Article Text

Abstract
Background Low back pain is one of the most prevalent musculoskeletal conditions in the world. Many exercise treatment options exist but few interventions have utilised free-weight resistance training. To investigate the effects of a free-weight-based resistance training intervention on pain and lumbar fat infiltration in those with chronic low back pain.
Methods Thirty participants entered the study, 11 females (age=39.6±12.4 years, height=164 cm±5.3 cm, body mass=70.9±8.2 kg,) and 19 males (age=39.7±9.7 years, height=179±5.9 cm, body mass=86.6±15.9 kg). A 16-week, progressive, free-weight-based resistance training intervention was used. Participants completed three training sessions per week. Participants completed a Visual Analogue Pain Scale, Oswestry Disability Index and Euro-Qol V2 quality of life measure at baseline and every 4 weeks throughout the study. Three-dimensional kinematic and kinetic measures were used for biomechanical analysis of a bodyweight squat movement. Maximum strength was measured using an isometric mid-thigh pull, and lumbar paraspinal endurance was measured using a Biering-Sorensen test. Lumbar paraspinal fat infiltration was measured preintervention and postintervention using MRIs.
Results Postintervention pain, disability and quality of life were all significantly improved. In addition, there was a significant reduction in fat infiltration at the L3L4 and L4L5 levels and increase in lumbar extension time to exhaustion of 18%.
Conclusions A free-weight-based resistance training intervention can be successfully utilised to improve pain, disability and quality of life in those with low back pain.
- Back injuries
- Biomechanics
- MRI
- Fat percentage
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Free weight resistance training is effective in rehabilitating patients with chronic low back pain.
Lumbar paraspinal muscle fat infiltration was significantly reduced following free weight resistance training without isolated lumbar extension exercise.
The biomechanics of the squat movement were altered following the intervention.
Introduction
Chronic low back pain (LBP) is a prevalent musculoskeletal diagnosis affecting a broad range of ages and educational and income levels; a mean prevalence rate of 18.1% has been reported in the literature.1 Existing classification systems demonstrating the wide range of possible symptoms highlight the complexity of the condition and offer a method of categorising patients by pathology and or psychological and social factors.2
In LBP cases where surgery is not appropriate, genetic, psychological, social and physical factors need to be considered as part of a biopsychosocial approach to treatment.3 When considering physical factors, exercise interventions have been recommended as a conservative treatment.4 ,5
In instances where pathology results in neurological deficit or pain, surgical intervention may be considered. These interventions include fusion for LBP due to disc degeneration, discectomy for radicular symptoms due to disc herniation or bulging and laminectomy for symptomatic stenosis.6 Another treatment for radicular symptoms is transforaminal steroid injection which has mixed outcomes.7
Multiple non-surgical interventions are described.8 It has been suggested that resistance training (RT) is an effective intervention that may obviate the requirement for injection or surgery. The evidence for RT in musculoskeletal rehabilitation9 demonstrates greater effectiveness than aerobic, coordination, mobilisation or Pilates training.10 ,11
Compensatory motor patterns have been associated with chronic LBP during completion of sit to stand tasks.12 It is recommended that treatments seek to restore normal kinetic and kinematic characteristics. It has also been demonstrated that individuals with LBP and greater pain-related fear change movement patterns in an effort to reduce lumbar spine motion during some tasks.13 While the use of RT may alter the fear-related aspects of LBP,14 limited support has been presented for the ability of rehabilitation interventions to change movement patterns.15 No research into the effects of free weight RT on biomechanics in those with LBP could be found.
It is common for those with LBP to undergo plain X-ray imaging, CT or MRI to delineate anatomical pathology.16 MRI provides accurate imaging of disk and neural tissue, bony stress and other soft tissue, in particular, muscle. Higher levels of MRI-defined lumbar fat infiltration and smaller paraspinal cross-sectional areas have been observed in those with LBP.17–20 This muscular atrophy occurs through a number of different cellular and molecular pathways and can be caused by inactivity.21 Willemink et al22 published the sole study examining alterations in MRI defined lumbar fat infiltration following training. No significant muscle structure changes were seen.
The use of free weight exercises is commonplace in the training of athletes and is considered effective in increasing strength, altering muscle structure and improving motor control.23 Despite deficiencies in these areas having been linked to LBP,12 ,24 the use of free weight RT in the rehabilitation of those with LBP is limited. It is known that RT can alter muscle composition and illicit high levels of lumbar erector and other posterior chain muscle activity.25 ,26 However, it is unknown what effect a free weight RT intervention has on MRI defined lumbar fat infiltration, biomechanics and pain in those presenting with LBP.
The aim of the current study is to investigate the effects of a free weight-based progressive RT intervention on pain, disability, quality of life, MRI-defined lumbar fat infiltration and functional cross-sectional area (FCSA), squat biomechanics and strength in those with chronic LBP.
Methods
Participants
Participants had presented with LBP to one of six sports physicians at a large sports medicine practice. All participants underwent clinical history and examination by a sports physician including MRI examination. The symptoms had been present for greater than 3 months, with or without radicular pain. Exclusion criteria were: previous spinal surgery, tumours, nerve root entrapment accompanied by neurological deficit, spinal infection, inflammatory disease of the spine and other disorders preventing active rehabilitation. Those who met the inclusion criteria were informed of the study, given an information leaflet and offered the opportunity to ask questions of the lead researcher. All participants completed and signed an informed consent form prior to partaking; the study met the approval of the Sports Surgery Clinic Hospital Ethics committee (25-EF-008).
Thirty participants, 11 females (age=39.6±12.4 years, height=164 cm±5.3 cm, body mass=70.9±8.2 kg,) and 19 males (age=39.7±9.7 years, height=179±5.9 cm, body mass=86.6±15.9 kg,) between the ages of 16 and 60 were recruited. There were four dropouts due to: an unrelated ankle injury (n=1), not attending all testing sessions (n=1), work commitments (n=1) and a lack of adherence to the programme (n=1).
Procedures
On entering the laboratory, participants were asked to fill out disability, pain, activity level and quality of life questionnaires; the Oswestry Disability Index (ODI); Visual Analogue Scale (VAS); a Godin-Shepherd Leisure-time Questionnaire and a Euro-QOL-5D V.2 (Euro-Qol) questionnaire were used, respectively. A flow chart of the testing, questionnaires and training can be seen in online supplementary content 1 and 2. An 8-camera motion analysis system (Bonita B10, Vicon, UK), synchronised with two 40×60 cm force platforms (BP400600, AMTI, USA) was used to collect kinematic and kinetic data for all tests. Data were sampled at 200 Hz and the Vicon Plug-in-Gait marker set was used as per Marshall et al.27
Supplementary content 1
Supplementary content 2
Ankle, knee, hip, pelvis and thorax angles and internal joint moments at the hip knee and ankle were calculated throughout the movement in all three planes. Angles were normalised to a standing static trial.28 A continuous waveform analysis, Analysis of Characterising Phases,29 was conducted to examine differences between the measurements. Before performing ACP, waveforms were landmark registered to the start of the concentric phase. This was done to remove temporal variations in the start of the concentric phase30 between the participants. Subsequently, ACP was applied to generate participant scores to describe a participant's behaviour over key phases (phases of variation). Participant scores were tested for significant differences using an analysis of variance (ANOVA). If participant scores differed within a key phases, phases were extended to discover the full phase of significant difference.29
Biering-Sorensen test protocol
A Biering-Sorensen (BS) test was used to measure back extension endurance.31 The patient lay on the examining table in the prone position with the upper edge of the iliac crests aligned with the edge of the table. The lower body was fixed to the table by two straps, located around the pelvis and mid-calf. With the arms folded across the chest, the patient was asked to isometrically maintain the upper body in a horizontal position (see online supplementary content 3). The time during which the patient kept the upper body straight and horizontal was recorded.
Supplementary content 3
Isometric mid-thigh pull strength test protocol
Isometric mid-thigh pull (IMTP) tests were completed using a custom set up with the laboratory force plates (Fit-tech, Australia, see online supplementary content 4). Testing protocol can be seen in online supplementary content 2. The IMTP was not included in the first testing session as a maximum isometric strength test was deemed inappropriate in an initial testing battery for those with LBP. To calculate maximum force, vertical ground reaction force (vGRF) data from both force plates were summed before the maximal vGRF was identified. This measure was then normalised to body weight (N/kg).
Supplementary content 4
MRI protocol
Lumbar spine MRIs were obtained at initial clinical assessment on entering the study (table 1) and following intervention. These were used to measure fat infiltration of the lumbar paraspinal musculature. The majority of images were obtained using a 3 T MRI system (GE Signa, General Electric Healthcare, USA). Five participants provided images completed on a 1.5 T MRI system. Axial T2 weighted non-fat-saturated sequences were used for evaluation. Fat infiltration and, where possible, FCSA (defined as the fat free area) was measured at the lower end plate at the L3L4, L4L5 and L5S1 levels. The region of interest was defined as the area of erector spinae and multifidus musculature32 ,33 and percentage fat infiltration was calculated for the total area using a standalone graphical user interface developed in Matlab R2010a34 (see online supplementary content 5). Intrauser reliability in selecting the region of interest and changes in signal intensity was tested using 60 images on two occasions, 2 days apart.
Supplementary content 5
A list of radiology reported MRI diagnoses on entering the study at L3L4, L4L5 and L5S1 levels and the number of times they were reported across all participants
Disk herniation includes reported: disk prolapses, disk protrusions, disk bulges, annular disk tears and annular fissures with or without a reported nerve compression. Facet joint degeneration includes reported degeneration and facet joint osteophyte formations.
Experimental intervention
After initial testing, participants were instructed regarding their training programme. During a 1 h gym session, participants were first asked to explain their beliefs around the causes of their pain to address psychosocial aspects that are a component of LBP.35 Any areas where it was felt that their beliefs were contributing towards their back pain were addressed (see online supplementary appendix 3). The exercises were delivered across two sessions (see online supplementary appendix 1). The 10RM and 6–7RM loads were estimated by the participant and adjusted where necessary at the end of each set. Emphasis in each of the exercises was placed on maintaining a neutral lumbopelvic position. In participants who were unable to prevent lumbar flexion when deadlifting off the floor, the bar was raised to a level in a squat rack where a straight back could be maintained. Participants were given a booklet containing their training programme and recorded missed sessions by crossing them out. Reported adherence was high with a mean of 2.1 missed sessions from a possible 48.
Coaching cues and support
Participants were filmed (iPad 3, Apple inc) completing their exercises with a commentary of the coaching points and given access to those videos online using Dartfish video analysis software (Dartfish, USA). Externally focused coaching cues were used to maximise skill acquisition and learning36; these are listed in online supplementary appendix 4.
Outcome measures of interest were pain VAS, ODI and Euro-Qol, peak vGRF) during IMTP, lumbar extensor time to exhaustion, percentage fat infiltration and cross-sectional area of lumbar paraspinals at L3L4, L4L5 and L5S1 levels, and kinetic and kinematic variables about the ankle, knee, hip and torso throughout a bodyweight squat.
Statistical analysis
All values were reported as mean, SD and 95% CI (for parametric data) (mean±SD CI), and percentage change following intervention. All data were checked for normality using a Shapiro-Wilk test. Parametric data were assessed using a paired samples t test and a repeated measures one-way ANOVA with Bonferroni adjusted post hoc pair-wise comparison. Non-parametric data were assessed using a Wilcoxon-Signed rank test. A p level of <0.05 was adopted for statistical significance. Intraclass correlation coefficients were used to examine intrauser (ICC [3 1]) reliability of measuring lumbar fat infiltration. The ICC classifications of Fleiss37 were used to describe the range of ICC values where less than 0.4 was poor, between 0.4 and 0.75 was fair to good, and greater than 0.75 was excellent. All statistical analyses were performed using IBM SPSS (V.21; IBM, New York, New York, USA).
Results
Pain, disability, quality of life, strength and endurance
The participants showed significant improvement in ODI, pain VAS and Euro-Qol scores at weeks 4 and 16 compared to baseline (table 2). The BS test scores showed significant increases between baseline and week 16. No significant improvement (p=0.08) was seen in maximum isometric strength.
Pain, disability, quality of life, isometric strength and endurance (mean±SD, 95% CI)
Fat infiltration
Significant reductions in percentage fat infiltration were seen bilaterally at L3L4 and L4L5 levels from preintervention to postintervention (table 3). No significant changes were seen at the L5S1 level. Significant increases in FCSA were seen bilaterally at L3L4 and L4L5 levels from preintervention to postintervention (table 4). The ICC was calculated at 0.97 giving an excellent level of intrauser reliability.37
Mean percentage fat infiltration±SD, 95% CI of the lumbar paraspinal muscles
Functional cross-sectional area (mm2)±SD, 95% CI of the 15 participants who had pre and post MRIs
Biomechanics
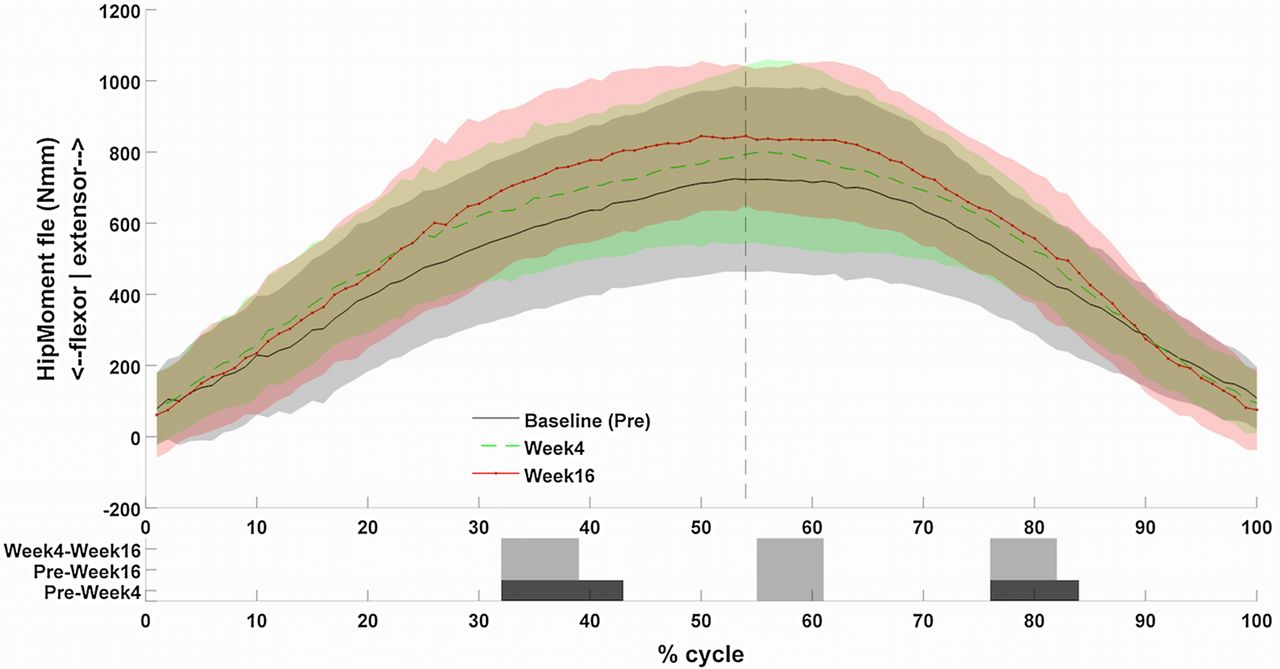
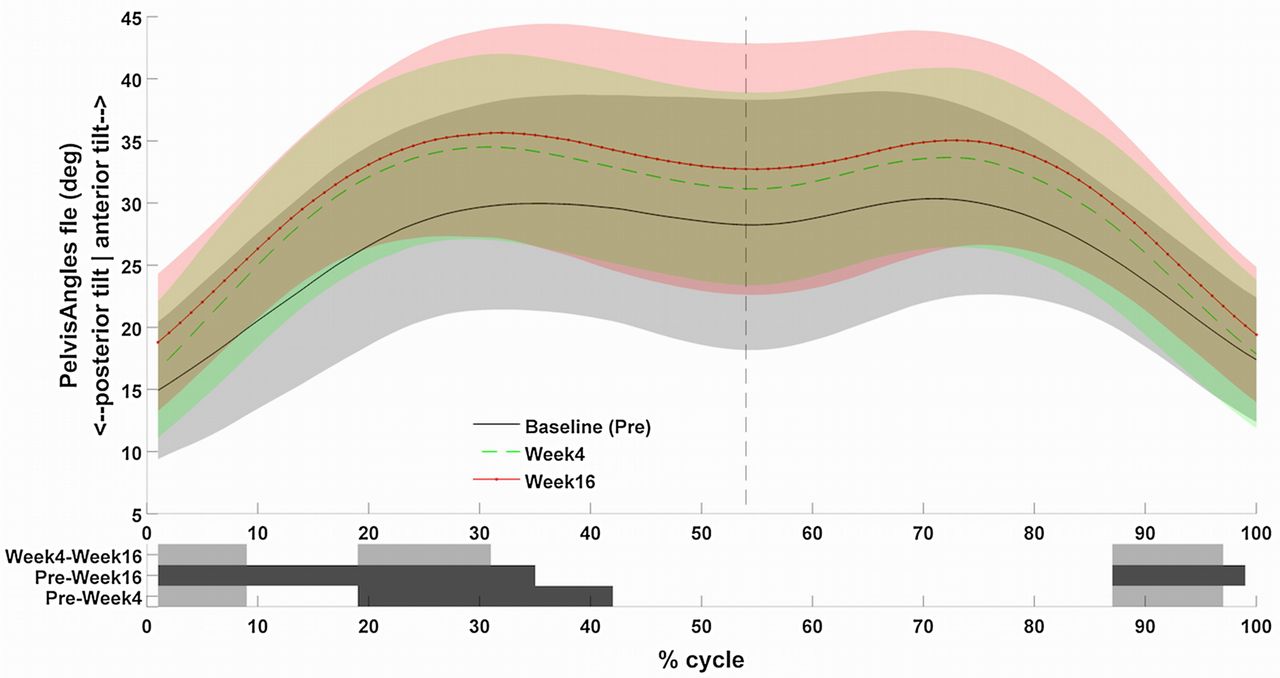
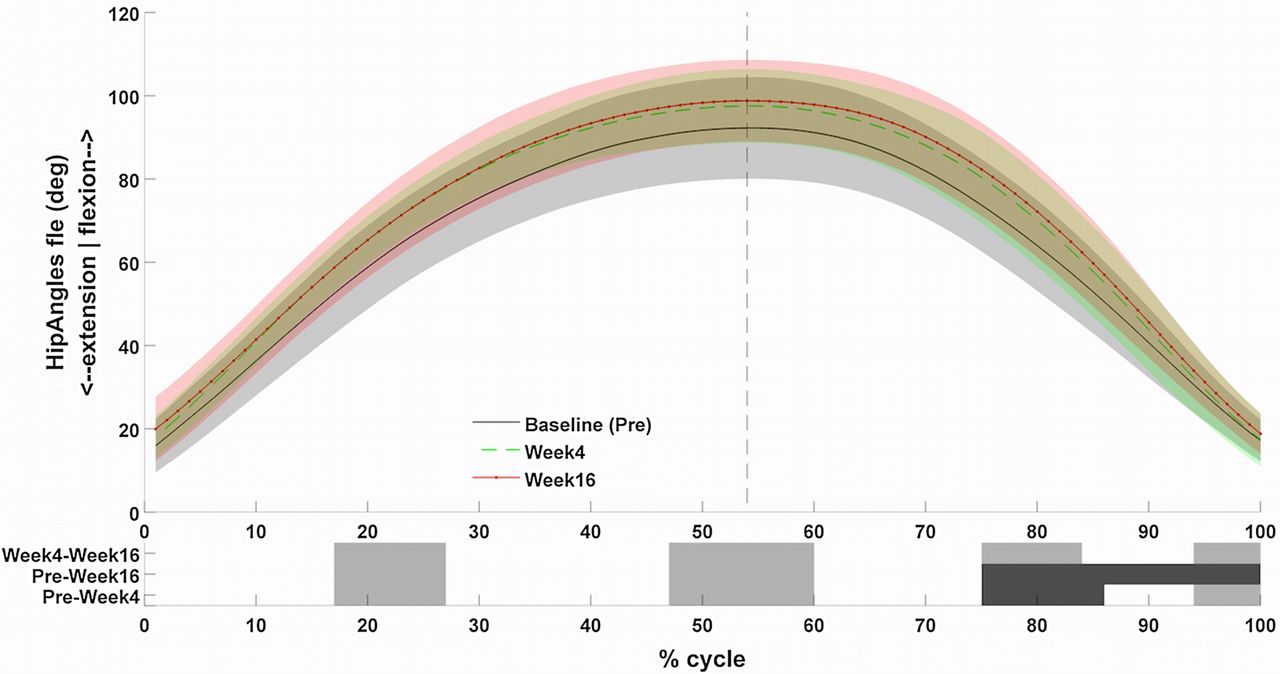
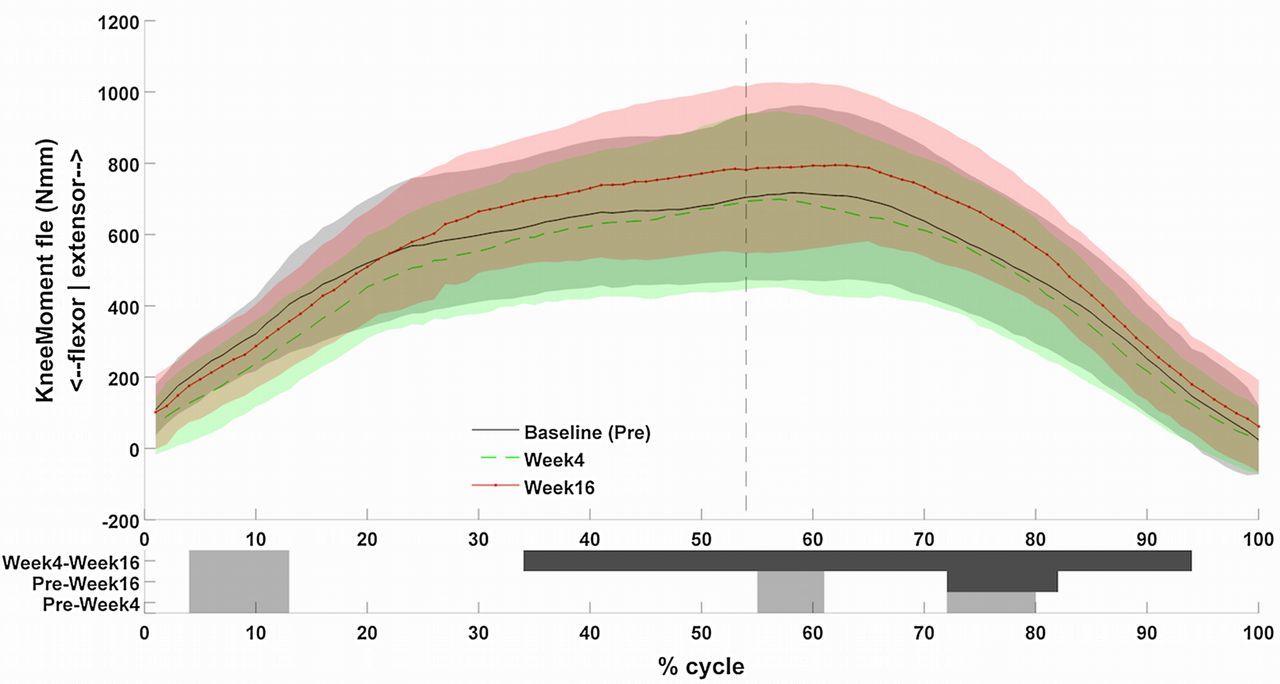
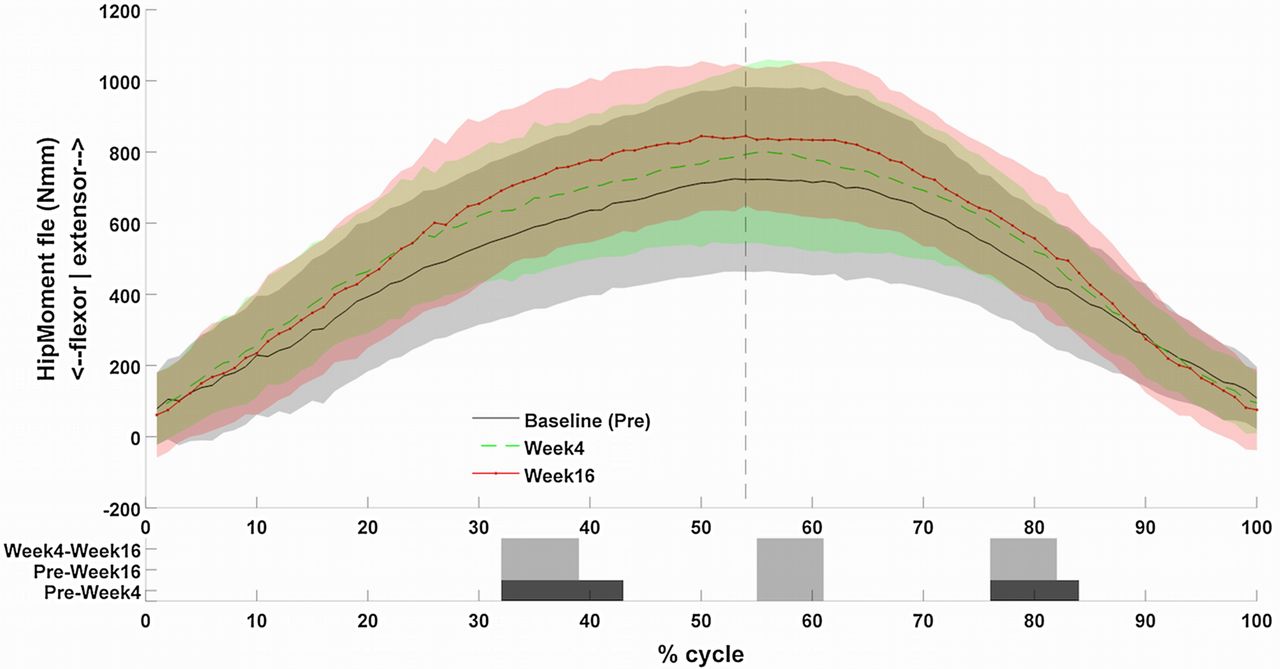
Significant increases in centre of mass vertical velocity, pelvis tilt angle, hip flexion angle, knee moment and hip moment were seen throughout the waveforms (figures 1⇓⇓⇓–5). No significant differences in ankle, knee, thorax and thorax to pelvis angles were seen. The reader should note the differences in knee, thorax to pelvis angle were close to significance.

Waveform of the vertical centre of mass velocity (mm/s) throughout the squat movement. Dark grey indicates areas of significant difference and lighter grey indicates significance before correction.

Waveform of the pelvis angles (degrees) throughout the squat movement. Dark grey indicates areas of significant difference and lighter grey indicates significance before correction.
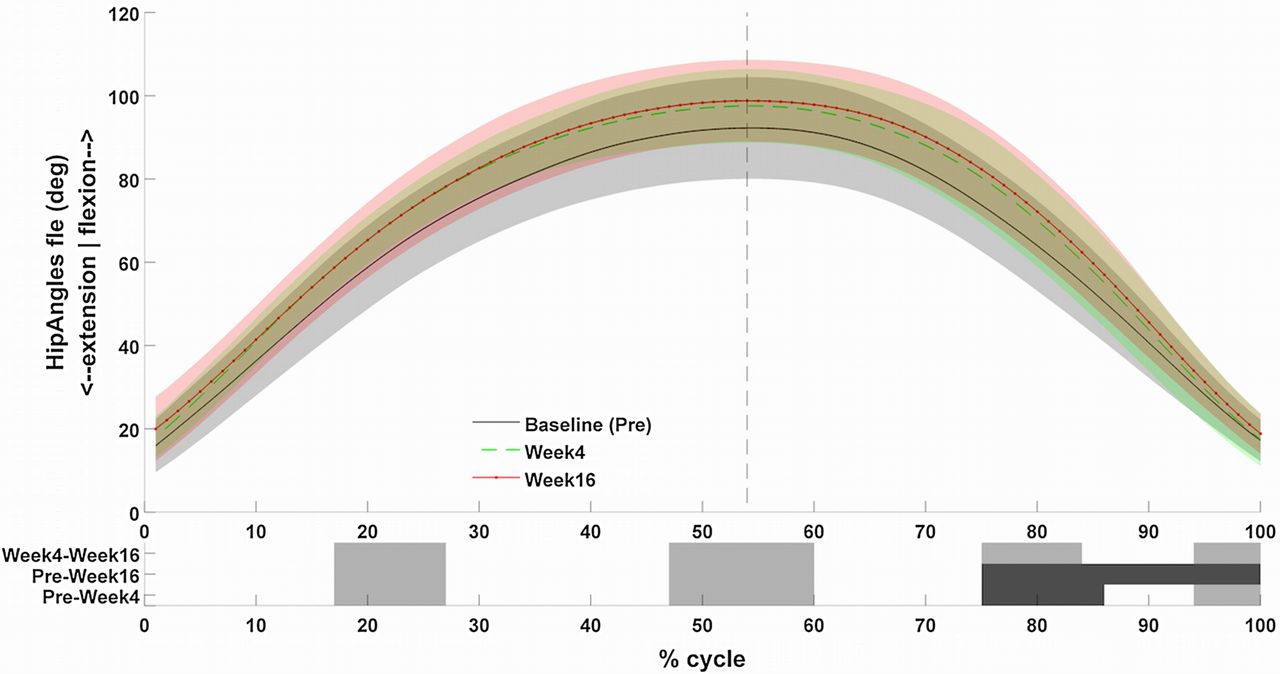
Waveform of the hip angles (degrees) throughout the squat movement. Dark grey indicates areas of significant difference and lighter grey indicates significance before correction.
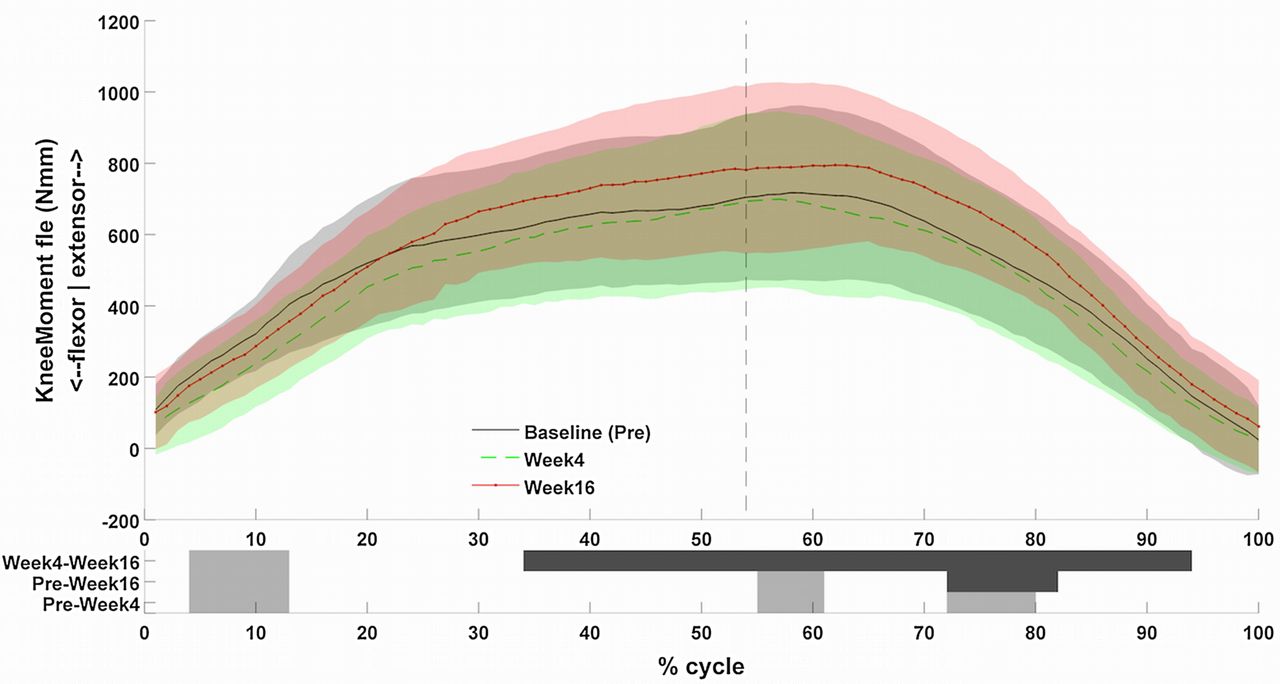
Waveform of the knee moment (Nmm) throughout the squat movement. Dark grey indicates areas of significant difference and lighter grey indicates significance before correction.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Waveform of the hip moment (Nmm) throughout the squat movement. Dark grey indicates areas of significant difference and lighter grey indicates significance before correction.
Discussion
This study demonstrates significant reductions in pain and disability (72% and 76% respectively) in patients with comorbidities presenting with LBP following a 16-week RT programme. These changes are large compared to other whole body RT interventions where positive impacts on mean pain scores (26%,38 39%39) and disability (46%,38 40%39) have been described. The presence of a lower baseline disability level of the participants (22.9±1.2 vs 43.1±3.338 40.4±2.439), but similar baseline pain level, was noted. While it could be suggested the greater the levels of modifiable disability present, the greater the chance for possible enhancements, the opposite was seen.
Associations have been made between fear avoidance beliefs and LBP40 and it has also been shown that those with LBP demonstrate protective guarding behaviour.12 This represents a freezing of degrees of freedom which is seen in early skill acquisition41 and is achieved by stiffening up surrounding musculature.42 Higher levels of fat infiltration and reduced cross-sectional areas of the lumbar paraspinals have also been linked with LBP.17–20
The present intervention differed from comparable RT studies38 ,39 by addressing patient beliefs which has been suggested can increase patient activity levels43 potentially breaking down belief based barriers to the RT. It utilised external cueing to enhance motor learning44 and free-weight exercises with higher intensity loading (75–83% RM vs 55–83% RM) to maximise the motor control challenge23 and mechanical stimulus. Adaptations to this type of RT include altered agonist antagonist coactivation patterns,45 or an un-freezing of degrees of freedom, and muscle hypertrophy.25 It is possible that the combined effect of these differences led to larger improvements in pain and disability.
Biomechanics
Increased velocity was observed throughout the squat movement mirroring the findings of Shum et al.46 They found significantly higher velocities in asymptomatic participants during sit to stand movements suggesting that slower movements were used to prevent provocation of pain. Muscle guarding patterns such as reduced speed have been listed as a movement impairment for those with LBP.3 The increased hip flexion and pelvis tilt angles occurred as a result of the RT cueing aimed at reducing the lumbar flexion and active extension patterns that have been associated with LBP.3
To the author's knowledge, this is the first study to demonstrate altered motor patterns in those with LBP using free weight RT. Moreover, these alterations moved participants towards the increased movement velocities seen in asymptomatic populations.46 Future work could utilise electromyography to observe changes in muscle recruitment patterns.
Paraspinal fat infiltration and FCSA
The reduction in fat infiltration and increased FCSA observed in the lumbar paraspinals are in line with changes found elsewhere as a result of RT.47 ,48 These changes, the opposite of which have been associated with LBP,18 ,20 ,49 may have enhanced force generation capabilities in this area50 improving load tolerance and contributing to reduced pain as has previously been observed in RT interventions.51
Changes in fat infiltration and FCSA were seen at the L3L4 and L4L5 levels but not at the L5S1 level. It was noted that percentages of fat infiltration were much higher at L5S1 than those above preintervention and postintervention. This may suggest that a higher fat content at L5S1 is a relatively normal state thus limiting the scope for improvement, that higher levels of fat infiltration are more resilient to change or that the level of loading may have been lower in this region. These possibilities require further investigation.
Strength
A significant improvement in strength endurance during the BS test was observed in line with other studies.39 This is indicative of an increased ability to resist lumbar flexion which, when viewed with the changes in fat infiltration, suggests improved conditioning of the lumbar extensors, a deconditioning of which has been suggested as a risk factor for LBP.24
This intervention applies many of the concepts that would be commonplace in training sporting populations, including progressive overload and high intensity RT52 with the aim of changing the way the participant moves. This study demonstrates that it is possible to impact many of the factors that have been suggested to contribute to LBP by applying basic RT practices.
An interesting finding is that no significant increase in IMTP strength was seen despite participants observed to be lifting greater loads dynamically throughout the intervention. It is possible that the increases in loads lifted in the exercises were as a result of neural changes, common in RT,45 ,53 specific to each exercise. Therefore, despite enhanced skill acquisition, the loads may not have reached levels where absolute maximum IMTP strength could be improved. However, it should be noted from an ecological validity perspective that most daily activities that involve high levels of lumbar muscular loading are likely to be dynamic rather than isometric.
Limitations
Two different MRI lumbar spine protocols were utilised as a number of participants had existing 1.5 T MRIs at presentation. To prevent unnecessary repeat imaging, these were not duplicated. The 1.5 T imaging came without the pixel-spacing values necessary to compare FCSA between different images.
The study was a cohort design, and while the inclusion of a comparison cohort would have added strength to the results, this was a pilot intervention and as such future work may be used to determine effectiveness relative to other interventions.
Conclusions
This study demonstrates that 16 weeks free weight RT addressing strength, motor control and physiological aspects is effective in participants with chronic LBP. This is the first study to identify changes in fat infiltration as an objective marker of improvement and highlights that changes are possible across comorbidities. Positive outcomes including reduced pain and disability, improvement in quality of life, strength endurance and lumbar paraspinal muscle quality in patients with LBP were seen, whereas changes in maximum strength were not observed as expected.
References
Footnotes
Twitter Follow Neil Welch at @nwconditioning
Contributors NW is the lead author, who designed, organised and conducted the study also drafting the final article. KM is PhD supervisor to NW and contributed to the design and drafting of the experimental write up. JA designed the software used for analysis of lumbar fat infiltration specifically for use in this study. CR analysed all of the biomechanical data and authored the biomechanical section of the methodology. JC is the radiologist involved with the study providing radiological reporting and analysis and writing the MRI section of the methodolgy. EF and AF-M were involved in recruitment of participants and study design. All authors were involved in drafting and revision of the final article.
Funding This study was funded by the Sports Surgery Clinic, Dublin and, additionally, NW, KM, JA, CR, BM received funding as part of INSIGHT by Science Foundation Ireland (SFI) under Grant Number SFI/12/RC/2289.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Sports Surgery Clinic Hospital Ethics committee.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.