Article Text

Abstract
Objectives The measures used to contain the COVID-19 pandemic led to a significant reduction in physical activity. Due to the health benefits of exercise, recommendations were made for lockdown restrictions. Within the CoCo-Fakt study (Cologne-Corona counselling and support for index and contacts during the quarantine period), we aimed to determine how these recommendations were implemented, especially by individuals who were officially quarantined due to an infected persons (IPs) or as close contacts (CPs), and how this affected their physical and psychological condition.
Methods From 12 December 2020 to 6 January 2021, all IPs and CPs registered by Cologne’s public health department up to the survey period were surveyed online. Of 10 547 people in the CoCo-Fakt sample, 8102 were integrated into the current analysis. In addition to demographic data, information regarding COVID-19-specific and persistent symptoms or conditions and their association with the amount and type of exercise and screen time before and during the quarantine were collected.
Results Before quarantine, 66.9% of IPs and 69% of CPs were physically active; during quarantine, this decreased by 49.4% in IPs depending on the course of the disease and by 30.6% in CPs. Physically active IPs and CPs felt less exhausted and more fit during their quarantine periods than those who were inactive, with active IPs significantly less likely to report prolonged physical and psychological symptoms than their more sedentary counterparts.
Conclusion Given the acute and long-term positive effects of exercise on quarantined individuals, corresponding recommendations should be communicated to those affected, especially CPs. Recommendations for IPs depend on their health status.
- COVID-19
- Exercise
- Infection
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Physical activity is considered a protective factor for non-communicable diseases, but due to the restrictions of daily life, less physical activity was observed during the pandemic.
What this study adds
Physical activity decreased during stay-at-home orders by 49.4% in infected persons and 30.6% in contact persons. People who were active during quarantine felt fitter, less tired and less exhausted during this period.
How this study might affect research, practice or policy
The benefits of exercise should be repeatedly emphasised during subsequent medical care, and people should be encouraged to exercise or exercise more.
Introduction
The COVID-19 pandemic has had an enormous impact on human life worldwide, with considerable economic, health and psychosocial consequences.1 In the absence of possible therapeutic countermeasures and vaccinations that only became available in Germany at the end of 2020, various contact restrictions and curfews were imposed to protect high-risk groups and prevent an overload of the health system. Due to these restrictions, the pandemic has had an enormous impact on the general population’s daily lives and mental health. Several studies described an increase in loneliness, symptoms of anxiety and depression.2 3 Physical activity is an important measure for maintaining mental health.4 Therefore, during a lockdown or political regulations that restricted contact in public and private spaces, especially during an individual quarantine ordered by the authorities, exercise and physical activity were and remained advised.4 Faulkner et al5 showed that people who exercised more during the initial COVID-19-related restrictions had better mental health and well-being than those who did not. Sallis et al6 also showed that physically inactive infected individuals had a more severe disease course than active ones. Inevitably, however, the lockdown has led to a reduction in physical activity in various ways; this is due in part to the closure of gyms, swimming pools and club facilities, although everyday activities have also been affected. Data from more than 450 000 people from 187 countries indicated a 27% reduction in daily steps, equivalent to a 1432-step decrease.7 Parallel to the reduction in physical activity, increased media time was observed in various studies.8 9 However, numerous recommendations regarding physical activity have been made (eg, by the WHO), which can and should be (implemented at home10–12) to counteract the negative effects of lockdown or quarantine measures (online supplemental table S1). Naturally, infected persons (IPs) are assumed to be not or less active. However, the symptomatology in the context of COVID-19 disease is very heterogeneous. Ma et al13 showed in a recent meta-analysis covering 29 776 306 individuals undergoing testing that the pooled percentage of asymptomatic infections among the confirmed population was 40.5%.
Supplemental material
So far, however, there have been no studies of the type, frequency or intensity of exercise undertaken by individuals in officially ordered quarantine like IPs and their close contacts (CPs). A stay-at-home order restricts the radius of affected persons even more. Moreover, such a requirement may be even more psychologically stressful than general lockdown measures. In addition, a violation of this order in Germany was punishable by severe financial penalties.14 Therefore, the Cologne-Corona (CoCo)-Fakt study15 (CoCo counselling and support for IPs and CPs during the quarantine period; author’s translation) analysed physical activity before and meanwhile officially ordered quarantine among IPs or CPs and how this affected their subjective perceptions of physical performance, fatigue and exhaustion during this time, and the (long-term) symptoms of IPs.
Methods
Study design
Since detecting the first COVID-19 infection in Cologne at the end of February 2020, all laboratories have reported all those who have tested positive for SARS-CoV-2 to the Cologne public health department. These people were contacted, registered in DiKoMa,16 the Cologne Health Department’s software tool, questioned in a standardised manner regarding, among others, possible routes of infection, pre-existing conditions and other risk factors. In addition, CPs were identified so that they could also be quarantined. In the survey period of this study, CPs were defined according to criteria established by the German Robert Koch Institute and European Centre for Disease Prevention and Control, among others, as individuals who had had contact with an IP for more than 10–15 min at a distance of less than 2 m and without sufficient protection.17 Based on the German Infection Protection Act, the quarantine period during the survey period was usually 10–14 days from the onset of symptoms or the positive test in IPs and from the last contact in CPs.
Sampling and study population
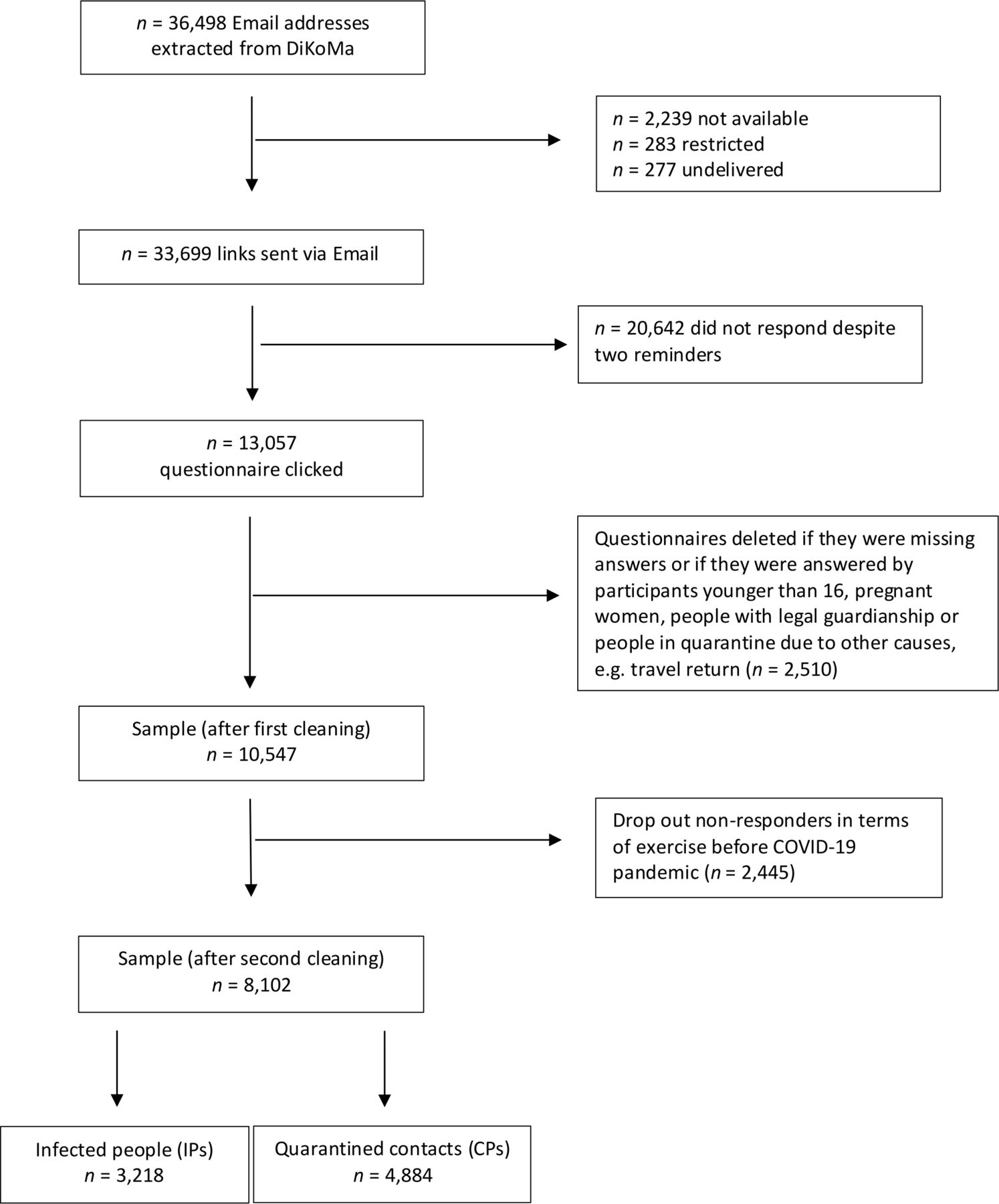
From this dataset, all people registered in DiKoMa up to 9 December 2020 (n=36 498) were extracted; people under 16 years of age, people with missing informed consent forms, non-compliant individuals, deceased patients and those who were in medical or nursing facilities or quarantined for other reasons (eg, travel returnees) were excluded. The detailed study design has already been published.15 From 12 December 2020 to 6 January 2021, the link to the online survey was sent via email to 33 699 people, 13 057 of whom responded by clicking. Twice, after 5 and 7 days, a reminder was sent asking for participation in the survey.15 After the data were cleaned, only individuals for whom information on prepandemic physical activity behaviour was available were integrated into this evaluation (n=8102; figure 1). On average, the quarantine period was over for 99.6 days (SD=87.5; see table 1). 17.7% (n=1278) participants were in quarantine during the first pandemic wave in Germany (February to April 2020), 17.0% (n=1228) between May and September and 65.4% (n=4632) during the second pandemic wave (October to December 2020; missing n=864).

Study population flow chart.
Population characteristics
Survey items
The following demographic data were assessed and included in this analysis: age, sex, presence or absence of chronic diseases (diabetes, cardiovascular diseases, orthopaedic disorders, etc), living situation (whether it had a balcony or garden) and family/household structure (partnership, married; children). We designated participants’ socioeconomic status (SES) as high, middle or low based on the categorisation in the German Health Update 2009.18 Those who spoke a language other than German at home were classed as having a migrant background.
Patient and public involvement
The research questions and methods were developed based on the literature.5 6 15 19 To optimise the survey and align it according to the research questions, affected persons from the personal environment were first approached and asked to answer and assess the draft. From this collective, 20 additional affected persons were recruited by snowball sampling, and the feasibility and duration were tested. Since the online survey is anonymised, no individual results are given to the patients. However, the results and the recommendations or support systems developed from them will be communicated via the press and the city’s homepage and the health department. Therefore, future quarantined persons will benefit from our study if our recommendations are considered in settings that influence their individual needs, worries and coping strategies.
Quarantine-specific situation
The assessment of the quarantine-specific situation on physical performance and fitness and state of exhaustion and/or fatigue (tiredness) was recorded with the following questions:
I feel/felt limited in my physical performance.
I feel/felt exhausted.
I feel/felt tired.
I always feel/felt physically fit.
Responses ranged from ‘not applicable at all’ (1) to ‘fully applicable’ (6) and were grouped into yes (1, 2), no (5, 6), partly (3, 4).
Symptoms
The assessment of COVID-19-specific and postinfection symptoms was recorded only in IPs, who were asked to describe the course of their disease according to the following options:
Physical symptoms
Completely symptom-free, clustered as asymptomatic.
Mild symptoms, clustered as mild progression.
1–3 days of clear symptoms clustered as a moderate course.
A severe feeling of illness, clustered as a severe course.
Psychological symptoms
Illness-related anxiety, psychological symptoms.
Free-text answers
Responses from this category were assigned to the clusters as mentioned above. For example, anxiety is related to the ‘psychological symptoms’ category, and hospitalisation is related to the ‘severe course’ category.
At the time of the survey, no uniform definition of long COVID-19 was available.20 Therefore, assessments of long-lasting and persistent symptoms (eg, weeks of reduced performance, fatigue, reduced concentration, memory disorders, permanent loss of smell and taste, hair loss and so on were based on the free responses).
Physical activity
Lifestyle was recorded in physical activity and sedentary behaviour prepandemic and during the mandated quarantine period in both IP and CP.
Were you active in sports before the pandemic period/during the quarantine period?
Yes/no.
If yes
Type of exercise.
How often per week.
For how many minutes per activity.
Independently.
In a club.
In a gym/with a coach.
Media/online based.
Other.
First, binary variables were formed based on whether participants engaged in sporting activities before the pandemic and during the quarantine period and whether they achieved the recommended 150 min of moderate activity per week. In addition, a qualitative analysis of the forms of exercise and types of sport performed was carried out based on the classifications defined by Ainsworth et al (table 2).21
Types of exercise and classifications
Sedentary activities
The survey recorded sedentary activities in minutes per week in professional and private spheres. The survey also explicitly asked about media time. In the context of the present analysis, only screen time in the private context was used.
How many hours per week did you usually spend sitting before the COVID-19 pandemic/during the quarantine period? (eg, in the car, on the sofa, while watching television and so on).
At work
Office work without screen work.
Office work with screen work (eg, computer work).
Driving a car.
Other.
In your private environment
Computer/phone/tablet.
TV.
Driving a car.
Reading/writing
Hobbies (sewing, handicrafts, etc).
Other.
Statistics
For the descriptive statistics, absolute and relative frequencies for categorical variables and mean values (M) and SDs for continuous variables were calculated. Associations between participants’ characteristics (eg, age, gender) and outcomes were examined using χ2 tests and independent t-tests.
Binary and multiple logistic regressions were used to analyse predictors of subjective feelings in IPs and CPs during isolation and long-lasting symptoms in IPs. For this purpose, ORs and 95% CIs of potential determinants of subjective perceptions/symptoms were calculated, taking age, gender, the presence of chronic diseases and level of prepandemic physical activity and screen time into account. Other variables, such as migration background, family/household structure, residential situation, SES, duration of quarantine, the period between quarantine and answering the questionnaire, were excluded from the models if they were not significant. Model fits were checked using pseudo R2 (Nagelkerke R2). The level of significance (α) was set at=0.05. The analyses were carried out with the statistical software SPSS V.27.0 (IBM).
Main analysis
Subjects
A total of 3218 IPs and 4,884 CPs could be integrated into this analysis. The study population had a mean age of 41.7 years (SD=14.3) and was 61.6% female (table 1). On average, the duration of quarantine was 11.8 (SD=4.6) days, which varied based on differences in the applicable guideline. The data for the entire group and subdivided according to IP and CP are shown in table 1.
Physical activity/screen time
Before the pandemic, 5522 people (68.2%) reported being physically active. 66.4% reached the 150 min of moderate activity or more per week recommended by the guidelines. During quarantine, only 2439 (30.1%) were physically active. 46.3% reported reaching the guidelines. IPs were significantly less active during quarantine than CPs (17.5% vs 38.4%, respectively; p<0.001; table 3). In both groups, those who were already regularly active before the pandemic were more active during quarantine (p<0.001 in each case).
Physical activity (PA), exercise and screen time before the COVID-19 pandemic and during quarantine
Overall screen time increased from 3.0 (SD 2.8) hours per day to 3.4 (SD 3.3; table 3). There was a significant increase in both groups, which was more pronounced in the CP group (table 3, p<0.05 in each case).
Types of exercise
Before the pandemic, endurance sports were the most common type of exercise participants engaged in, followed by strength sports/strength endurance (see table 4). During the quarantine, there was a reduction in overall time spent exercising and a clear shift from endurance sports towards strength and coordination training (see table 4). Even though online workouts were not high overall, they were used more frequently by CPs (n.s., table 4).
Prepandemic sport types and exercise during quarantine; multiple answers were possible
Subjective perceptions during the quarantine period
A total of 1684 people (23.0%) stated that they always felt fit during quarantine; 4554 (61.4%) felt limited in their physical performance, 3271 (44.4%) felt exhausted and 3563 (48.4%) felt tired. IPs differed significantly from the CPs in all areas (table 5).
Subjective perceptions during the quarantine period
Responses ranged from ‘not applicable at all’ (1) to ‘fully applicable’ (6) and were grouped into yes (1, 2), no (5, 6), partly (3, 4).
For both groups, the analysis showed that those who were physically active during quarantine felt physically fitter, less limited in their physical performance, less tired and less exhausted than those who were physically inactive during quarantine. This was influenced by age, sex, pre-existing conditions and sports participation before the pandemic; for IPs, this was also influenced by whether symptoms were present. A detailed table of regression results appears in online supplemental material S3 (figure 2A,B).
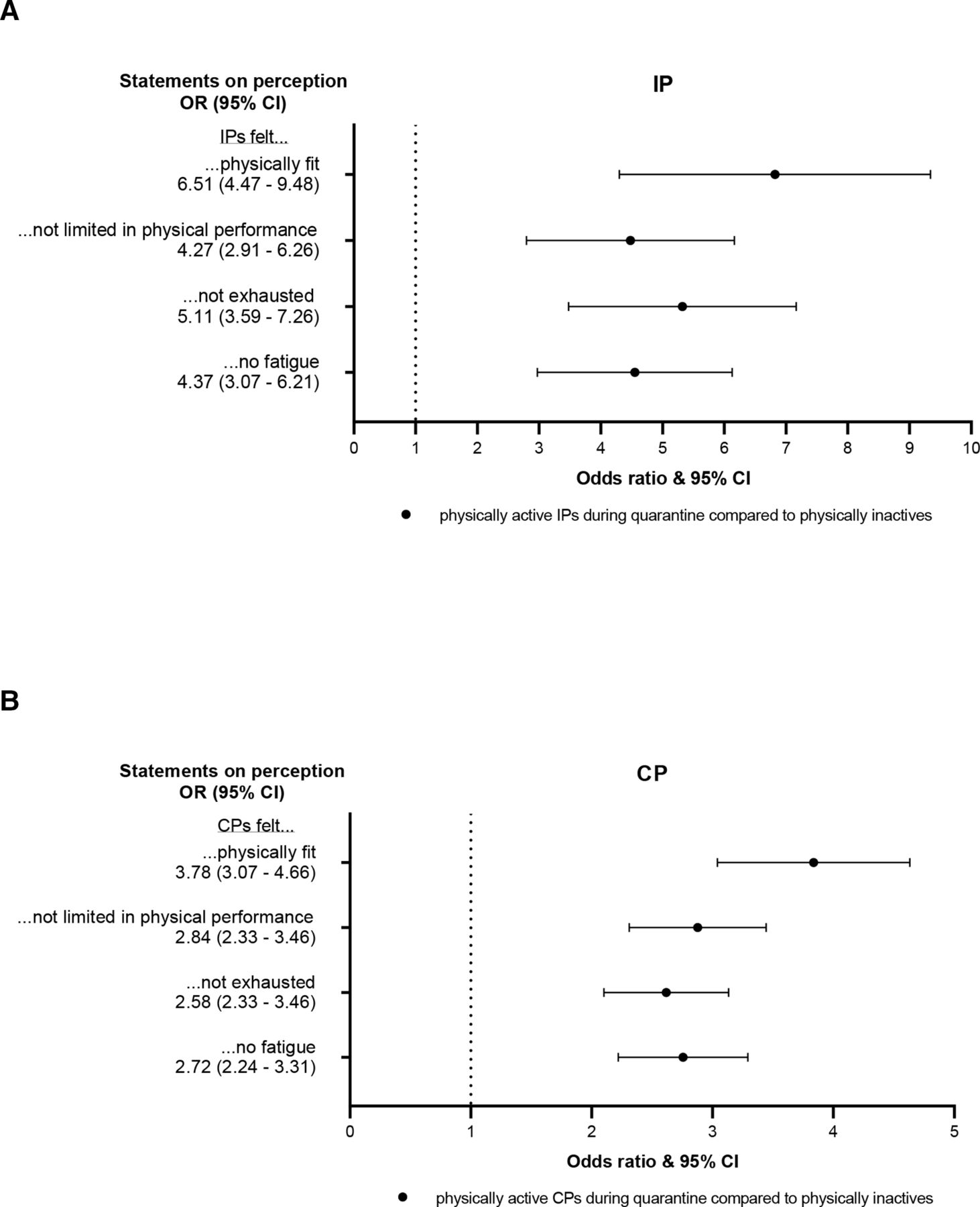
Impact of physical activity on IPs (A) and CPs (B) subjective perceptions; multiple logistic regression, adjusted for age, gender, chronic disease status, physical activity before quarantine and screen time. CPs, close contacts; IPs, infected persons.
Symptoms
Of the IPs, 503 (18.4%) reported being asymptomatic, 848 (31.1%) were mildly symptomatic, and 835 (30.6%) were moderately symptomatic. Severe symptoms were reported by 19.9% (n=544). Psychological symptoms were reported by 11.6% of IPs (n=407); these included disease-related anxiety and depressed mood. At least 139 IPs (4.0%) reported long-term complaints at the time of the survey, including exhaustion, loss of taste and smell, impaired performance, lack of concentration and persistent headaches (table 6).
Symptoms of IPs during and after quarantine
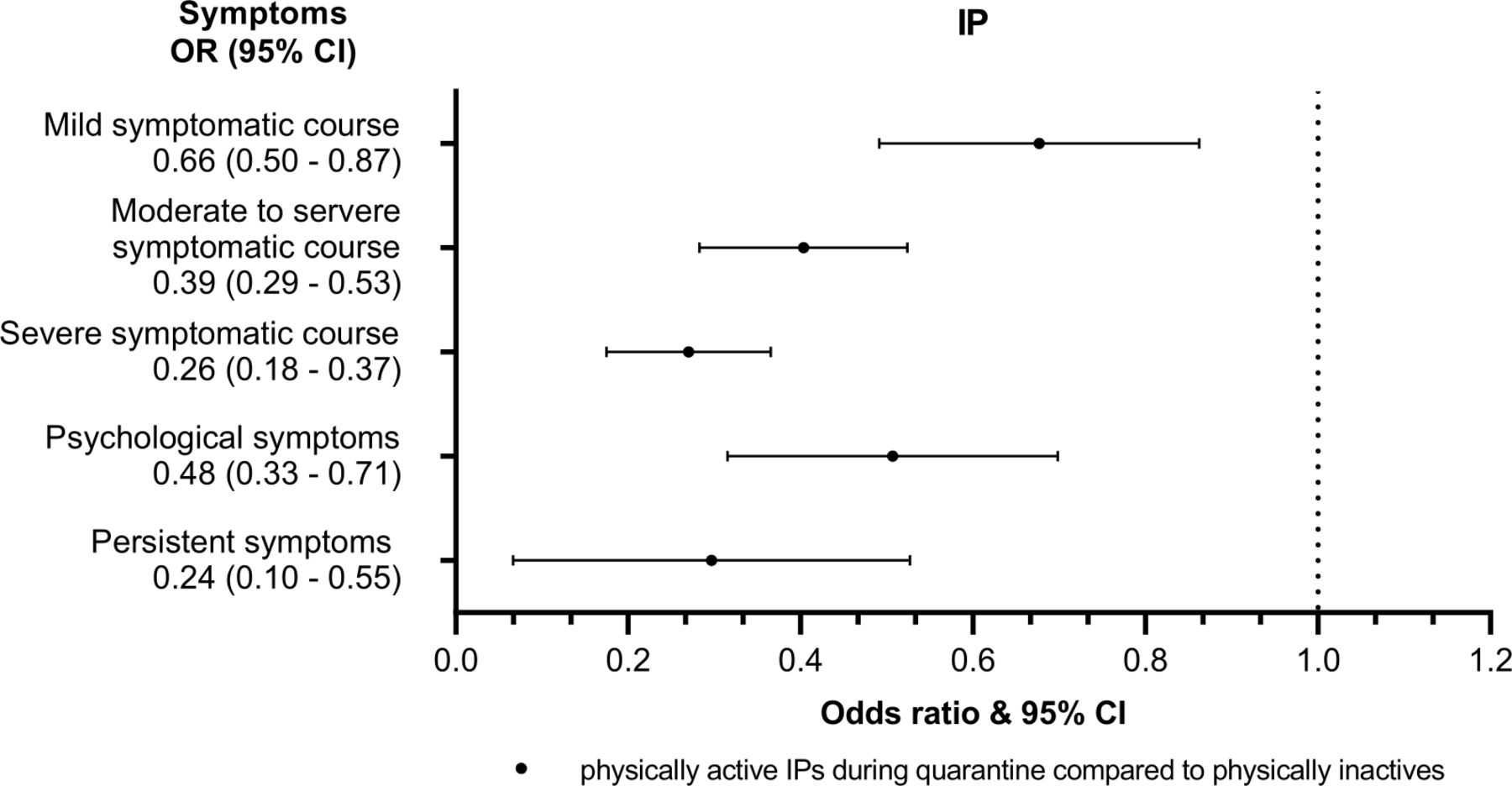
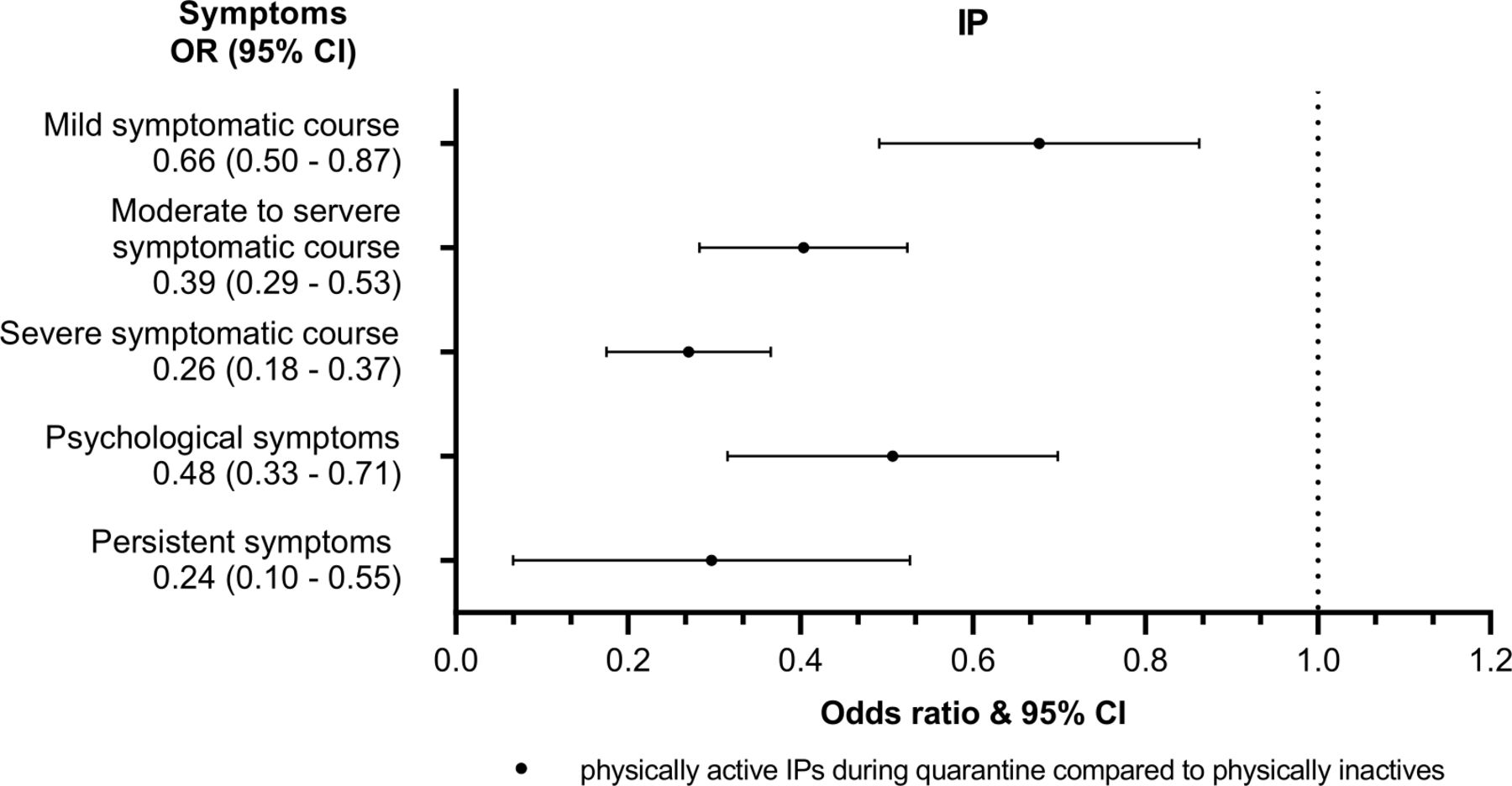
Considering the cross-sectional design, physical activity was found to predict the severity of physical symptoms and the occurrence of psychological and persistent symptoms. Physically active IPs were less likely to display COVID-19-induced symptoms during quarantine (see figure 3). The effect increased with symptom severity. Thus, active IPs were 34% less likely to have mild physical symptoms, 61% less likely to have moderate physical symptoms and 74% less likely to have severe physical symptoms than inactive IPs. Active IPs were 52% less likely to have psychological symptoms and 76% less likely to have persistent symptoms (figure 3).
{kind=link}
{kind=link}
{kind=link}
Impact of physical activity during quarantine on perceived symptoms of IPs; multiple logistic regression, adjusted for age, gender, chronic disease status and physical activity before the quarantine. IPs, infected persons.
Discussion
Main findings
This is the first study to analyse the associations between subjective perceptions of physical fitness, exhaustion and fatigue in IPs and CPs under legally enforced quarantine imposed by the health department. In our cohort, screen time increased by about 10% among IPs and about 20% among CPs during the quarantine period. Overall, only about one-third of participants reported being physically active during this period, regardless of family, respectively, household structure or the presence of a garden or balcony (data not shown). Due to infection with COVID-19 and the associated symptoms, IPs were less active during the quarantine period (only about 18%, compared with about 67% before the pandemic) than the CPs (about 39%, compared with about 69% before the pandemic). While the reduction in physical activity time was related to symptoms in the IPs, there were no disease-related restrictions for CPs. Active CPs, however, clearly benefited during the quarantine period with regard to their subjective perceptions: they felt fitter, less restricted in their ability to perform, less exhausted and less tired than inactive CPs. They mainly used riding exercise bikes, strength training with home dumbbells or dancing as forms of exercise. There was an overall shift from endurance sports prepandemic to strength and flexibility exercises that can be done at home during the pandemic. Surprisingly few participants used online exercise programmes.
Regarding the benefits of home-based exercise on physical fitness in healthy older adults, Chaabene et al22 described improvements in muscle strength, muscular endurance and balance in a systematic review. More frequent training sessions (>3 per week) and longer sessions (>30 min per session) had greater effects. Due to the positive correlations with mental health, CPs without symptoms should be advised to exercise regularly and limit media use/screen time.23 24
IPs who had symptoms were understandably less active during the quarantine period. Active IPs reported fewer limitations such as lesser physical performance, exhaustion, fatigue and persistent symptoms than IPs who were not active during the quarantine period. These two aspects are, of course, mutually dependent so that no causal association can be concluded. Thus, based on cross-sectional analysis, we can only speculate about a possible preventive effect of exercise in the context of Long COVID-19.25 In addition, it must be decided individually and, depending on the severity of the disease, to what extent IPs should be advised to exercise during the quarantine period.26 Acute infections are generally a contraindication to physical activity. Asymptomatic patients can be advised to do very light physical exercises, such as yoga and flexibility exercises. To prevent complications such as myocarditis or postacute COVID-19 syndrome, symptomatic patients should start light exercise again about 7 days after symptoms have subsided, depending on their severity.26 If symptoms reoccur, exercise should be discontinued, and medical advice sought if necessary.
Strength and limitations
A great strength of this study is a large amount of data, systematically collected by the largest health department in Germany and consisting exclusively of data on quarantined people. However, people with a significantly low proportion of education or migration background were significantly less likely to respond to these interviews despite the availability of translated questionnaires. In addition, respondents had undergone quarantine anywhere between 1 week and 9 months before the survey; the different intervals could have changed the subjective assessment and influenced the data. The majority of participants were quarantined during the second wave of the pandemic (October–December 2020). An advantage is that they probably remember their situation more clearly; a disadvantage is that this limits the significance of possible persistent symptoms. The survey’s cross-sectional nature also limits its validity. Unfortunately, inhibiting and supporting factors for movement opportunities were also not recorded; in another survey examining overweight families, space and digital equipment requirements were mentioned.14 We cannot determine how these factors played a role in this survey; however, participants’ living situation had no relevant influence on their exercise. Therefore, it is recommended that these factors be investigated in further surveys.
Conclusion
In summary, taking selection bias and the methodological limitations of a cross-sectional analysis into account, this study showed that being physically active increases the subjective well-being of IPs and CPs and can thus contribute to their ability to positively adjust to stressful life situations such as quarantine measures due to illness or contact. However, it also became clear that the majority of both IPs and CPs were significantly less physically active during stay-at-home orders. Therefore, depending on an individual’s physical condition, more exercise should be advised during the quarantine period, especially for asymptomatic CPs. Throughout the pandemic, the number of offers for exercise-related digital content and fitness training increased. It could contribute to increased exercise and associated well-being.27 Therefore, such issues could be addressed during the health department’s monitoring of quarantined individuals but also by general practitioners.
Because exercise is important for physical and mental health, the benefits of exercise should be repeatedly emphasised during subsequent medical care, and people should be encouraged to exercise or exercise more.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Rheinisch-Westfälische Technische Hochschule (RWTH) Aachen Human Ethics Research Committee (351/20). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We want to thank all members of the contact tracing team at the Cologne Public Health Department. We would like to thank Hidayet Oruc for his support with the Turkish translation. Additionally, we would also like to thank all persons who participated in this questionnaire.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators We would like to thank Julian Book, Lukas Broichhaus, Monika Daum, Alisa Fabrice, Anna Carlotta Graf, Wanja Nöthig, Markus Lorbacher and Marc Tappiser who contributed to the design of the CoCo-Fakt questionnaire.
Contributors CJ, BG, SF, AK, JN and GAW conducted the study. Data collection was done by AG, SW, NE and NS. AG and CJ analysed the data. AG wrote the manuscript. AG is the guarantor of this work. All authors critically revised the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.