Article Text

Abstract
Background Cross-country skiers have a high prevalence of asthma, but its phenotypes and association with success in competitions are not known.
Objective To investigate, by means of a postal survey, the relative proportions of allergic and non-allergic asthma in competitive cross-country skiers compared with the general population, to study how performance level and training volume are related to asthma and its type and to assess the possible risk factors for allergic and non-allergic asthma in competitive skiers.
Methods All Finnish cross-country skiers enrolled in the largest national competitions in winter 2019 (n=1282), and a random sample (n=1754) of the general population of the same age were sent a postal questionnaire. The response rate was 27.4% (n=351) for skiers and 19.5% (n=338) for the controls. International Ski Federation (FIS) ranking points measured the level of success in skiers. Asthma was defined as self-reported, physician-diagnosed asthma. Asthma was considered allergic if associated with doctor-diagnosed allergy, and exposure to allergens provoked asthma symptoms.
Results The prevalence of asthma was higher in skiers than in the controls (25.9% vs 9.2%, p<0.001), and it was the highest (56.1%) in the most successful quartile of skiers. Asthma was more often non-allergic in skiers than in the controls (60.1% vs 38.7%, p=0.036). Being a skier came with a higher risk for non-allergic (OR 5.05, 95% CI 2.65 to 9.61) than allergic asthma (OR 1.92, 1.08–3.42). Using multivariable regression analysis, training volume was associated with non-allergic asthma, while age, family history of asthma and allergic rhinitis were associated with allergic asthma.
Conclusion The prevalence of asthma is the highest in the most successful cross-country skiers. The asthma in skiers is mostly non-allergic compared with the general population of the same age. The most important risk factor for non-allergic asthma in skiers is high training volume.
- Asthma
- Cross-country skiing
- Performance
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Asthma is highly prevalent in cross-country skiers, and the age of onset of asthma is in early adolescence.
What this study adds
The prevalence of asthma is the highest in the most successful skiers—up to 56.1%.
Cross-country skiers mainly have non-allergic asthma. The excess prevalence of asthma compared with the general population is largely because non-allergic asthma emerges a couple of years after the onset of an active skiing career.
High training volume is associated with non-allergic asthma, while older age, family history of asthma and allergic rhinitis are associated with allergic asthma.
How this study might affect research, practice and/ or policy
Asthma does not prevent competition success in cross-country skiing. High prevalence of non-allergic asthma should be taken into account when diagnosing and treating asthma in skiers.
Introduction
Asthma is a heterogeneous disease characterised by variable airway obstruction and is usually associated with chronic airway inflammation.1 Different phenotypes of asthma can be identified based on patient characteristics and the type of airway inflammation. The onset of allergic asthma usually occurs in childhood or early adulthood and is associated with a family history of asthma and IgE-mediated airway allergies, and eosinophilic inflammation.2 Airway inflammation in non-allergic asthma can be eosinophilic, neutrophilic, mixed or pauci-granulocytic.3 The risk factors for different types of non-allergic asthma are not known in detail. Non-allergic asthma has been associated with airway infections, long-term exposure to irritants and airway damage.4–6 The incidence of non-allergic asthma is relatively low in childhood and early adulthood and increases in older age.7
Asthma is at least twice as common in cross-country skiers as in the general population, with a prevalence of approximately 21%.8 This may be related to years of endurance training and high ventilation rates in cold and dry air, which strain the airways. Airway allergies and allergic asthma are common in children, whether or not they take part in competitive sports such as cross-country skiing.9–11 The total burden of asthma among competitive skiers can be speculated as consisting of a ‘background’ prevalence of asthma that these individuals would have anyway, even without competitive sports, and an ‘excess’ of asthma prevalence triggered by competitive skiing. The mechanisms of asthma triggered by skiing may differ from the most common form of asthma in children and young adults—namely, allergic asthma. The type of airway inflammation in cross-country skiers with asthma is reported to more often be neutrophilic than eosinophilic in comparison with asthma in the general population.12–14 The prevalence of asthma has not been thoroughly assessed by performance level in cross-country skiers, but one might speculate that asthma is most common among those who train the most. Indeed, in the Winter Olympics from 2002 through 2010, athletes using inhaled β2-agonists won approximately twice as many medals as their proportion of all the athletes across all disciplines.15 However, their asthma status was not explicitly reported.
The purpose of this study was to investigate the relative proportions of allergic and non-allergic asthma in competitive cross-country skiers compared with the general population, to study how performance level and training volume are related to asthma and its type and to assess the possible risk factors for allergic and non-allergic asthma in competitive skiers. We hypothesised that asthma is associated with training volume and is more often non-allergic in competitive cross-country skiers.
Methods
Study design and recruitment
The present study has been described in detail previously.16 In short, all Finnish cross-country skiers who had enrolled in either national championships (from 17 years of age onwards to seniors) or the largest national junior skiing competition (13–16 years of age, Hopeasompa competition) were invited to participate in this cross-sectional questionnaire survey (n=1282). The control group was collected from the Finnish Digital and Population Data Services Agency, matching the control population to the skiers who had responded by age, gender and region of the country in which they lived. The controls were allowed to participate in competitive sports, but none competed in cross-country skiing.16 The total response rate was 27.4% (n=351) in skiers and 19.5% (n=338) in the controls. Written informed consent was obtained from each respondent and guardian for subjects under 18. The study was approved by the ethics committee of Pirkanmaa Healthcare District (R18108).
The questionnaire included three questions from the FinEsS questionnaire17 regarding self-reported physician-diagnosed asthma, asthma in parents or siblings and age at asthma diagnosis. In addition, the subjects with asthma were asked at which age they experienced their first asthma-related symptoms. Current asthma was defined as self-reported physician-diagnosed asthma and at least one of the following: currently having three asthma-related symptoms (cough, chest pain, shortness of breath, wheezing or sputum production), active use of any asthma medication or an Asthma Control Test (ACT) score of fewer than 25 points. ACT was used to evaluate asthma control.18
Asthma was defined as allergic if the subject reported a doctor-diagnosed allergy and asthma-related symptoms when exposed to furry animals or pollens. Otherwise, asthma was defined as non-allergic. As a sensitivity analysis, two additional definitions of allergic asthma (doctor-diagnosed asthma and doctor-diagnosed allergy to pollens or animals or doctor-diagnosed asthma and asthmatic symptoms when exposed to furry animals or pollens) were used.
International Ski Federation (FIS) points for skiers were obtained from the International Ski Association’s 8th FIS points list from the 2018/2019 season, which was in effect at the time of the study.19 FIS points are awarded in competitions and calculated based on the level of competition, the level of the top five finishing athletes and the relative loss of the athlete compared with the winner. In World Cup competitions, the winner is awarded zero points (the lower the FIS points, the better the performance). FIS points were used to divide skiers into subgroups by performance level.
Statistical analysis
Statistical analyses were performed using SPSS version 27.0 (IBM Corp, Armonk, New York, USA). The continuous variables were tested for normality (Kolmogorov-Smirnov). Unpaired t-test, Mann Whitney U test and one-way analysis of variance were used to compare the groups, as appropriate. A Χ2 test or Fisher’s exact test was used to compare the categorical variables. Binary logistic regression was used to calculate the risk factors for current asthma, allergic asthma and non-allergic asthma. Variables were included in the multivariable analysis if the p value was <0.1 in the univariate analyses. A p value of <0.05 was considered statistically significant.
Patient and public involvement
Patients and/or the public were not involved in this research’s design, conduct, reporting or dissemination plans.
Results
Prevalence and type of asthma
The characteristics of the skiers and controls are presented in table 1. The controls were slightly older, and a larger proportion of the controls than skiers were female. Cross-country skiers trained more, had asthma more often and were older at the onset of asthma symptoms and diagnosed asthma. Although skiers reported allergies to pollen or animals and allergic rhinitis more often, their asthma was more often regarded as non-allergic.
Subjects’ characteristics and asthma-related results in cross-country skiers and controls
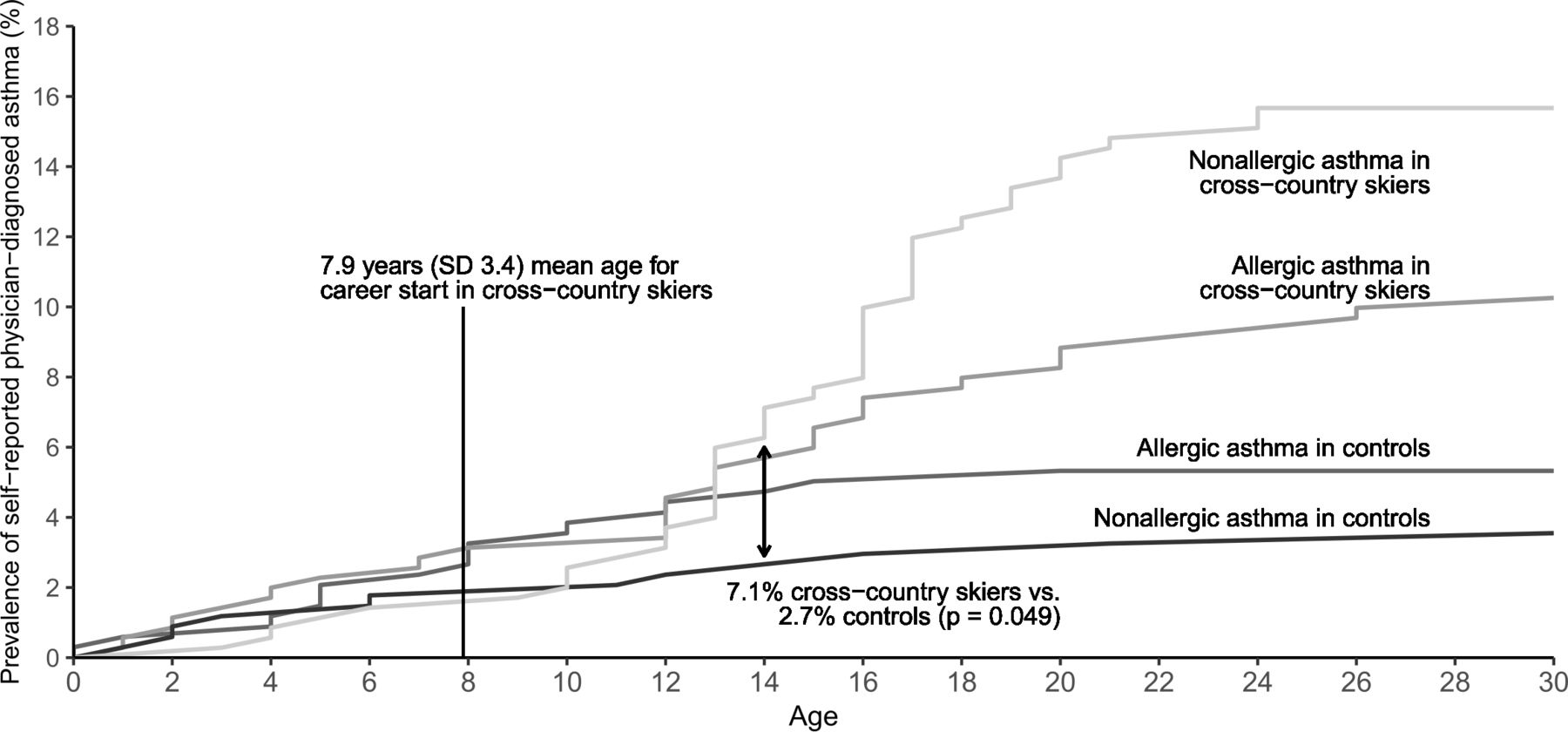
To illustrate the relation between age at asthma diagnosis and type of asthma, we calculated the prevalence of allergic and non-allergic asthma in skiers and controls based on their reported age at asthma diagnosis (figure 1). A rapid increase in the prevalence of non-allergic asthma occurs at 10 years of age in cross-country skiers. The difference in the prevalence of asthma between skiers and controls with non-allergic asthma was significant (p<0.05) starting from 14 years of age onwards. The difference in allergic asthma between skiers and controls was not statistically significant.

{kind=link}
Prevalence of self-reported physician-diagnosed asthma categorised as non-allergic and allergic in relation to age in competitive cross-country skiers and controls. The median (IQR) age at diagnosis of non-allergic asthma was 16.0 (13.0–17.0) years in cross-country skiers and 8.5 (2.3–15.5) years in controls (p=0.022). Age at diagnosis of allergic asthma was 13.0 (7.0–18.0) years in skiers and 8.0 (4.8–12.0) years in controls (p=0.018). A rapid increase in the prevalence of non-allergic asthma occurred at 13 years of age in the cross-country skiers. The difference in the prevalence of non-allergic asthma between the groups was statistically significant (p<0.05) from 14 years of age onwards but no difference in allergic asthma was significant.
Asthma in relation to performance level
In total, 163 (46.4%) skiers had participated in FIS competitions to earn FIS points. The prevalence of asthma and other asthma-related factors among these skiers are presented according to their performance level (table 2). In the most successful subgroup of skiers, as measured by the lowest FIS points, the prevalence of asthma was the highest (56.1%). This group was also the oldest and trained the most. The use of asthma medication differed between the groups, with more successful skiers using asthma medication. Asthma was well controlled in all subgroups. In skiers who did not report current asthma, 37.7% (98/260) reported that asthma had been suspected and investigated but not confirmed. In the subgroup analysis and based on the performance level, 85% of the skiers in the most successful quartile had been either investigated for, or diagnosed with, asthma. Skiers with asthma had lower (better) FIS points (SD) than skiers without asthma (173.22 (117.46) vs 213.65 (108.83), p=0.026).
Subject characteristics, training volume, prevalence of asthma, use of asthma medication and asthma control in cross-country skiers divided by performance level according to FIS points
Skiers who did not have FIS points consisted mostly of juniors under 16 years of age (n=132) who did not yet participate in FIS competitions and, to some extent, also of athletes over 16 years of age but who, for some reason, had not yet participated in FIS competitions to earn FIS points (n=56). In this population (n=188), 62.8% were female (n=118), 37.8% had a known family history of asthma (n=71), 62.2% were suspected of having or diagnosed with asthma (n=117), 14.9% had current asthma (n=28), 6.4% had allergic asthma (n=12), 8.5% had non-allergic asthma (n=16), and the median (IQR) ACT score was 23 (21–24). Median (IQR) age was 14.4 (13.6–15.7), and the median weekly training hours was 8.6 (7.0–10.5) hours. In addition, in juniors under 16 years of age, the prevalence of asthma was 16.7% (n=22).
Risk factors for asthma and its different phenotypes
The risk factors for current asthma in cross-country skiers and the controls are presented in table 3. In both groups, asthma in parents or siblings and allergic rhinitis were associated with current asthma. In cross-country skiers, older age, higher training volume and success—here as measured by FIS points—were also associated with current asthma. Being a cross-country skier was associated with OR of 3.47 (95% CI 2.23 to 5.38, p<0.001) for having asthma, 1.92 (1.08 to 3.42, p<0.027) for having allergic asthma and 5.05 (2.65 to 9.61, p<0.001) for having non-allergic asthma.
Univariate analysis of the risk factors for current asthma in cross-country skiers and controls represented as ORs with 95% CIs
Skiers’ risk factors for allergic and non-allergic asthma are presented according to the univariate and multivariate analyses in tables 4 and 5, respectively. We found that older age and higher training volume were associated with non-allergic asthma, while older age, family history of asthma and allergic rhinitis were associated with allergic asthma (table 4). In the multivariable analyses, the association between larger training volume and non-allergic asthma persisted, while older age, family history of asthma and allergic rhinitis were independently associated with allergic asthma (table 5).
Univariate analysis of the risk factors for allergic and non-allergic asthma in cross-country skiers represented as ORs with 95% CIs
Multivariable analysis for the risk of current asthma in cross-country skiers represented as ORs with 95% CIs
Two additional definitions of allergic asthma were used as a sensitivity analysis, and the results remained similar. See online supplemental file 1 for the full analysis.
Supplemental material
Discussion
From the same population, we have previously reported that there is more than a 2.7 times higher prevalence of physician-diagnosed asthma in competitive cross-country skiers than in the general population, along with a rapid increase in asthma prevalence about 5 years after starting a skiing career.16 In the current study, we found that asthma in skiers was mainly non-allergic compared with the general population of the same age. We also found that the rapid increase in asthma prevalence in skiers after the start of their careers is mainly because of non-allergic asthma. In skiers, higher training volume was associated with non-allergic asthma, while older age, family history of asthma and allergic rhinitis were independently associated with allergic asthma. In line with this, asthma was most prevalent among the most successful skiers who trained the most.
Prevalence and type of asthma
This is the first study to report the relative proportions of allergic and non-allergic asthma in competitive cross-country skiers and controls and assess the risk factors for different types of asthma in skiers. Our finding of higher asthma prevalence in competitive skiers aligns with many previous studies presented in our recent meta-analysis.8 Interestingly, the difference in the prevalence of asthma in skiers and controls seems to be mainly because of the excess prevalence of non-allergic asthma in skiers. The current findings suggest that intensive training in cold air is the trigger for inducing the excess of non-allergic asthma in skiers. The increase in the prevalence of asthma in skiers after their career started was mainly because of an increase in the prevalence of non-allergic asthma. During this time, young athletes also start increasing training volume and intensive training in the cold and participating in competitions over longer distances. Increased training volume was a risk factor for non-allergic, but not allergic, asthma. This relation between intensive training and non-allergic asthma might be related to airway damage caused by cold air because airway damage has been suggested as one of the risk factors for non-allergic asthma.4–6 The inflammatory mechanisms of non-allergic asthma can be non-allergic eosinophilic, neutrophilic, mixed or pauci-granulocytic.2 In biopsy studies, skier’s asthma is more neutrophilic than asthma in controls.12–14 Non-allergic eosinophilic asthma is more often severe with onset in late adulthood2 and, therefore, is not very likely among young competitive athletes with extremely good physical performance. The phenotypes of asthma in athletes have been previously categorised into atopic asthma and sports asthma by Couto et al,20 which were defined quite similarly as allergic and non-allergic asthma in this study.
Another key finding in our study was that before starting their skiing career, there was no difference in asthma prevalence between cross-country skiers and the controls and the controls mainly had allergic asthma. New cases of asthma in the Finnish population are mostly allergic until the age of 40, and in subjects of similar age to the current population, about 65% of asthma is allergic.7 This is in line with 61% of the control subjects with asthma in the current study reporting allergic asthma. The risk factors for allergic asthma in childhood are allergic sensitisation of the subject and parental asthma or allergy.4 This is in accordance with a family history of asthma and doctor-diagnosed allergy being risk factors for allergic asthma among competitive skiers in the current study.
Prevalence of asthma and competition success
To the best of our knowledge, this is the first study reporting asthma prevalence in cross-country skiers based on success in competitions. Interestingly, the prevalence of asthma was highest among the most successful skiers. This might be related to several factors. First, the most successful skiers also trained the most. If a high volume of training in cold air causes asthma, this might be the reason for the higher prevalence of asthma in the most successful skiers. To support this finding, athletes using β2-agonists in the Olympic games from 2002 through 2010 won approximately twice as many medals as their proportion of all athletes across all disciplines.15 Skiers also reported a high burden of respiratory symptoms.8 Another possible explanation for the high prevalence of asthma in the most successful skiers is related to the propensity to seek medical attention. The most successful skiers also invest the most in their careers so that they might seek medical help for any symptoms more often than the general population. This is supported by the high rate of suspicion for asthma in this group in the current study. Although the prevalence of asthma is very high among the most successful competitive cross-country skiers, they also seemed to have the best symptom control, even though the difference was not statistically significant. This suggests that asthma in skiers is often well controlled and mostly does not prevent success in skiing careers. On the contrary, it has also been discussed whether asthma could provide a training stimulus not available to non-asthmatic athletes.21
The current study’s categorisation of asthma as allergic and non-allergic asthma was based on a questionnaire rather than direct measurement of allergic sensitisation or allergen challenge tests. However, the results were similar with three different definitions of allergic asthma, supporting the robustness of our results. Relevant aeroallergens in Finland are pollens and pets, covered in our questionnaire. Because of dry indoor air during the cold winter, house dust mite is rarely a clinically relevant allergen in Finland.22
Limitations
The response rate in this study was relatively low (27.3% in skiers and 19.5% in the controls), but this is still the largest survey in competitive cross-country skiers based on the number of respondents (n=351). Self-reported, physician-diagnosed asthma is the most commonly used method to evaluate the prevalence of asthma. The tests used in each skier’s diagnostic workout could not be verified. However, in Finland, diagnosis of asthma is based on objective lung function measures because of the criteria for drug reimbursement. Asthma medication is fully reimbursed only if the diagnosis is based on such measures. Validation of self-reported asthma by lung function measures has been studied in a similar demographic population compared with the subjects in this study, finding that among Finnish university students aged 18 to 25 years, the specificity of physician-diagnosed current asthma was 99%.23 The present study was conducted in a single country, but the results are probably generalisable to all competitive cross-country skiers in other countries. Responses regarding age at onset of asthma symptoms and age at diagnosis of asthma might be subject to recall bias. However, the questions were similar for both skiers and the controls, so comparison of the groups should be reliable. In addition, skiers with poorly controlled asthma might already have quit, so the respondents in the study might be subject to survivor bias. Some adolescents might never have taken part in cross-country skiing because of respiratory health concerns. This type of cross-sectional study is also limited in investigating time effects.
Conclusion
We conclude that the excess prevalence of asthma among competitive cross-country skiers compared with that in the general population is mainly because of non-allergic asthma emerging a couple of years after the onset of an active skiing career. Among skiers, a high volume of training seems to be a risk factor for non-allergic asthma, which might be the reason for the highest prevalence of asthma in the most successful cross-country skiers. On average, asthma is well controlled in all success categories of competitive skiers and does not seem to prevent a successful career. However, the findings in this study are limited owing to the response rate. Prospective studies with direct measures of the type and level of airway inflammation would verify a causal relationship between training volume and the type, severity and prognosis of asthma in competitive cross-country skiers.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of Pirkanmaa Health Care District (R18108). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to thank Eero Hietanen and Larissa Erola from Finnish Ski Association for their help in contacting the athletes for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Twitter @rikhardfi
Contributors All authors designed the study. RM-H collected data. RM-H and HH conducted analyses. RM-H wrote the first version of the manuscript. All authors approved the final version. RM-H was the guarantor of the study.
Funding This study was financially supported by Tampere Tuberculosis foundation and Foundation of the Finnish Anti-Tuberculosis Association, Väinö and Laina Kivi Foundation, Ida Montin Foundation, Urheiluopistosäätiö, Allergy Research Foundation and The Research Foundation of the Pulmonary Diseases.
Competing interests The ICMJE forms are filled by all authors and declare no conflicts or interest that are relevant to this study.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.