Article Text

Abstract
Background Strategies to prevent or attenuate the age-related decline in physical and physiological function and reduce chronic disease risk factors are of clinical importance.
Objective To examine the health benefits of recreational soccer in middle-aged and older adults.
Design Systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources All available records up until 9 June 2017 in PubMed, Web of Science, SPORTDiscus, MEDLINE, Embase, CINAHL Plus, PsycINFO and Cochrane Library databases.
Eligibility criteria for selecting studies All randomised trials with or without a control group (randomised controlled trials or randomised uncontrolled trials) and non-randomised controlled trials that used recreational soccer, which includes small-sided soccer games, as the sole or principal intervention, and reported relevant effects in untrained/sedentary, healthy or unhealthy adults aged 40 years and above were included.
Results Five trials described in 13 articles were included, which scored 6–9 out of 12 points on the modified Delphi quality rating scale. The duration was from 12 to 52 weeks, with various frequencies, volumes and game formats performed both outdoors and indoors with men and women. The trials indicate that recreational soccer may result in improvement in cardiovascular function, body composition and functional ability, although no significant changes were observed in postural balance.
Conclusion Recreational soccer should be considered an alternative exercise modality for untrained, healthy or unhealthy middle-aged and older adults of both sexes to maintain an active lifestyle and mitigate a wide array of physical and physiological age-related changes.
- recreational soccer
- healthy
- diseases
- middle-aged adults
- older adults
- systematic review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Recreational soccer is a health promotion activity for a wide range of populations.
Considerable health-related benefits are derived in both healthy and clinical populations.
Participation in recreational soccer appears to be safe for older adults.
What are the new findings?
Recreational soccer played with 3–7 people each side on an outdoor field or indoor court for 12–52 weeks results in significant positive adaptations in cardiorespiratory capacity, body composition, lower limb muscle function and strength in untrained, healthy and unhealthy middle-aged and older adults.
Postural balance appears to be less responsive to change following recreational soccer training in this age group.
Introduction
Human ageing is characterised by a progressive decline in physical and physiological function,1 and is a major risk factor for most non-communicable diseases.2 The occurrence of multiple clinical conditions is higher from mid-life to old age, including cancer,3 hypertension,4 5 sarcopaenia,6 osteoporosis7 8 and diabetes.9 Thus, preventive strategies that can defer and/or prevent age-related declines in physical and physiological function and reduce chronic disease risk factors are of clinical importance.
It is well established that physical activity is an effective and low-cost approach to counter most age-related conditions with minimal side effects or risks10; however, inactivity generally increases with advancing age.11 Sport is recognised as a mechanism to promote an active lifestyle among the general public, and as suggested by Khan and colleagues12 sport participation can contribute to a healthier nation by increasing the physical activity level of the population. However, the efficacy of a given sport to improve public health will be dependent not only on the prevalence of and participation in the sport, but also on physical demands of the activity and the resulting health-derived benefits.13
Soccer has long been considered the world’s number one sport.14 Over the last decade, recreational soccer (RS), characterised by fewer players per side and played on a smaller field than a standard competitive soccer game, and includes small-sided games, has emerged as a health promotion activity for various populations. Work to date indicates that RS positively motivates individuals and facilitates social interaction, which may enhance compliance and adherence to the activity and contribute to a physically active lifestyle,15 and has considerable health benefits in both healthy and clinical populations.16 In addition, RS has been shown to be superior to traditional exercise regimens (such as running) in enhancing postural balance,17 lower limb bone health,18 body composition19 and maximum oxygen uptake (VO2max)20 in inactive, healthy and unhealthy adults. Moreover, RS has proven to be safer than competitive soccer games with a comparable injury risk (<5%) to the low-impact activity (eg, endurance running),21 and the incidence of injury tends to be lower with older participants due to the reduction in movement speed as well as less impact and contact of players.22
Although a small but increasing number of papers regarding the training effects of RS in middle-aged and old-aged adults have been published in recent years, to the best of the authors’ knowledge no systematic review is available focusing exclusively on the health-related effects of RS in untrained middle-aged and older adults. This is important as strategies to prevent the development of chronic disease in middle-aged and older adults, as well as improve health outcomes in those with chronic disease, are an important public health outcome and sport medicine may have a substantial role to play. Therefore, the purpose of the present systematic review was to examine the effects of RS training on health-related outcomes in middle-aged and older persons.
Methods
This systematic review was conducted and reported in accordance with the recommendations in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses23 (see online supplementary file 1).
Supplemental material
Search strategy
Electronic searching of all available records up until 9 June 2017 was undertaken in SPORTDiscus, MEDLINE, CINAHL Plus, PsycINFO, PubMed, Embase, Cochrane Library and Web of Science databases. Thesaurus terms and free-text terms were used either singly or in every possible combination. Thesaurus terms used were ‘football’ OR ‘soccer’. Free-text terms used in combination with thesaurus terms were keywords for intervention (‘recreational soccer’ OR ‘small-sided soccer’ OR ‘street soccer’ OR ‘walking soccer’ OR ‘small-volume soccer’ OR ‘indoor soccer’ and the related terms) AND keywords for population (‘untrained’ OR ‘patient*’ OR ‘premenopausal’ OR ‘postmenopausal’ OR ‘middle*aged’ OR ‘old*aged’ and their synonyms) (see online supplementary file 2). No limitations were defined for the results during the search. In addition, author searches were performed for the influential authors Peter Krustrup, Jens Bangso and Morten Bredsgaard Randers, who were the authors most published in the area of recreational football/soccer (ranked by Web of Science). The reference lists of relevant primary and secondary studies (review articles, executive summary and editorials) were checked to ensure further identification of eligible studies.
Supplemental material
Selection criteria
To identify eligible articles, the titles and abstracts of identified records were first reviewed by HL to exclude irrelevant articles. Only peer-reviewed journal articles with full text and published in English were eligible for further review. Two review authors (HL and DRT) checked the eligibility of full-text articles independently based on the following inclusion criteria: (1) intervention—RS played for health and fun on an indoor or outdoor field was included (no limitations were imposed on such factors as duration, frequency, intensity or volume of the intervention programme); (2) population—untrained, healthy or unhealthy adults aged 40+ years, both men and women, were included (older adults were classed as those aged 65 years and above, and there was no upper age limit for inclusion in the review); and (3) study design—randomised controlled trials (RCTs), randomised uncontrolled trials (RUTs) and non-randomised controlled trials (NRCTs) with RS as the sole or major intervention were included (interventions with more than one comparison group including control group were also accepted).
When differences occurred, a third review author (RUN) evaluated the article, and consensus among the three reviewers was achieved. Eligible articles were further examined to differentiate articles based on the same trials and subjects.
Data extraction
The characteristics of all included trials with regard to populations, intervention programme and outcomes were collected by using a pre-established data extraction form, which was pilot-tested by HL. Data extraction was performed independently by HL and DRT. Due to the numerous inconsistencies and ambiguities existing among included papers from the same trial regarding the characteristics of the participants, intervention programme and outcomes, a consensus agreement was sought and achieved among all review authors in cases of discrepancy on data extraction.
Risk of bias assessment
The risk of bias assessment of all included trials was performed by DRT and HL independently in accordance with a modified Delphi list.24 When consensus was not achieved for a trial, one of two review authors (FM or RUN) was employed for adjudication.
The Delphi list is a commonly used rating tool for methodological quality of RCTs for systematic review, which consists of nine rating items.24 Given the characteristics of the exercise intervention, two of the nine original items were removed, that is, blinded care provider and blinded patient, while another five items were added, that is, power calculation, between-group statistical comparison, exercise adherence, reporting dropouts and provision of supervised training25 (see online supplementary file 3).
Supplemental material
Items were equally rated by ‘yes’, ‘no’ or ‘not reported’, in which ‘yes’ was counted for 1 point, while ‘no’ and ‘not reported’ equalled 0 point. Consequently, 0–12 points could be attained for any included articles, with a higher score indicating higher methodological trial quality.26
Results
Study selection
The electronic search yielded 8671 records and the detailed search process is shown in figure 1. After duplicates were removed, a total of 4259 records were screened by titles and abstracts. After removing the articles out of scope (irrelevant to RS), the full text of 79 articles was further evaluated and 66 articles were removed based on relevant selection criteria. No extra records were identified after checking the reference lists of the eligible papers, review articles, executive summaries or editorials.

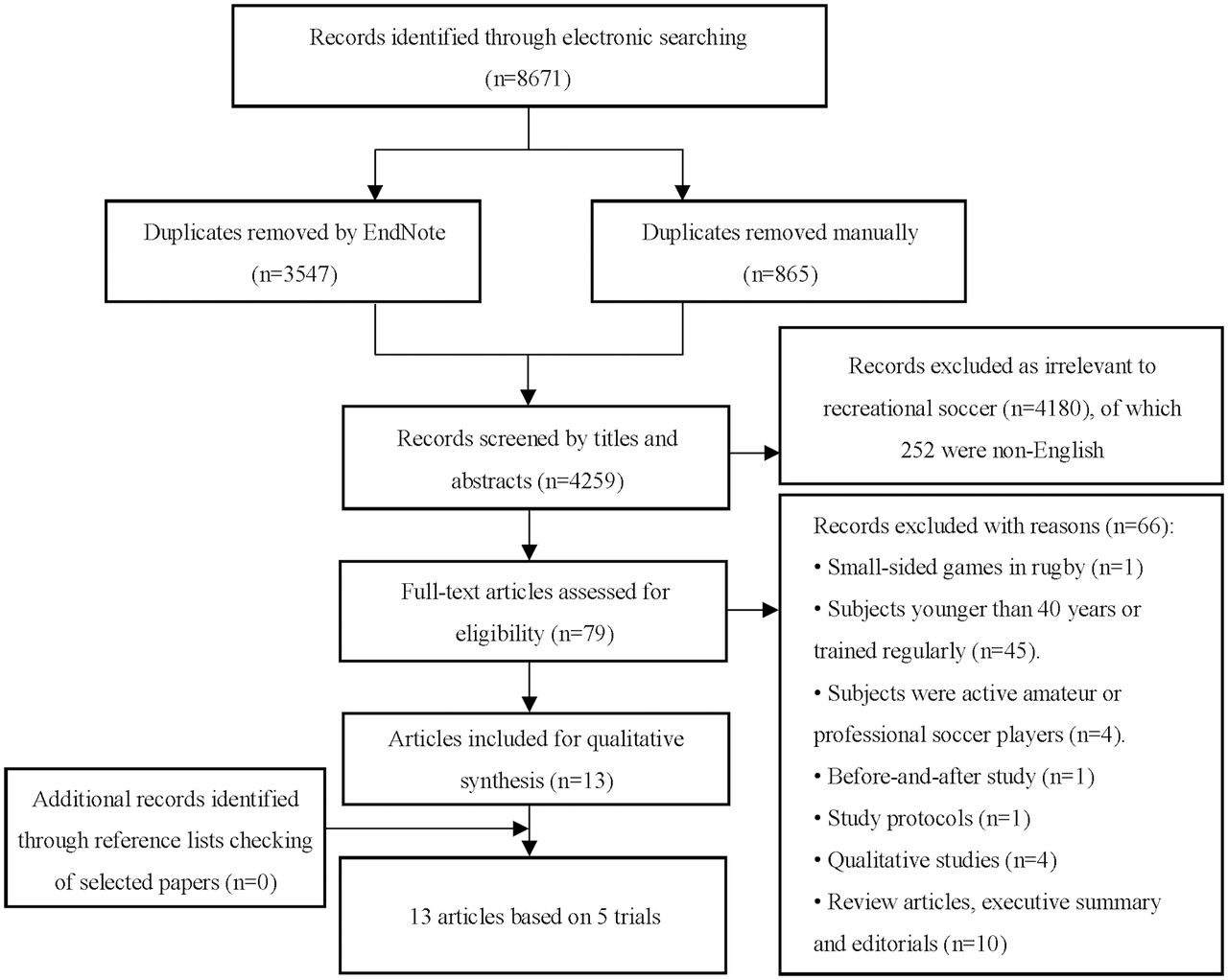{kind=link}
Flow diagram of study selection.
According to the inclusion criteria, 5 trials described in 13 articles22 27–38 were finally included, of which 4 independent trials were described in more than one paper. As all articles22 27–38 reported different health-related outcomes resulting from RS training, they were included in this systematic review.
Risk of bias assessment
The risk of bias assessment of the trials is presented in online supplementary file 4. As four trials were described in more than one paper, the risk of bias was assessed based on the first published article.22 27 33 36 38 However, due to various disparities in trial description among papers from the same trial, the scores of the trials reported in the follow-up papers28–32 34 35 37 are also listed. Scores of the included trials22 27 33 36 38 ranged from 6 to 9 points out of 12. The least scored criteria for the included articles were items 5 (blinded outcome assessor, 100% absent), 2 (treatment allocation concealed, 92% absent) and 7 (intention-to-treat analysis, 85% absent), while the most scored criteria were items 3 (groups similar at baseline, 100% present), 4 (specific eligibility criteria, 100% present), 6b (point estimates and measures of variability with values for each group, 100% present) and 9 (between-group statistical comparison, 100% present).
Supplemental material
Study characteristics
The characteristics of included trials with regard to participants, intervention programme and outcomes are presented in tables 1–3, respectively. All papers were published between 2013 and 2017, with the majority undertaken by a Danish group and the remainder by Brazilian and UK investigators.
Characteristics of the included articles: participants
Characteristics of included articles: interventions
Characteristics of included articles: outcomes
Participants
Demographic data and health status
Two trials reported in three articles36–38 included both men and women, while the other three trials reported in ten articles22 27–35 involved only men (table 1). Sample sizes ranged from 20 to 57 subjects, but in three of the five trials, the number of participants randomised was reported differently in the published articles.22 27–32 36 37
The age range of participants was from 43 to 75 years. Five articles27 28 32 34 35 did not report the age range but only provided the mean and SD or SE. However, in the trial with five papers,22 29–32 two22 30 reported the participants’ age as 65–75 years, two29 31 as 63–74 years, and the remaining one32 referred to the articles by Schmidt et al 22 and Andersen et al.29 Regarding participant health status, one trial by Schmidt et al 22 29–32 involved healthy subjects, two trials27 28 36 37 involved patients with type 2 diabetes (T2D), the trial by Uth et al 33–35 included men with locally advanced or metastatic prostate cancer (PCa) undergoing androgen deprivation therapy (ADT), and the trial by Reddy and colleagues38 did not report health status.
Participant dropouts
Participants’ withdrawal was reported except for the study by Reddy and colleagues,38 which apparently had no dropouts. However, the dropout number was reported inconsistently among the other trials and accompanying articles. In the trial by Schmidt et al,27 six and nine participants were reported dropping out in weeks 12 and 24, but in the companion paper by Andersen et al 28 there were no dropouts at week 12 and only three dropouts were reported at week 24. Three articles22 29 31 from the trial with healthy older men reported that one participant withdrew from the trial, but four and two participants were reported dropping out in the companion papers by Helge et al 30 and Sundstrup et al,32 respectively. Two33 35 of the three published articles from the trial by Uth and colleagues reported eight and nine participants dropping out. Both articles36 37 from the trial by de Sousa and colleagues reported 10 participants withdrawing from the trial, but the dropout rates were 22.7% and 19.6%, respectively, due to different sample sizes provided.
Interventions
Of the five trials,22 27–38 three were RCTs,22 29–35 38 one RUT36 37 and one NRCT27 28 (table 2). All the RCTs allocated participants into a soccer training group and a control group, but the RCT with healthy older men22 29–32 had an extra comparative treatment group, that is, resistance training. The trial by de Sousa et al with patients with T2D36 37 randomised participants into soccer+diet group or a diet-only group, while in the NRCT participants formed a training group and a control group.
Intervention period, frequency and session duration
The average duration of the intervention was 28 weeks, with specific reported durations of 12,33 35–38 16,29 24,27 28 3234 and 52 weeks22 30–32. Except for the trial by Reddy et al,38 all programmes required participants to exercise two or three times weekly, in which two trials (with six articles)22 30–33 35 progressed from two to three sessions per week, and one paper34 from the PCa trial reported that training commenced with two sessions per week for 8 weeks, increased to three sessions per week for 4 weeks, then decreased to two sessions per week for 20 weeks. In the trial of patients with T2D by de Sousa et al,36 37 nutritional counselling and nutritional education programme were undertaken once per week and every 2 weeks, respectively. The most common session duration was 60 min.22 27–32 38 In the PCa trial by Uth et al,33–35 training session duration increased from 45 to 60 min after week 5, while 40 min sessions were undertaken in the trial with patients with T2D.36 37
Training volume, intensity and attendance
The prescribed soccer training volume varied greatly with either progressive or a fixed volume prescribed. In the trial for healthy older men,22 29–32 volume progressed from 15 min per game for three games per session for the first 3 months to four games per session in months 3–12, with a 2 min rest interval between games. An incremental training volume was also provided in the trial by Uth et al 33–35 in patients with PCa, which was 15 min per game for two games per session in weeks 1–4 to three games per session in weeks 5–32. An unchanged volume of 10 min per game for five games per session with a 2 min rest interval between games was prescribed in the trial of men with T2D by Schmidt et al,27 28 and in the trial by de Sousa and colleagues36 37 the volume for each training session was 12 min per game for two games with 3 min rest between games. In the remaining trial by Reddy et al, 38 the volume was not specified.
Although training intensity was not prescribed, session monitoring indicated that the average training intensity was at least 76% of the maximum heart rate (HRmax), although most studies had an intensity of approximately 80% and this was reported in nine articles27–30 32 33 36–38 that comprised all trials. Of these, six papers27–30 32 33 from three trials with healthy participants, and patients with T2D and PCa, reported an average training intensity of >82% HRmax. All trials reported training attendance rate (ranged from 46.2% to 77.1% of prescribed sessions completed), excluding the trial by de Sousa and colleagues36 37 in which one article37 only reported that 19 of the 22 RS intervention participants completed 100% of the training sessions.
Game formats
A variety of soccer game formats were used with three to seven players a side. However, the number of players involved was reported differently among some papers from the same trial. In the article by Schmidt et al 22 in healthy men, games comprised three to five players a side, while the maximum number was six when reported by Andersen et al,29 and a minimum number of four a side when reported by Andersen et al 29 and Sundstrup et al.32 In addition, the minimum number of players each side was reported as five in the first published paper by Uth et al 33 from the PCa trial, although this was reported as three in one35 of the follow-up articles.
Field of play
Seven papers22 31–33 35–37 from three trials reported that both an outdoor natural grass pitch and an indoor wooden floor were played on due to alterations in weather conditions. Three articles29 30 38 that comprised two trials reported playing only on an outdoor surface (natural grass29 30 or artificial grass pitch38), although this was reported as both indoor and outdoor in the other papers22 31 32 from the same trial with healthy older men, and the trial by Schmidt et al 27 28 in patients with T2D reported an indoor wooden court was used. Only one34 paper from the PCa trial did not report the field of play, although both outdoor and indoor surfaces were stated in the other two trial papers.33 35 Three trials reported in five papers22 27 28 31 35 mentioned the size of the field, with 30–45 m×45–60 m for the outdoor pitch and 20 m×40 m for the indoor court or about 100 m2 per player.
Supervision
Supervision was provided in two22 29–35 of the five trials by either a research staff member22 29–32 or an experienced exercise instructor (exercise physiologist or physiotherapist).33–35 In another trial by de Sousa et al reported in two articles,36 37 one article37 reported that intervention training was supervised, although it did not specify who the supervisor was, while the other article36 did not mention supervision.
Outcomes
A wide array of endpoints were reported in the included articles22 27–38; however, due to the focus of the review on health-related benefits, only the most commonly reported variables relating to cardiovascular function, body composition and functional ability were assessed (table 3).
Cardiovascular function
The VO2max and blood pressure (BP) were the two most commonly evaluated cardiovascular variables. Four trials reported in seven articles22 27–29 33 36 37 measured VO2max using either an incremental cycle ergometer test22 27–29 33 or treadmill test,36 37 and all reported a significant improvement between pretest and post-test, in which six22 27–29 36 37 quantified the increase as a percentage from 10.0% to 17.1%, and one33 presented it relative to body weight as 1.0 mL O2/kg/min (~3.7%). However, there was some variation in the amount of improvement within the same trial. For example, in the trial of healthy older men, Schmidt et al 22 reported an improvement at 16 weeks of 15.7%, while in the companion paper by Andersen et al 29 it was 13.5%. In a similar fashion, the change in VO2max was reported as 10% and 11.4% in the two papers36 37 from the trial of patients with T2D by de Sousa and colleagues. Of the seven aforementioned articles, two22 36 reported a significant difference from the resistance training group22 or diet group,36 and the trial by Schmidt et al in T2D27 28 found a significant change compared with controls. BP was reported in three trials,22 27 38 in which only one27 reported a significant within-group and between-group change.
Body composition
Lean body mass (LBM) was assessed by dual X-ray absorptiometry (DXA) in four trials and reported in six articles,28 31 33 34 36 37 with only one paper33 from the trial of patients with PCa reporting a significant within-group change. Two articles31 33 from different trials reported significant between-group changes, but only one33 was in favour of the soccer training group.
Seven articles28 31 33 34 36–38 comprising all trials reported on body fat (four trials that reported fat mass and fat percentage (%fat) used DXA,28 31 33 34 36 37 and one trial that reported only %fat used bioelectric impedance38), in which two articles28 37 from different trials in T2D reported a significant decrease from baseline in fat mass and %fat, and one accompanying paper by de Sousa et al 36 in only fat mass. Interestingly, in the two papers36 37 from the trial of patients with T2D by de Sousa et al, one36 reported that the reduction of fat mass from baseline was 3.7 kg in the diet-only group, but the change was 2.7 kg in the companion paper.37
Total body bone mineral density (BMD) assessed by DXA was provided in two trials30 35 with no significant changes reported. Femoral neck and total hip BMD results were presented in papers from two trials,30 34 of which one30 in healthy older men reported a significant difference between baseline and 16 weeks, and the other one34 in men with PCa reported a significant difference compared with controls in total hip BMD. Leg BMD was reported in two trials28 35 and lumbar spine BMD in one,34 but no significant changes were noted.
Functional ability
Lower limb muscle function and strength were predominantly measured by sit-to-stand (STS), stair climbing (SC) and 1-repetition maximum (1RM). STS results were presented in four articles29 32–34 from two trials with healthy older men and patients with PCa with a significant improvement from baseline, although the reported change was somewhat inconsistent in two29 32 of the companion papers. In addition, two companion articles29 32 in the trial of healthy older men reported a significant difference in STS compared with the control group. SC was reported in two articles32 34 from different trials and both reported significant changes from baseline and the control group. 1RM knee extension strength was reported in two33 34 papers from the same trial in patients with PCa with a significant change from baseline, but only one33 reported a significant between-group difference. Postural balance was assessed in three trials and reported in four articles32 34 35 38 using either the Flamingo test38 or SWAY balance test (with such stances as single-leg, bipedal and tandem)32 or both,34 35 although none reported a significant within-group or between-group difference as a result of training.
Discussion
To our knowledge, this is the first systematic review examining the various health-related effects of RS exclusively in middle-aged and older adults. Based on the current evidence, RS has many potential benefits for middle-aged and older adults. Regardless of the substantial heterogeneity among subjects, study designs and intervention programme in the included trials, RS may induce significant changes in cardiovascular function, body composition, lower limb muscle function and strength, although no significant adaptive changes were observed in postural balance.
Cardiovascular adaptations
Soccer is an intermittent activity involving various intensities of locomotive movements, ranging from walking to high-speed sprints, imposing considerable demands on the cardiovascular system.39 Studies suggest that cardiovascular fitness is superior in older soccer players with lifelong soccer participation than for age-matched sedentary individuals40–42 and lifelong strength-trained athletes,42 and comparable with elderly endurance runners.42 It is well established that RS has similar high aerobic demands to elite soccer training.21 43 Moreover, several reviews and a meta-analysis indicate that short-term to long-term RS training is similar to interval training and superior to continuous running and strength training in improving VO2max 16 20 21 44 and BP16 21 44 in untrained, healthy or unhealthy persons.
The results of this review agree with previously conducted reviews mentioned above. In the four trials22 27–29 33 36 37 that assessed aerobic capacity, VO2max significantly increased ~4%–17% following RS. However, it needs to be noted that not all included trials assessing BP reported significant changes following training. Two trials22 38 with subjects of either healthy or unknown health status did not report any significant within-group and between-group changes. However, participants in the soccer training groups in these two trials had either normal BP or mild hypertension at baseline. In addition, in the trial of subjects with mild hypertension,38 the training stimulus provided of only one session per week for 12 weeks was likely suboptimal to induce a reduction in BP according to the American College of Sports Medicine45 and the Exercise and Sports Science Australia46 position stands on exercise and hypertension.
Body composition and skeletal health
RS is also well documented to be beneficial in inducing positive changes in body composition in various populations. Multiple studies have shown that short-term (12–16 weeks) low-moderate volume RS training is effective in inducing significant changes in total body or regional fat mass,19 47–52 %fat47 48 50–52 and LBM19 47 53–55 in untrained persons.
In contrast, only a few studies have demonstrated beneficial effects on skeletal health after short-term training, and the positive effects were only for lower limb bone mass and markers of bone turnover.18 19 These changes likely result from the increased mechanical loading induced by RS.39 56 However, detecting changes in BMD by DXA following short-term training is unlikely given that the length of the bone remodelling cycle is approximately 4–6 months.57 Enhanced bone mass has been reported to be higher in elite female soccer players than in untrained young women58 and in untrained women undergoing prolonged RS training.59–61
The results from the reviewed trials indicate that RS can be conducive to positive changes in body composition in middle-aged and older adults and especially for those with T2D or PCa undergoing ADT. Of all the papers examining the effects of RS on body composition,28 30 31 33–38 three papers28 36 37 from two separate trials with patients with T2D reported a significant reduction in fat mass and %fat; one paper33 from the trial with PCa survivors reported an increase in LBM similar to that observed with combined resistance and aerobic training62; and one article30 from the 52-week trial with healthy older adults reported significant improvement in regional BMD.
The mechanisms behind the larger reduction of fat mass in middle-aged and older patients with T2D through RS training could be the enhanced effects resulting from their antidiabetic medications28 36 37 or additional dietary intervention36 37 concurrently received during training. Studies have shown that metformin, the widely used oral antihyperglycaemic agent,63 can significantly reduce fat mass and %fat,64 as well as appetite and caloric intake,65 in patients with T2D. On the other hand, the greater improvement of LBM in the PCa survivors undergoing ADT for 1–2 years after a 12-week training programme is probably due to lower baseline values of the participants, given that a substantial loss of muscle mass occurs during the initial period of ADT.66 67
Functional ability
Maintaining or enhancing functional ability is essential in older persons in order to maintain independent living. Many factors such as cardiovascular fitness, muscle strength and endurance, and balance can influence functional ability. In addition to the positive adaptations in aerobic capacity, RS as an intermittent sport has particular benefits for anaerobic performance,54 60 postural balance,17 55 61 lower limb muscular strength53 55 and function61 in young and middle-aged adults, with some changes more significant than continuous running. Similarly, in this review, significant positive adaptations in lower limb muscle function29 32–34 and strength33 34 were observed. But unlike the findings in younger adults, no marked difference was reported in postural balance.32 34 35 38
Engagement in RS for middle-aged and older adults
RS is reported to be an enjoyable activity that may lead to continued exercise engagement during68–70 and even after44 participation in a study intervention; however, the highest attendance rate reported in the reviewed articles was ~78% for a short-term (12 weeks) low-frequency (one session per week) programme.38 In the long-term trial of healthy older men,22 30–32 even traditional resistance training had a higher attendance rate than RS training (73% vs 66%). Furthermore, in the 32-week training study on patients with PCa,34 only 46% of the training sessions were completed, which contrasts with the conclusion from a qualitative investigation related to the trial that soccer is a unique strategy contributing to higher physical activity adherence in patients with PCa.71 However, reporting of programme compliance was lacking in the trials, which is one of the determinants of the effects derived from an activity programme, as it is possible that a subject may attend a session but not comply with the prescribed intensity or volume.72 Therefore, additional work would be beneficial in examining the long-term sustainability of RS in untrained/sedentary middle-aged and older adults, and those with chronic conditions including cancer survivors. In addition, although participation in RS may be safe for middle-aged and older adults, it is still necessary to provide close supervision during the play to prevent potential injury, as the reduction in muscle strength and balance in combination with unfamiliar movements especially in older adults may contribute to falls and subsequent facture.
Limitations
Since the earliest retrievable RCT by Krustrup et al 19 published in 2009, a number of trials have been conducted investigating the health-related effects of RS in untrained subjects, the majority of which involved young adults, adolescents and children, which limited the number of trials available for the current review. Moreover, we found that many articles titled with ‘middle-aged’ or stated investigating the effects of RS in mid-life actually included young adults as participants.18 53 60 73–75
Within the five separate trials22 27–38 included in this review, the sample sizes were generally small, although an extensive array of outcomes were assessed. As a result, there are some potential limitations which are worthy of comment. First, we only presented the most commonly reported variables that may have been assessed with the use of different technologies and procedures. Second, numerous inconsistencies and ambiguities exist among the papers in trial description with regard to participants, the intervention programme and outcomes. Third, a complementary search strategy undertaken to ensure thorough literature searching and avoid missing any relevant literature was to search for well-known authors in the field,76 although this also has the potential to introduce bias in the selection of papers. However, no additional papers were identified through author searching. Moreover, although major bibliographic searches were undertaken, manual searching of electronic publication lists of key journals and forward citation tracking were not used during the literature search. Fourth, although study eligibility was examined by two independent reviewers and a third reviewer when required, the initial screening of title and abstract was only undertaken by one reviewer. In addition, due to the heterogeneous nature of the included trials, a meta-analysis was not performed. Lastly, the risk of publication bias may exist as only full-text, peer-reviewed journal articles were included, and risk of language bias may also exist as we only included articles published in English.
Future directions
RS appears to be feasible and beneficial for untrained, healthy or unhealthy middle-aged and older men and women, although robust evidence is lacking. Additional high-quality RCTs are required with focus on study design and reporting of factors related to bias to determine the benefits of RS for different populations especially those with various chronic conditions, as well as in women given that most trials to date have been predominantly in men. In addition, the presence of small or moderate effects of RS training on some health-related endpoints justifies further investigation into the optimal prescription of RS with larger sample sizes and power calculations provided. Finally, additional work is necessary to compare the beneficial effects between RS and other team sport activities (such as touch rugby, netball or basketball) and to develop approaches maintaining higher training adherence in the target populations, especially those with chronic conditions and no prior soccer experience.
Conclusion
RS as sport medicine has potential benefits and should be considered an alternative exercise modality for untrained, healthy or unhealthy middle-aged and older men and women to maintain an active lifestyle and mitigate a wide array of age-related changes in physical and physiological function. However, due to the paucity and variation in quality of available trials, additional high-quality RCTs are required to establish more compelling evidence on the positive effects of RS for various populations and especially those with chronic conditions such as cancer, T2D and cardiovascular disease.
References
Footnotes
Contributors HL, RUN, FM, DAG and DRT contributed to the development of the research question, study design and literature search strategy. HL conducted the literature search. HL and DRT performed the study selection, methodological quality assessment and data extraction. All authors contributed to data interpretation. HL developed the first draft, and all authors developed the subsequent drafts of the manuscript. All authors reviewed and approved the manuscript.
Funding HL is funded by the China Scholarship Council (CSC) in conducting collaborative study into sport medicine at Edith Cowan University (ECU) as a visiting scholar. DAG is funded by a Cancer Council Western Australia Research Fellowship.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.