Article Text

Abstract
Objectives In the literature on proximal hamstring avulsions, only two studies report the outcomes of non-surgically treated patients. Our objective was to compare subjective recovery after surgical and non-surgical treatment of proximal hamstring avulsions in a middle-aged cohort.
Methods We included 47 patients (33 surgically and 14 non-surgically treated) with a mean (SD) age of 51 (±9) years in a retrospective cohort study. Follow-up time mean (SD) of 3.9 (±1.4) years. The outcome variables were the Lower Extremity Functional Scale (LEFS) and questions from the Proximal Hamstring Injury Questionnaire. Outcome variables were adjusted in regression models for gender, age, American Society of Anestesiologits (ASA) classification and MRI findings at diagnosis.
Results The baseline characteristics showed no differences except for the MRI result, in which the surgically treated group had a larger proportion of tendons retracted ≥ 2 cm. The mean LEFS score was 74 (SD±12) in the surgically treated cohort and 72 (SD±16) in the non-surgically treated cohort. This was also true after adjusting for confounders. The only difference in outcome at follow-up was the total hours performing physical activity per week, p=0.02; surgically treated patients reported 2.5 hours or more (5.2 vs 2.7).
Conclusion This study on middle-aged patients with proximal hamstring avulsions was unable to identify any difference in patient-reported outcome measures between surgically and non-surgically treated patients. The vast majority of patients treated surgically had complete proximal hamstring avulsions with ≥ 2 cm of retraction. We conclude that to obtain an evidence-based treatment algorithm for proximal hamstring avulsions studies of higher scientific level are needed.
- non-surgical repair
- surgical repair
- outcome
- proximal hamstring avulsion
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What are the new findings?
This is, to our knowledge, the largest cohort of non-surgically treated patients thus far reported in the literature. It increases the number of non-surgically treated patients reported in the literature by a third (n=14).
How might it impact on clinical practice in the near future?
In this study, we were unable to find any difference in the primary outcome, Lower Extremity Functional Scale (LEFS), at a mean follow-up time of 4 years after injury.
Considering surgical complications, for example, Venous Thromboembolism (VTE), and the non-significant PROM difference in this middle-aged cohort, surgery should be carefully chosen to healthy patients with large tendon retraction and clinical signs of avulsion.
Introduction
In the published literature on proximal hamstring avulsions, only two studies (with a total 28 subjects) report the outcomes of non-surgically treated patients.1 2 This is in contrast to the 767 surgically treated subjects included in the meta-analysis done by Bodendorfer et al.3 As there are few studies with non-surgically treated patients with proximal hamstring avulsions, the evidence for the best method for treatment of this injury is not yet scientifically clear.
The objective of our study was to compare the subjective recovery after surgical and non-surgical treatment in patients with proximal hamstring avulsions. We hypothesised that, in a middle-aged population, small functional differences exist between surgically and non-surgically treated patients more than 2 years after injury.
Methods
Study design and setting
A single-centre retrospective cohort study on patients treated from 2007 to 2013 at an academic university tertriary care centre. It is one of the five major emergency hospitals in the Stockholm area, with a catchment area of approximately 500 000 inhabitants. The guidelines of the STRrengthening the Reporting of OBservational studies in Epidemiology statement were followed.
Participants
We included patients with a proximal avulsion injury during the study period and identified them from the following: (A) all MRI exams at our department where the radiologist described a proximal hamstring injury and (B) from the digital surgical administrative system, in which surgical codes indicated surgery for proximal hamstring injury. We excluded patients with Wood type 1 and 24 (no avulsed tendons or bony avulsion on MRI), those with inconclusive MRIs and those with a previous hamstring injury or previous surgery of the thigh or knee in the affected leg (table 1). All participants gave their informed consent. A flow chart of patient enrolment is demonstrated in figure 1.
Eligibility criteria
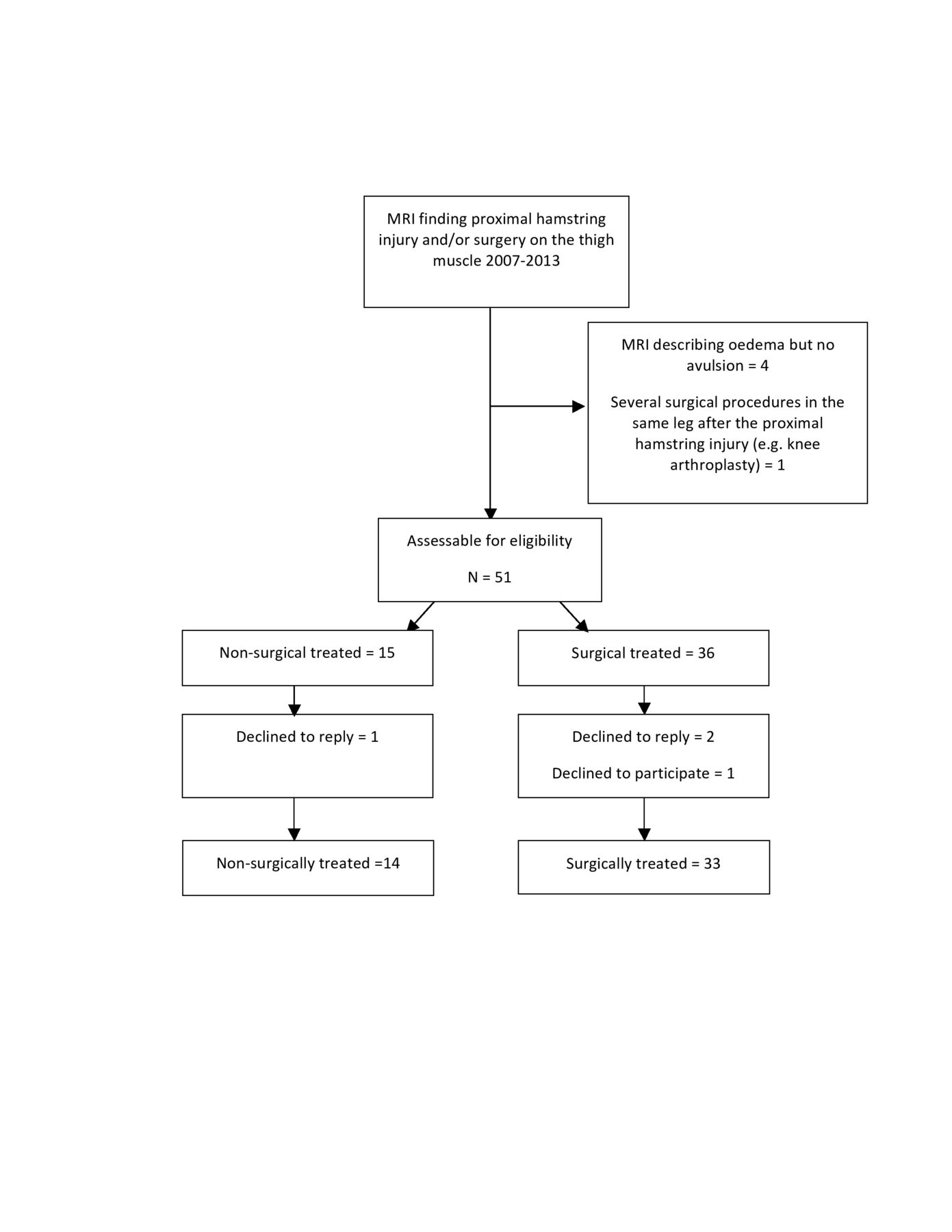
Flow of patients in the study.
MRI examinations
MRI was performed with a 1.5 T system (Signal HDxt; General Electric) using a 16-channel abdominal coil. The examination consisted of coronal and axial T1 and fat-saturated proton density-weighted and sagittal T2-weighted sequences. A consultant in radiology evaluated all images, and the consultant described the radiology report. We defined proximal hamstring avulsion to be present when at least one of three tendons were avulsed from their origin on the ischial tuberosity and a described space between the ischial tuberosity and the tendons (Wood type 3, 4 and 5)4 in the radiology report.
Variables
Exposure
The choice of treatment was decided at the outpatient clinic after the MRI diagnosis. Our treatment algorithm is a combined assessment of age (with younger patients more likely to receive surgical treatment), where ASA 3 or 4 indicates high comorbidity and is more likely to receive non-surgical treatment, the patient’s subjective activity level (high performance amateur athletes were more likely to receive surgical treatment), MRI findings (patients with Wood type 5 with more than 2 cm retraction were offered surgical treatment) and clinical findings. Lastly, the most commonly used clinical test in our department is the hip extension test, in which the patient is asked to extend the hip in prone position. Surgery is favoured when the patient is unable to extend the hip (figure 2).

{kind=link}
{kind=link}
Hip extension test. When patient can lift the affected leg from prone position as shown in the picture, non-surgical treatment is the favoured option. Photo by: S Jonhagen
Outcomes
Our primary outcome was the validated patient-reported outcome measure Lower Extremity Functional Scale (LEFS).5 It contains 20 questions about a person’s ability to perform everyday tasks and heavier physical activities (online supplementary file 1). The lower the score, the greater the disability; the maximum score is 80. The minimal detectable clinical change is nine scale points.5 6 We used the patient-reported outcome measure LEFS because it is widely used, validated for lower extremity dysfunction and good correlation has been shown between LEFS and the objective function after proximal hamstring avulsion.5 7
Supplemental material
Our secondary outcome was the Proximal Hamstring Injury Questionnaire (PHIQ; online supplementary file 28). The PHIQ is a questionnaire containing questions about function in daily activities, physical activity and self-estimated function and satisfaction. This questionnaire has questions about numbness, self-reported strength and recovery that are not included in the LEFS. The questions regarding pain, numbness and recovery in the PHIQ were analysed as dichotomous variables with answers of no pain, no numbness and 100% recovery analysed as 1 and the other subgroups for each question as 0.
Supplemental material
The original questionnaires were individually translated to Swedish by four of the authors (E Pihl, CJ Hedbeck, P-K Pettersson and H Nasell) according to online supplementary file 3.
Supplemental material
Confounders
We identified ASA classification, age, MRI and gender as potential confounders.
Interventions
Surgical treatment
Surgery was performed under general or spinal anaesthesia. The patient was placed in the prone position, and the subcutaneous tissue was infiltrated with 20 cc of local anaesthetic including epinephrine. A transverse incision in the gluteal crease, carefully avoiding the posterior femoral cutaneous nerve, a transverse incision in the crural fasciae and a longitudinal incision of the muscle fasciae were performed. The anatomical footprint at the tuber ischii was identified and suture anchors were introduced. Neurolysis of the sciatic nerve was performed in one older injury. The common proximal hamstring tendon was then reinserted into the footprint. After coagulation of eventual bleeding, the fascia and cutis were closed in layers.
Postoperatively, there was a structured rehabilitation programme.9 During the first 2 weeks (to protect the hamstring), the patient mobilised with two crutches, taking small steps with no stride out to protect the hamstring. Thereafter, the patient focused on the range of motion increase at weeks 2–4. Weeks 5–6 consisted of strength training, and weeks 7–8 consisted of progress with complex neuromuscular strength training exercises.
Non-surgical treatment
The patients who were non-surgically treated had no planned for any follow-up at the clinic. Most were referred to a physiotherapist using the same rehabilitation protocol as the surgically treated patients, which is well known in the Stockholm area.
Data collection and follow-up
The baseline data and demographics (age, sex, ASA classification, type of activity at injury, registered clinical findings and MRI findings) were collected from the hospital administrative data collection systems for surgery and radiology collected in the same manner for both groups. We also registered the time from injury to the start of treatment, surgeon, surgical incision and registered complications.
At follow-up, all included participants were sent two patient-reported outcome measurement questionnaires: the LEFS and PHIQ. The questionnaires were resent twice to those who did not respond. Those who declined to reply per post were phoned by the first author (E Pihl).
Statistical methods
Descriptive statistics (means and SD) were used to describe the patient characteristics and outcome variables. Fischer’s exact test was used for categorical variables and Student’s t-test for continuous variables. A linear regression analysis was performed to adjust for confounders that could affect the primary outcome. The statistical model included the exposure variable and confounders (ie, surgery/non-surgery group, age, sex, ASA classification and tendon retraction ≥2 cm). All analyses were considered statistically significant at a p value of ≤0.05. The statistical analyses were performed using SPSS V.23 for Mac. A power analysis was not preformed prior to the study.
Results
Participants and descriptive data
We enrolled 47 patients (29 males, mean (SD) age 51 (9) years, all except one within the age range of 34–68 years), 33 in the surgery group and 14 in the non-surgery group completed the follow-up at a mean (SD) of 3.9 (1.4) years (range: 2.0–7.3 years) (figure 2). The only outlier was 23 years and was surgically treated. The baseline characteristics of the two groups were similar except for the MRI, in which the surgical treated group had a larger proportion of tendons with a retraction ≥2 cm (p=0.025) (table 2). Four orthopaedic consultants performed the surgeries. In the surgically treated group, one patient suffered a postoperative pulmonary thrombosis, one patient suffered a wound infection and one patient suffered from severe persistent pain postoperatively. There were no adverse events in the non-surgically treated group. In one patient, nerolysis of the sciatic nerve was preformed.
Baseline demographics
Main results
We found no association between the treatment arm and our primary outcomes. The LEFS score was 72 (SD ±16) in the non-surgically treated group and 74 (SD ±12) in the surgically treated group (p=0.80) (table 3). When adjusting for confounders in the linear regression model, only increasing age was associated with a lower LEFS score (B −0.5 (95% CI −0.9 to −0.0), p=0.037). Most patients in both groups received their treatment in the acute phase within 4 weeks after the injury.
Main outcome
In addition, we found no significant difference between the groups regarding pain or stiffness and numbness in the injured leg. The proportion of patients who regularly used analgetics for their proximal hamstring injury at the time of follow-up was similar in both groups, 21% in the non-surgically treated group and 18% in the surgically treated group. Twenty-one per cent of non-surgically treated and 31% of surgically treated patients who experienced numbness in the injured leg (table 3). Eighty-nine per cent of the patients regarded themselves as high-performance amateur athletes at the time of follow-up, and although this proportion was slightly higher in the surgically treated group (94% vs 79%), this did not reach statistical significance. The only statistically significant difference in our outcome variables was the total hours per week the patients were performing physical activity at the time of follow-up, p=0.02 (table 3).
Discussion
In this retrospective study of middle-aged patients with proximal hamstring avulsions, we found no clinically relevant differences in the outcomes between surgically and non-surgically treated patients 4 years after injury. Our study will increase the number of non-surgically treated patients reported in the literature by a third (n=14). In the latest review of 24 studies and 795 proximal hamstring avulsions, the non-surgical group consisted of only 28 individuals.3
Together with Shambaugh,2 this is the first study comparing patient-reported outcomes after surgical and non-surgical treatment of total proximal hamstring avulsions. There are to date no level 1 or 2 evidence studies presented on method of treatment for this injury, nor are there any large studies comparing the treatment allocations.
Strengths
The two key strengths of this study are that the follow-up is performed using a validated questionnaire, the LEFS, and only 5 of 52 subjects who were assessed as eligible were lost to follow-up. Previous publications found a significant correlation between return to activity, hamstring muscle strength and the single-leg hop test.7 This indicates that LEFS is a validated patient-reported outcome measure and an indicator of the objective function for patients treated for proximal hamstring avulsions. It is notable that the LEFS scores in our study match the LEFS scores in previous studies both for surgically7 10 11 and non-surgically1 2 treated cohorts. In addition to this, we also assessed treatment outcomes quantitatively with patient-reported length of physical activity at follow-up.
Limitations
The most obvious limitation of this retrospective study is that there is bias by indication; the surgeon allocated the patient to the treatment arm at baseline before the study was initiated. This is highlighted by the significant difference between the cohorts with 85% in the surgical treated group having complete proximal hamstring avulsion with at least 2 cm retraction compared with 50% in the non surgical treated group. Since there is no published evidence-based treatment algorithm in the literature indicating on how to treat patients with proximal hamstring avulsion, the treatment decision was based on the orthopaedic surgeon’s experience and local guidelines. The strongest indicators for surgery were MRI finding (Wood type 5 with the tendons avulsed more than 2 cm from the ischial tuberosity), clinical findings and a healthy and active patient. We found a difference at baseline in MRI findings, as there were more patients in the surgically treated group with an MRI result with the tendons avulsed ≥2 cm from the ischial tuberosity than in the non-surgically treated group. This indicates a bias by indication in terms of severity of injury. Thus, cases with a more significant injury and higher activity level were more likely to receive surgical treatment. However, previous published studies also have this problem and are generally case series of surgical treatment.
In addition, there were more females in the non-surgical group and more males allocated to surgical treatment.
LEFS can be a non-specific instrument in patients suffering from a proximal hamstring avulsion. There are studies indicating a risk of the ceiling effect in LEFS.5 12 However, studies have also shown the opposite, recently a systematic review concluded the good reliability, validity and responsiveness of LEFS scores for assessing functional outcomes in patients with various lower musculoskeletal disorders.2 6
The possibility of the ceiling effect was one reason we chose to add several questions from the PHIQ. We found that both groups complain of numbness in their injured leg and that patients in both groups continued to take painkillers for their injured leg.
In the surgical-treated group, patients were training twice as much as in the non-surgical-treated group at our follow-up. As we do not know the physical activity level prior to the injury, it cannot be concluded that there is no difference in physical activity level between the surgically and non-surgically groups.
Interpretation
Considering that this study was performed in a public hospital setting and most of the patients are active middle-aged non-elite athletes, our primary hypothesis was that there would be no differences in LEFS between the two groups at follow-up. The surgical cohort demonstrated a higher severity of injury, with the vast majority of them having complete avulsions with greater than 2 cm of retraction. At t follow-up the surgical cohort were doing physical activity 2.5 hours more than the non-surgical treated cohort. We are aware that this might be a bias by indication. However, we did not find any difference in our primary outcome, LEFS, for surgically treated and non-surgically treated patients. Because the patients in the non-surgical treatment group did not follow any specific physiotherapy protocol, although many physiotherapists in the Stockholm area use the Askling protocol for this injury, we do not know the extent of physiotherapy in this treatment arm. We also do not know if these patients were followed up or if they were left to train by themselves. The non-surgically treated group may thus have scored a higher LEFS result if a comprehensive physiotherapy protocol had been used. Many previous studies describe good results after surgical treatment of proximal hamstring avulsion,13–15 but the problem with many of these studies is that heir instruments are not validated and standardised and that they all lack a control group.
Comparing the results of the validated LEFS in the non-surgically treated cohort of Hofmann et al1 and a surgically treated cohort,7 the scores are similar in both cohorts. The non-surgically treated cohort had 70.2 out of a maximum of 80, and the surgically treated cohort was slightly higher with a mean of 71 out of 80, results that are remarkably consistent with our study. Shambaugh et al2 included 25 patients, with 11 patients in the non-surgical group with a LEFS score of 68.5 (±7.9) and 14 patients in the surgical group with a mean score of 74.7 (±5.4). Notably, the surgically treated patients were, on average, almost 9 years younger (47 vs 55.7 years) in this study.1 2 The LEFS score is also similar to other studies using this validated score with Chahal et al11 reporting LEFS of 75 (±7.8) and Cohen et al10 and Skaara et al7 reporting 75 and 71, respectively, for their patients who underwent surgical treatment. However, all studies have the same problem of bias by indication as with our study.
In the systemic review by van der Made et al,12 the rate of satisfaction with surgery was 88%–100%. Strength ranged in nine studies from 78% to 101% of the uninjured side. From this, most people would be convinced of the benefits of surgery. Interestingly, pain was not uncommon and was reported by 8%–61% of the patients.12 Bodendorfer et al3 summarised the complication rate for the surgically treated patients as high as a 23.7%. The complications described were 2%–3% rerupture, reoperation and infections, 5%–8% incisional numbness and neurological symptoms and 0.68% Venous Tromboembolism (VTE)/Pulmonary Embolism (PE). This indicates surgery is reasonable option for the properly indicated patient, but it is not without risk.
Generalisability
We believe that our results apply to the middle-aged population that we retrospectively reviewed. Retrospective studies are weakened by bias, which likely occurred in this study given the disparity in injury characteristics of the surgical-treated and non-surgical-treated cohorts.
Conclusion
In this retrospective study on middle-aged patients with proximal hamstring avulsions, we were unable to identify a difference in LEFS between surgically and non-surgically treated patients. However, surgically treated patients did report 2.5 hours of additional physical activity per week. It should be noted that surgical bias was likely in the surgical cohort, given the vast majority of patients treated surgically had complete proximal hamstring avulsions with at least 2 cm of retraction. We believe that healthy active patients with significant tendon retraction can benefit from surgery in order to improve muscle strength, function and patient satisfaction. We conclude that to obtain an evidence-based treatment algorithm for proximal hamstring avulsions, future studies of a prospective and randomised nature may assist orthopaedic surgeons in determining the ideal treatment for specific patients.
Acknowledgments
We would like to acknowledge the patients who took part in this study. Furthermore, we would like to acknowledge consultant in radiology Anders von Hejne, who have described the MRI protocol.
References
Footnotes
Contributors All authors that have contributed to this manuscript have agreed on the final revised version of the manuscript. If necessary do not hesitate to contact us for further specifications.
Competing interests None declared.
Patient and public involvement statement Patients who took part in this study will receive a short summary of the results.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted by the Regional Ethical Review Board DNR 2015/622-31.
Provenance and peer review Not commissioned; internally peer reviewed.