Article Text

Abstract
Nutrition is an undeniable part of promoting health and performance among football (soccer) players. Nevertheless, nutritional strategies adopted in elite football can vary significantly depending on culture, habit and practical constraints and might not always be supported by scientific evidence. Therefore, a group of 28 Portuguese experts on sports nutrition, sports science and sports medicine sought to discuss current practices in the elite football landscape and review the existing evidence on nutritional strategies to be applied when supporting football players. Starting from understanding football’s physical and physiological demands, five different moments were identified: preparing to play, match-day, recovery after matches, between matches and during injury or rehabilitation periods. When applicable, specificities of nutritional support to young athletes and female players were also addressed. The result is a set of practical recommendations that gathered consensus among involved experts, highlighting carbohydrates periodisation, hydration and conscious use of dietary supplements.
- soccer
- consensus
- elite performance
- sports and nutrition
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study. No data are available. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
There is a growing interest in establishing valid nutritional approaches that may enhance health and performance in elite sports; football is not an exception. Thus, it is now well established that food, dietary supplements or specific diets can improve performance, accelerate recovery or prevent injuries in football players.1
The importance of nutrition was newly recognised by UEFA (Union of European Football Associations) earlier in 2018, when a group of experts was established to specifically update recommendations on nutrition for football,2 following a more generic sports nutrition consensus.3 With a similar purpose, the Portuguese Football Federation established a network of nutritionists from elite football clubs in Portugal, aiming to discuss and outline current practices and find consensus in the practical application of nutrition-related strategies to promote health and improve performance for football players.
The meeting took place in Oeiras (Portugal) on 14 February 2020 gathering 17 out of the 18 nutritionists working in elite male football clubs in Portugal (Liga NOS) and 11 other experts, including sports nutritionists, sports scientists and team physicians working with elite football teams and academia. When preparing the consensus meeting that originated this manuscript, ethical considerations were addressed and, given this is a review and consensus work, it was assured no competing interests would emerge. As with similar publications,2–4 the authors received no funding, directly or indirectly, to produce this manuscript. An external medical writer attended the meeting and was responsible for reviewing all declarations produced by the authors. Overall, nutritional and physiological requirements for training and playing football were discussed. Also, body composition assessment methods and the potential role of nutrition in injury rehabilitation were addressed.
The participants agreed on focusing the discussion on nutritional considerations for adult, male, elite players for the current consensus. Although some authors might be working with female soccer individually, we could not discuss the evidence. No consensus has been established regarding the nutritional aspects for female soccer players. Given the relevance of such a topic, we would like to address this issue in future work. The discussion was organised according to a real-world timeline of the daily life of a football player: preparing to play, match-day (MD) and recovery between training sessions and matches. As a starting point for the discussion on each topic, the physical and physiological demands of training and MD were presented so that a more comprehensive understanding of the nutritional requirements could be determined.
Nutrition should start from understanding the physical and physiological demands of football
Football is described as a high intensity intermittent, non-cyclic sport, with several maximal or near-maximal activities interspersed with low or moderate-intensity periods of activity.5 Although most of the time is spent walking or running at low speed, matches are decided by actions performed at higher intensities (eg, sprints, accelerations, tackling, jumping, duels). Total distance covered can range from 9816 to 12 277 m, from which 681–881 m are covered at high intensity,6 and top speed during matches can reach >31 km/hour.7 This means that despite the meaningful differences between the physical demands of players, both aerobic and anaerobic energy pathways are required during a match. It has been estimated ~1106 kcal of mean energy expenditure for a football match,8 and daily energy requirements for elite football players are set to be ~3566 kcal.9 These values are lower for elite female players, with mean values for match day, training days and rest days being 2914, 2783 and 2213 kcal, respectively.10
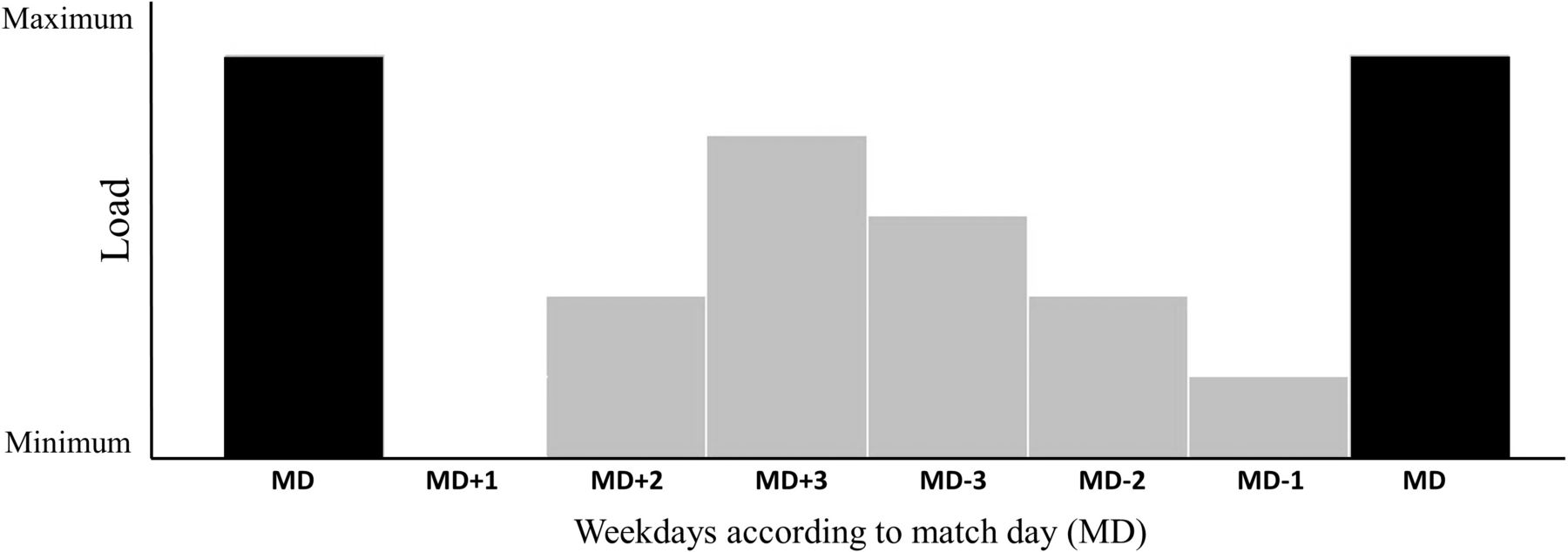
In football, training might be planned in relation to the distance to and from the MD,11 as it is the most demanding exercise session of the week. For this reason, it is common to categorise the days in weekly plans as MD– and MD+ (eg, the day before the match is MD–1, and the day after the match is MD+1). For a typical once-per-week match cycle, a conceptual model might be used to define training: MD+1 might be focused on recovery; the following days, training load might increase consistently; and finally, on MD–2 and MD–1, training load might decrease, so that players are at their highest capacity on MD. Moreover, training sessions last less (typically, 60–90 min) and have lower intensity than matches. Overall, a conceptual framework for the football training cycle with one match per week is outlined in figure 1.

Conceptual framework for the football training cycle with one match per week.
Still, congested fixtures are a reality in football, and teams might need to play more than one match per week for several weeks. This impacts programming training loads; for instance, MD+2 can be simultaneously MD−1, and matches can be distanced by only 72 hours, which may limit recovery and increase injury risk.12 Overall, a conceptual framework for the football training cycle with two matches per week is outlined in figure 2.

{kind=link}
{kind=link}
Conceptual framework for the football training cycle with two-three matches per week.
Nutrition should contribute to preparing players to play
Pre-match nutritional strategies may consider the period from MD–2 to the last main meal before players go to the dressing room at the stadium. Match performance can be affected by nutritional choices from MD–2 onwards, namely if carbohydrate intake is not adequate or hydration is inappropriate. Glycogen is an important energy source for football-specific high-intensity intermittent demands, but glycogen storage in the muscle is limited.13 Thus, it is fundamental that players start the match with muscles filled up with glycogen. This means carbohydrate ingestion is key in preparing to play. Still, several other nutrients and substances should also be considered when establishing the nutritional strategies from MD–2 to MD.
Carbohydrates
MD–2 and MD–1 might still include training sessions that may demand muscle glycogen. Therefore, the last 2 days before the match should consider nutritional strategies to stimulate or optimise glycogen storage. To achieve this goal, actual recommendations support the ingestion of 6–8 g/kg/day of carbohydrates in the 24–48 hours before the match.2 9 Based on their practice, the authors recognise that such recommendations may lead to optimal glycogen storage but achieving this carbohydrate ingestion may be difficult for several players. Available literature shows that the average carbohydrate content of the pre-match meal (<1.5 g/kg body mass) was lower than recommended (2–3 g/kg body mass).14 15 Nevertheless, this might not be a problem if training loads decrease from MD–2 and carbohydrate intake keeps roughly the same. Monitoring players' food intake (eg, carbohydrates and total energy) and training loads may be key to determining each player’s nutritional needs and, therefore, establish tailored nutritional interventions.16 The authors agree that regular diet recalls or food frequency questionnaires conducted by trained practitioners are useful and easy-to-use tools to adjust nutrients intake according to player’s needs.
Fibre and fats
When applying retrospective methods for food assessment, it is important to monitor fibre and fat intake due to potential effects on slowing gastric emptying, impairing nutrient absorption in the small intestine and invoking gastrointestinal discomfort.17
Dietary fibres are considered an important nutrient in healthy eating, but athletes often reduce their ingestion in the days before competitions, particularly in endurance sports.18 Since the possible impact of fibre ingestion in football performance is short-termed, the authors considered that players’ diet should consistently attend the European Food Safety Authority (EFSA) dietary reference values (DRV),19 set at 25 g/day for adults (adequate intake). A reduction of fibre ingestion could be limited to MD, depending on individual tolerance.
Regarding fat intake, a recent meta-analysis20 suggested overall fat ingestion among football players has been decreasing in recent years, representing less than 30% of total energy intake. Regarding the type of fat, there is not enough evidence to establish specific recommendations for football players, so EFSA DRV should be used as a guideline.
Protein
Dietary protein is necessary to support metabolic adaptation to training and protein turnover from muscle repair and remodelling. However, there is no evidence of benefits associated with acute protein intake in preparing to play. Since the mid-1990s, protein intake recommendations for football players have consistently ranged between 1.2–2 g/kg/day.21 22 Accordingly, protein intake observed among adult players is ~1.8 g/kg/day, and ~1.9 g/kg/day in youth players.20 Finally, current recommendations for protein intakes during weight loss in athletes were set at 1.6–2.4 g protein/kg/day.23 Special attention should be given to vegan athletes and those trying to reduce their energy intake to control body fat mass because total protein requirements may not be achieved.24
Hydration
Dehydration can significantly impair physical and cognitive performance in sport.25–27 Factors such as weather conditions (eg, temperature and humidity), travelling, fluid availability and sweating may influence hydration status and optimal conditions to play. Sweat rates change with environmental temperature during exercise28 and can range between 1.13±0.30 L/hour, 0.71–1.77 L/hour in cool temperatures (5±1°C) and 1.46±0.24 L/hour, 1.12–2.09 L/hour in hot weather (37±3°C).29 Furthermore, under the same environmental conditions, sweat rates can vary significantly at the individual level.30
Assessing hydration status is challenging as every method (eg, bioimpedance, weight control, urine colour scales) has its limitations.31 Still, urine specific gravity tests and urine colour are reliable, easy-to-use methods.
Overall, the authors gathered consensus on the following recommendations when preparing to play (table 1).
Nutritional Strategies when preparing to play from MD–2 to MD (until the last main meal before the match)
Nutritional strategies during the match—from arrival to the stadium to the final whistle
Nutritional strategies during the match typically include the 90–120 min preceding kick-off and the 90-min match (120 min with extra time). The main goals are to ensure enough energy to play and an adequate state of hydration. Additionally, some strategies of acute effect can be applied to improve performance or prevent fatigue during the match. However, nutritional strategies for the match should be mindful that some players will play the full match, while others will only play sometime or even not play at all. Moreover, specific positions such as goalkeepers may have different needs.
Carbohydrates
Current recommendations to ensure energy availability for the match suggest an intake of 30–60 g of carbohydrates during the match.32 33 Ingesting such an amount of carbohydrates might not be easy, despite the clear advantages in doing so (eg, improving the ability to perform high-intensity intermittent actions).34 35 Interestingly, such benefits are not evident for sprint, change direction or specific skills.36 Similarly, the effects of carbohydrate intake on the ability to jump and cognitive function (attention and response time) appear to be minimal.36
Authors recognise that frequent carbohydrates choices among players on MD include beverages (isotonic or not), gels or bars with carbohydrates mixtures (eg, glucose, maltose, maltodextrin) and fruit or derivatives (eg, fruit bars or purees rich in fructose and glucose). The diversity of carbohydrates present in these products raises questions about their absorption, namely the possibility of causing glycaemia peaks and consequent reactive hypoglycaemia. However, this hypoglycaemia seems rare, transient (~10 min during exercise) and might have little impact in soccer-specific efforts.37 38
Most studies focused on determining the most appropriate carbohydrate, favouring those with rapid digestion, absorption and oxidation (eg, glucose, sucrose and maltodextrin).39 Maltose and amylopectin have also emerged recently, with equal metabolisation profiles. Keeping in mind that in football, hardly more than 60 g/hour will be necessary, the issue of varying the type of carbohydrates may not arise due to the unlikely saturation of their co-transporters sodium-glucose linked transporter 1 in the intestine.
Hydration
To prevent players from starting the match hypohydrated, athletes should fractionally drink small amounts of fluids before kick-off and during or right after the warm-up: 5–7 mL/kg body weight in the 2–3 hours before match.40 Monitoring hydration status during this period might be difficult to perform, so athletes should be advised to ensure adequate fluid intake since the feeling of thirst changes with effort41 and players may not realise their hypohydration promptly.
The American College of Sports Medicine position stand42 highlighted the benefits of using a drink with sodium and potassium (osmolality 20–30 mEq/L and ~2–5 mEq/L, respectively) to compensate for electrolyte losses in sweating. This recommendation recognises that sweating rates vary among individuals due to intrinsic or environmental conditions. The inclusion of sodium may also have the effect of stimulating thirst and forcing fluid intake. As for the inclusion of carbohydrates in the drink to be used during the game, drinks with 6%–8% carbohydrates (eg, glucose and sucrose) may be beneficial in maintaining performance in intermittent efforts.43 44 Drinks with carbohydrate content greater than 8% (without maltodextrin) should not be recommended, as they may delay gastric emptying.45–47
In summary, since sweat losses can vary significantly among professional players during a match (1680±500 mL to 4448±1216 mL),48–50 fluids (including water or a sports drink with electrolytes and carbohydrates) should always be available. Athletes must be encouraged to drink in every opportunity, to minimise perspiration losses.
Caffeine
Caffeine is one of the most popular supplements among athletes. Its stimulant effect is long known. The International Olympic Committee consensus statement for dietary supplements stated that ingesting 3–6 mg/kg of caffeine 20–60 min before exercise can improve performance.3 Lower doses (<3 mg/kg) may also enhance performance,51 52 particularly in female or younger athletes. The possibility of some athletes being non-responders to caffeine ergogenic effects should also be considered.
For an average 75 kg athlete, caffeine intake for ergogenic purposes could range between as low as 75 mg (barely under the average caffeine content of an espresso cup) or as high as 450 mg (as much as 1.4 L of a typical energy drink). This raises the question of how much caffeine is too much. Concerns regarding potential adverse effects on fluid balance in caffeine consumers are unfounded,53 particularly in exercise settings. Since caffeine sources are largely available (eg, coffee, energy drinks, gels, pills or chewing gums) and individual response may vary considerably,54 personalised strategies should be planned and tested in advance to achieve individual tolerable and effective intakes. For some players, it might be easier to ingest caffeine in pill form with usual fluids. Others might prefer caffeinated carbohydrates gels. When a precise amount of caffeine is not required by players, coffee might also be used.
Notably, additional caffeine intake during half-time may not be recommendable since it takes 20–60 min for its effect to occur, which in turn extends between 2 and 12 hours after ingestion.55 But for substitute players, who cannot predict if or when they will be called to play, caffeinated chewing gum may be an option since caffeine absorption is faster.56
Pickle juice
The use of pickle juice in situations where athletes report of cramps has become common in recent years. About 25% of certified trainers recommended using pickle juice to prevent and treat exercise-associated muscle cramps.57 Still, evidence supporting the efficacy of pickle juice in rapidly replenishing electrolytes in plasma lacks.58 59
Its mechanism of action in cramps is not yet fully understood. Studies carried out with electrical stimulation-induced cramps (different from exercise-associated muscle cramps) suggest that the ingestion of pickle juice triggers a reflex in the oropharyngeal region, which reduces the alpha motor neuron pool activity.60 Considering the evidence yet available, it is premature to recommend using pickle juice to prevent exercise-associated muscle cramps. Notwithstanding, pickle juice can be considered for the acute relief of reports generated by exercise-associated muscle cramps if players demand it. For this purpose, about 1 mL/kg of pickle juice can be used,60 typically in the form of available flavoured prepacked 75 mL bottles, to increase players adherence.61
Protein and amino acids
Recently, a set of ready-to-drink products with added protein or amino acids (particularly branched-chain amino acids, BCAA) have emerged. These formulas are advertised as being able to minimise the harmful effects of exercise on muscles if taken before or during exercise. However, the existing literature showed limited benefits in ingesting amino acids/protein during exercise.62 Considering that protein intake is current practice during recovery, practitioners’ use of BCAA alone in MD should be questioned.
Recommendations for MD
The MD demands total focus from players. Opportunities for nutritional interventions are limited and should be defined at the outset. Since arrival to the stadium, during warm-up and at half-time, food, drinks or supplements should be readily available in the locker rooms. Fluids or selected snacks should be available on the bench to be provided to players during the match, if appropriate. And, for matches that contemplate the possibility of extra-time (ie, knock out matches in tournaments or play-offs), support staff should focus on hydration and energy supply63 during the short break after regular time.
Overall, table 2 summarises the nutritional strategies for the playing period.
Nutritional strategies to be used on match-day (from the arrival to the stadium until the end of the match)
Nutrition should be part of recovery—from the end of the match to MD+2
After a typical football match, players need to recover from the physical, physiological and mental demands of the game.5 64 65 Recovery strategies include a myriad of procedures besides nutrition, such as cold-water immersion, sleep, active recovery, stretching, compression garments, massage, electrical stimulation, among others.66
In the nutritional context, the 3-R strategy might apply rehydration, replenishment (of muscle glycogen) and repair (of muscle fibres). It is necessary to distinguish acute nutritional strategies to be implemented soon after the end of the match from those that will follow the following 48 hours.
Rehydrate
Among the 3-R rule of recovery, rehydration is almost unanimously the first to be put into practice. After the match, players commonly feel thirsty and might be more willing to drink. This is positive because adequate rehydration is also part of muscle glycogen replenishing and protein synthesis in the muscle.67 Adequate rehydration is attained by drinking 1.5 L/kg of body weight lost, preferably up to 2–4 hours after the match.25
We should bear in mind electrolyte content lost by perspiration when choosing fluids to be used for rehydration. Rehydrating with only water can increase up to three times the time required to restore plasma volume.68 Also, it may increase diuresis and inhibit the feeling of thirst, thus limiting the necessary fluid intake for rapid rehydration. On the other hand, beverages with sodium content greater than 600 mg/L induce lower urine production, a greater increase in plasma volume and faster re-establishment of water balance.68
Alcohol intake is not recommended during the recovery period. We acknowledge the social and celebratory context associated with alcohol consumption, but we cannot neglect its negative effects on normal immunoendocrine function, blood flow and protein synthesis.69
Refuelling
Muscle glycogen stocks can be significantly depleted during a match, making carbohydrate intake a key factor for fast recovery. Muscle glycogen synthesis occurs at a maximal rate for approximately 4 hours after the match if enough carbohydrates are consumed.70 71 Low energy and carbohydrate intake in the 24 hours after the match compromise the ability of players to train up to 72 hours.72
To maximise muscle glycogen synthesis, ingesting 1–1.5 g/kg/hour of carbohydrates in the first 4 hours after the match73 or 0.8 g/kg/hour if combined with 0.2–0.4 g/kg/hour of protein72 have been recommended. This means a significant amount of food to be consumed. Therefore, carbohydrate intake should be split into several meals and snacks, including different sources (eg, food, beverages, gels). Fractioning carbohydrates intake in shorter periods showed better results in glycogen synthesis when compared with a more widely spaced intake.74 Finally, regarding the type of carbohydrates to be used, several studies support those with a higher glycaemic index.75
Since it is not always feasible to ingest the recommended amounts of carbohydrates immediately after the match, specific strategies may be considered to accelerate muscle glycogen synthesis. Notably, carbohydrates could be associated with protein intake (≥0.3 g/kg/hour of protein when carbohydrates intake is less than 1.2 g/kg/hour).75 Protein is a key nutrient to be included in recovery strategies, particularly because of its role in repairing muscle fibres. Hence, joint strategies for protein and carbohydrates intake should be considered.
Repairing
A significant number of eccentric muscle actions and various muscle-damaging actions occur during a football match.76 These might harm muscle fibres.
Both exercise and protein intake have an anabolic effect. Therefore, post-match meals should include sources of essential and non-essential amino acids that promote myofibrillar protein synthesis. Despite common belief, there might not exist an anabolic ‘window of opportunity’, that is, a period immediately after exercise when ingesting protein would be beneficial.50 Ingesting 20–40 g of quality protein (ie, with all amino acids) up to 2–4 hour after the match may be enough to prompt protein synthesis in the muscle.
Other nutrients and substances for recovery
Aiming to accelerate or enhance recovery after a match, several nutrients and substances have been used. We selected those with acute effect immediately after the match.
Tart cherry
Tart cherry concentrates are rich in phytochemicals with antioxidant and anti-inflammatory properties. Continuous supplementation with tart cherry concentrates (ie, 30 mL two times a day, for at least 7 days) is common practice, but no studies with a single intake after exercise have been documented. As far as sleep is concerned, tart cherry supplementation can improve sleep time and quality (measured using subjective questionnaire and actigraphy), particularly after intense exercise, since it increases circulating melatonin levels.77 78 But since Montmorency cherries and their concentrates have been reported to reduce inflammatory response after exercise, it is questionable if there are benefits in its use when focusing on developing adaptations.79 Thus, tart cherry concentrate can be useful to promote rest and recovery, particularly when matches are frequently played at night.
Antioxidants
Several substances with potential antioxidant effects have been studied regarding performance improvement or accelerating post-exertion recovery.80 However, continued intake of different substances with potential antioxidant effects may be more harmful than beneficial.81 While the occasional intake of some of these products may have advantages (eg, reducing delayed onset muscle soreness), it seems preferable to ingest the involved nutrients through antioxidant-rich foods.
Nutritional strategies in MD+1 and MD+2
Despite the importance of nutritional strategies in recovery soon after the match, various recovery mechanisms continue to occur until MD+2, namely muscle protein synthesis and glycogen replenishment.76 82 83 Therefore, it is appropriate to ensure the intake of certain nutrients during this period.
Players may not properly rehydrate after a match due to the lack of willingness to drink, fear of interrupting sleep to urinate or travel-related constraints. Therefore, we recommend that an array of fluids and foods with higher water content be available during this time frame. Validated urine colour scales can help players assess their hydration status, and monitoring players body mass variation (assuring weight loss is under 2% of body weight) during MD+1 and MD+2 contributes to proper rehydration.
Although the rate of glycogen synthesis is reduced 4 hours after the match, it is important to continue with appropriate carbohydrate ingestion.84 Glycogen synthesis remains stable with an intake above 7 g carbohydrates/kg.4 To prevent weight gain, it is not necessary to increase daily carbohydrates intake, and the option for faster digestion and absorption of carbohydrates is no longer imperative.
Protein intake in MD+1 and MD+2 must be aligned with the usual requirements: 1.6 g/kg/day distributed fractionally every 3–4 hours to ensure optimal protein synthesis, allowing both muscle repair and adaptation processes.
Congested fixtures
When the interval between matches is short (<72 hours), the recovery period may overlap with the preparation for the following match. It should be noted that the proximity between matches (two to three matches per week vs one match per week) increases the risk of injury and can compromise a player’s performance.85 In this scenario, it is important to support a fast and effective recovery of players, which should include nutritional strategies.
For this purpose, the importance of carbohydrate intake should again be highlighted. With a short time between matches, rapid replenishing of muscle glycogen is a priority. Also, protein intake should be monitored to ensure the repair and adaptation of muscle tissue. Additionally, nutritional strategies can be considered to reduce inflammation and muscle soreness. Anything that may accelerate recovery might have practical interest, although evidence around some commonly used solutions (eg, omega-3, tart cherry concentrate, pomegranate juice) is still limited.
Overall, a set of nutritional recommendations for recovery on MD, MD+1 and MD+2 is summarised in table 3.
Nutritional strategies for recovery (from the end of the match to MD+2)
Nutrition is also crucial between matches, all season long
Beyond MD–2 to MD+2 nutrition can play an important role in athletes’ preparation.
Manipulating body composition or testing strategies during matches are tasks that nutritionists can develop throughout the season on non-competitive days. Also, food education of athletes should be fostered within these periods, particularly by ensuring that players learn to follow a varied, balanced and adequate diet. It is also important to mention that goals of nutritional interventions between matches may vary throughout the season. During pre-season, body composition control and optimisation of training adaptations can be a priority, while at the off-season, attention may be focused on weight management. Thus, four key areas of intervention can be outlined: (1) food education, (2) monitoring and manipulation of body composition, (3) definition and testing of supplementation strategies and (4) nutritional strategies to be applied in injury rehabilitation periods.
Food education
Nutritional strategies to be applied between MD–2 and MD+2 may be of little use if the athlete has a poor baseline diet. Implementing appropriate food choices on MD–1 and MD only is insufficient to ensure proper nutrients supply and generate desired training adaptations.
A recent meta-analysis20 revealed that carbohydrate intake in both young and adult players is below the recommendations (5.5–5.9 and 4.3–5.0 g/kg/day; respectively), whereas daily protein intake is higher than recommended (1.8–2.0 and 1.6–2.0 g/kg/day, respectively). Low carbohydrate intake in football players raises concerns about energy necessary to play and appropriate replenishment of muscle glycogen. On the other hand, although slightly above the recommendations, protein intake does not raise concerns in healthy individuals. Interestingly, a trend towards a decrease in daily ingested calories adjusted to body mass has been reported. Given that football’s physical and physiological demands have been increasing over time,86 both reductions of carbohydrates and energy intake should be acknowledged.
A complete nutritional assessment at the beginning of each season is recommended for better knowledge of individual eating habits and body composition. Body composition assessment (via DXA, BIA or perimeters and skinfold measurement, depending on available resources), food frequency questionnaires plus self-reported food records and blood analysis for the biochemical profile are part of the usual procedures. This evaluation enables the definition of personalised nutritional intervention strategies for each player, focusing on tailored intake of nutrients, adjusted to training loads and goals of body composition manipulation. Team nutritionists must liaise with the multidisciplinary health and performance team, aiming for adequate knowledge of training goals and their adaptations. After the initial nutritional evaluation and consequent intervention, follow-up moments should be defined throughout the season to assess and adjust strategies. In addition to individualised work, nutritionists should also define and monitor squad meals, ensuring each athlete finds the food options to their liking. Regular contact with the players throughout the season is of utmost importance to an appropriate assessment of interventions and the necessary adjustments.
Body composition
It is difficult to determine the precise influence of body composition on performance,87 but body composition optimisation may improve training adaptations and develop interventions aiming to enhance performance. For instance, a higher percentage of fat mass is negatively associated with a 20 m sprinting speed.88 Though body composition may vary throughout the season89 it is important to put individual scores into perspective.
Although body composition might relate to food intake, it does not exclusively depend on it.90 There are several techniques for assessing body composition, all with advantages and disadvantages.91 Specifically, the authors recognise that skinfolds and perimeters measurement are the most commonly used methods in football.
Regarding body composition manipulation, nutritional strategies should be aligned with other interventions, particularly specific individualised training programmes. Thus, a careful and personalised approach is warranted for players to reduce fat mass or aim to increase muscle mass.90
Dietary supplements
For this document, the authors considered the IOC definition of dietary supplements: ‘a food, food component, nutrient or non-food compound that is purposefully ingested in addition to the habitually consumed diet to achieve a specific health and/or performance benefit’.3
Safety is the main issue when considering the use of dietary supplements. Estimates indicate that 12%–58% of food supplements on the market contain substances that can positively result in an anti-doping control.92 Since quality control of dietary supplements is the sole responsibility of the manufacturers, it is necessary to ensure that products supplied to players are not a source of prohibited substances, both intentionally and accidentally. The use of products tested in independent laboratories duly credited for this purpose is an additional guarantee of safety. It is important to ensure that batches to be consumed by athletes have been effectively tested in these cases.
When planning nutritional strategies to support football players, it is important to distinguish between dietary supplements taken sporadically (acute effect) and continuously (when the goal is to fill nutritional deficiencies or when ergogenic benefits are obtained with prolonged intake). Here, we only addressed substances with evidence to support their use in football.
Creatine
Creatine is synthesised in the human body and obtained through food (main sources are meat and fish). Creatine supplementation (the most frequently used form is creatine monohydrate) aims to increase its concentration in the muscle to accelerate phosphocreatine re-synthesis, thus improving performance in repeated bouts of short duration, high intensity exercises.93
Typically, creatine supplementation is done with a loading phase (a higher dose for approximately 1 week), followed by a maintenance phase (lower dose, maintained for longer periods of at least 28 days).94 Concerns about fluid retention with high doses explain why the most common protocol in football encompasses 20 g/day for 5 days (to quickly increase creatine reserves in the muscle), followed by a steady dose of 3–5 g/day. The loading phase is frequently suppressed (especially if there is no urgency in obtaining a more immediate response), relying on a continued intake of 3–5 g/day, depending on body weight and individual tolerance.95
Creatine supplementation may also be of interest as a booster of muscle glycogen replenishment.96 On MD, creatine should be taken after the match because of the benefits mentioned above in accelerating muscle glycogen replenishing.
However, potential side effects (eg, fluid retention) and the existence of non-responders should be considered.97
Nitrate
Nitric oxide (NO) is a molecule involved in regulating blood flow and mitochondrial respiration. Dietary nitrate supplementation (particularly beet juice concentrates) aims to increase NO production and thus obtain benefits in prolonged submaximal efforts and intermittent, short-term high-intensity exercises.98
The use of beet juice concentrate supplements, taken in shots with ~400 mg nitrate, has become frequent in soccer.99 However, it is uncertain how supplementation should be conducted (ie, acute, before exercise or continued) and what benefits can be expected, particularly in trained athletes.100
Although no adverse effects of nitrate supplementation are known, some athletes may be more susceptible to gastrointestinal disorders. Athletes must be aware that supplementation with beet juice concentrate can give a reddish colour to urine, limiting the use of urine colour scales in the surveillance of the hydration state.
Beta-alanine
Beta-alanine is a non-essential amino acid and is the precursor of carnosine, an important intracellular buffer. Carnosine oral supplementation is ineffective because it is metabolised before reaching the muscle. Beta-alanine supplementation increases carnosine content in the muscle and delays pH drops induced by exercise. Increased carnosine levels may attenuate the build-up of fatigue, allowing the strength and power needed for high-intensity actions such as sprints or jumps.101
The typical protocol for beta-alanine supplementation consists of a continued intake (for at least 28 days) of 4–6 g per day, which can be divided into smaller doses of 2 g to avoid gastrointestinal discomfort and reports of paraesthesia.102 The performance benefits, particularly in football, seem to be limited. That can be explained by high inter-individual variability and that supplementation efficacy is less evident in trained athletes.103
Sodium bicarbonate
Sodium bicarbonate (NaHCO₃) is an alkalising agent of the blood and the muscles.104 The evidence on the benefits of using NaHCO₃ in football is limited and restricted to intermittent high-intensity exercises.105 Gastrointestinal disorders associated with NaHCO₃ intake may be reduced or eliminated when progressive increases in daily dose (up to 150 mg/kg of body weight) are adopted.106 Given the small extent of possible performance gains, the benefits of NaHCO₃ supplementation in football are doubtful.
Vitamin D
Vitamin D is primarily synthesised in the human body with sunlight exposure. Additionally, foods like fatty fish and egg yolk also contain variable amounts of vitamin D. Supplementation has become popular in recent years as assessment of 25-hydroxy vitamin D levels became more frequent and low values have been found among athletes.107 Insufficient vitamin D in serum has been associated with increased risk of bone disease, cardiovascular diseases, hypertension and infectious diseases.108 Considering that synthesis through the skin is variable (depending on weather conditions, latitude, season, use of clothes or sunscreen and skin pigmentation) and that dietary intake is frequently not sufficient (particularly in vegan athletes and those with low fish consumption,24 supplementation with 2000–4000 IU vitamin D3 daily might be considered after appropriate assessment.109 Nevertheless, it is important to consider the potentially harmful effects of vitamin D supplementation, namely toxicity from inappropriate practice.110
Omega-3
Omega-3 polyunsaturated fatty acids are essential in various cellular functions. Because of their potential anti-inflammatory and antioxidant activity, they raised interest within athletes looking for health and/or performance benefits.111 Foods like cold-water fish are good sources of EPA and DHA (eicosapentaenoic acid and docosahexaenoic acid, the fatty acids associated with health benefits). At the same time, flaxseeds, rapeseed oil, pumpkin seeds and walnuts provide considerable amounts of alpha-linolenic acid, that is poorly converted in EPA and DHA by the body.112 Since some of the dietary sources of these essential fatty acids might not be regularly consumed by players, supplementation can be considered to attend daily requirements by EFSA (250 mg) and raises no safety concerns.113 Positive associations between moderately increased omega-3 intakes and performance have been observed.114
Nutrition role in recovery from injury
The most common injuries in elite football players are muscle injury. The majority (56%) of these injuries led to a lay-off between 7 and 28 days, while mild injuries (up to 7 days) represent 42% of cases.115 Most injuries occur in the lower limbs, meaning a significant reduction of physical activity, with consequences for muscle mass and joint tissue.116 Inactivity might lead to atrophy and loss of function from the first days of immobilisation.
Nutrition has an important role in stimulating protein synthesis in the muscles, and strategies that can minimise the catabolic effects resulting from lack of training and/or immobilisation are warranted. Although there are several nutrients with possible benefits in injury recovery, the main goal of nutritional strategies should be to ensure no lack of energy and nutrients.117 Weight gain concerns related to inactivity can lead players to restrict their diet, not ingesting the necessary nutrients and/or calories required for the normal process of tissue healing.
Therefore, the first step is to determine the energy needs of injured players, assessing whether the rehabilitation period involves a complete stoppage of exercise or if the athlete will continue to perform some type of training. It is also necessary to consider that the process of tissue healing increases energy consumption per se, particularly in serious injuries.118 It is estimated that energy needs may increase by 15%–50% during recovery. By itself, muscle protein synthesis can represent ~500 kcal/day.119
It is also interesting to consider that individuals moving on crutches can double or triple the energy expenditure necessary to move when compared with walking.120 Thus, it is important to ensure that caloric intake is neither insufficient (compromising the process of tissue repair) nor excessive (leading to an undesirable weight gain). Therefore, players should follow a normocaloric (or slightly hypercaloric) and normoproteic or hyperproteic (2–2.5 g protein/kg/day) dietary plan during the recovery period.117 No evidence supports the benefits of increasing micronutrient intake above DRV values during this period.
Similarly, evidence supporting the use of other nutrients to accelerate rehabilitation is scarce. Creatine supplementation to minimise muscle atrophy has not produced consistent results. However, it may be useful in returning to play when the player is ready to exercise at high intensities.121 Supplementation with omega-3 fatty acids does not seem to accelerate recovery. Despite its anti-inflammatory action, the development of an inflammatory response can be part of the natural recovery process.122 Therefore, supplementation with omega-3 should not be automatically considered in case of inflammation.123 The same is true for vitamin C; despite its antioxidant properties and role in collagen formation, there is no evidence to support the intake of doses above DRA for faster or better recovery.117
Although it may be tempting to consume alcoholic beverages while not training or playing, players should be aware that alcohol can negatively interfere in the recovery process.69 124 Therefore, players should be educated to avoid, or at least limit, alcohol consumption during rehabilitation.
Specific considerations for female players
Nutritional needs for women are different from those for men. Iron and calcium, among other minerals and vitamins and water daily intake recommendations, change between genders, highlighting the need for individual assessments to develop appropriate nutritional strategies for female players. The available information on energy expenditure in female players during training sessions or matches is scarce. However, relative carbohydrate intake recommendations (in g/kg/hour) before, during and after the match for male players may apply to female players.
The authors agreed that athletes must be aware of relative energy deficiency in sport (RED-S), an energy imbalance with multisystemic involvement. Although the real prevalence in football is unknown, RED-S might be more prevalent among women.125 Ensuring the necessary dietary intake in female players might be a challenge, as they tend to eat less when training and competing, resulting in energy, carbohydrates and some nutrients deficits.126 Extra care should be taken to identify and support players with harmful eating disorders. Food education from early ages and assessment of nutritional demands are key actions in RED-S screening and prevention.127 These programmes, which might take place outside the sport context, should support players in understanding energy and nutrients requirements for training and playing and provide counselling for body composition manipulation.128
Overall, a set of considerations for nutritional strategies is summarised in table 4.
Nutritional strategies to be used between matches
Conclusion
Food and nutrition are for performance and recovery strategies in football. With this document, a consensus was sought on the nutritional strategies to be adopted before, after and between matches. The role of nutrition in rehabilitation was also addressed, and some considerations about the female player were added. Sports nutrition, particularly applied to football, is a constantly evolving science with new findings and regular updates. Exchanging knowledge and experiences among experts contributes to supporting players’ health and performance.
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study. No data are available. Not applicable.
Ethics statements
Acknowledgments
The authors would like to acknowledge the contribution of medical writer Ana Santos.
References
Footnotes
Contributors The main steering committee consisted of RA, PF and JB. RA and an external medical writer compiled all authors inputs during the experts meeting and conference. RA wrote the original draft. All authors contributed to the full manuscript, providing editing suggestions and comments. JB, PF, JPM, CS, MS, PC and VHT reviewed the manuscript. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer All mentioned affiliations refer to the date of the consensus meeting that originated this manuscript.
Competing interests RA has received consulting fees Danone Portugal, The Coca-Cola Company Iberia and Glanbia Performance Nutrition Iberia. He did not receive any form of financial support directly related to this manuscript. RA, PF, PB, JPM and JB work in the Health and Performance Unit from the Portuguese Football Federation.
Provenance and peer review Not commissioned; externally peer reviewed.