Article Text

Abstract
Background Recent studies have examined haemodynamic changes with stressors such as isometric handgrip and rapid atrial pacing in heart failure with preserved ejection fraction (HFpEF), but little is known regarding left ventricular (LV) pressure–volume responses during dynamic exercise.
Objective To assess LV haemodynamic responses to dynamic exercise in patients with HFpEF.
Methods Twenty subjects with normal ejection fraction (EF) and exertional dyspnoea underwent invasive haemodynamic assessment during dynamic exercise to evaluate suspected HFpEF.
Results LV end-diastolic pressure was elevated at rest (>15 mm Hg, n=18) and with exercise (≥20 mm Hg, n=20) in all subjects, consistent with HFpEF. Heart rate (HR), blood pressure, arterial elastance and cardiac output increased with exercise (all p<0.001). Minimal and mean LV diastolic pressures increased by 43–56% with exercise (both p<0.0001), despite a trend towards a reduction in LV end-diastolic volume (p=0.08). Diastolic filling time was abbreviated with increases in HR and the proportion of diastole that elapsed prior to estimated complete relaxation increased (p<0.0001), suggesting inadequate relaxation reserve relative to the shortening of diastole. LV diastolic chamber elastance acutely increased 50% during exercise (p=0.0003). Exercise increases in LV filling pressures correlated with changes in diastolic relaxation rates, chamber stiffness and arterial afterload but were not related to alterations in preload volume, HR or cardiac output.
Conclusion In patients with newly diagnosed HFpEF, LV filling pressures increase during dynamic exercise in association with inadequate enhancement of relaxation and acute increases in LV chamber stiffness. Therapies that enhance diastolic reserve function may improve symptoms of exertional intolerance in patients with hypertensive heart disease and early HFpEF.
- Heart failure
- diastolic dysfunction
- haemodynamics
- exercise
- old age
Statistics from Altmetric.com
Introduction
In the healthy human, cardiac output increases over threefold with exercise through coordinated increases in heart rate (HR), contractility, vasodilation and ventricular preload.1 The latter, quantified by left ventricular (LV) end-diastolic volume, increases 20–40% during low-level exertion despite abbreviation of the time available for ventricular filling with tachycardia.2 Enhanced chamber filling during exercise is accomplished with little change in ventricular filling pressures in the healthy heart, related principally to the greater ‘suction’ of blood from atrium to a compliant LV chamber.3 Indeed, the ability to enhance preload volume with exercise is a critical mechanism by which the aged heart maintains cardiac output responses during exercise, partially compensating for age-associated losses of systolic, chronotropic and vasodilator reserves.4
LV diastolic dysfunction is common with ageing and is a hallmark finding among patients with heart failure with preserved ejection fraction (HFpEF),5 leading to increases in LV filling pressures both at rest and with exertion.6–10 Previous studies have investigated LV haemodynamic responses during stress in HFpEF but were performed during stressors that are less typical of activities of daily living such as rapid atrial pacing11 or isometric handgrip,7 9 10 and little is known regarding the LV pressure–volume response to dynamic exercise. The current study examined haemodynamic changes with supine dynamic exercise in patients with newly diagnosed HFpEF.
Methods
Subjects
This was a prospective single-centre study conducted between February 2006 and April 2007 examining consecutive patients with normal LV ejection fraction (>50%) referred to the Mayo Clinic catheterisation laboratory for the assessment of exertional dyspnoea who were found to have invasive haemodynamic findings diagnostic of HFpEF. HFpEF was defined by invasive evidence of diastolic dysfunction: prolonged LV relaxation at rest (τ >48 ms) and/or elevated filling pressures (LV end-diastolic pressure >15 mm Hg at rest or >22 mm Hg with exercise).8 10 12 Patients with obstructive coronary artery disease (any stenosis ≥50%), significant valvular heart disease (any stenosis, >mild left-sided regurgitation, severe tricuspid regurgitation, prior valve surgery), hypertrophic or infiltrative cardiomyopathy, pulmonary disease, atrial fibrillation or acute pulmonary oedema were excluded. Subjects were studied on chronic medications.
Cardiac catheterisation
Left heart catheterisation was performed through a 6 Fr sheath placed in the femoral or radial artery after minimal sedation. LV pressures were continuously measured using high fidelity micromanometer-tipped catheters (Millar Instruments, Houston, Texas, USA) and digitally saved (250 Hz). All pressures were measured at end-expiration and represent the mean of ≥3 beats.
Echocardiography
Transthoracic echocardiography was performed during catheterisation by an experienced sonographer. High-fidelity pressure data were input directly to the echocardiography machine, projected simultaneously over Doppler spectra and stored for offline analysis. LV end-systolic and end-diastolic volumes were determined by the modified single-plane Simpson method from the apical four-chamber view with determination of LV mass.13 Transmitral filling waves and E wave deceleration times were determined from pulse wave Doppler. Time-varying LV volume was derived by integrating the mitral inflow Doppler signal over time and using the end-systolic and end-diastolic LV volumes calculated from two-dimensional echocardiography.5 Resting tissue Doppler early diastolic velocity (e′) was measured at the septal mitral annulus. Stroke volume (SV) was determined from pulse wave Doppler of the LV outflow tract. Cardiac output was determined by the product of SV and HR. Arterial afterload was assessed by effective arterial elastance (Ea=end-systolic pressure/SV), a lumped measure of pulsatile and mean resistive arterial load.14 Volumetric data were scaled to body surface area.
Assessment of diastolic function
The beginning and end of diastole were defined by peak negative pressure change and closure of the mitral valve, respectively.15 Diastolic filling time was defined from opening to closure of the mitral valve. Minimal diastolic LV pressure was determined as a surrogate measure for early diastolic suction.3 Mean LV diastolic pressure (mLVDP) was determined from opening to closure of the mitral valve and used as the primary index of LV filling pressures. LV end-diastolic pressure (LVEDP) was determined after the atrial deflection and prior to isovolumic contraction. The time constant of isovolumic relaxation (τ) was calculated using the monoexponential zero asymptote method16 as well as non-zero asymptote and hybrid logistic methods.15 While the time to ‘complete relaxation’ cannot be determined, we approximated this time after 3.5 monoexponential time constants, as shown by Weisfeldt et al.17 The proportion of diastole which had elapsed at estimated complete relaxation was then calculated as 3.5τ/diastolic filling time and examined as an index of relaxation reserve.16–18
LV volume was plotted against pressure to derive the single-beat diastolic pressure–volume relationships. The linear slope of the single-beat diastolic pressure–volume relationship was designated as diastolic elastance (Ed) and was used as a measure of chamber stiffness.15 18 Pressure measured in this way does not accurately gauge passive ventricular stiffness properties because relaxation is incomplete during early to mid diastole, making measured pressures higher than they would be from passive chamber filling alone.19 In order to examine the ‘passive’ compliance properties of the ventricle (independent of ongoing pressure relaxation), the theoretical ‘excess’ pressure attributed to ongoing relaxation was determined from monoexponential extrapolation of isovolumic pressure decay.5 This excess LV pressure was then subtracted from the measured LV pressure to obtain corrected LV pressure (figure 1).20 Relaxation-corrected LV pressure was then plotted against the simultaneous LV volume to construct the relaxation-corrected diastolic pressure–volume relationship. The linear slope of this relation (EdC) was used to reflect passive diastolic chamber stiffness at rest and during exercise.

Estimation of left ventricular (LV) passive diastolic stiffness: ‘corrected’ LV pressure (dotted line) is obtained by subtracting the ‘relaxation pressure’ (dashed line), obtained by monoexponential extrapolation of the isovolumic relaxation period from the measured LV pressure. This ‘corrected pressure’ is then plotted against simultaneous LV volume and the points are fitted into a straight line.
Study protocol
Haemodynamic measurements were made at baseline and during supine exercise (cycle ergometer, n=11; arm weight adduction, n=9) performed to the level of patient exhaustion or systolic blood pressure >230 mm Hg. Cycle ergometry was started at 20 Watts and increased by 20 Watts every 2 min, then maintained at the maximally tolerated level to allow completion of echocardiographic measurements. For arm exercise, repetition frequency was gradually increased to subjective maximum tolerated effort.
Statistical analysis
Continuous variables are reported as median (IQR) and categorical variables as percentages. Changes in haemodynamics with exercise were assessed by the Wilcoxon signed-rank test. Bivariate (Pearson coefficient) linear regression was performed to test associations between changes in diastolic filling pressures and changes in haemodynamic responses during exercise.
Results
Study population and baseline haemodynamics
Subjects were predominantly older men and women with chronic NYHA class II–III symptoms of exertional dyspnoea (table 1). Half were obese, 47% had left ventricular hypertrophy and 65% had left atrial enlargement. Systolic blood pressure and LV filling pressures were elevated at rest (table 2). All subjects displayed objective evidence of diastolic dysfunction indicative of HFpEF as the aetiology of chronic dyspnoea: 85% had elevated resting LVEDP (>15 mm Hg), 50% had prolonged LV relaxation (τ >48 ms) and one subject had diastolic dysfunction only during exercise (LVEDP >22 mm Hg).
Baseline characteristics
Resting and exercise haemodynamics
Exercise performance
Subjects performing cycle ergometry (n=11) exercised for 9.8±4 min reaching peak workload of 60±40 Watts, while subjects performing arm weights (n=9) exercised for 5.8±1 min. Haemodynamic responses were similar for cycle and arm exercise and patients with or without chronic β blocker use (p>0.1 for all). HR, blood pressure, cardiac output and EF increased significantly with exercise (table 2) while LV end-systolic volume decreased, consistent with an increase in contractility.
LV diastolic reserve with exercise
While cardiac output increased with exercise, LV end-diastolic volume tended to decrease (p=0.08) despite a marked increase in LV diastolic filling pressures (table 2). Minimum, mean and end-diastolic pressures increased by 43–58% during exercise (all p<0.0001). The time constants of isovolumic pressure decay (τ) tended to shorten as did the echo-Doppler isovolumic relaxation time (p=0.003). However, enhancement in relaxation with exercise was inadequate to compensate for rate-related shortening of the diastolic filling period, as the proportion of diastole elapsed prior to estimated complete relaxation lengthened from 32% to 50% (p<0.0001).
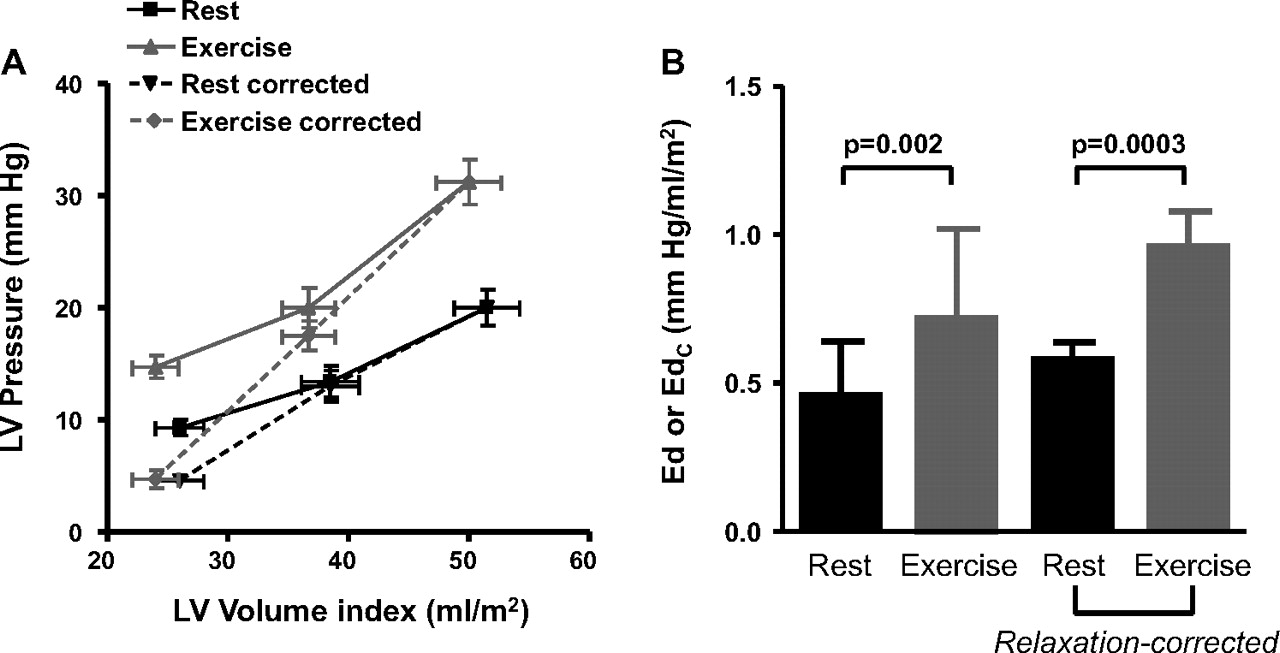
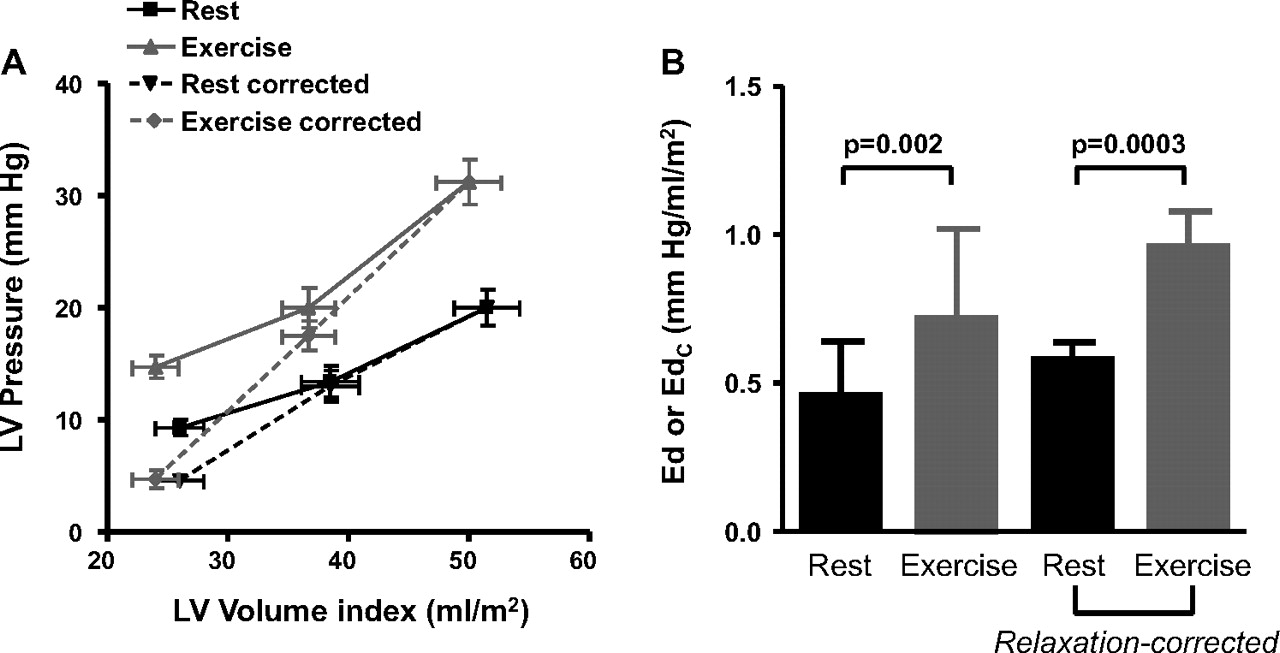
The increase in filling pressure without an increase in preload volume suggests an increase in the slope and/or position of the diastolic pressure–volume relationship. Single-beat diastolic pressure–volume relationships demonstrate an acute change in position with exertion (figure 2A), with an increase in the linear slopes of these relationships (figure 2B), both prior to and after correcting for effects of ongoing/incomplete relaxation (table 2). E wave deceleration time, which varies inversely with chamber stiffness,21 similarly declined with exercise.
{kind=link}
{kind=link}
(A) Summary data for diastolic pressure–volume relationships of all patients at rest (black) and with exercise (shaded), plotting both raw (solid lines) and relaxation-corrected data (dashed lines). With exercise the position of the diastolic pressure–volume relationship curve shifts upward with increasing pressure despite similar chamber volume. (B) Chamber stiffness determined from the linear slopes of (A) similarly showed significant increases in chamber stiffness during exercise.
The change in mean LVDP with exercise was correlated with acute changes in chamber stiffness (r=0.76, p=0.0007), the time constant of relaxation (r=0.59, p=0.007) and arterial elastance (r=0.61, p=0.02), but were unrelated to changes in end-diastolic volume, HR or cardiac output. In multivariate analysis, the combination of the changes in τ and Ed explained 74% of the variability in the change in mean LVDP (p=0.0002).
Discussion
We examined LV diastolic responses to dynamic exercise in stable outpatients with exertional dyspnoea and normal ejection fraction who were found to have HFpEF based on invasive diagnostic criteria.8 10 12 Marked elevations in LV filling pressure were noted during exercise despite reductions in preload volume. Diastolic reserve with exertion was impaired: chamber elastance acutely increased and enhancement in relaxation kinetics was insufficient to compensate for rate-related reduction in diastolic filling time. Exercise changes in relaxation and stiffness were each associated with the extent of elevation in filling pressures, as was the change in arterial afterload (Ea). These findings confirm and extend recent studies7–11 showing that abnormalities in diastolic reserve contribute to elevation of filling pressures with exercise in patients with hypertension and early stage HFpEF and represent candidate therapeutic targets.
Diastolic relaxation reserve
Dynamic increases in cardiac output with physical exercise are achieved by augmentation in HR, contractility, vasodilation and diastolic ventricular chamber filling.1 2 The former three mechanisms become impaired with ageing and in patients with chronic hypertension, making the aged hypertensive heart more dependent upon diastolic reserve to increase cardiac output with exercise4 and thus more vulnerable to the deleterious effects of diastolic dysfunction. Enhanced diastolic filling is achieved via two principal mechanisms in the healthy heart: contraction to lower end-systolic volumes (increasing elastic recoil) and enhanced relaxation related to β-adrenergic stimulation—promoting augmented diastolic ‘suction’ during exercise.3 These reserve mechanisms are lost in chronic heart failure with reduced EF, such that increased chamber filling occurs at the expense of left atrial (and ventricular) hypertension.22
Previous studies in healthy humans have shown that, while preload volumes increase during exercise, LV filling pressures remain stable or increase only slightly.18 23 However, few studies have directly examined LV diastolic pressure–volume responses during dynamic exercise. Nonogi et al showed in nine healthy patients that isovolumic relaxation rates increase by more than 50% with supine exercise, such that relaxation is more complete during early diastole and the ventricle can fill to greater preload volumes during a shorter interval without increasing filling pressures.18 In contrast, relaxation rates (assessed by τ) increased by half of this amount in the current study, and the extent of relaxation was consequently less complete in early diastole, promoting an increase in early diastolic LV minimal pressure. These findings observed during dynamic exercise are consistent with and extend recent studies in patients with HFpEF showing blunted enhancement of diastolic relaxation during rapid atrial pacing,11 and in response to isometric handgrip.9
Nonogi et al showed in normal humans that, while LV end-diastolic pressures were not affected by exercise in healthy humans, viscoelastic diastolic chamber stiffness nonetheless increased, similar to increases noted in the current study.18 However, in contrast to our data, this was due to a marked decrease in early diastolic LV minimal pressure in the latter study with no change in end-diastolic pressure, and this led to an increase in the slope of the pressure–volume relationship. In contrast, we found a marked increase in early diastolic minimal pressure in patients with early stage HFpEF, indicating insufficient ventriculoatrial suction with exercise.22 Similar impairments in LV diastolic suction and untwisting with exercise have recently been demonstrated non-invasively in studies from the Sanderson laboratory in both patients with HFpEF and hypertensive patients with exertional dyspnoea.24 25 We observed an increase in the atrioventricular pressure gradient, as evidenced by an increase in the transmitral E wave velocity. This increase in the atrioventricular pressure gradient was achieved only at the expense of an increase in diastolic filling pressure, as would be expected to contribute symptoms of exertional dyspnoea. The potential relevance of these findings to the pathophysiology of HFpEF is underscored by the observations that, while healthy humans can increase cardiac output by about 300% with little change in LV filling pressures,1 the current study population were only able to achieve a 35% increase in cardiac output at the cost of a 50% increase in LV filling pressures. This increase in diastolic pressures would be expected to contribute to pulmonary congestion, increase wall stress, myocardial oxygen demand and perhaps precipitate ischaemia in vulnerable patients.
Comparison with previous studies in HFpEF
A number of recent studies have examined diastolic reserve responses to stress in hypertensive heart disease and HFpEF, both invasively and non-invasively,6–11 24–29 yet none has directly assessed LV pressure–volume responses during dynamic exercise. Kitzman and colleagues first showed that depressed cardiac output reserve with exercise in HFpEF was associated with a flat stroke volume response which in turn was related to an inability to augment LV end-diastolic volume.6 This preload reserve deficit occurred despite marked increases in pulmonary capillary wedge pressure, similar to the findings noted in the current study, although LV pressures were not measured. In another seminal study examining LV pressure–volume relationships in HFpEF, Kawaguchi et al found that while relaxation rate (τ) was not different at rest in patients with HFpEF compared with healthy controls, abnormalities in diastolic reserve could be precipitated during the stress of isometric handgrip.9 Handgrip led to marked increases in blood pressure and cardiac afterload in HFpEF, and this was coupled with a prolongation of relaxation and increase in LVEDP. While we noted inadequate relaxation relative to the diastolic period, we did not detect prolongation of relaxation with stress and blood pressure elevation as noted by Kawaguchi and colleagues.9 This difference is probably due to fundamental differences in haemodynamic responses to isometric and dynamic exercise stressors.30
The current results are the first to our knowledge to describe acute increases in viscoelastic chamber stiffness during dynamic exercise in human HFpEF. Westermann and colleagues recently showed that both diastolic stiffness and relaxation are impaired in patients with HFpEF compared with healthy controls at baseline, and that isometric handgrip leads to greater increases in LV filling pressures in HFpEF.7 However, in contrast to the current study, they did not observe that chamber stiffness was acutely altered during exercise—it was similarly more abnormal at rest and during exercise compared with controls, with no stress-induced exacerbation.7 The reason for these disparate findings in our study are not clear but may relate to differences in the type of exercise performed (handgrip versus dynamic ergometry30), the duration of exercise (mean of 8 min in current study vs 1.5 min in prior study), the methodology (single vs multi-beat technique) or the HFpEF populations enrolled. Penicka and colleagues reported an increase in the ratio of LVEDP to end-diastolic volume with isometric handgrip in early HFpEF,10 and Ha et al observed an increase in Ed as estimated by the ratio of E/e′ to stroke volume.29 The current data show that these changes in filling pressure are probably due to a shift up in slope and the position of the diastolic pressure–volume relationship (figure 2). We noted a significant reduction in mitral E wave deceleration time, which varies inversely with chamber stiffness, providing further independent evidence for an acute increase in operant LV diastolic stiffness with exercise.21
Impact of afterload
Elevated arterial elastance is characteristic of both hypertension alone and hypertensive HFpEF,13 and the decrease in arterial stiffness with low-level exercise is known to be attenuated in HFpEF.28 There is important crosstalk between afterload and diastolic function, such that abnormal vascular loading may contribute to or exacerbate diastolic reserve in these diseases.31 Indeed, both diastolic relaxation and chamber compliance are reduced with acute increases in afterload in animal models and some human studies,14 31–33 and recent data suggest that blood pressure reduction may enhance diastolic relaxation.34 The significant correlation between the increases in Ea and changes in LV filling pressures in the current study lends further support to the relationship between abnormal LV loading and diastolic reserve in HFpEF.
Limitations
This study did not include a control group so we cannot determine how the observed changes in diastolic reserve in HFpEF would compare with haemodynamic responses to dynamic exercise in normal humans. However, previous studies have shown that filling pressures remain stable despite increases in LV preload during exercise in healthy humans,23 in association with more dramatic enhancement of relaxation than observed here.18 The theoretical time to ‘complete’ relaxation was estimated as 3.5 time constants. This is an oversimplification that assumes the monoexponential model can be extrapolated beyond the points where the data are analysed and that filling does not alter relaxation, and these assumptions were probably violated although prior studies support this approach17 and it is only intended as an approximation. The true diastolic pressure–volume relationship is curvilinear rather than linear (as estimated here), and is optimally measured from pressure–volume points obtained during diastasis at variable preload using caval occlusion.15 This was not feasible to perform during dynamic exercise so we relied on single-beat techniques. Approximately 40% of LV pressure is due to extrinsic restraint from right heart and pericardial interaction,15 and these forces were not measured and probably contributed to rest and exercise pressures. Previous studies have found that the proportionate contribution of extrinsic forces to LV pressures remains fairly constant during exercise,8 15 although we cannot determine what effect pericardial restraint had on the shape, position or slope of the measured diastolic pressure–volume relationships at rest or with exercise in this study. The type of exercise (arm vs leg) was not standardised, although both were dynamic.
Conclusions
Patients with early HFpEF develop increased LV diastolic filling pressures during supine exercise in concert with acute increases in chamber stiffness and an inability to enhance relaxation to compensate for shortening of diastolic filling time. Dynamic increases in filling pressures correlate with the changes in relaxation, chamber stiffness and afterload during exercise, suggesting that these play important roles in limiting diastolic reserve function and contributing to symptoms of exertional intolerance. Therapies targeting diastolic reserve and abnormal vasodilation with exercise may mitigate symptoms of exertional dyspnoea in patients with HFpEF.
References
Footnotes
BAB and WAJ contributed equally to this manuscript.
Funding BAB receives support from NIH grant HL84907.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Mayo Clinic Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.