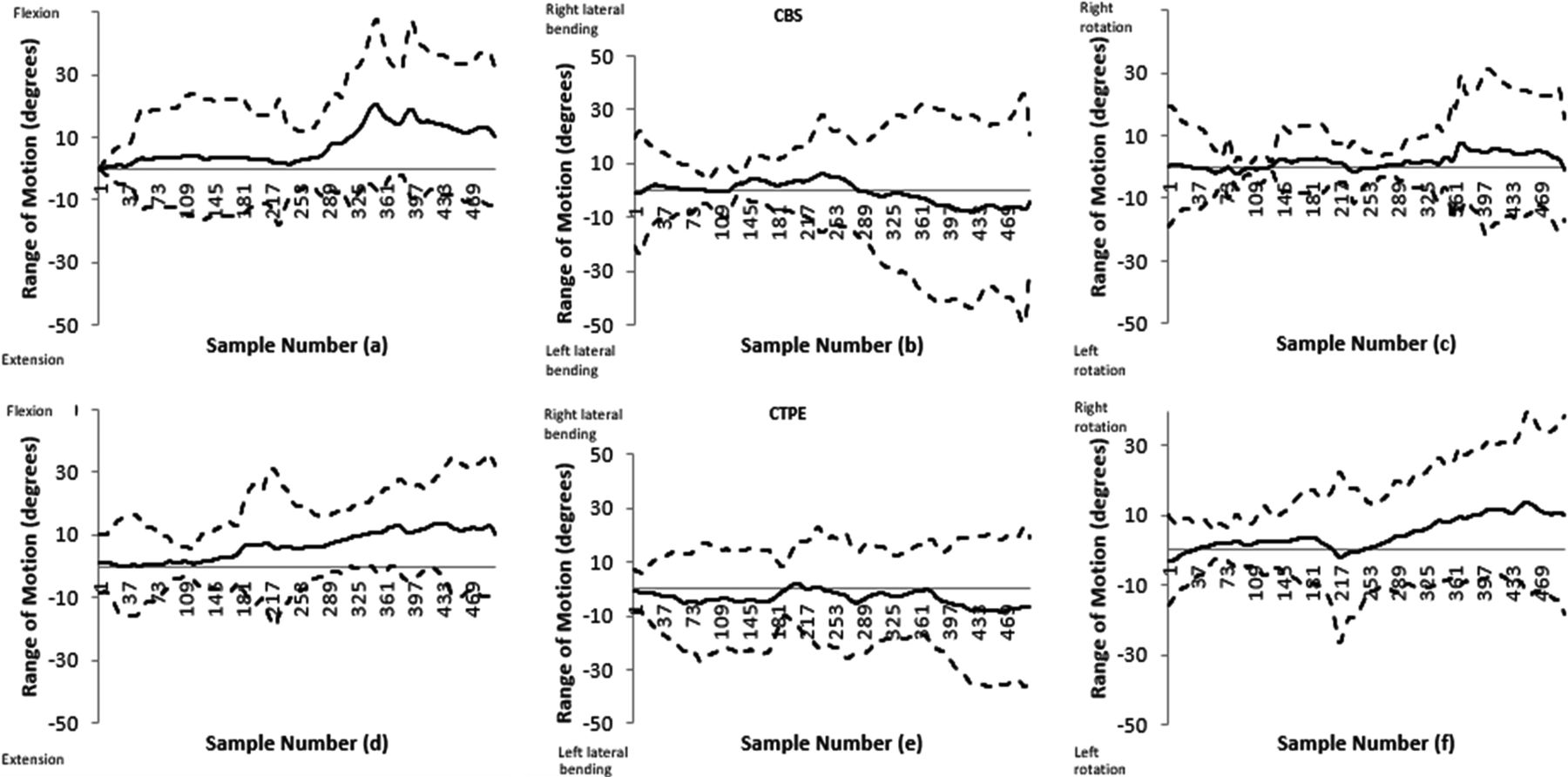
Data presented in figures 2A–C provides dynamic cervical ROM across the competitive CBS scrum scenarios, describing the flexion-extension, lateral bending and rotation left to right, respectively. Figures 2D–F describe equivalent data from the older CTPE engagement sequence. In each case, data has been time normalised and combined to yield a confidence corridor for ROM during scrummaging. The solid line represents the cohort mean and the dotted lines represent the upper and lower 95% CIs.
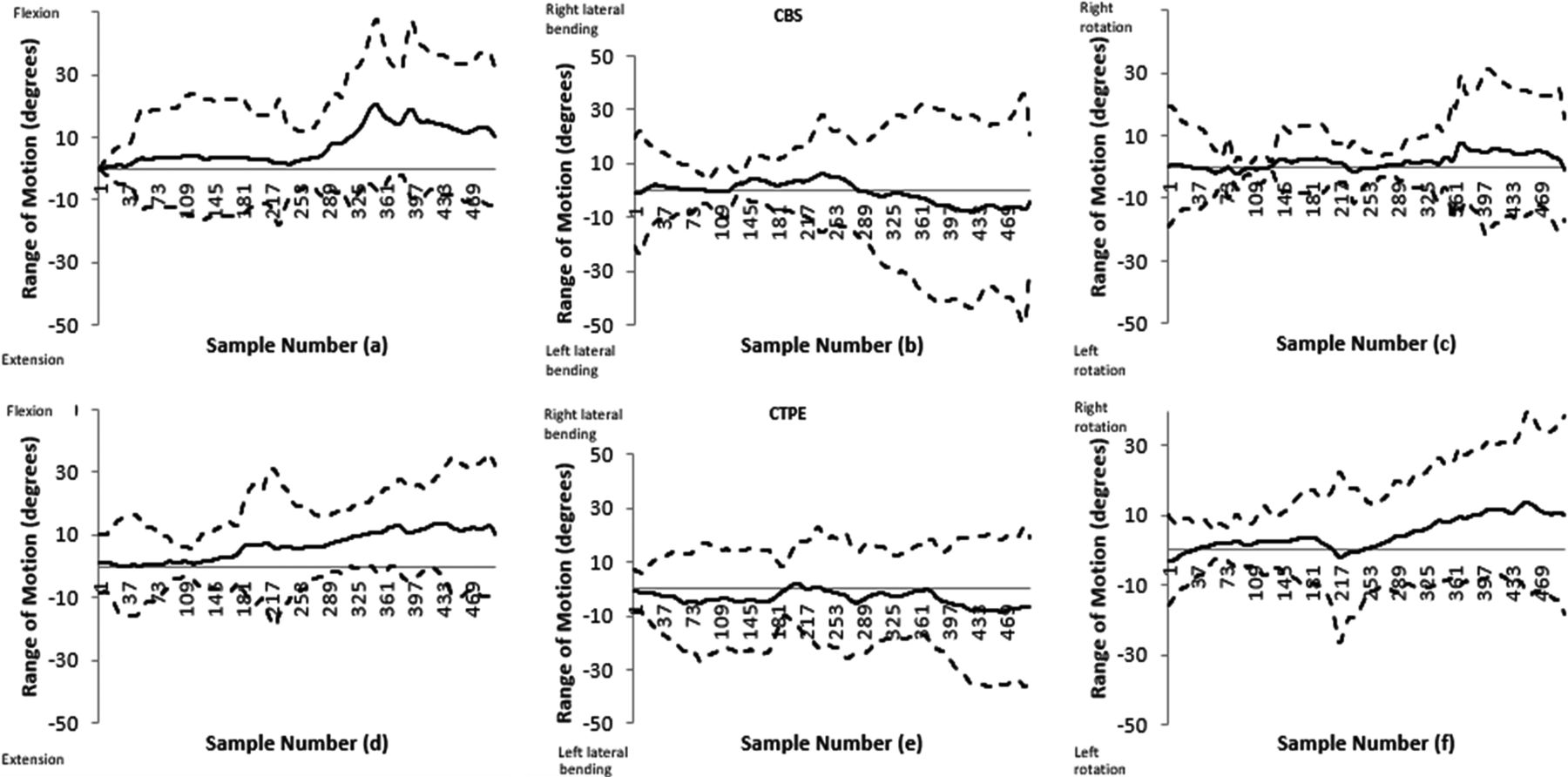
Dynamic cervical spine ROM during competitive (CBS and CTPE) training scrums. Solid line=mean; dashed lines= upper and lower 95% CI limits. CBS figures—(a: flexion/extension, b: lateral bending, c: rotation); CTPE figures—(d: flexion/extension, e: lateral bending, f: rotation). CBS, Crouch-bind-set; CTPE, Crouch-touch-pause-engage; ROM, range of motion.
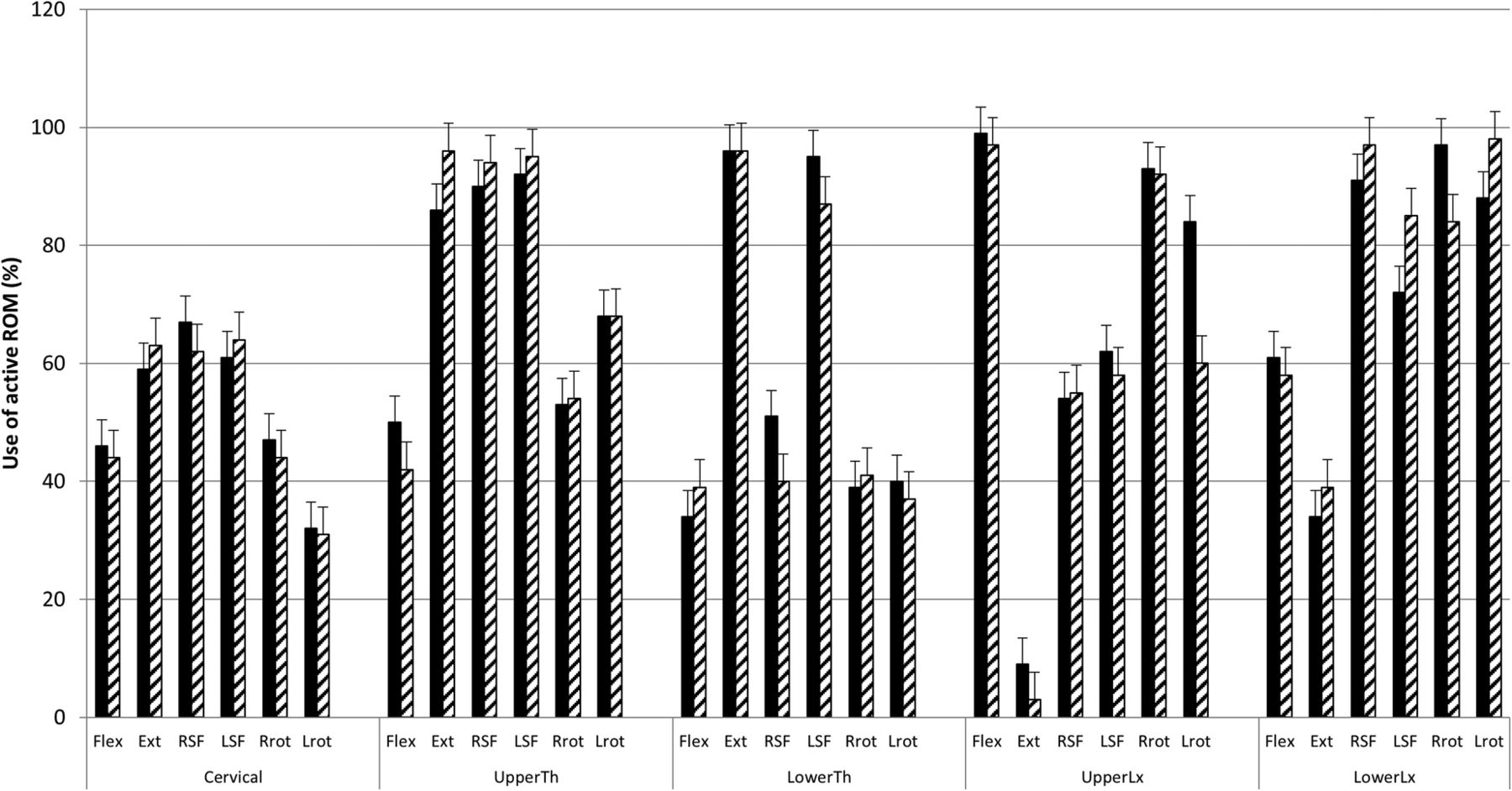
ROM relative to maximal ROM (figure 3) demonstrated no significant difference between scrummaging sequences (p>0.05). It did, however, identify that almost all available ROM was used for a number of spinal regions.
{kind=link}
{kind=link}
{kind=link}
The relative proportion of active ROM used during competitive scrummaging per spinal region, averaged across the cohort. Black columns = CTPE; Hatched columns = CBS. Error bars represent SE. CBS, Crouch-bind-set; CTPE, Crouch-touch-pause-engage; ROM, range of motion.
Discussion
This study set out to determine whether the evolution of rugby laws relating to the scrum had any effect on hooker spinal kinematics during competitive scrums. The results presented here indicate that the changes in laws do not have any significant effect on hooker spinal kinematics when comparing between the CBS (new) and CTPE (old) scrummaging sequences. There were some kinematic differences between training and competitive scrummaging trials but only for the upper spinal regions. This study performed the first multiregional spinal analysis, generating data that enhances our understanding of spinal kinematics within both a training and competitive environment, and using the new and old scrummaging sequences.
Previous studies have demonstrated that CBS engagement has significantly influenced the biomechanics of scrummaging.31 ,48 Indeed, growing evidence exists that the impact of engagement is reduced using CBS, as measured by the impact to the shoulder girdle in both machine,49 and live48 ,50 scrummaging. This was attributed to a reduced distance between front-row players prior to the impact phase. The current study did not measure the impact phase specifically, nor impact at the shoulders. Instead, we sought further understanding of the law change on other biomechanical measures. To this end, the findings of the current study do not support or refute the recommendations to move to the new laws, though synthesising all available data would suggest that the new laws result in reduced shoulder impact, and do not negatively influence spinal kinematics.
The data presented in this study demonstrated no difference in spinal ROM across the scrummaging sequences. The extent of spinal motion varied across the population, and appeared to be dependent on both the participant and the nature of the scrum. The particularly large variability observed in the cervical ROM (figure 2) would indicate that intrinsic control of ROM is the main determinant of kinematics during scrummaging; hence, it could be extrapolated that spinal kinematics may not be readily influenced solely by evolving scrum laws. It is also noted that approximately 60% of total sagittal ROM was utilised during scrummaging, suggesting that both sequences (CBS and CTPE) represent a relatively low risk of hyperflexion for most participants, a mechanism believed to be linked to catastrophic injury.51 It may be that catastrophic hyperflexion injuries are the sole domain of the collapsed scrum; however, a more substantive claim can only be levied on observing a greater number of scrums.
Our data also indicated that machine scrummaging utilised significantly less ROM for the upper spinal regions, which is consistent with reports of less cervical muscle demand of machine versus live scrummaging.32 Combining this data seems to suggest that machine scrummaging requires significantly less cervical and upper thoracic ROM, and less cervical muscle activity; hence, this appears to be an environment which poorly reflects the true cervical demands of live scrummaging. Indeed, knowledge of this less-intense environment may prove a useful addition to the rehabilitation pathway following cervical injury, while also highlighting the importance of additional conditioning prior to competitive scrummaging.
Reducing chronic injury from the scrum environment is complex. Greater or excessive spinal motion is associated with chronic degeneration in all regions of the spine,52 ,53 thereby leading to conclusions regarding reduced ROM being beneficial for chronic injury potential. Indeed, we observed only a modest range of cervical motion (63% of total available range), suggesting that excessive motion may not be the main source of degenerative change in the cervical spines of front-row players. For a front-row player to constrain motion in an oppressing environment requires significant muscle activity. Such muscle activity would, of course, result in a cost of compressive load, also known to be linked to chronic degeneration.54 The relatively modest cervical ROM observed in this study may be the result of a large amount of ‘stabilising’ muscle forces, where the demands of the dynamic competitive scrum see the hooker attempt to minimise head displacement. To this end, the greater muscle activity noted in previous CBS studies32 would indicate relatively high compressive loads on the cervical spine.54 This may provide some explanation as to the relationship between scrummaging and long-term degenerative changes in the cervical spine.
Scrummaging utilises a greater proportion of thoracic and lumbar spine ROM, versus cervical spine ROM. Indeed, over 90% of the available range was used during extension and lateral bending in the thoracic spine, flexion for the upper lumbar spine, and side bending and rotation for the lower lumbar spine. This is significant, as end-range spinal positions may result in reduced muscle activity,55 altered muscle function,56 increased load on the passive osteoligamentous spine,57 and increased risk of tissue damage.46 Indeed, reduced tissue compliance and bony opposition associated with end-range, negatively influences the available motion in other planes;58 ,59 hence, the use of such large proportions of the available range may expose the thoracic and lumbar spine to greater risk of injury.60
In performing the first multiregional spinal kinematics evaluation of the hooker within the rugby union scrum, this study is unique in presenting the greatest detail of spinal kinematic data. This analysis revealed that, when considering the relative motion of the five spinal regions, there was statistically insignificant kinematic variation between the new (CBS) and old (CTPE) sequences. This study adds to the debate surrounding scrummaging, by using novel methods to report the first spinal kinematics from within a competitive environment. Our data does not, however, support the notion that the new scrum laws will succeed in reducing chronic spinal injury.
Limitations of the current study include that it was conducted during training, which is unlikely to represent an identical biomechanical loading pattern to the more aggressive and physical nature of a competitive match. No detail regarding the specific phases of scrummaging were captured; therefore, it was not possible to relate specific ROM to specific scrum phases. Owing to the sampling frequency of data capture, it was not possible to report on the impact forces experienced at the spinal regions, although this was not the primary aim of our study.
Conclusions
Our data indicates that the scrum engagement sequence does not affect spinal kinematics of the hooker during competitive scrummaging. Machine scrummaging results in less ROM for the upper spinal regions compared to competitive scrummaging. Approximately 60% of available flexion ROM of the cervical spine was used during competitive scrummaging, whereas the lumbar spine utilised the entire ROM. Our data adds to the debate that influencing spinal kinematics within the scrum may require more drastic changes in law, owing to an individual's intrinsic control of motion.
Acknowledgments
The authors would like to acknowledge all the participants who volunteered for this study without whom it would not have been possible. Furthermore, the authors would like to declare that there is no conflict of interest.
References
Footnotes
Competing interests None declared.
Ethics approval Cardiff School of Engineering Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.