Article Text

Abstract
Background Heart rate variability (HRV) can disclose the specific adaptation of sympathovagal modulation to exercise. This study investigated the change in HRV measures after anaerobic and aerobic intermittent exercises in university football and futsal players.
Method 36 male university students with physically active lifestyle (n=14), football (n=12), and futsal (n=10) participated in this study. The participants completed the repeated sprint ability (RSA) test and Yo-Yo (YY) intermittent recovery test level 1 in randomised order. ECG signals of the participants were recorded in supine position 15 min before and 30 min after exercises. Before exercise, and 5 and 30 min after exercise, the blood pressures were also taken.
Results In the RSA protocol, the percentage changes in normalised high-frequency power (nHFP) were significantly decreased, while the percentage changes in the very low/high frequency power ratio (VLHR) and low/high frequency power ratio (LHR) were significantly increased in futsal players after exercise, as compared with the controls. No significant changes in all HRV indices were found in the YY protocol, except the respiratory frequency.
Conclusions After exercise, the percent decrease in vagal modulation in futsal players was significantly reduced, while the percentage increase in sympathetic modulation in futsal players was significantly enhanced in the RSA test, but not in the YY test, as compared with the control group. The increase in sympathetic activity and the decrease in vagal activity in the futsal players were greater than the corresponding increase and decrease in the football players in the RSA test.
- Cardiology physiology
- Football
- Sports & exercise medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Measuring changes in the HR paces during rest or postexercise is an appropriate method to monitor individual adaptation of the ANS to sports training.
Professional football and futsal players improved sport-related exercise capacities associated with increased cardiac modulation of vagal tone after a preseason training and competitive season.
Evidence with a professional Brazilian futsal sample pool showed that the mature futsal players have better aerobic capacity and cardiac autonomic modulation than younger futsal players.
Introduction
The average exercise intensity of a football player in a football match is equivalent to 70–80% of his maximum oxygen consumption, and the average heart rate (HR) response of a football player in a football match lies between 165 and 175 bpm (about 80–90% of the maximum HR (HRmax)).1 ,2 Football players also need to recover quickly after a short-distance sprint as the exercise pattern in a match involves multiple sprints and high-intensity running. Mohr et al3 reported that the top-level football players covered 28% of high-intensity running distance and 58% of sprinting distance more than the low-level professional football players during a competitive season. In contrast, futsal players more frequently perform all-out sprint and a fast-paced movement than football players because of the rules and cramped space during a futsal game. The HR responses during a futsal match ranges between 170 and 190 bpm and the intensity of futsal competition is relatively high (above 85% of HRmax during the majority of match time).4 It has been suggested that futsal players cover more high-intensity running distance than do football players during a regular match (22.6% vs 10% of total covering distance in high-intensity running).1 4 Therefore, a greater physical demand in anaerobic performance is required in futsal players as compared with football players.
What this paper adds?
There was no significant difference in HRV measures and physical performance between university football and futsal players when anaerobic and aerobic intermittent exercise stresses were imposed.
The RSA exercise induced acute effects on vagal withdrawal during the 30 min postexercise period in university futsal players.
There was no significant difference in the cardiac autonomic nervous modulation between physically active university students and football and futsal players after the YY intermittent exercise.
The underlying mechanisms modulating the heartbeat pattern are mainly related to the neural regulation of the autonomic nervous system (ANS). One of the non-invasive methods used to assess the cardiac autonomic nervous modulation is to record the ECG signals, measure the intervals between consecutive R waves, and assess the HR response and variation in the R-R intervals (RRI) by using the power spectral analysis. The HR variability (HRV) obtained in this way can provide useful information to understand the intrinsic factors involved in cardiac modulation during exercise5 or physiological adaption after an acute and chronic training regime.6–8 Specific adaptation of a vagal-related HR change has been shown in professional futsal players after a preseason training7 ,9 or over a competitive season.10 A similar finding has also been observed in professional football players after 8 weeks of preseason training6 and during a competitive season.11 These studies suggested that the positive adaptation of autonomic nervous modulation was strongly associated with the improvement in repeated sprint ability (RSA) and Yo-Yo (YY) intermittent recovery test level 1 performance. For example, Soares-Caldeira et al has reported that there was about 25% reduction in the RSA decline rate and about 23% increase in the total covered distance of the YY test in association with an increase in the SD of normal R-R interval (SDRR), root mean square different of successive normal R-R intervals (rMSSD), and low-frequency power after 4 weeks of preseason training in Brazilian professional futsal players.9
Clearly, the physical, technical and tactical demands of the sports may contribute to the discrepancy in the anaerobic and aerobic capacities between football and futsal players. However, information regarding the physiological characteristics between these two sister sports is limited in the literature. Recently, we found increased vagal modulation, decreased sympathetic activation and lower resting HR in amateur football players than in sedentary adults.12 However, the participants in our study were measured without exercise-induced physiological stress. This limits our ability to understand the underlying mechanisms modulating the cardiac responses during different exercise modalities. Since the energy consumption during anaerobic and aerobic intermittent exercises requires different metabolism and cardiovascular regulation as a result of physiological stimuli,13 ,14 the aim of this study was to investigate the acute effects of RSA and YY exercises on the autonomic nervous modulation in university football and futsal players.
Methods
Participants
Thirty-six male collegiate students voluntarily participated in this study (control group: n=14; football group: n=12; futsal group: n=10). The participants with a football or futsal training background were recruited from the first division of a university championship in Taiwan, whereas the control participants were physically active collegiate students with a background of physical education (no football or futsal activity within a year). The first reason for using physical education students as the control group in this study was that they matched with the study groups (football and futsal groups) in terms of age, body figure, lifestyle, etc. The major difference among the control group and the study groups was football exercise. Although some control subjects were engaged in other kinds of sports such as volleyball, cycling, jogging, etc, they had no experience in regular football or futsal training. This specific difference made them suitable for studying the effects of football and futsal training on the body adaptations of the participants. The second reason was that the exercise intensity in the RSA and YY protocols was extremely high. Non-physically active participants were unable to complete the exercise protocols in our study.
While the frequency of a training session was four times a week, the duration of a training session was around 2 h in the football and futsal groups. The experiment was conducted during the precompetition period. The physical characteristics in all three groups are presented in table 1. A physical condition status screening questionnaire was used to identify the physical status and contraindication to participation in this study. The participants then signed a written consent form and undertook a familiarisation session. The study has been approved by the Institute Review Board of the hospital and was performed in accordance with the Declaration of Helsinki.
Physical characteristics of the participants
Exercise protocols
Aerobic exercise protocol
The validity and reliability of the YY test to assess the aerobic capacity in football and futsal players have been described elsewhere.13 ,15 ,16 The YY test consisted of 10 s of active recovery after each bout of shuttle running, a jogging distance of 5 m recovery zone, and repeated 20 m runs back and forth between the start and return lines with a gradually incremental speed. The speed of the shuttle running was controlled by digital audio bleeps from a laptop. The speeds of the first four bouts were 10–13 km/h (0–160 m) and those of seven other bouts were 13.5–14 km/h (160–440 m). Afterwards, the speed increased by 0.5 km/h after every eight bouts (ie, after 760, 1080, 1400, 1720 m, etc). The total covered distance was recorded when the participants failed to reach the start line in time twice.
Anaerobic exercise protocol
The RSA protocol consisted of a 20 m shuttle sprint repeated six times. A starting position was set 30 cm behind the starting line. The participants performed a 20 m all-out shuttle sprint with a 20 s rest interval. They were given two preliminary trials to familiarise themselves with the RSA followed by a 5 min rest. A passive recovery during a 20 s rest interval was allowed. A time gate system (Fusion Sport, Coopers Plains, Australia) was aligned on the starting line to record the sprint time. The best, worst and mean of the first three, mean of the last three, mean, and total sprint time were recorded as RSAbest, RSAworst, RSAmean 1–3, RSAmean 4–6, RSAmean, and RSAtotal, respectively.
Physiological measurements
Heart rate variability
The ECG signals were recorded by using a multichannel recorder (MP35, Biopac Inc, California, USA) from conventional lead II arrangement. The ECG signals were measured 15 min before warm-up and 30 min after exercises. The analogue signals of ECG were transformed into digital signals by using an analogue-to-digital converter with a sampling rate of 1000 Hz via Biopac Student Lab system. The ECG waveforms were then filtered to remove any artefact by using Acqknowledge 4.2.1 software (Biopac Inc, California, USA). The RRI were calculated after eliminating the ectopic beats. If the percentage of ectopic beats was greater than 5%, then the participant was excluded from the analysis. A custom-written programme was then used to identify the peaks of the R waves (Mathcad 15, Parametric Technologies, Natick, MA). The last 512 RRI were obtained for HRV data analysis.
The mean, SDRR, coefficient of variation of R-R interval (CVRR) and rMSSD of RRI were calculated by using the standard formula for time domain analysis. The power spectra of RRI were calculated by means of fast Fourier transformation. The direct current component was eliminated before the calculation of the power spectrum. The area under the curve of the spectral peaks within the ranges of 0.01–0.4, 0.01–0.04, 0.04–0.15 and 0.15–0.4 Hz were defined as the total power (TP), very-low-frequency power (VLFP), low-frequency power (LFP) and high-frequency power (HFP), respectively. The frequency of power ranging from 0.01 to 0.4 Hz was used for the normalisation of VLFP (nVLFP=VLFP/TP), LFP (nLFP=LFP/TP) and HFP (nHFP=HFP/TP), in accordance with the recommendations from the Task Force of the European Society of Cardiology and the North American Society of Pacing Electrophysiology.17 Since the frequency range of 0.04 to 0.4 Hz in the recommendation from the Task Force does not cover the frequency of VLFP, we used the frequency of 0.01 to 0.4 Hz to normalise VLFP, LFP and HFP instead in this study. The low/high frequency power ratio (LHR), very low/high frequency power ratio (VLHR=VLFP/HFP), and the frequency of high-frequency component (HFF) or the respiratory frequency were also calculated.
The nVLFP were used as the indices of vagal withdrawal, renin-angiotensin modulation and thermoregulation,18–20 the nLFP as the index of combined sympathetic and vagal modulation,21 the nHFP as the index of vagal modulation, and the LHR as the index of sympathovagal balance.22 Since VLFP is an index of vagal withdrawal and HFP is an index of vagal modulation, a novice index VLHR was defined as an index of sympathetic activation in this study, similar to the LHR.
Haemodynamic measurement
Left arm blood pressure (BP) was measured by using an automatic BP monitor (HEM-770A, Omron Healthcare, Taiwan). Systolic BP (SBP), diastolic BP (DBP), mean arterial pressure (MAP) and pulse pressure (PP) were obtained in supine position before exercise, and 5 and 30 min after exercise. PP was calculated as the pressure difference between SBP and DBP, and MAP was calculated by using the formula SBP+1/3 DBP.
Blood lactate test
Blood lactate (BL) was measured by using finger blood samples. A blood sample test was taken from the middle fingertip before and immediately after completing the exercises. An alcohol swab was used to clean the area of blood withdrawal and the blood sample was drawn into the test strip (cos14827–01, h/p/Cosmos Sirius, Leipzig, Germany). A lactate test metre was used to measure the level of BL concentration (h/p/Cosmos Sirius, Leipzig, Germany).
Rating perceived execution
A conventional 15-point Borg scale was used to evaluate the rate of perceived exertion (RPE).23 The rate of RPE was measured at the first stage and immediately after the exercises.
Experimental procedure
All participants were randomly assigned to the RSA and YY protocols within 7 days, and the tests were completed within 7 days so that the interferences from environmental, social, training and other factors could be minimised. The participants were informed to take light training 1 day before the visits and refrain from taking caffeine-containing substances and smoking 2 h before the experiments. At the beginning of the experiments, the participants rested comfortably in supine position in a sports massage room. The locations of lead II arrangement were cleaned with alcohol wipes prior to application of ECG electrodes (Kendall 200 Series Foam Electrodes, Covidien, Mansfield, Massachusetts, USA). A portable HR monitor (FT 80, Polar Electro, Finland) was used to assess HR during exercises. Adhesive tapes were applied to secure the electrode placements during exercises. Resting ECG signals were then recorded for 15 min by using a multichannel recorder (MP35, Biopac Inc, California, USA), followed by pre-exercise BL concentration measurement. The room temperature was controlled at 25° Centigrade, and the humidity ranged from 50 to 60%.
The warm-up activity consisted of 5 min of a 50 W cycling exercise with a pedalling rate of 60 rpm (Optibike Med, Ergoline, Germany). The participant wore sports shoes and performed the exercise protocols indoors on artificial lanes. The blood sample was taken immediately after the RSA or YY test, and the ECG signals were recorded 30 min after exercise with supervision throughout the experiment. To avoid the potential influence of circadian rhythm and daily physical activity, the anaerobic and aerobic exercise experiments were conducted at the same time of the day.
Statistical analyses
Statistical analyses were conducted with Sigmaplot 13 for Windows (Systat Software, Inc, California, USA). Descriptive data are presented as median values with IQR. Kruskal-Wallis one-way analysis of variance on ranks was used to determine the differences in physical characteristics, HRV, BP and exercise performance among the groups. A post hoc analysis with Dunn's method was used to identify the differences among the groups when a significant difference was identified. To avoid daily variation of physical status, the percentage changes in HRV and haemodynamic measures 5 min and 30 min after the exercise were calculated by using the following formulae:

where “X” stands for the HRV or haemodynamic measure to be evaluated. Wilcoxon signed rank test was used to compare the percentage changes in HRV and haemodynamic measures after exercise between the exercise protocols. The α level of significant difference was set at p<0.05. The Sigmaplot 13 for Windows was used to conduct a post hoc analysis of statistical power for comparisons among groups. The power was calculated as the minimum detectable difference in means of variable and expected SD of residuals of variable in the comparison among three groups of participants. The number of groups was set at 3, the group size was set at 36 participants and the level of α value was set at 0.05. The resultant powers of each variable are shown in all tables. We also used Sigmaplot 13 for Windows to estimate the sample size of the study. By using %LHR as the variables for the estimation of sample size, we found that 34 participants were required to minimise the type I errors in our study. Therefore, we recruited 36 participants in our study. The reason for choosing %LHR as the variable for estimation was that LHR is an essential HRV measure which is often used to represent sympathovagal balance of the subject. The sympathetic modulation of the subject was expected to be different in various sports protocols.
Results
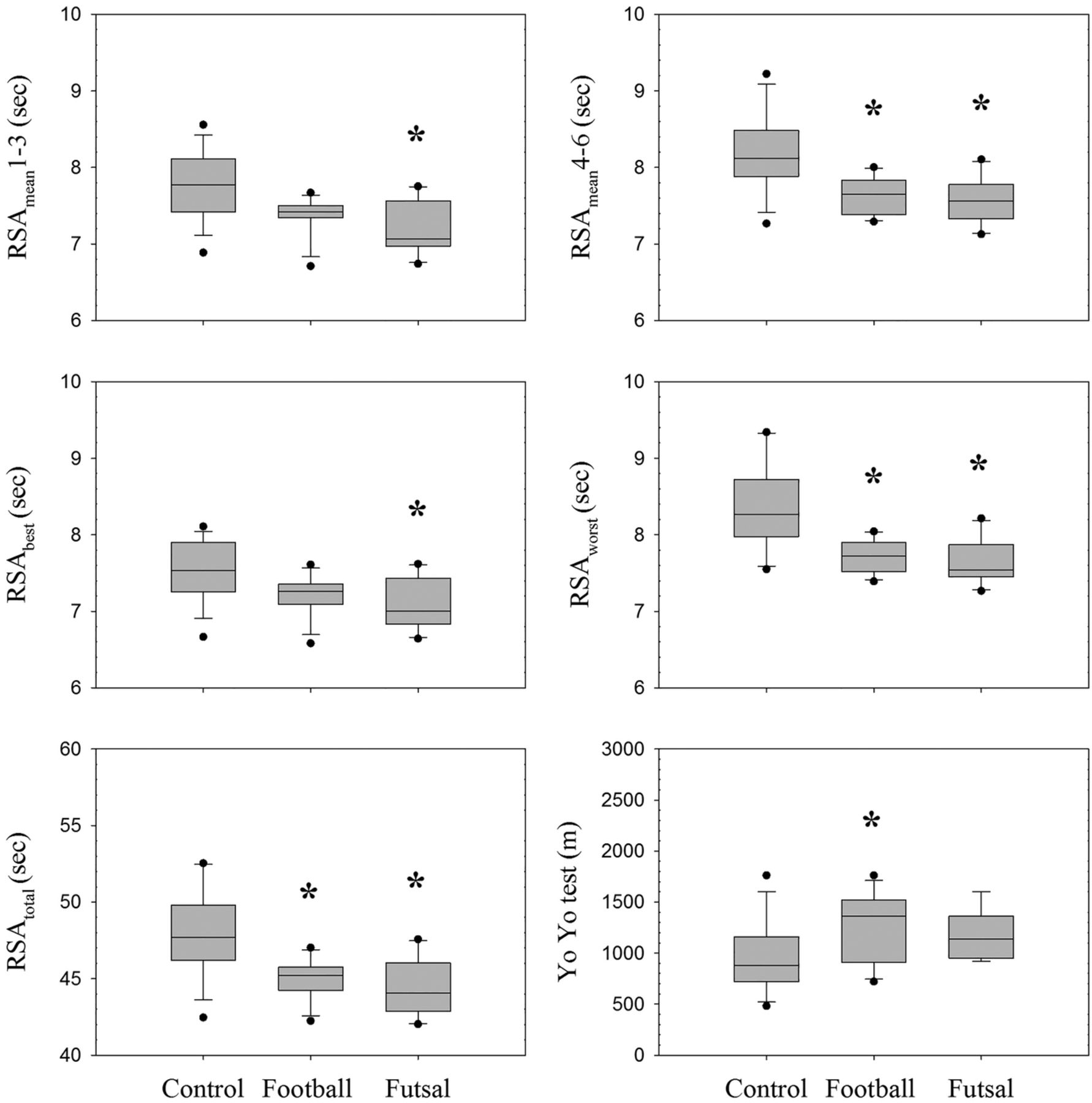
Exercise performance is presented in figure 1. Pairwise comparisons showed significant differences in all RSA variables between the control and futsal groups, and in the RSAmean 4–6, RSAmean, RSAworst, RSAtotal, and YY total covered distance between the control and football groups. No significant difference in the RSA and YY performance between the football and futsal groups was found despite a greater RSA performance and a less YY covered distance in the futsal group.

Performance profiles during repeated sprint ability (RSA) and Yo-Yo intermittent recovery test level 1. Data are presented as median values (25–75 percentile). *Significant difference versus control group (p<0.05).
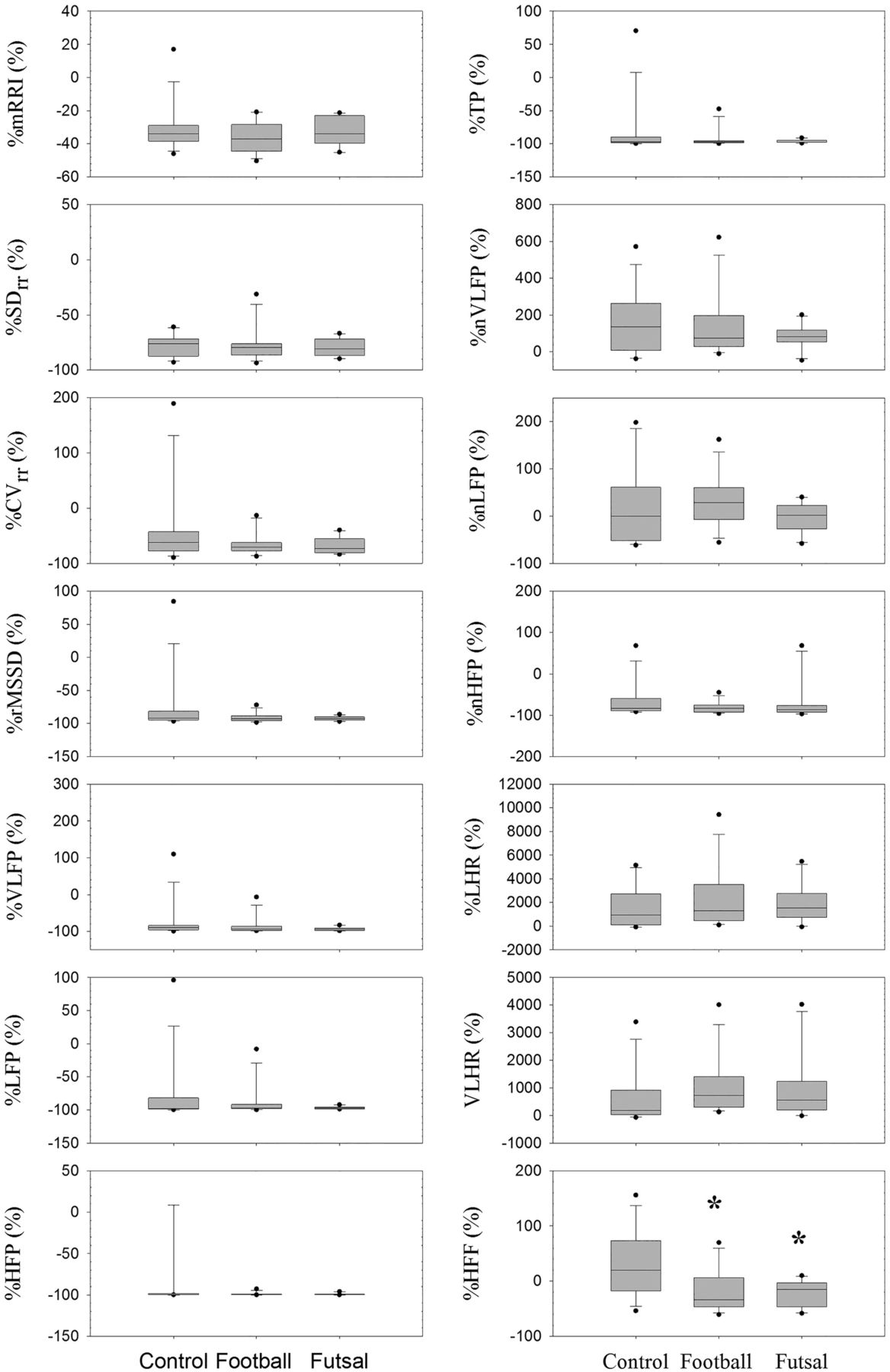
The baseline HRV measures were not significantly different among the groups (tables 2 and 3). Significant changes in the percent change in HRV indices were found in %nHFP, %VLHR and %LHR between the futsal and control groups in the RSA test (figure 2). The futsal group had significantly increased %VLHR and %LHR and significantly decreased %nHFP, as compared with the control group. In the YY test, the group difference in %HFF after exercise was significantly reduced in the football and futsal groups, as compared with the control group (figure 3).
Baseline measurement of HRV measures in the anaerobic exercise protocol (RSA test)
Baseline measurement of HRV measures in the aerobic exercise protocol (YY test)

Comparison of the percentage change in HRV measures after anaerobic exercise (RSA test) among the control, football and futsal groups. Data are presented as median (25–75 centile). mRRI, mean R-R interval; SDRR, SD of R-R interval; CVRR, coefficient of variation of R-R interval; rMSSD, the mean sum of the squared differences between R-R intervals; TP, total power; VLFP, very-low-frequency power; LFP, low-frequency power; HFP, high-frequency power; nVLFP, normalised VLFP; nLFP, normalised LFP; nHFP, normalised HFP; VLHR, VLFP/HFP ratio; LHR, LFP/HFP ratio; HFF, frequency of the high-frequency component; HRV, heart rate variability; RSA, repeated sprint ability. *Significant difference versus control group (p<0.05).

{kind=link}
{kind=link}
{kind=link}
Comparison of the percentage change in HRV measures after aerobic exercise (YY test) among the control, football and futsal groups. Data are presented as median (25–75 centile). mRRI, mean R-R interval; SDRR, SD of R-R interval; CVRR, coefficient of variation of R-R interval; rMSSD, the mean sum of the squared differences between R-R intervals; TP, total power; VLFP, very-low-frequency power; LFP, low-frequency power; HFP, high-frequency power; nVLFP, normalised VLFP; nLFP, normalised LFP; nHFP, normalised HFP; VLHR, VLFP/HFP ratio; LHR, LFP/HFP ratio; HFF, frequency of the high-frequency component; HRV, heart rate variability; YY, Yo-Yo intermittent recovery test level 1. *Significant difference versus control group (p<0.05).
In the control group, the %nVLFP and %VLHR in the RSA were significantly larger than those in the YY test (table 4). In the futsal group, the percentage decreases in TP, VLFP and LFP in the RSA test were also significantly greater than those in the YY test.
Significant difference of percentage changes in HRV measures between RSA test and YY intermittent recovery test level 1
In haemodynamic measurements, no significant differences in %SBP, %DBP, %MAP and %PP were observed in either %X5 min or %X30 min among the groups (table 5). The results also revealed no significant differences in exercise peak HR, pre-exercise and postexercise BL concentration, and RPE values (table 6).
Percentage changes in haemodynamic measures after exercises
Descriptive data of peak heart rate during exercises, BL concentration and rating of perceived exertion
Discussion
The main finding in the current study was that the futsal group had a decrease in the percentage change in nHFP after exercise and increases in the percentage changes in VLHR and LHR after exercise in the RSA test, as compared with the control group. In addition, the HFF was found to be significantly reduced in the football and futsal groups as compared with the control group in the YY test, but not in the RSA test.
Our findings regarding the HRV indices in the RSA test are in agreement with a series of futsal studies investigating the effects of futsal training on the autonomic functions.7 ,9 ,10 Interestingly, football and futsal are sister sports with high physiological demands, with variations in running patterns and physical activities. However, in contrast to the aerobic-oriented energy demand in football, the futsal outfield players are required to continuously execute all-out sprints (3–4 bouts) with short recovery time (20–30 s low-intensity activities).4 de Freitas et al7 reported that an anaerobic exercise test was more sensitive at reflecting the training adaptation to futsal players than an aerobic exercise test. In this study, the futsal group demonstrated significantly decreased %nHFP and significantly increased %VLHR and %LHR during the recovery period, as compared with the football and control groups. Solid evidence has supported that the component of HFP is related to vagal influence, whereas LHR is a mathematical expression to assess the autonomic balance between the sympathetic and parasympathetic controls. Owing to the reciprocal relationship and coactivation between the sympathetic and parasympathetic branches in the ANS, autonomic control is the consequence of neural interaction between these two neural mechanisms. The result of this study demonstrated the excitatory effect of cardiac sympathetic activity in university futsal players after repeated bouts of short-distance sprint.
It is interesting to note that the main HRV indices had no significant differences among the groups in the YY protocol. Dutra et al24 found that individual aerobic capacity was not a factor to determine cardiac autonomic modulation in healthy adults at rest. In contrast, our laboratory recently reported that there are increased vagal and decreased sympathetic modulations in amateur football players at rest, as compared with sedentary health adults.12 Regarding the physiological adaptation to specific exercise training, previous studies have shown that the resting HR was decreased while the parasympathetic modulation was increased after completing a period of aerobic training.25 ,26 However, no significant changes in all HRV indices were found after exercise in the YY test. This finding seemed to be in contradiction to the common notion that the autonomic nervous modulation of the participants should be changed after specific exercise training. The control participants in this study were physical education students. It seems that university students with high compliance of sports adherence demonstrated similar postexercise profile of cardiac autonomic nervous modulation with football or futsal players after aerobic intermittent exercise, despite an attenuation of the total covered distance. The higher respiratory rate found in the control group after acute aerobic intermittent exercise may be a potential factor to undermine the true interpretation of cardiac autonomic activation during the recovery period. In addition to the HRV indices, other physiological markers such as plasma epinephrine and norepinephrine might be used to indicate the level of sympathetic activation. The lack of blood sample analysis in this study might therefore limit our understanding about the changes in sympathetic and parasympathetic modulations in the YY protocol.
Exercise duration and exercise mode may contribute to the discrepancy in sympathovagal balance and baroreflex control.5 Baroreflex control via the sympathetic and parasympathetic activities is a key determinant to adjusting the HR response.27 Our results showed increases in SBP and PP and decreases in DBP and MAP after completing both exercise protocols. The increases in SBP and PP are related to the elevation of peripheral vasoconstriction and stroke volume. However, no significant difference in the postexercise BP changes in all groups indicated that vasomotor activation was not a major mechanism in the findings of sympathetic activation and sympathovagal balance after the RSA exercise in futsal players and the change in %HFF after the YY exercise. Indeed, all groups experienced similar physiological and psychological strains during the RSA and YY exercises due to no significant differences in peak HR, RPE and BL concentration in group comparison. Thus, the metabolic demand and exercise intensity was equivalent in these three groups. The potential mechanisms related to postexercise change in HR responses in the football and futsal groups may not be supported by the carotid-cardiac baroreflex.
Conclusions
Our study showed that the percentage decrease in vagal modulation after exercise in futsal players was significantly reduced, while the percentage increase in sympathetic modulation in futsal players after exercise was significantly enhanced in the RSA test, but not in the YY test, as compared with the control group. The increase in sympathetic activity and the decrease in vagal activity in the futsal players were greater than the corresponding increase and decrease in the football players in the RSA test. In addition, the respiratory frequency was significantly reduced in the football and futsal players as compared with the controls in the aerobic YY test, but not in the anaerobic RSA test.
References
Footnotes
Contributors Y-SC contributed to research design, data collection and manuscript preparation. C-JL contributed to data collection and statistics. W-AL contributed to data collection and statistics. C-DK contributed to research funding, IRB application and manuscript preparation.
Funding This study was supported by a research grant MOST103-2410-H-075–001 from the Ministry of Science and Technology, TAIWAN and a grant V99C1-106 from the Taipei Veterans General Hospital, TAIWAN.
Competing interests None declared.
Ethics approval Institute Review Board of the hospital, Taipei Veterans General Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.