Article Text

Abstract
Objective Football players are at risk of developing hip osteoarthritis (OA). Cam morphology (present in almost two of every three football players) may explain this heightened risk, but there is limited research on its role in hip OA development in younger athletes. Knowledge of this relationship will advance our understanding of the aetiology of hip OA in football players. We aimed to study the relationship between cam morphology size and MRI-defined cartilage defects and labral tears, and if this relationship differs by symptomatic state in young adult football players.
Methods For this case–control study, 182 (288 hips) symptomatic (hip and/or groin pain >6 months and positive flexion-adduction-internal-rotation (FADIR) test) and 55 (110 hips) pain-free football players (soccer or Australian football) underwent anteroposterior and Dunn 45° radiographs, and 3-Tesla MRI. Cam morphology size was defined using alpha angle, and cartilage defects and labral tears were scored semiquantitatively. Presence, location and score (severity) of cartilage defects and labral tears were determined. Each participant completed the International Hip Outcome Tool 33 and Copenhagen Hip and Groin Outcome Score.
Results Greater alpha angle was associated with cartilage defects (OR 1.03, 95% CI 1.01 to 1.04) and labral tears (OR 1.02, 95% CI 1.01 to 1.04). Greater alpha angle was associated with superolateral cartilage defects (OR 1.03, 95% CI 1.02 to 1.05) and superior labral tears (OR 1.03, 95% CI 1.02 to 1.05). The association of alpha angle with MRI-defined cartilage defects and labral tears was no greater in football players with symptoms than in those without (p=0.189–0.937)
Conclusion Cam morphology size was associated with cartilage defects and labral tears in young adult football players with and without pain. This study provides evidence that cam morphology may contribute to the high prevalence of hip OA in football players. Prospective studies of football players are now needed to establish if cam morphology causes progression of cartilage defects and labral tears and development of hip OA.
- rehabilitation
- hip
- football
- soccer
Data availability statement
Data (MRI and patient-reported outcome measures) are available on reasonable request. Suitability of data request and access to data will be determined by the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known?
Playing football is associated with an up to ninefold greater odds of developing hip OA in later life.
Cam morphology is present in almost two-thirds of football players.
Cam morphology is a risk factor for hip OA in middle-aged to older populations, but its role in the development of early hip OA features (cartilage defects and labral tears) in young adult football players is unclear.
What are the new findings?
Cam morphology (greater alpha angle) was associated with the presence, location and severity of MRI-defined cartilage defects and labral tears in young adult football players
The relationship between cam morphology size and MRI-defined cartilage defects and labral tears (presence, location and severity) was no greater in young adult football players with hip and/or groin pain (including a positive FADIR test) than in those without pain.
Introduction
Hip osteoarthritis (OA) is a leading cause of hip pain, disability and socioeconomic burden.1 Traditionally considered to have an idiopathic aetiology, recent evidence suggests that mechanical factors play an important role in hip OA development.2–4 For example, playing football is associated with an up to ninefold greater odds of developing hip OA.5 This may be related to the presence of cam morphology, which is characterised by extra bone at the anterolateral head–neck junction,3 and present in almost two-thirds of football players.6 7 Associations between cam morphology and hip OA have been demonstrated consistently across studies of non-athletic people, aged 50 years and older.2 8 However, this body of evidence adds little to our understanding of the role that cam morphology plays in hip OA development in younger football players.
In football players, cam morphology likely develops during adolescence.9 10 It is possible that early OA changes, which might include the pathological interaction between cam morphology and chondrolabral structures, first begins during this period. However, in a recent cross-sectional study, cartilage composition did not differ between adolescent football players with and without cam morphology.11 It is more likely that features of early OA (ie, cartilage defects and labral tears) gradually develop and only present in football players with cam morphology from early adulthood. However, little is known about the relationship between cam morphology and MRI-defined cartilage defects and labral tears in young adult football players.12
Our previous work showed that many football players with cam morphology, as well as those with cartilage defects and/or labral tears, do not report symptoms.7 13 However, no studies have examined the relationship between cam morphology and cartilage defects and/or labral tears, and symptoms in football players. The genesis of hip-related symptoms could relate to the presence, location and/or severity of cartilage and labral damage specifically in football players with cam morphology. If the relationship between cam morphology, intra-articular features and symptoms were better clarified, it may improve our understanding of the aetiology of hip OA.
The aims of this study were to: (1) examine the relationship between cam morphology size and the presence and severity of MRI-defined cartilage defects and labral tears in young adult football players with and without hip and/or groin pain; (2) examine the relationship between cam morphology size and the presence of cartilage defects and labral tears in specific anatomical subregions in football players with and without hip and/or groin pain and (3) investigate if the association between cam morphology size and cartilage defects and labral tears is stronger in young adult football players with hip and/or groin pain.
Methods
Study design and recruitment
This case–control study was nested within the femoroacetabular impingement and hip osteoarthritis cohort (FORCe) study. The FORCe study is a prospective study investigating changes to hip joint structures over a 2-year period in 184 subelite football players (soccer or Australian football) with long-standing hip and/or groin pain (>6 months) aged between 18 and 50 years, described previously.7 14 A convenience sample of 55 pain-free subelite football players aged between 18 and 50 years were recruited to match the mean age and sex distribution of the FORCe study and serve as control participants.7 Symptomatic and control participants competing in the same league/competition level were recruited between August 2015 and October 2018 from sporting clubs or via online and print advertising, with recruitment undertaken in Melbourne and Brisbane, Australia. The data for this study are taken from baseline examination. All study participants provided written informed consent prior to being involved in this study.
Study participants
Hip and/or groin pain group
Eligibility criteria are presented in online supplemental table 1. Briefly, inclusion criteria were self-reported hip and/or groin pain (>6 months in duration) that was >3 and <8 on an 11-point numerical pain rating scale with football or football specific movements; participation in ≥2 football sessions (training or competition) per week; a positive flexion-adduction-internal-rotation (FADIR) test, that elicited hip (anterior, lateral or posterior) and/or groin pain in at least one hip. Exclusion criteria were history of previous pathological hip conditions and radiographic hip OA (ie, Kellgren and Lawrence (KL) ≥2).
Supplemental material
Control group
For control participants, inclusion criteria were no prior history of hip and/or groin pain; participation in ≥2 football sessions per week; and a negative FADIR test in both hips (see online supplemental table 1). Exclusion criteria were similar to the hip and/or groin pain group, but also included previous lower limb surgery (eg, knee reconstruction).
Radiographs
Standardised supine anteroposterior (AP) pelvis and bilateral Dunn 45° radiographs were obtained for each participant. For the AP radiograph, the participant was placed in supine, with both legs internally rotated 15°. For the Dunn 45° radiograph, the hip was flexed to 45°, abducted 20° and positioned in neutral rotation.
Cam morphology
For each radiograph, one investigator (JH), who was blinded to clinical findings, positioned a set of landmark points to the surface of the proximal femur and acetabulum using statistical shape modelling software (ASM toolkit, Manchester University, Manchester, UK), followed by automatic calculation of the alpha angle (MATLAB V.7.1.0. MathWorks, Natick, Massachusetts, USA). Dichotomisation of continuous measures should be avoided in epidemiological studies.15 Thus, we present alpha angle as a continuous measure. For intraobserver reliability, the intraclass correlation coefficients (ICCs) for alpha angle were 0.92 and 0.93 for AP and Dunn 45°, respectively.7 Interobserver reliability ICCs were 0.76 for AP and 0.93 for Dunn 45°.7
MRI acquisition and scoring
All participants underwent a non-contrast 3 Tesla MRI (Phillips Ingenia, The Netherlands). Participants were positioned in supine, hips fixed in internal rotation and neutral abduction/adduction with patient positioning aids, and a 32-channel torso coil placed over the hips and pelvis, with right and left hips imaged separately. The MRI sequences acquired were coronal proton density (PD) spectral attenuated inversion recovery (SPAIR), sagittal PD SPAIR and oblique axial PD SPAIR (online supplemental table 2).
Each MRI was evaluated using the Scoring of Hip Osteoarthritis with MRI (SHOMRI) scoring system by one musculoskeletal radiologist (RS) with 8 years’ experience who was blinded to clinical and radiographic findings. Morphological changes to cartilage and the labrum are important features of early hip OA,16 and were selected as outcome measures. Cartilage defects were graded from 0 to 2 (0=no defect, 1=partial defect or 2=full thickness defect) and scored in 10 (4 acetabular and 6 femoral) subregions, providing a total cartilage score per hip of 0–20. A cartilage defect was present if a partial or full thickness defect was reported. For the superolateral, superomedial, anterior and posterior subregions, acetabular and femoral cartilage defects were combined. Labral abnormalities were graded from 0 to 5 (0=normal or normal variant (eg, aplasia, hypoplasia), 1=abnormal signal or fraying, 2=simple tear, 3=labrocartilage separation, 4=complex tear or 5=maceration) and scored in 4 subregions (anterior, posterior, anterosuperior and superior), with a total labral score per hip of 0–20. A labral tear was scored as present when graded ≥2. The SHOMRI subregions were used to describe the location of cartilage defects and labral tears for each hip. Intraobserver reliability was determined by 20 randomly selected hips being reread 2 weeks after the initial grading. Intraobserver agreement for cartilage defects and labral tears had prevalence adjusted bias adjusted kappa values of 0.76 (kappa 0.62) and 0.80 (kappa 0.77), respectively.13
Patient-reported outcome measures
For each participant, demographic characteristics were recorded and the International Hip Outcome Tool 33 (iHOT33)17 and Copenhagen Hip and Groin Outcome Score (HAGOS)18 were completed. The iHOT33 and HAGOS are recommended for young adults with hip and/or groin conditions19 20 and each contain several unique questions.21 The inclusion of both questionnaires provides a comprehensive understanding of hip and/or groin pain burden.
Statistical analysis
Data analyses were performed with Stata/IC V.16.1 for Mac (StataCorp). All analyses were undertaken at a per hip level, with cam morphology (evaluated as a continuous (alpha angle) variable) considered as the independent variable and cartilage defects or labral tears as the dependent variable. For the first study aim, logistic regression (presence of cartilage defects and labral tears) and negative binomial regression (severity of cartilage defects and labral tears) models with generalised estimating equations (GEE) (to allow for within-person correlation between right and left hip data) were used to determine whether cam morphology was associated with cartilage defects and labral tears. Models were checked for linearity of continuous alpha angle associations by graphical assessment and testing models with nonlinear terms for superior fit. Odds ratios (OR) and incidence rate ratios (IRR) with associated 95% CIs and p values are presented. For the second study aim, logistic regression models with GEE were used to estimate the relationship between cam morphology and the presence of cartilage defects and labral tears in specific anatomical subregions (cartilage defects=superolateral, superomedial and lateral; labral tears=superior and anterosuperior), with results presented as OR with 95% CI and p values. The remaining subregions for cartilage defects (inferior, anterior and posterior) and labral tears (anterior and posterior) were not compared statistically as there was a low prevalence in all hips. The probability (presence and location) and score (severity) of cartilage defects and labral tears were estimated for increases in size of cam morphology (5° increase in alpha angle) from regression models. For study aim three, an interaction term (alpha angle×symptoms) was incorporated into all regression models to test if the association between cam morphology and cartilage defects or labral tears was stronger in those football players with symptoms. For all analyses, symptomatic and control hips were combined, and models adjusted for sex, age, body mass index, KL grade and symptoms.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Participants
Of the 184 eligible football players, 182 (288 hips, 20% female, median age 26 (IQR 7), 50% soccer) were included (table 1 and online supplemental figure 1). The two excluded participants had incomplete MRI data. In 74 of 182 symptomatic football players, the contralateral hip was excluded as it did not fulfil study inclusion criteria. Twelve participants (22 hips with hip and/or groin and 2 control hips) had AP, but not Dunn 45° radiographs due to protocol deviations. A further two hips (two participants) with hip and/or groin pain were excluded due to the presence of hip OA. A standing and not a supine AP pelvis radiograph was taken in seven participants (14 hips) with hip and/or groin pain, with these radiographs included in the overall analysis. Fifty-five football players (110 hips, 25% female, median age 26 (IQR 8), 55% soccer) formed the control group (table 1 and online supplemental figure 2).
Demographic characteristics, radiographic and patient-reported outcome measures for hip and/or groin pain and control participants
Association between cam morphology and presence of cartilage defects and labral tears
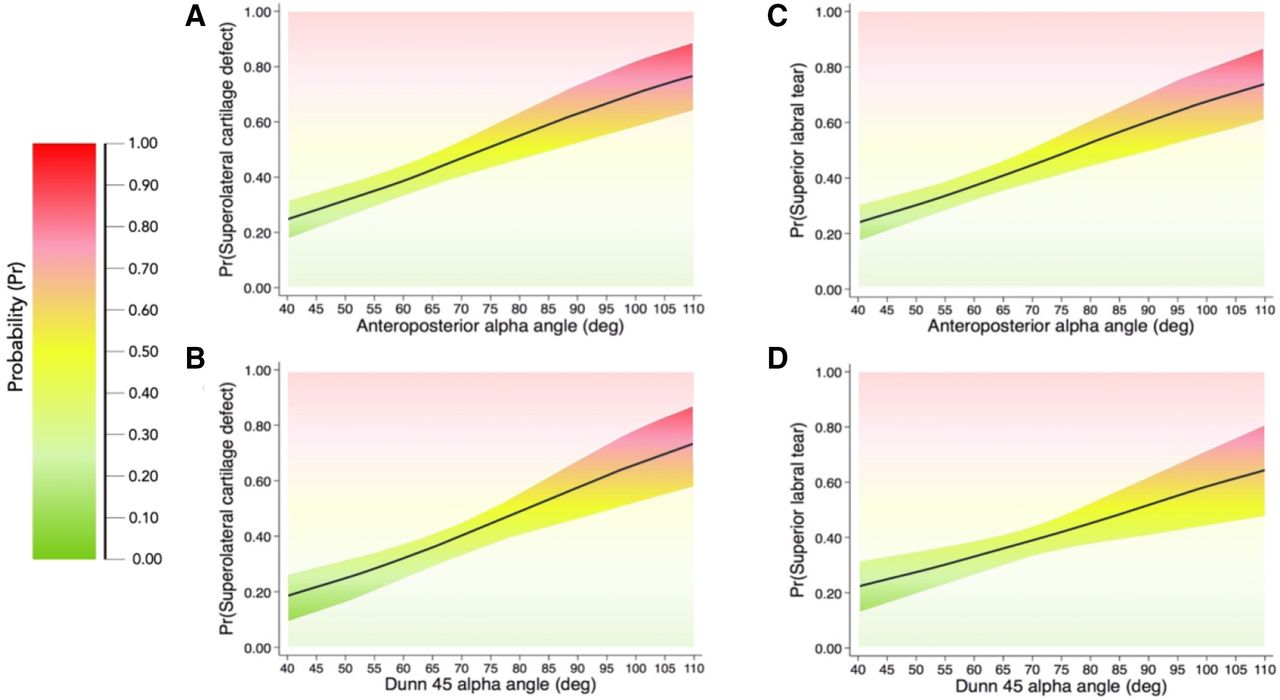
Greater AP and Dunn 45° alpha angle were associated with cartilage defects (table 2). Greater AP and Dunn 45° alpha angle were associated with labral tears (table 3). Figure 1 and online supplemental table 3 specify the probability of a cartilage defect or labral tear for a 5° increase in AP and Dunn 45° alpha angle.

Probability plots from 0 (0%) to 1 (100%) of cartilage defects and labral tears (presence) for values of alpha angle in 5° increments in all hips (hip and/or groin pain and control hips combined). (A) Cartilage defect (anteroposterior alpha angle); (B) cartilage defect (Dunn 45° alpha angle); (C) labral tear (anteroposterior alpha angle); (D) labral tear (Dunn 45° alpha angle).
Association between alpha angle and cartilage defects (presence) for all hips (hip and/or groin pain and control)
Association between alpha angle and labral tears (presence) for all hips (hip and/or groin pain and control)
Association between cam morphology and location of cartilage defects and labral tears
Greater AP (adjusted OR (aOR) 1.03, 95% CI 1.02 to 1.05; p<0.001) and Dunn 45° alpha angle (aOR 1.04, 95% CI 1.02 to 1.05; p<0.001) were associated with superolateral, but not superomedial or lateral cartilage defects (online supplemental table 4).
Greater AP (aOR 1.03, 95% CI 1.02 to 1.05; p<0.001) and Dunn 45° alpha angle (aOR 1.03, 95% CI 1.01 to 1.04; p=0.003) were associated with superior, but not anterosuperior labral tears (online supplemental table 5). The probability of a superolateral cartilage defect and superior labral tear for every 5° increase in alpha angle is presented in figure 2 and online supplemental table 6.
{kind=link}
{kind=link}
Probability plots from 0 (0%) to 1 (100%) of cartilage defects and labral tears (location) for values of alpha angle in 5° increments in all hips (hip and/or groin pain and control hips combined). (A) Superolateral cartilage defect (anteroposterior alpha angle); (B) superolateral cartilage defect (Dunn 45° alpha angle); (C) superior labral tear (anteroposterior alpha angle); (D) superior labral tear (Dunn 45° alpha angle).
Association between cam morphology and severity of cartilage defects and labral tears
Greater AP (adjusted IRR (aIRR) 1.01, 95% CI 1.00 to 1.02; p=0.017), but not Dunn 45° alpha angle was associated with worse cartilage score (online supplemental table 7). Greater AP (aIRR 1.01, 95% CI 1.00 to 1.01; p<0.001) and Dunn 45° alpha angle (aIRR 1.01, 95% CI 1.00 to 1.01; p=0.021) were associated with worse labral score (online supplemental table 8). Predicted cartilage and labral scores for every 5° increase in alpha angle is presented in online supplemental figure 3 and table 9.
Interaction between cam morphology and symptoms (hip and/or groin pain alongside a positive FADIR test)
There was no evidence for a difference in size of association between cam morphology and cartilage defects or labral tears between football players with and without symptoms (online supplemental table 10–15).
Discussion
Cam morphology (greater alpha angle) was associated with MRI-defined cartilage defects and labral tears in football players. Cam morphology was mostly associated with superolateral cartilage defects and superior labral tears. We did not observe a difference in the size of association between cam morphology and cartilage defects or labral tears in football players with and without symptoms.
Cam morphology and MRI-defined cartilage defects and labral tears in football players
Playing football is associated with an up to ninefold greater odds of developing hip OA in later life,5 but the underlying mechanism for this relationship has remained unclear. Cam morphology is a risk factor for hip OA in middle-aged to older populations,4 22 23 and thought to contribute to early hip disease in active football players.7 Our findings suggest that cam morphology size is associated with cartilage defects and labral tears in young football players (median age, 26), but that this relationship with joint damage is no greater in football players with symptoms (including a positive FADIR test) than in those without.
A dose–response association was found between cam morphology and MRI-defined intra-articular features in football players, similar to reports from people undergoing hip arthroscopy.24–26 For example, a 10° increase in AP alpha angle was associated with a small increase in the odds of having a cartilage defect (30%) or labral tear (20%). It is unclear if associations of this magnitude are of clinical relevance. It also remains unknown if the effect of cam morphology remains the same during the ageing process in football players and/or if cartilage and labral damage—which may be signs early OA—is expediated into hip OA in those with cam morphology.
Combined with others,27–30 our findings in football players might implicate cam morphology as a risk factor for early hip OA. The progression of joint disease may involve the interplay between bony parameters, hip and/or pelvic biomechanics and muscle function, and be unrelated to symptoms. Future well designed multicentre prospective cohort studies (to allow sharing of data) of athletes are needed to determine the role of cam morphology in symptom genesis and/or worsening, and hip OA development.
Location of MRI-defined cartilage defects and labral tears
Our semiquantitative MRI data support a pathomechanical model of femoroacetabular impingement syndrome with cam morphology, where premature contact between the proximal femoral head–neck junction and acetabular rim is associated with region-specific cartilage and labral damage.3 Higher alpha angle was associated with superolateral cartilage defects and superior labral tears, whereby, a 10° increase in AP alpha angle was associated with 1.34-fold increase in the odds of having either MRI finding. Mechanical abutment between the femoral head-neck junction and acetabulum may occur throughout the full arc of flexion in hips with larger cam morphology,31 which over time, could induce prolonged impingement and resultant damage to chondrolabral structures. Our findings suggest that MRI-defined chondrolabral damage corresponds to the location of cam morphology, and that the presence of this damage is associated with the size of cam morphology rather than the presence of symptoms.
Why do some football players with cam morphology and MRI-defined cartilage defects and labral tears remain asymptomatic and others do not?
Not all football players with cam morphology and coexisting cartilage defects or labral tears had hip and/or groin pain. The question then emerges, what factors differ in football players with and without pain? For many, their symptoms may emanate from structures external to the hip joint, even in the presence of cam morphology and intra-articular features. For example, clinical groin pain entities, such as adductor-related groin pain are present in close to 70% of players with long-standing symptoms.32 33 Also, we examined cam morphology in isolation from acetabular morphology and/or rotational aspects such as acetabular and femoral version. It could be that symptoms are only generated when specific femoral and acetabular bony parameters exist together alongside cartilage defects or labral tears.1 34 However, consideration of structural factors alone fails to appreciate the complex aetiology of pain.35 Joint injury (eg, labral tears) may occur without pain36 37 and pain may persists despite the completion of tissue healing.35 Long-standing hip and/or groin pain is often accompanied by altered psychological state, disturbed sleep and social limitations, which can all modulate pain levels.35 38 39 A symptomatic football player with cam morphology and MRI-defined intra-articular features requires a comprehensive assessment that considers the contribution of structural and non-structural factors.
Clinical implications
Young adult football players with cam morphology are likely to display MRI-defined cartilage defects and labral tears; however, the severity and extent of structural damage appears to be no greater in football players with symptoms (including a positive FADIR test) than in those without pain. Cam morphology is a risk factor for hip OA,4 22 23 but not all people with cam morphology develop symptoms40 or display progression of joint disease.4 Treatments targeting cam morphology (eg, surgery) can improve patient-reported outcome measures, but it is unknown if they are needed to slow the progression of joint disease in football players, without prospective studies.
The way that medical information is communicated can influence patients’ understanding of their diagnosis and treatment preferences. Information provided by healthcare practitioners can lead patients to believe their hip and/or groin pain and associated disability is solely caused by damaged intra-articular joint structures observed on imaging (eg, labral tears).41 This can result in patients seeking interventions that ‘cure’ structural joint damage, such as hip arthroscopy. When communicating hip joint imaging findings, clinicians should use consistent and non-threatening language, and provide patients with accurate epidemiological (ie, prevalence of hip joint imaging findings in asymptomatic populations of similar, age, sex and activity level) and prognostic information.42
Limitations
First, a number of different clinical entities may elicit symptoms in football players.43 We did not evaluate our football players for the presence specific clinical entities, including adductor-related, iliopsoas-related, pubic-related or inguinal-related groin pain, and some football players may have had coexisting conditions that contributed to their symptoms. The FADIR test is sensitive, but not specific to intra-articular hip conditions.44 It is possible that some football players did not have pain generated by intra-articular conditions. We used a single imaging parameter (ie, alpha angle) to define cam morphology. Other imaging measures (eg, femoral neck-shaft angle) are associated with symptoms and might play a role in the pathogenesis of cartilage defects and labral tears.45 46 The SHOMRI is a valid and reliable semi-quantitative measure for grading intra-articular features involved in hip OA.47 Not all intra-articular structures involved in the pathogenesis of hip OA are evaluated by the SHOMRI48 and other methods (ie, quantitative MRI) can be used to evaluate cartilage and labral integrity.30 49 It is possible that a relationship may exist between cam morphology and SHOMRI features not reported in this study (eg, bone marrow oedema, subchondral cysts), as found in previous studies.30 50–52 A single musculoskeletal radiologist completed the SHOMRI scoring for all hips and we did not determine inter-rater reliability. As a result, we may over or under-report the severity of MRI-defined features. The accuracy of contrast-enhanced MRI is superior to unenhanced MRI for assessment of cartilage and labral conditions,53 54 but high-resolution, unenhanced 3 Tesla MRI can provide comparable accuracy to contrast-enhanced approaches.55–57 Furthermore, contrast-enhanced MRI is associated with risk and not appropriate for asymptomatic populations.58 Our cohort consisted of young-adult football players who responded to study adverts or participated in information sessions; therefore, they may not be representative of all young adults participating in football. Despite the large sample size of this study (n=237) it is possible that we were underpowered to detect an interaction effect.59 The case–control design of this study precludes inferences of a cause-and-effect relationship between cam morphology and MRI-defined features.
Conclusion
In young adult football players, cam morphology size was associated with MRI-defined cartilage defects and labral tears. This relationship was no greater in football players with symptoms than without, suggesting a complex relationship between cam morphology, specific intra-articular features and symptoms. Clinicians who treat young football players with cam morphology should be careful with what they say and do–we do not yet know enough about the long-term consequences of cam morphology on joint structure and symptoms.
Data availability statement
Data (MRI and patient-reported outcome measures) are available on reasonable request. Suitability of data request and access to data will be determined by the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was obtained from the La Trobe University Human Ethics Committee (HEC 15-019 and HEC16-045) and the University of Queensland Human Ethics Committee (2015000916 and 2016001694).
Acknowledgments
The authors would like to thank the staff at Imaging at Olympic Park and Qscan radiology clinics, as well as the study participants, who all assisted in the collection of data for this study. MJS is supported by the La Trobe University Postgraduate Research Scholarship. KC is supported in part by funding from the National Health and Medical Research Council (NHMRC) project grant (GNT1088683).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jheerey, @JoanneLKemp, @DrTaniaPizzari, @mattgmking1
Contributors JH contributed to conception and design of the study, acquisition of data, analysis and interpretation of data, writing and revising the manuscript and is the guarantor of the study. RS contributed to scoring of MRIs and interpretation of data, revision of the manuscript and final approval of the article. AJS contributed to conception and design of the study, statistical analysis and interpretation of data, revision of the manuscript and final approval of the article. RA, JK, RS, TP, TL and SM contributed to conception and design of the study, revision of the manuscript and final approval of the article. MK, PRL and MJS contributed to conception and design of the study, acquisition of data, revising the manuscript and final approval of the article. KC contributed to conception and design of the study, obtaining funding, analysis and interpretation of data, revision of the manuscript and final approval of the article.
Funding The study was supported by an Australian National Health and Medical Research Council (NHMRC) project grant (grant number 1088683).
Disclaimer The funding body did not have a role in study design, collection, analysis and interpretation of data, writing of the manuscript or decision to submit the manuscript for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.