Article Text

Abstract
Background Training recovery is vital for adaptation and performance, and to avoid cumulative fatigue and symptoms associated with overtraining. The use of cold-water immersion (CWI) as a recovery strategy is common; however, the physiological and biochemical rationale behind its use remains unclear. This study aimed to assess the relationship between body temperature responses to water immersion and individual perception of recovery, with subsequent exercise performance.
Methods Twelve male rugby players participated in a 3-week cross-over trial where an intense 60 min conditioning session was followed immediately by 15 min of either 14°C CWI, 30°C warm-water immersion (WWI) or passive control (CON) recovery intervention. Postexercise body temperatures and subjective ratings of the recovery intervention were recorded and subsequently related to performance in a 5×40 m repeated sprint protocol undertaken 24 h later.
Results CWI induced large reductions in core body temperature postimmersion (effect size (ES) range 1.05–3.21) and improved subsequent sprint performance compared to WWI (ES 1.04±0.84) and CON (ES 1.44±0.84). Both the degree of temperature decrease at 60 min postimmersion (r=0.6948; p=0.0121) and the subjective rating of the recovery intervention (r=0.5886; p=0.0441) were related to subsequent sprint performance. A very strong linear correlation was observed when these two factors were integrated (r=0.7743; p=0.0031).
Conclusion A combination of physiological and psychological indices provides an improved indication of subsequent performance and suggests an important role of individual perception in enhancing training recovery.
- Intervention effectiveness
- Muscle damage/injuries
- Rugby
Statistics from Altmetric.com
Introduction
Bishop et al1 have identified ‘training recovery’ as the vital period between successive training sessions or competitions with the potential to improve subsequent performance, and highlight the fact that athletes will spend more of their time recovering than they do in training. Thus, the recovery process is a crucial component of the adaptive process2 and it is necessary for athletes to engage in effective strategies to avoid the potential maladaptive physiological and psychological effects of overtraining.3
Hydrotherapy is one strategy that is commonly employed to assist in recovery4 and cold-water immersion (CWI) has been heavily researched as a strategy to mitigate the negative effects of muscle damage and has been shown to improve subsequent exercise performance.5–9 Repeated sprint ability has been demonstrated to correlate with on-field performance in rugby10 and in a male team-sport cohort, researchers have demonstrated that CWI improves sport-specific recovery to a greater extent than passive rest when performing repeated circuits that simulate rugby union games.11 However, the same researchers did not demonstrate this benefit in power tests.12 Additional studies have also shown either no benefit2 ,13 ,14 or even negative effects of CWI on subsequent exercise performance.15–17
The equivocal results seen in the literature may be partially explained by discrepancies in the water immersion protocols, participants of differing training levels, variable measures of recovery that may not be related to athletic performance, gender effects and the fact that the mechanisms responsible for the beneficial effects of CWI have yet to be fully elucidated.4 ,18 ,19 One possible mechanism suggested to account for the positive effects of CWI on subsequent maximal exercise performance is the marked effect on core body temperature,4 ,20–22 although other mechanisms including an attenuation of inflammation and an analgesic effect likely contribute to the effectiveness if the intervention.23
Interestingly, in the study by Higgins et al,15 the detrimental effect of CWI on performance indices was associated with negative subjective measures of its effectiveness, suggesting the contribution of a psychological mechanism. Indeed, a psychobiological tool has been reported to provide valuable information regarding recovery and has been related to sprint performance.24 Further, psychological factors such as expectancy have been suggested to significantly contribute to the both positive and negative sports performance.25
Thus, we suggest that ‘training recovery’ may be better accounted for by employing an integrated approach that combines the psychological perception of the recovery intervention with a range of physiological measures, including a decrease in body temperature. To test this hypothesis, the present study utilised a 60 min high-intensity conditioning session followed by 15 min of either CWI or warm-water immersion (WWI) or a passive seated recovery protocol. Specifically, the relationship between an individual's core body temperature perception of the recovery strategies were evaluated against repeated sprint performance undertaken 24 h after the conditioning session in well-trained team-sport athletes.
Methods
Subjects
Twelve male semiprofessional rugby union athletes who played in a range of positions (mean±SD, age 23.3±1.4 year; height 1.85±0.04 m and body mass 96.7±10.8 kg) and for the same club, were voluntarily recruited. All players had a minimum of 2 years of resistance training experience and the 3-week study was incorporated into the preseason phase of their training programme. The players were divided into three groups with a similar age, body mass, height, strength and speed performance profiles. All participants provided written informed consent, and the study was approved by the ethics committee of the local university.
Experimental protocol
All players first performed a 60 min high-intensity gym and track-based conditioning session which they consistently rated 5 on a 1–5 Likert scale, where 5 was represented by the anchor point ‘Extremely Hard’. Maximal heart rate assessed during the conditioning session ranged from 171 to 204 beats/min (Polar S610i, Kempele, Finland). Three identical conditioning sessions were performed at 1100 h by each player as part of the experimental protocol and each session was separated by 7 days.
Five minutes after the completion of a conditioning session the players performed one of three recovery interventions described below in a counter-balanced, cross-over design. Core body temperature was recorded using an ingestible sensor (CorTemp, HQ Inc, Palmetto, Florida, USA) before and after the conditioning session, and 0, 30 and 60 min postintervention. The ingestible sensor was swallowed at breakfast on the day of the conditioning session and was assumed to be active once it registered 36.5–37°C. If the sensor was lost through defecation subsequent to postrecovery testing, it was replaced.
For the CWI intervention, players sat for 15 min in a temperature-controlled water bath set to maintain a temperature of 14°C6 and immersed their body to the level of the anterior superior iliac spine. They were then removed, seated and rested at room temperature (20°C) for 60 min. Core body temperature was recorded at the 0, 30 and 60 min postintervention time points. The WWI intervention replicated the CWI intervention, except that the water temperature was maintained at 30°C. The passive control (CON) recovery intervention involved the players sitting on a chair for 15 min at room temperature (20°C). They then remained seated for a further 60 min and core body temperature was recorded at the 0, 30 and 60 min postintervention time points.
Within 5 min postintervention, the players were asked to rate each recovery intervention on a 1–5 Likert scale, where 1 was represented by the anchor point ‘Like Very Much’ and 5 was represented by the anchor point ‘Dislike Very Much’. To combine the subjective perception measure with the physiological measure, the percentage decrease in core body temperature was multiplied by (5−rating)+1.
Twenty-four hours after each conditioning and recovery session, core body temperature was recorded again and was followed by 5×40 m repeated maximal running sprints. Sprint speed was assessed via electronic timing light gates on a grass surface (Brower Timing System, Salt Lake City, Utah, USA). One minute separated each sprint effort. Performance maintenance was calculated based on the decrease in sprint speed from the first to last sprint ((Sprint #5/Sprint #1)×100). Participants were instructed not to take any anti-inflammatory drugs and refrain from consuming alcohol in the 48 h prior to each testing day. In addition, the players were instructed to consume at least 750 ml of fluid, avoid consumption of caffeinated products and to replicate their dietary consumption in the morning of testing days.
Statistical analyses
Physiological data were log-transformed for analysis to reduce bias arising from non-uniformity error. Data were analysed for practical significance using magnitude-based inferences.26 Qualitative analyses were conducted using modified statistical spreadsheets.27 A qualitative approach was used because traditional statistical approaches seldom indicate the magnitude of an effect, which conveys important information relevant to athletic performance. Between-trial standardised differences or effect sizes (ES±90% confidence limits; likelihood of positive/trivial/negative effect(%)) in core body temperature, sprint performance times and subjective ratings of recovery were calculated using appropriate between-subject SDs.28 Magnitudes of the standardised effects were interpreted using thresholds of 0.2, 0.6 and 1.2 for small, moderate and large ES, respectively, and were calculated at each time point.26 Standardised effects of between −0.19 and 0.19 were termed trivial. Quantitative chances of higher or lower differences were evaluated qualitatively as follows: <1%, almost certainly not; 1–5%, very unlikely; 5–25%, unlikely; 25–75%, possible; 75–95%, likely; 95–99%, very likely; >99%, almost certain. The effect was deemed ‘clear’ if its CI did not overlap the thresholds for small positive and negative effects.26 Magnitudes of correlations were interpreted using thresholds of 0.1, 0.3, 0.5 and 0.7 for small, moderate, large and very large correlations, respectively.27
Results
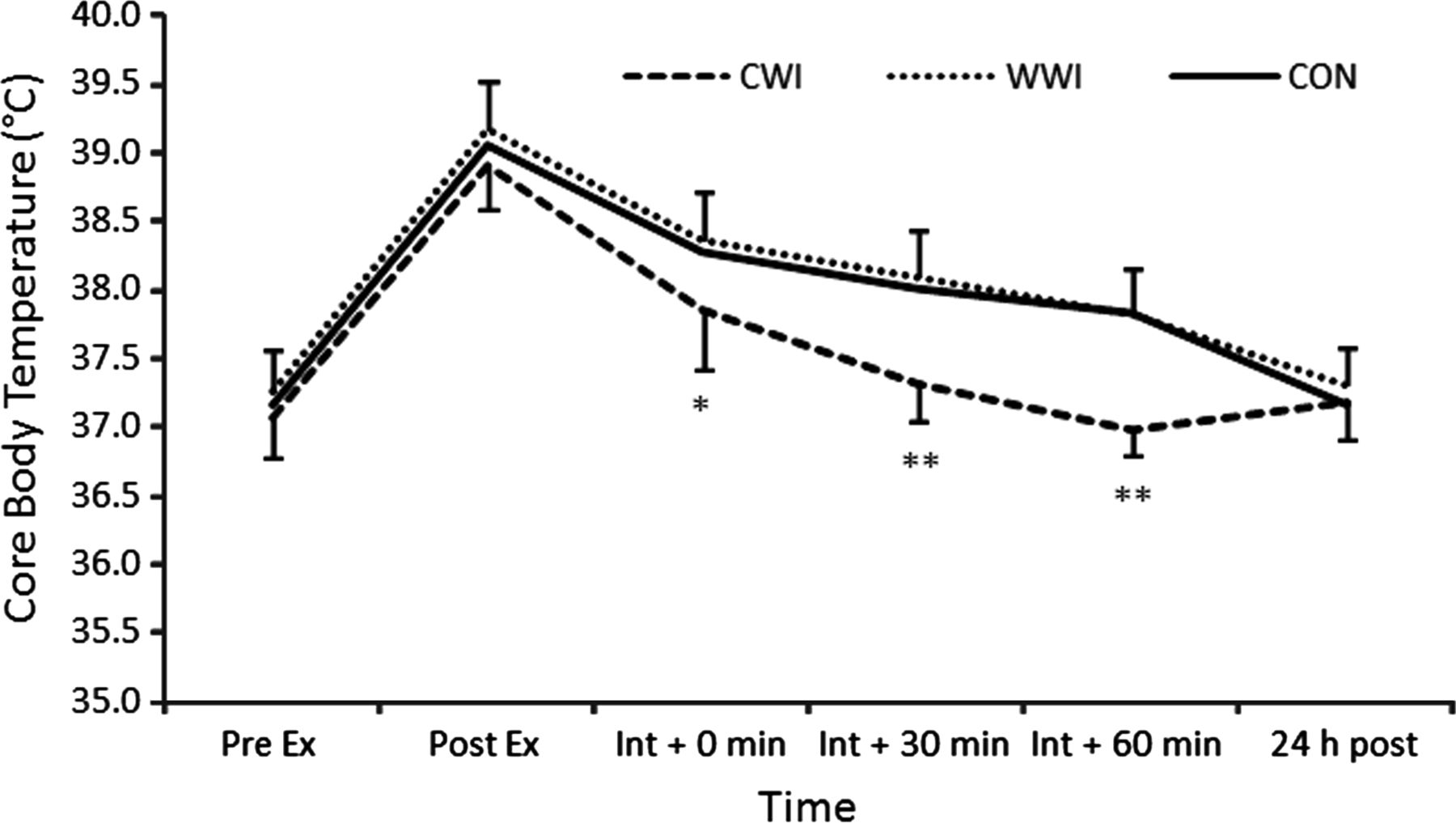
All players completed the experimental protocol. Core body temperature data are presented in figure 1 and demonstrate that the CWI protocol produced sizeable decreases in body temperature compared to the WWI and CON interventions (ES ranging from 1.05 to 3.21) at all postimmersion time points, except for 24 h. Core body temperature continued to decrease after the conclusion of the 15 min immersion, with the lowest postexercise temperature observed in the CWI intervention 60 min after exiting the water bath. The temperature at 60 min post the CWI intervention represented a return to pre-exercise values (pre 37.07±0.30 vs 60 min post 36.97±0.17; p > 0.05). There was no difference between core body temperature in the WWI and CON intervention at any time point (p>0.05).
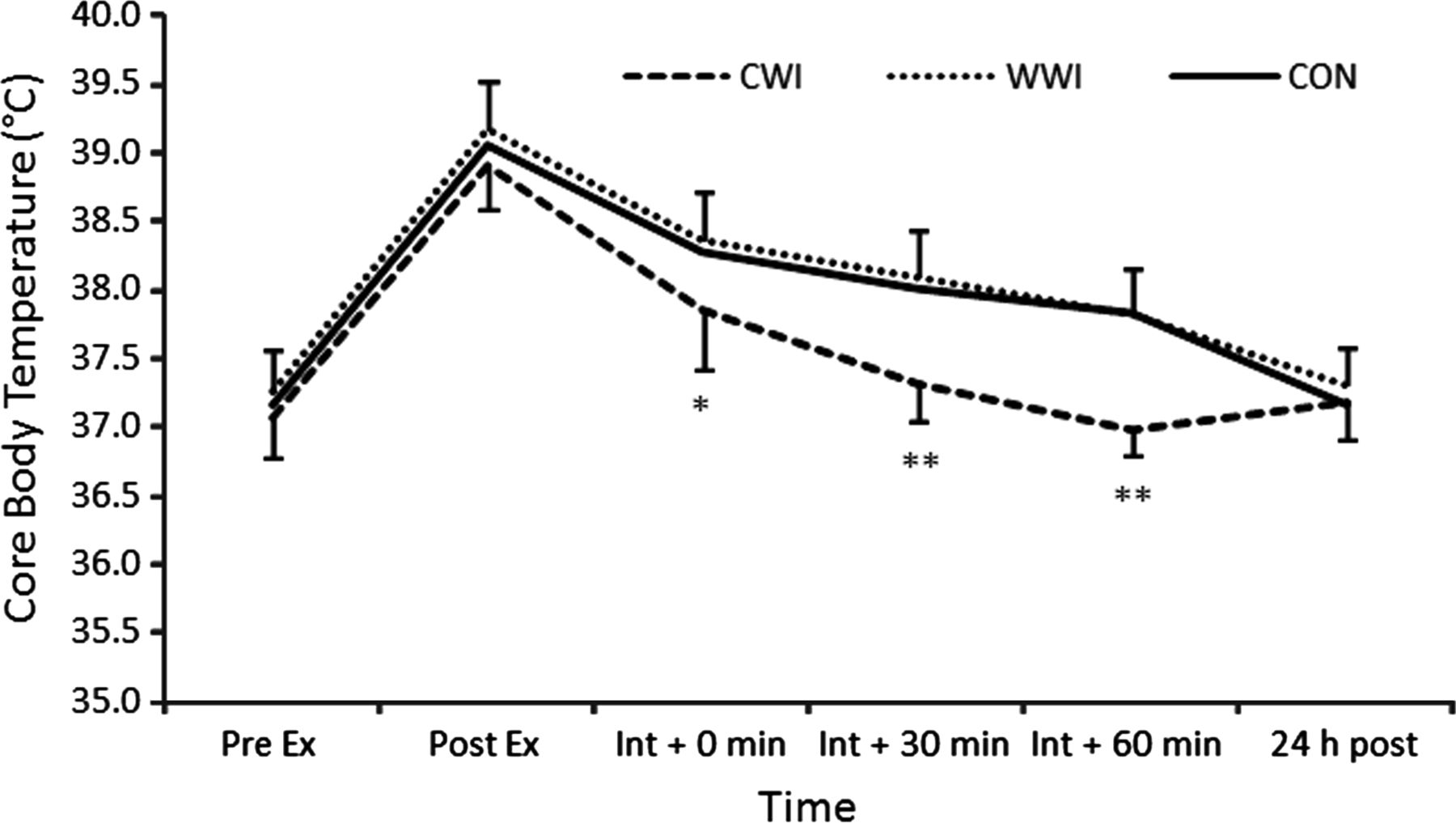
Temporal profile of core body temperature pre-exercise and postexercise and recovery interventions. CON, passive control recovery intervention; CWI, 15 min cold-water immersion; Ex, exercise; Int, intervention; WWI, 15 min warm-water immersion. * CWI significantly lower than WWI and CON p<0.05, ** CWI significantly lower than WWI and CON p <0.01. Error bars represent SDs.
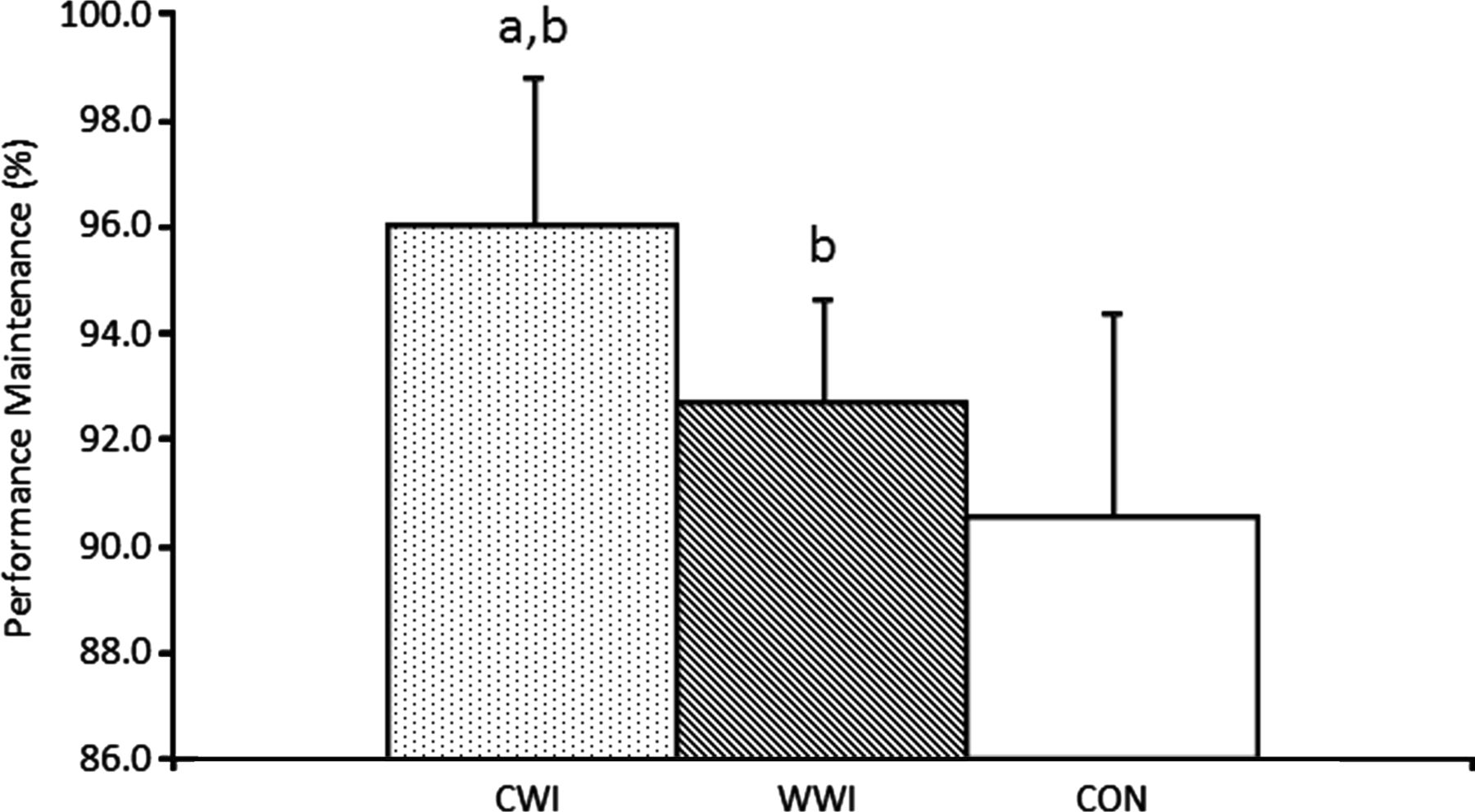
Data from the subjective ratings of the three interventions showed that both the CWI (ES 0.49±0.68; 76/19/5%) and WWI (ES 0.61±0.68; 85/12/3%) were preferred over the CON intervention by the players. With respect to repeated sprint performance 24 h after the intervention, there was a clear trend for initial sprint speed to be faster following the WWI intervention compared with the CON intervention (ES 0.48±0.68; 76/19/5%). The fifth sprints were substantially faster following the CWI intervention compared to the WWI (ES 1.06±0.68; 98/2/0%) and CON (ES 1.11±0.68; 99/1/0%) interventions. As a result, the percentage performance maintenance (see Methods section) was substantially greater following the CWI intervention compared with the WWI (ES 1.04±0.84; 95/4/1%) and CON (ES 1.44±0.84; 99/1/0%) interventions (figure 2). There was also a clear benefit, in terms of performance maintenance, of the WWI over the CON intervention (ES 0.72±0.84; 86/10/4%).

Performance maintenance during 5×40 m sprints 24 h after the recovery interventions. a, substantially greater than WWI; b, substantially greater than CON; CON: passive control recovery intervention; CWI: 15 min cold-water immersion, WWI: 15 min warm-water immersion. Error bars represent SDs.
When the correlation between performance maintenance and the percentage decrease in core body temperature was calculated, a large linear relationship (r=0.6948; p=0.0121) was found (figure 3A). Interestingly, a large linear correlation (r=0.5886; p=0.0441) was also found between the subjective player ratings of the recovery interventions and performance maintenance (figure 3B). When a combined index of player perception and body temperature decrease (see Methods) was plotted against subsequent sprint performance, a very large linear relationship was apparent (r=0.7743; p=0.0031; figure 3C).

{kind=link}
{kind=link}
{kind=link}
Correlations between physiological, subjective and combined indices and subsequent sprint performance. (A) Plot of percentage decrease in core body temperature against performance maintenance in repeated 5×40 m sprints, (B) plot of subjective rating of recovery intervention against performance maintenance in repeated 5×40 m sprints, (C) plot of a combined index of decrease in core body temperature and a subjective rating of recovery intervention against performance maintenance in repeated 5×40 m sprints. A.U., arbitrary units; CON, passive control intervention; CWI, cold water-immersion intervention; WWI, warm-water immersion intervention.
Discussion
We report here that the psychological perception of recovery, combined with the measured decrease in core body temperature as a result of CWI in well-trained rugby union players following an intense conditioning session, was strongly related to ‘training recovery’ as assessed by subsequent performance in a repeated 40 m sprint protocol. Three important points are raised here in an attempt to address issues that have previously been highlighted in studies of recovery.1 First, the participants were well trained, as it is intuitive that untrained or recreationally trained participants will have markedly different physiological and psychological responses to novel exercise protocols in terms of coping with aspects of fatigue and muscle damage. Second, the protocol used to induce fatigue and muscle damage was dynamic and sport-specific, without the predominance of eccentric contractions commonly used to assess functional, physiological and subjective perceptions of recovery. Third, a reliable and ecologically valid performance measure was used to assess recovery rather than biochemical markers, as improvement in these markers are of little practical importance to athletes if performance itself is not improved. In addition, the participants were all male as variable responses to CWI protocols may be due to a suggested gender difference.19 In fact, two prior reports that have found no performance benefit when utilising CWI have included only female participants.13 ,14
Despite the widespread use of CWI as a recovery strategy in athletes the physiological rationale behind its use has been questioned and performance benefits have not been consistently demonstrated.4 ,18 CWI is well known to rapidly decrease body temperature and this effect is prolonged after immersion is discontinued.20 ,29–31 Thus, our physiological data are in accordance with the reported literature. In addition to acutely reducing body temperature, mechanisms suggested to enhance recovery as a result of CWI include: a reduction of oedema formation;5 ,32 minimising inflammation;8 ,33 stabilising creatine kinase activity;34 accelerating parasympathetic activation35 and altering peripheral vasoconstriction and limb blood flow.20 ,30
The study by Vaile et al20 that demonstrated a decrease in limb flow, resulting from 15 min CWI, also reported a negative correlation (r=(−0.70) between the ensuing decrease in rectal temperature and performance in a 35 -min cycling performance test that culminated in a 15 -min time trial. In our trial, a positive correlation (r=0.6948) was observed between the percentage decrease in core body temperature and subsequent repeated sprint performance. The discrepancy in these results could be explained by a number of factors. First, the performance measure was performed 40 min after the CWI in the study by Vaile et al,20 at a time point where rectal temperature was below baseline levels; whereas in our trial, the performance test was performed the following day when core body temperature had returned to baseline levels. The nature of the performance test and the magnitude of the temperature decrease induced by the CWI (Vaile et al20: 0.5–3.5°C; current trial 0.6–1.9°C) also differentiate the two studies. These data led Vaile et al20 to suggest a cooling threshold below which performance decrements were likely, and it is possible that in the current study this threshold was either not exceeded, or was of lesser importance when exercise performance is assessed 24 h after immersion when core body temperature had returned to normal. It is noteworthy that a core temperature reduction of approximately 0.5°C has been suggested to be required to elicit improvements in performance.21 ,22
It is important to distinguish the effects of CWI on ‘training recovery’ from the possible acute fatigue-attenuating benefits of precooling on exercise performance.20 ,21 ,36 Further, it is necessary when prescribing CWI to be cognizant of the temperature and duration of immersion, the proportion of the body immersed, the duration of effects, the recovery interval and the nature of subsequent exercise given that reduced muscle temperature will affect muscle contractile properties and slow nerve conduction velocity.37 ,38 It is apparent that different CWI protocols will have distinct physiological effects, and differential performance effects have been reported following CWI and ice-water immersion.22 Our water immersion protocol may be regarded as cool (14°C) and thus have different effects to ‘cold’ protocols (∼10°C) reported in the literature.9 ,11 ,13 ,39 We also acknowledge that the timing of the application of CWI will likely influence the practical outcomes and our data suggest that performing the immersive protocol soon after exercise (5 min) may be worthwhile if practicable.
When looking at CWI as a strategy for ‘training recovery’, researchers have shown improved performance in protocols designed to simulate the demands of rugby matches,11 competitive cycling,6 netball matches39 and field hockey matches.9 CWI has also been demonstrated to improve run time to fatigue,40 return of function in dynamic power and isometric force5 and repeated running efforts.9 ,41 These observed positive effects of CWI are clearly multifaceted. The hydrostatic pressure applied during water immersion has been reported to displace fluids from the periphery to the central cavity resulting in a reduction in peripheral resistance and increase central blood volume23 and decrease inflammatory responses.40 ,41 However, the positive effects of CWI on subsequent performance cannot be solely attributed to hydrostatic pressure as researchers have demonstrated a positive effect of CWI over thermoneutral water immersion6 ,33. Indeed, CWI has been reported to have a long-lasting analgesic effect4 ,23 and reduce microvascular blood flow to muscle tissue, which should reduce oedema, the induction of inflammatory events and subsequent secondary damage.29 We acknowledge, however, that beneficial effects of CWI are not consistently reported12–14 ,16 ,17 and could potentially inhibit nerve conduction37 so the application of this intervention requires careful consideration.
The range of physiological effects of CWI likely contributes to the individual variability in the ‘training recovery’ response has been reported.42 We noted that differences in the maintenance of performance in repeated 40 m sprints were related to the magnitude of decrease in core body temperature (r=0.6948). Interestingly, one study that showed negative effects of CWI on Wingate performance,17 reported an increase (rather than a decrease) in tympanic core temperature as a result of seated CWI. Another study that reported a negative effect of CWI on repeated sprints, performed in young male rugby players, noted that all seven participants reported a negative perception of the recovery intervention.15 This led us to speculate that the psychological perception of the recovery intervention was related to its effectiveness. The majority of studies reporting a performance benefit of CWI also report an improved subjection perception of recovery5 ,7 ,9 ,33 ,39 ,41 ,43 and a recent study of elite team-sport athletes demonstrated that CWI was a component of all postmatch recovery practices that were associated with significantly enhanced perceived recovery.44 Further, Stanley et al2 reported that, even though there were no clear positive performance effects of CWI in their study of well-trained cyclists, the improvements in a 10-point psychophysiological recovery questionnaire led them to support its use based on the beneficial effects on perceived recovery.
Here we report that the perception of the effectiveness of a CWI recovery intervention was correlated with subsequent performance (r=0.5886). This correlation is of similar magnitude to the correlation observed between performance and our physiological measure (0.6948).26 It is known that psychosocial and mental stress can impact physiological processes45 and that a subject's belief of the efficacy on an intervention can influence subsequent responses.25 Further, previous research has reported that perceived recovery is related to subsequent performance24 and that psychometric measures can be more sensitive than physiological markers in determining the recovery state of athletes.46 ,47 From a psychophysical perspective, the performance enhancing effect of the placebo effect has been linked to dopamine release from the nucleus accumbens, a central component of the brain reward system48, and it is known that the expectation of an analgesic effect can trigger endogenous opioid systems.49 ,50
Thus, we suggest a potential new framework for assessing recovery strategies based on the data from the current study that assimilates both a positive perception of the recovery intervention, and addresses appropriate physiological mechanisms. This paradigm is based on our observation that this integrated approach is associated to a greater extent (r=0.7743) than either index alone with actual performance outcomes. Therefore, such an approach might be implemented to positively influence training recovery and subsequent performance by incorporating positive reinforcement of recovery strategies and recovery-specific education.
What are the new findings?
-
The magnitude of the core body temperature decrease following cold-water immersion (CWI) was related to subsequent repeated sprint performance.
-
The subjective perception of recovery following CWI is related to subsequent repeated sprint performance.
What is the possible impact?
-
An approach that elicits a positive perception of a recovery intervention and addresses appropriate physiological mechanisms can be used to positively influence training recovery and subsequent performance.
Acknowledgments
We wish to acknowledge the contribution of the willing participants and Dr H-C Holmberg and Dr Kim Hébert-Losier for manuscript comments.
References
Footnotes
-
Contributors CJC provided substantial contributions to conception and design, acquisition of data, article or revision and final approval of the version to be published and takes responsibility for the integrity of the work as a whole. CMB provided substantial contributions to the interpretation of data, drafting of the article and the final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Imperial College Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Correction notice This article has been corrected since it was published Online First. The ethics approval section has been corrected from Bath University to Imperial College.
-
▸ References to this paper are available online at http://bjsm.bmj.com