Article Text

Abstract
Background Eating disorders (ED) and disordered eating (DE) among male elite athletes share some of the characteristics seen in female elite athletes and the population, but also exhibit some key differences.
Objective Scoping review of ED and DE in male elite athletes.
Methods In May 2020, a comprehensive systematic literature search was conducted for DE and ED in male elite athletes.
Results We identified 80 studies which included 47 uncontrolled, 14 controlled studies, one interventional trial and 18 reviews.
Discussion There was a wide range of definitions of DE and a high level of heterogeneity regarding competitive level, age and sport type. In adult male elite athletes, ED prevalence rates up to 32.5% were found, higher than in the general population. Prevalence was not higher in young/adolescent male elite athletes. The most frequently associated factor was competing in weight-sensitive sports. Male elite athletes tended to exhibit less body dissatisfaction than controls and were not always associated with DE. There were no studies looking at the prognosis or reporting an evidence-based approach for the management of DE in male elite athletes.
Conclusion Existing literature indicates high prevalence of DE and ED in male elite athletes, with a wide range of aetiopathogenesis. There is a need for longitudinal studies to characterise the pathology and long-term outcomes, as well as develop standardised tools for assessment and treatments.
- Male
- Elite performance
- Athlete
- Eating disorders
- Review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Eating disorders in elite athletes: the spectrum of disordered eating
Disordered eating (DE) and eating disorders (ED) are classified in the WHO ICD-10 or in the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders1 (DSM-IV) and have high mortality rates: 4.0% for anorexia nervosa (AN), 3.9% for bulimia nervosa (BN) and 5.2% for Eating Disorders Not Otherwise Specified (EDNOS).2 In elite athletes, they are one of the most common psychiatric pathologies.3 4
According to Sundgot-Borgen et al, 5 DE should be viewed and understood as a continuum model. Starting with appropriate eating and exercise behaviours including healthy dieting and the occasional use of more extreme weight loss methods such as short-term restrictive dieting (<30 kcal/kg fat free mass (FFM)/day).6 The pathological continuum ranges from subclinical EDs such as anorexia athletica (AA) and ends with clinical EDs such as AN, BN, EDNOS along with other medical complications and impairment of performance.5 6 Since existing literature examined a variety of different manifestations along the spectrum of DE, we will specify the characteristics where appropriate.
Male elite athletes have a higher rate of DE compared with male non-athletes.5 7–11 However, male elite athletes suffering from DE have largely been ignored by research in this area focusing mainly on female elite athletes.
Rationale and objective of the present scoping review
To the best of our knowledge, there are not any reviews focusing exclusively on DE in male elite athletes. The existing literature indicates several gender-specific differences among elite athletes regarding prevalence,4 5 8 12–20 assessment,8 12 16 associated factors and aetiology12–14 16 18–23 and prevention.22 Thus, it may be a mistake to transfer findings from studies conducted in female elite athletes or non-elite athletes to male elite athletes. That may subsequently create or maintain an unrecognised knowledge gap among the subpopulation of male elite athletes.
A 2016 meta-analysis examining the DE prevalence in male athletes found higher DE rates among male athletes compared with non-athletes, but no difference among sport categories or levels of competition (elite vs non-elite).24 They did not analyse age groups separately and the results were exclusively analysed based on self-reported questionnaires and sometimes even solely on the Drive for Thinness (DFT).24 The DFT is a subscale of the Eating Disorder Inventory25 26 that measures the desire to be thinner.27 Because of that those results may not be valid or representative of the population of (adult) male elite athletes. Furthermore, they did not examine other dimensions of DE in male elite athletes such as the particular assessment, other risk factors than sports categories, comorbidities, consequences and management of DE in male elite athletes. Therefore, the objective of this scoping review was to condense the existing evidence and to identify gaps in knowledge on DE in male elite athletes.
METHODS
Our protocol was drafted using the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA), which was revised by the research team after feedback from peer experts. The final protocol was not registered beforehand but can be requested from the corresponding author. For the present scoping review, a systematic literature search was conducted in May 2020 by use of PsycINFO, PubMed, SPORTDiscus and Web of Science with the following keyword string: (‘eating disorders’ OR ‘anorexia’ OR ‘bulimia’ OR ‘disordered eating’) AND (‘elite athlete’ OR ‘high performance athlete’ OR ‘high level athlete’ OR ‘national athlete’ OR ‘international athlete’ OR ‘professional athlete’ OR ‘NCAA Division 1 athletes’) AND (‘males’ OR ‘men’ OR ‘male’ OR ‘man’ OR ‘boys’). Relevant studies in English or German without any restriction on publication date were identified. Controlled studies were defined as studies comparing male elite athletes with male non-athletes. The PRISMA statement28 29 was used to guide our systematic literature search; all mandatory items for Scoping Reviews Checklist were applicable to our review.
We included studies that examined male athletes competing at an international or national level, since this is the most common definition of an elite athlete (supplemental table S1). ‘NCAA Division 1 athletes’ compete at the highest collegiate level and are sometimes also categorised as elite athletes.30 31 We also included studies conducted in NCAA Division 1 athletes if they were declared as elite athletes. Because of the similar definitions, we used the term ‘elite athlete’ synonymous to terms like ‘high level athletes,’4 15 18 ‘high performance athletes’32 33 and ‘national athlete.’21 Adult was defined as age 18 and above. We included male elite athletes at any age.
Supplemental material
Studies exclusively conducted in female athletes or non-elite athletes (such as recreational, club, varsity, non-NCAA Division 1 collegiate or unspecified athletes) were excluded. The same goes for studies without focus on disordered eating, editorials, languages other than English or German or full text not available.
Two reviewers screened the publications and sequentially evaluated the titles, abstracts and then full text of all publications identified by our searches for potentially relevant publications. We resolved disagreements on study selection and data extraction by consensus and discussion with other reviewers if needed. Literature references from the full-text articles were used to identify additional records. The search process flowchart is presented in figure 1.

Flow diagram of search process.
A data-charting form was jointly developed by two reviewers. They independently charted the data, discussed the results and continuously updated the data-charting form in an iterative process. Any disagreements were resolved through discussion between the two reviewers or further adjudication by a third reviewer. Data from eligible studies were charted using a standardised data extraction table designed for this study. The table captured key study characteristics and detailed information on metrics used to estimate or describe DE on at least two data points per group.
We extracted data on the sample characteristics (eg, type of sports, gender, age range, weight sensitivity of sport), ED assessment (eg, type of reporting, questionnaire), ED prevalence in male athletes and additional findings (eg, important conclusions of the authors, significance of result). Reviewers did not appraise systematically the quality of evidence for methodological quality or risk of bias.
Data from studies were then summarised by risk factors for DE (general, sport type-specific risk factors, body dissatisfaction), prevalence and comorbidities, management, health consequences and performance consequences. For data from systematic reviews, the results were extracted as such. For data from narrative reviews, the underlying original literature was identified, and the data extracted from the original study and cited as original literature in the data-charting table, unless the review contributed significantly to the original study question.
RESULTS
We identified 717 records from the first search, of which 250 were duplicates. In the remaining 467 records, we removed 330 based on title and abstract screening. A further 86 from the remaining 137 full-text articles were removed for the following reasons: no gender differentiation, unspecified level of competition, no elite-level athletes, not focused on disordered eating, not English or German or results were not relevant to this review. Twenty-nine additional records were identified by manual search of text references and coauthors added to the pool of studies analysed. We identified 80 studies including controlled (n=14, 18%), uncontrolled (n=47, 59%), interventional (n=1, 1%) studies and reviews (n=18, 23%) relevant to our scoping review.
The analysed studies were summarised in data tables and grouped according to the prevalence and assessment of DE for male adult elite athletes (online supplemental table S2) and male adolescent elite athletes (online supplemental table S3). The tables show the sample characteristics, how the DE was assessed, the prevalence found and any additional findings from the paper for each literature cited. Potential risk factors of DE in male elite athletes (at any age) are summarised in table 1.
Associated factors in male elite athletes with disordered eating (DE)
Supplemental material
Supplemental material
DISCUSSION
General risk factors
In addition to general risk factors for DE,50 51 several sport-specific risk factors have been suggested,52 but no longitudinal studies analysing male elite athletes were found. In some studies, causal relationship was not established; hence, risk factors in those studies were considered as associating factors.53 In addition, most associating factors of DE in elite athletes have been examined among female elite athletes only54 and cannot automatically be applied to male elite athletes.
Thompson et al 55 suggested that personality traits required to be a good athlete are similar to those found in anorexic patients (eg, perfectionism). The existing literature showed no significant association between DE and perfectionism.7 33 34 Looking at different subtypes of perfectionism, ‘other oriented perfectionism’ was significantly positively associated,11 33 ‘positive perfectionism’ significantly negatively35 associated with DE in male elite athletes. No significant association was found for ‘negative perfectionism.’35 The sport environment itself may put athletes in a vulnerable position.48 56 A greater ratio of power/musculature to bodyweight/fat mass often enhances performance in many sports.56 Furthermore, appearance is believed to influence the ratings of the judges in aesthetic sports.12 Whereas in weight class sports, weight loss may be needed to match the qualified weight class. Although genders were not analysed separately, weight and shape concerns were attributed to improvement of performance by 81% to 94% of elite athletes.15 A causal relationship of the desire to be leaner to enhance performance was found among adolescent elite athletes competing in aesthetics sports.57 Two studies found performance enhancement to be the most frequent reason for dieting in male elite athletes.8 13 Because the loss of body fat or body weight often leads to an initial improvement of performance, it may force elite athletes to continue dieting whereby vulnerable athletes may unconsciously slip into the DE spectrum.31 58
Higher levels of competition were significantly associated with DE in male elite athletes in three studies16 32 36 and more aggressive weight loss behaviour in one study.36 Whereas five studies did not find any significant correlation between the level of competition and DE.19 33 37–39 However, we could not find any study in which a lower level of competition was associated with DE.
Studies that examined the possible association between age9 10 40 or between ineffectiveness7 15 and DE in male elite athletes showed mixed findings.
Career dissatisfaction was associated with DE in male elite athletes in two studies.41 42
A significant association between the BMI and DE in male elite athletes was shown in two studies,8 whereas other two studies19 43 found no significant association.21
In addition, underreporting of DE behaviour in questionnaires was observed in several studies among adolescent8 and adult male elite athletes.5 15 Underreporting may be explained by the reports of athletes seeing their ED as natural part of the sport12 59 or by fear of being discovered and having their athletic career jeopardised.5
Other potential general risk factors that were only examined in only one study are listed in table 1.
Sport type-specific risk factors
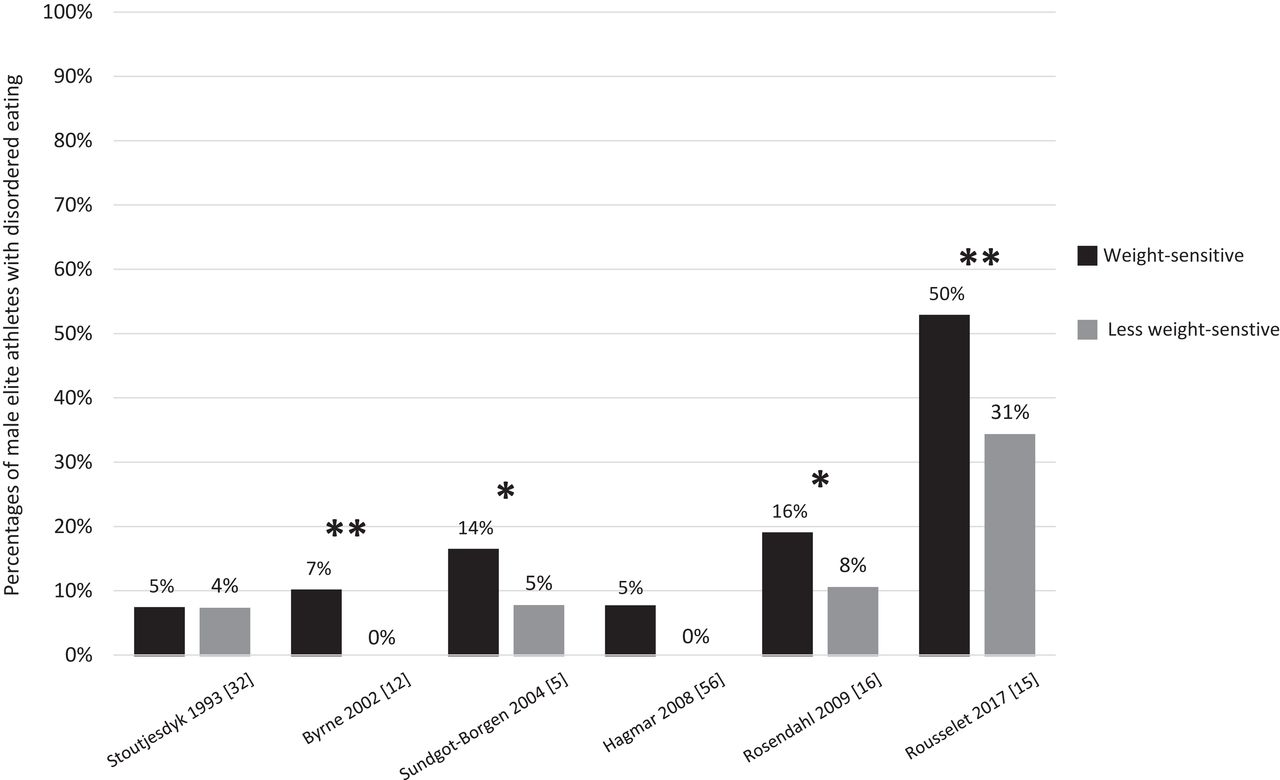
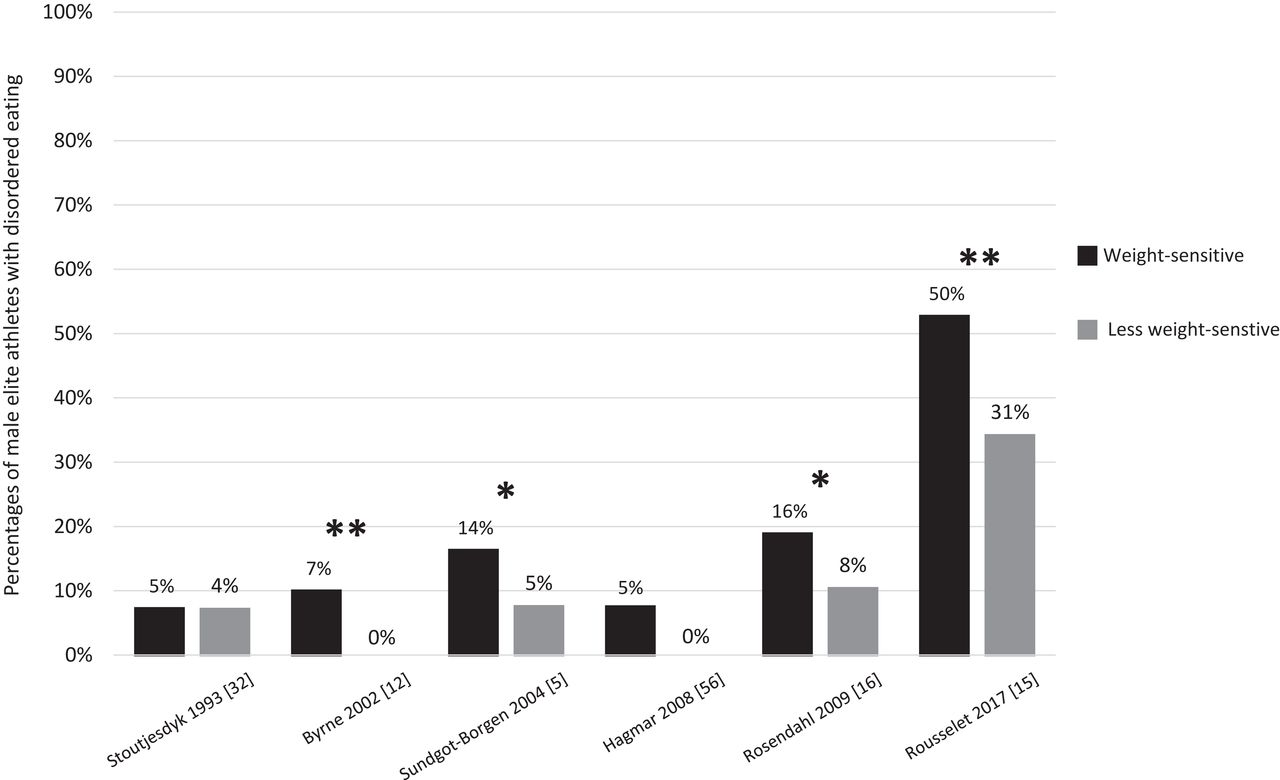
Sport types have been classified into two categories: less weight-sensitive sports and weight-sensitive sports in which leanness and weight play a major role in terms of performance.5 8 12 13 15 16 32 It was suggested that even in the absence of high-level body dissatisfaction, the demands of a weight-sensitive sport may be sufficient to initiate DE behaviour in athletes.60 Figure 2 depicts the findings of studies that compared DE prevalence between male elite athletes competing in weight-sensitive and less weight-sensitive sports.
{kind=link}
{kind=link}
Disordered eating in male elite athletes competing in different sport categories.
Significant difference (*); one study13 that did not find significantly different prevalence rates of DE between the two sport categories could not be included in this figure, because the authors did not provide any concrete numbers. *P≤0.05, **P≤0.01, according to a t-test.
Male elite athletes competing in weight-sensitive sports reported higher pressure to be lean,12 higher prevalence of DE compared with other athletes and non-athletes,5 12 14 15 44 higher drive for thinness,12 higher level of dietary constraint12 and higher engagement in bulimic behaviours.12 A higher prevalence of DE among male athletes competing in weight-sensitive sports was also found in a sample of male athletes with a mixed level of competition.16 On the contrary, three studies found no difference of DE behaviour between the two sport categories. Two of them analysed adult male athletes with mixed levels of competition,32 37 another analysed adolescent male elite athletes.13
Regarding subgroups of sport types, a significantly higher prevalence of DE behaviour was found among male elite athletes competing in weight class sports,5 12 14 61 antigravitational sports,5 combat and contact sports.4 Lastly, competing in a lightweight sport was correlated with extremely high levels of cognitive control of eating behaviour, an assumed risk factor for DE.10
Other potential sport-type specific risk factors that were only examined in only one study are listed in table 1.
Body dissatisfaction
The male western sociocultural model of aesthetic standard constitutes a lean and muscular physique, with an emphasis on the upper body (ie, a V-shape, muscular shoulder girdle), which is hard to reach without dieting and exercising.62
Besides the pressure to perform well, male elite athletes may also experience the same omnipresent sociological pressure to meet the prevailing aesthetic ideal.59 They are potentially accumulated by pressure to embody the optimal paradigm of their sport, because they do not match or feel like they do not match the ideal.59
Results obtained from a meta-analytical review including 78 studies indicated moderately lower body dissatisfaction among athletes; however, only 19.2% of the sample involved male athletes and only 7.8% involved elite athletes.63 Nevertheless, six later studies found lower body dissatisfaction among male elite athletes compared with male non-athletes.10 13 14 45 64 65 Eight studies reported no difference between male elite athletes and non-athletes regarding body dissatisfaction.7 8 12 16 21 23 34 38 We found no other studies in which male elite athletes showed more body dissatisfaction than male non-athletes.
In male elite athletes, body dissatisfaction was positively associated with DE in six studies,7 9 15 20 21 46 whereas three studies found no significant association8 12 34 and one even a negative association.45 However, another study found a five times higher DE prevalence among dissatisfied male elite athletes, but only if the male elite athletes had a thinner body ideal.16
Other body-dissatisfaction-related potential risk factors that were only examined in only one study are listed in table 1.
Assessment, prevalence and comorbidities
Assessment
Two studies suggested that existing tools to assess eating disorders in general population are not appropriate to detect DE pathologies among elite athletes.15 63 66
First, some argue that dieting behaviour and preoccupation with food in the context of high-level sports should not be seen pathological per SE Specific behaviours, generally labelled as ‘disordered’ may represent a part of the subculture within their sport and a functional strategy to enhance performance. For these reasons, they should rather be seen as a sign of commitment.5 14
Second, body dissatisfaction tended to be lower10 13 14 45 64 65 or equally pronounced7 8 12 16 21 23 34 38 among male elite athletes compared with male non-athletes and was per SE not necessarily associated with DE.8 12 34
Third, the usage of BMI values to assess AN in male elite athletes must be viewed critically, because higher muscle mass elevates the BMI regardless of body fat percentages. Moreover, the amount of food necessary to cover the energy demands of a male elite athlete may easily be misinterpreted as bingeing.5 40
Fourth, self-reports (ie, questionnaires) led to significant rates of underreporting and false classification in male elite athletes5 8 15 indicating insufficient sensitivity and specificity of the used questionnaires. Therefore, additional clinical interviews are viewed as essential to detect DE and determine prevalence rates reliably.3 5 8 15 21 53 54 56 67 68 Clinical interviews may discourage some athletes from participation.12 According to the 2014 International Olympic Committee (IOC) consensus statement,6 the Eating Disorder Examination interview (EDE-16)68 is the Gold Standard for the diagnosis of EDs. Whereas the 17th edition of the EDE (EDE-17) should be used in future to generate DSM-5 ED diagnoses. The Brief Eating Disorder in Athletes Questionnaire (BEDA-Q)69 is the only specific diagnostic tool or ED in elite athletes and has only been validated in female elite athletes.
Prevalence
Online supplemental tables S2 and S3 provide an overview over the findings from studies conducted in male elite athletes. A significantly higher prevalence of DE among male elite athletes compared with male non-athletes was found in seven controlled studies.5 7–11 45 Three studies found no significant difference16 21 37 and one study found an even lower prevalence of DE among male elite athletes.13
Except for one,37 all controlled studies which did not find a higher prevalence of DE were conducted in adolescent male elite athletes.13 16 21 Although two studies conducted in male adolescent athletes found a higher DE prevalence compared with male non-athletes,8 65 no difference of DE rates among athlete groups was found in a systematic review examining young (on average <25 (±SD) years) elite athletes.30 However, the meta-analysis from 2016 on DE in male athletes found significantly higher DE rates among male athletes compared with non-athletes, but no difference between male elite athletes and non-elite athletes.24
Uncontrolled studies4 12 14 15 18–20 22 32 35 36 40–44 46 70–73 showed prevalence rates ranging from 0% to 85.8% for DE symptoms, 1.5% to 11.0% for subclinical EDs and 1.3% to 32.5% for clinical EDs. Because no standardised definitions for DE symptoms and subclinical EDs were used, we compared the prevalence rates of clinical EDs between male elite athletes and male non-athletes. A systematic review from 2019 found a weighted mean of point ED prevalence of 2.2% (range: 0.2% to 7.3%) for men in the general population.74 Considering the evidence for increasing prevalence of clinical EDs roughly over the last 20 years,74 the prevalence of EDs seems higher among male elite athletes compared with the male general population.
Based on the observation of greater bodyweight and BMI values among female elite athletes exhibiting AN symptoms, the concept of AA was introduced.75 To date, it was only applied to male elite athletes in one study.5 However, EDNOS prevalence rates of up to 90% were found in male elite athletes.4 5 8 15 EDNOS was the most frequent ED among male elite athletes;4 5 8 15 only one study found no significant difference among the ED subtypes.12 This result may be explained by the assessment differences in male elite athletes, which may have met several AN or BN criteria but did not meet the requirements for a clinical AN or BN diagnosis.
Comorbidities
The following variables were also significantly associated with DE in elite male athletes: comorbid mental illnesses, doping behaviour, loss of self-confidence15 and excessive exercising.37 A connection between doping behaviour and preoccupation with body image was already suggested.76 No significant association between musculoskeletal injuries or concussion47 was found.
Despite the limited data available, two categories of comorbid mental illnesses were found in eating disordered male elite athletes: affective disorders and substance abuse disorders. Significantly increased rates of depression19 34 46 and anxio-depressive states14 in male athletes with DE were found in self-report studies. The only study that used a semistructured interview (Interview Grid for Multidimensional Assessment of Athletes; IGMAA) found significantly more anxio-depressive states in the ‘DE detected’ group but only in a univariate and not in a multivariate comparison.15 However, the characteristics of the relationship (eg, risk factor, comorbidity, consequence) between DE and affective disorders remains unclear.
Management
No study looked at evidence-based intervention for the prevention or treatment of DE in male elite athletes. One study described a first successful attempt to prevent DE in young female elite athletes but not among male elite athletes.22
Because there are no elite sport-specific guidelines on the management of EDs, we refer to the general region-specific guidelines. Until an elite sport-specific guideline is developed, the review and position statement under the auspices of the IOC may provide guidance on how to minimise the health risks to athletes competing in weight-sensitive sports,54 plus the IOC consensus statement regarding risk assessment, treatment and return-to-play decisions in athletes with a Relative Energy Deficiency Syndrome (RED-S) in sport.77
In summary, the existing literature suggests a combined approach consisting of:
Extensive education of athletes, families and coaches.6 54 59 76
Periodic assessment of psychological and somatic parameters for the early detection of DE and their associated consequences and comorbidities.6 54 59 78
Professional counselling of the athlete regarding nutrition and sport-specific factors by a professional who is experienced in working with athletes of the respective sport.6 54 59 76
Use of multimodal therapeutic approach consisting of psychotherapy and psychopharmacotherapy by a mental health professional specialised in DE, ideally with experience in working with athletes.6 54 59 76
Treatment of co-morbid psychiatric and somatic conditions by the particular specialised professional such as psychiatrists, endocrinologists and others.6 54 76
Development of regulations by the federations such as adjustments of weight classes and rules in weight-class sports, adjustments of judging criteria in aesthetic sports and strict compliance with the official IOC return-to-play guidelines and others.6 54 59 79
Health and performance consequences
Health and performance consequences in elite athletes with DE are believed to be dependent on the duration and form of DE behaviour and the physical demands of their sport.5 No evidence in male elite athletes could be found to support this assumption.
DE can result in a RED-S and vice versa.6 The concept of RED-S plays therefore an important role in the explanation of the consequences of DE. RED-S refers to a variety of physiological function impairments caused by relative energy deficiency including inter alia metabolic rate, endocrine/menstrual function, bone health, immunity, protein synthesis, cardiovascular health.6 The aetiological factor of RED-S is low energy availability (EA), relative energy deficiency between dietary energy intake and energy expenditure in exercise to support homoeostasis, health and growth.6 As the formerly used term of ‘female athlete triad’ indicates, literature on low EA has mainly focused on female athletes. Yet, low EA and RED-S do also occur among male athletes.6 77 Because male athletes show no diagnostic hallmarks such as amenorrhoea, the exhibition of DE signs should receive special attention.59 Significantly reduced bone mineral mass and endocrine alterations have been found among male professional jockeys, likely caused in response to chronic weight cycling habitually experienced by this group.80
Additionally, the practice of extreme weight control methods such as fasting, vomiting, abuse of diuretics and laxatives may lead to serious performance and health consequences.6
Besides somatic consequences, the stress of constantly denying hunger, agonising over body weight and fearing weight gain is mentally exhausting.59 Furthermore, low EA and DE and psychological stress and depression affect each other reciprocally.50 It should be taken into account that athletes in an energy deficit may exhibit DE behaviour despite lacking a psychological component. Among those athletes just achieving a neutral or positive energy balance may resolve DE behaviour without further intervention.5
Limitations
This review has some limitations: the heterogenous definition of an elite athlete makes it difficult to draw final conclusions and may be responsible for some of the mixed results. We suggest to exclusively use the term ‘elite athlete’ to describe athletes who compete at an international or national level since this term and criteria were used the most (supplemental table S1). The classification of NCAA Division 1 athletes as elite should be addressed by future research. Additionally, the quality of evidence for methodological quality or risk of bias was not appraised systematically. Results were however weighted according to the expertise of the authors for the discussion. Furthermore, existing assessment tools seem to exhibit insufficient sensitivity and specificity. No evidence-based approach for the management of DE in male elite athletes currently exists. Data on the prognosis are missing.
Implication for future research
The present scoping review revealed a knowledge gap on the evidence-based management of DE in male elite athlete, since only one interventional study was found, which has failed to prevent DE among male elite athletes.22 Health consequences such as the RED-S are not well researched in male athletes.77 The lack of prognosis of DE in male elite athletes represents another knowledge gap, since only two conflicting studies on the prognosis of weight cycling among male athletes competing in weight-class sports were found.81 82 Moreover, the only study on DE in male elite para athletes found similar rates of DE among male elite non-para athletes,72 although they may be at greater risk of DE consequences.77
In this scoping review, we identified 80 studies addressing ED and DE in male elite athletes across a variety of sports. Current literature indicates that male elite athletes are equally or more satisfied with their bodies, even when gender neutral or male-specific questionnaires were used.13 14 16 21 45 Taking part in sports may result in a physique embodying a western sociocultural ideal for males as a result of the intensive training and dieting, which may drive higher rates of sport participation and higher level of competition. It remains unclear if BD is associated with DE in male elite athletes, since mixed results were found (table 1). Future research should not only address factors that are possibly associated with DE in male elite athletes, but also the characteristics of the relationship (eg, risk factor, comorbidity, consequence).
Study questionnaires seem to assess DE inappropriately in male elite athletes due to specific characteristics: (1) preoccupation with nutrition may reflect functional behaviour,5 45 (2) BMI as a criterion for AN may be greater due to increased lean body mass, (3) high food intake necessary to maintain energy balance may be misinterpreted as bingeing,5 40 (4) under-reporting in questionnaires,5 8 15 possibly due to the stigmatisation and fear of jeopardising their career, (5) male elite athletes seem more satisfied with their bodies than male non-athletes10 13 14 45 64 65 and (6) lacking BD does not rule out DE in male elite athletes.8 12 34 45 Consequently, future research should focus on the development of a questionnaire with sufficient sensitivity and specificity for male elite athletes. This future questionnaire should not include the SCOFF questionnaire (SCOFF83), contain modified BMI cut-off values or use the DSM-5 criteria14 and define bingeing as loss of control. Until the role of BD in male elite athletes with DE is better understood, DE criteria including body dissatisfaction should be modified to prevent underestimation or false-negative results. Furthermore, questionnaires should always be combined with clinical interviews.3 5 8 15 21 53 54 56 67 68 Discouragement of study participation may be counteracted by offering strict anonymity and specific professional help.
Existing literature indicates a higher prevalence of DE among male elite compared with male non-athletes.5 7–11 45 This does not apply to young/adolescent male elite athletes.13 16 21 30 They may have not been exposed to the pressure of the sports environment and weight-sensitive sports long enough, which may also explain the lacking association of weight-sensitive sports or sport types with DE among young/adolescent male elite athletes. However, this hypothesis can only be confirmed by longitudinal studies. Because several findings varied among age groups, adolescent elite athletes should always be analysed separately. In addition, existing literature indicates that health professionals, athletes and coaches should be warned of the prejudice of DE and false assumption of DE only concerning female athletes.15 31 49 Future research should address different potential comorbidities of DE in male elite athletes such as exercise dependence,84 overtraining syndrome85 and muscle dysmorphia and its role as potentially relevant differential diagnosis.86
CONCLUSION
Existing literature indicates a higher prevalence of DE among male elite compared with male non-athletes.5 7–11 45 This does not apply to young/adolescent male elite athletes. Sports federations should introduce periodic DE screening in elite athletes,78 particularly in weight-sensitive sports. They should also comply with the recommendations of the IOC77 and their associates54 to assess the efficacy and efficiency of those recommendations59 on the management of DE in male elite athletes. The link between body composition and performance seems to play a key role in the development of DE in elite athletes.57 The literature indicates an association of DE and the participation in weight-sensitive sports5 12 15 44 among other factors (table 1) in male elite athletes. Study questionnaires seem to assess DE inappropriately in male elite athletes due to specific characteristics. Questionnaires should always be combined with clinical interviews. The present scoping review demonstrates an urgent need for longitudinal studies which are indispensable to examine the prognosis, to identify risk factors, comorbidities and consequences of DE in male elite athletes, which are needed to develop and assess efficient interventions.
Summary box
What is already known?
Eating disorders and disordered eating are one of the most common mental illnesses in elite athletes.
In addition to self-reported questionnaires, clinical interviews are needed to assess disordered eating and eating disorders in elite athletes.
Disordered eating can result in a Relative Energy Deficiency Syndrome (RED-S) and vice versa.
What are the new findings?
The most frequently associated factor for disordered eating in male elite athletes is participation in weight-sensitive sports.
Male elite athletes tend to be more satisfied with their bodies compared with non-athletes.
Body dissatisfaction is not necessarily associated with disordered eating in male elite athletes.
Acknowledgments
Assistance and advice during the revision of this scoping review provided by Simon Manuel Ewers was greatly appreciated.
REFERENCES
Footnotes
YK and RH are joint first authors.
Contributors MCC proposed the idea of the paper in discussion with YK, RH, MJ. MJ and MCC were responsible for the conceptualisation and methodology of the paper with inputs on the conceptualisation and methodology by YK, RH and methodological inputs by SM. YK and RH conducted the systematic literature search. YK, RH and MCC manually searched full-text references for additional relevant papers. YK wrote the original draft, that was reviewed by RH, SM, ES, MJ, MCC and edited by RH and YK. YK, RH and SM were responsible for the visualisation. YK and SI carried out the full revision of the paper after initial review and were supported during the second revision by SME. MCC and ES were responsible for the research planning and execution. MCC supervised the whole project and is guarantor. YK, RH, SM, SI, ES, MJ, MCC, SME approved the version of the manuscript to be published.
YK, RH, SM, SI, ES, MJ, MCC, SME agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. YK: Yannis Karrer. RH: Robin Halioua. SM: Dr Sonja Mötteli. SI: Dr Samuel Iff. ES: Prof. Dr Erich Seifritz. MJ: PD Dr Matthias Jäger. MCC: Dr Malte Christian Claussen. SME: Simon Manuel Ewers.
Funding The authors received no specific funding for this work.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the authors. It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the authors and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.