Article Text

Abstract
Background In this double-blind randomised controlled trial, we tested if leisure-time runners using shoes with less compliant midsoles have a higher running-related injury (RRI) risk.
Method We provided 247 runners with standard running shoes having either a soft study shoes (soft-SS) or a hard study shoes (hard-SS) midsole and followed them prospectively for 5 months regarding RRI. All information about sports practice and injuries was uploaded on a dedicated internet platform and checked for consistency and completeness. RRI was defined as any first-time pain sustained during or as a result of running practice and impeding normal running activity for at least 1 day. Cox proportional hazards regressions were used to identify RRI risk factors.
Result The type of study shoes used for running was not associated with RRIs (HR=0.92; 95% CI 0.57 to 1.48). The hard-SS had a 15% greater overall stiffness in the heel region. The two study groups were similar regarding personal and sports participation characteristics, except for years of running experience, which was higher (p<0.05) in the hard-SS group. Global RRI incidence was 12.1 RRI/1000 h of running. No between-group differences were found regarding injury location, type, severity or category. Nevertheless, the adjusted regression model revealed positive associations with RRI risk for body mass index (HR=1.126; 95% CI 1.033 to 1.227), previous injury (HR=1.735; 95% CI 1.037 to 2.902) and mean session intensity (HR=1.396; 95% CI 1.040 to 1.874). Protective factors were previous regular running activity (HR=0.422; 95% CI 0.228 to 0.779) and weekly volume of other sports activities (HR=0.702; 95% CI 0.561 to 0.879).
Conclusions Midsole hardness of modern cushioned running shoes does not seem to influence RRI risk.
- Injury Prevention
- Running shoes
- Running
- Sporting injuries
Statistics from Altmetric.com
Introduction
Running is one of the most popular and accessible sporting activities. It has many positive health benefits and may contribute to the prevention of many inactivity-related chronic health problems.1 However, running activity also generates a non-trivial amount of running-related injuries (RRIs). The reported incidence of RRIs varies between 19% and 79%2 or 2.5 and 38 injuries per 1000 h of running.3 Most are overuse injuries and concern the lower limbs, with knee injuries alone reaching an incidence of up to 50% of all runners.2 Moreover, RRIs are considered to be one of the main reasons for dropping out of a training programme in novice runners.4
Many studies have focused on RRI risk factors, but the knowledge of specific injury determinants is still limited.2 Training characteristics are considered essential, since most overuse injuries are believed to be caused by training errors.3 On the other hand, footwear has received much attention in the scientific literature, triggered by various claims of the running shoe industry when promoting high-tech shoes which are supposed to protect from RRIs. The shock-absorbing qualities of a running shoe are put forward as being especially important, since they influence repetitive impact forces that could be responsible for microtrauma and overuse injuries. In vitro experiments on impact attenuation of running shoes have shown that more compliant shoes are characterised by a lower peak force, a longer time to peak and a greater deformation of the cushioning system compared to those produced by stiffer shoes.5 In vivo force plate measurements have revealed conflicting results regarding the effect of midsole hardness on peak impact force magnitude.5 ,6 However, more compliant cushioning consistently reduces the impact loading rate and tibial acceleration5 ,7 and might thus have a protective effect on RRIs.
Within a large-scale randomised controlled trial on some 1200 Air Force recruits, Withnall et al8 investigated if the use of shock-absorbing insoles would be beneficial in reducing lower limb injuries during basic training. Their results showed similar rates of injury, independent of whether shock-absorbing or non-shock-absorbing insoles were used. The extent to which these findings can be extrapolated to a population of runners using running shoes of different shock-absorbing characteristics remains to be analysed. Therefore, we set out to do a randomised controlled trial on two groups of leisure-time distance runners using running shoes of strictly similar design, except for their midsole hardness, and to investigate if the latter influences RRIs. Based on experiments which showed that compliant cushioning systems decrease the vertical loading rate and tibial acceleration, variables that are supposed to be related to RRI risk,7 we hypothesised that the participants provided with shoes with more compliant midsoles would have a lower RRI risk. A secondary aim was to determine other modifiable and non-modifiable risk factors for RRIs.
Material and methods
Participants and study design
Leisure-time distance runners were recruited for this double-blind randomised controlled trial via advertisements in local newspapers and on specialised internet sites. A total of 299 volunteers agreed for an initial visit to provide preliminary personal information. This sample size was deemed appropriate to test our main hypothesis based on the following assumptions: given a desired power of 0.8 and an α level of 0.05, to detect a significant difference for injury incidence between both groups, based on expected injury rates of 40% and 25% over a 5-month follow-up period, the number of participants required is 294. Stratified random allocation into one of two running shoe groups was performed based on the age, sex, body mass index (BMI) and recent regular running practice. The latter was evaluated with reference to the 12 months prior to the study, based on regular training (at least once a week) for more than 50% of the time. Thus, the participants with more than six cumulated months of regular running training were defined as regular runners. Additionally, we recorded running experience (years of regular practice) and previous injury to the lower back or lower limbs preventing the participant from normal running activity and sustained during the 12 months preceding the follow-up. Participants were briefed about the following study requirements: (1) to train on average at least once a week, (2) to report systematically training data pertaining to running and all other sports at least once a week, (3) to report systematically any injury sustained during the follow-up period, (4) to use the provided study shoes for the majority of running sessions but not for other sporting activities and (5) not to replace the shoe insole with another (orthopaedic) insole. Healthy (uninjured) volunteers above 18 years were eligible for the study, regardless of the running fitness level. All participants received a full description of the study objectives and protocol, and provided written informed consent for participation at the moment of registration. The study protocol and procedures had previously been approved by the National Ethics Committee for Research (ref.201201/02).
Study shoes characteristics
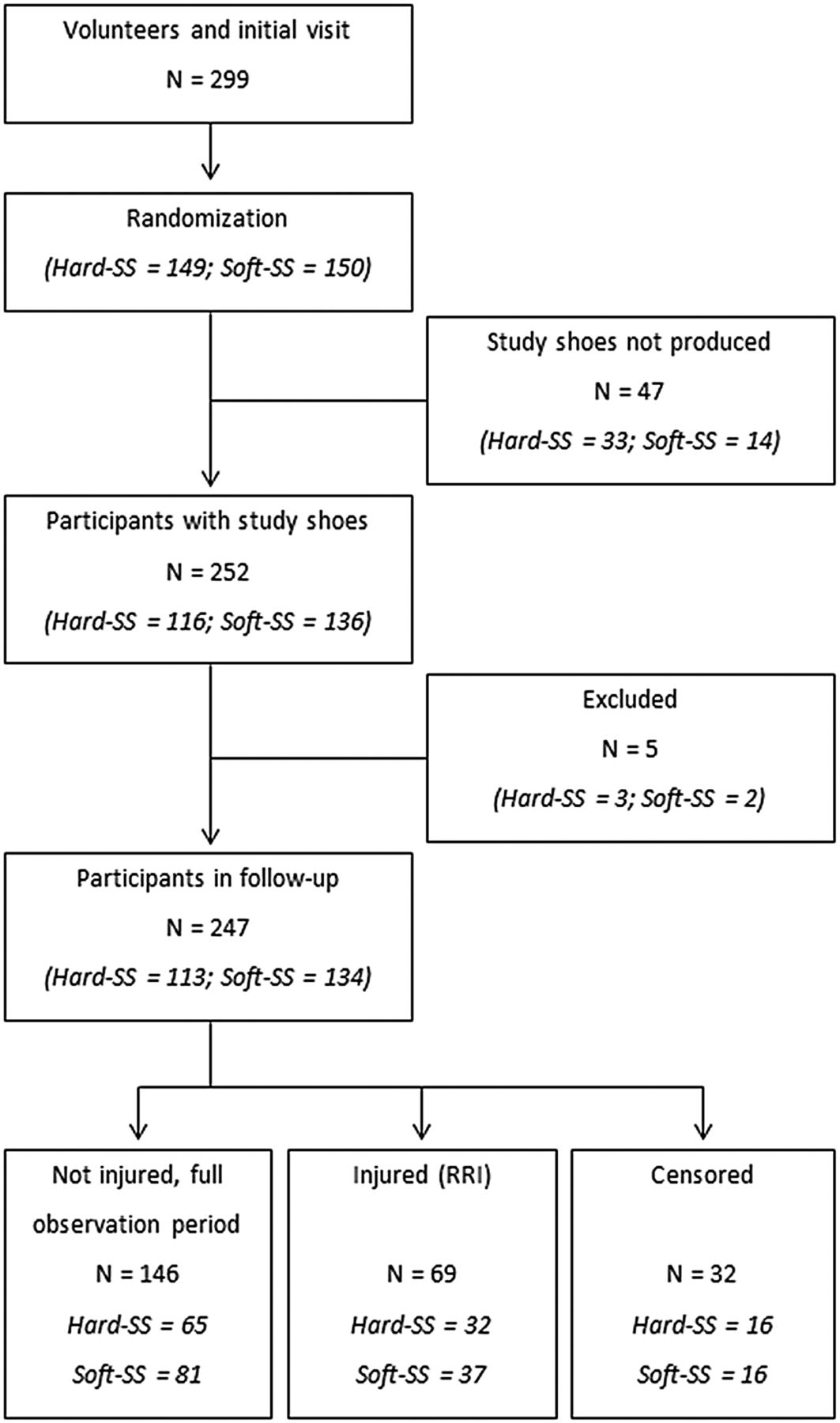
For the specific purpose of this trial, anonymised running shoes were provided by a renowned sport equipment manufacturer. The study shoes were derived from an existing model and had a heel-to-toe drop of 12 mm. They came in two versions, one with a more compliant midsole, termed soft study shoes (soft-SS), and one with a stiffer midsole, termed hard study shoes (hard-SS). Apart from midsole hardness, the two shoe versions were strictly identical. Before their use, a subset of each type was characterised regarding midsole hardness using an Asker-C durometer (average value of 3 independent measures/shoe). Furthermore, a standard impact test (ASTM standard F1976-06) was performed on the heel region of another subset to assess their impact attenuation properties.9 Each shoe version was characterised by the linear equivalent stiffness, calculated from the force-displacement curve obtained from these impact tests on the shoe sole.5 Owing to unforeseen production constraints, some volunteers could not be provided with the study shoes as planned, reducing the final number of distributed pairs to 252 (cf. figure 1). Each shoe pair was coded by a coworker not involved in the study, such that neither the participants nor the researchers in charge of the trial knew what shoe version a particular runner was using.
{kind=link}
Flow chart of volunteers and study participants. SS, study shoes; RRI, running-related injury.
Data collection during follow-up
Participants were asked to upload all information pertaining to sports participation and injuries on a dedicated internet-based platform (TIPPS, Training and Injury Prevention Platform for Sports (TIPPS)) using personal access codes.10 Data were rendered anonymous during the extraction process before the statistical analyses. Participants were instructed to upload all running sessions and any other sporting activity undertaken during the follow-up period, specifying the context, type of activity, volume, subjectively perceived intensity and whether the participant had experienced any pain during the session forcing him/her to reduce volume or intensity or to interrupt the practice. For running, additional required information was the distance covered and shoe pair used. Subjectively perceived intensity was assessed using the Borg CR-10 Scale (arbitrary unit).11
All adverse events preventing normal running activity were uploaded by the participants via a standardised questionnaire on their TIPPS account. A new injury could be declared either via the sport practice session interface (see above) or a dedicated injury declaration page. An RRI was defined as physical pain or a complaint sustained during or as a result of running practice and impeding normal running activity for at least 1 day (time-loss definition).12 ,13 RRIs were recorded in accordance with published recommendations for sports injury surveillance studies, 14–16 considering the runner as the unit of analysis.
Data quality control
Uploaded data underwent automatic validity and consistency checks by the TIPPS system. Individual email reminders were sent to participants if they had not provided any data over the previous week. Personal phone calls were made to participants who did not react to the email reminders or if they reported inconsistent or incomplete information in either the training log or on the injury form. Information regarding injuries was systematically checked by one of the investigators for completeness and coherence. Participants who did not comply with data reporting were contacted by one of the investigators to ensure that RRI was not the reason for dropping out.
Statistics
The shoe properties and the study group characteristics were compared using Student t tests for independent samples after checking the data for normal distribution. RRI incidence was calculated as the number of RRIs/1000 h of running activity. The two groups were tested for differences regarding the main injury characteristics using a χ2 test. Average sport participation characteristics were calculated for each participant over his/her specific period of observation, that is, from the shoe delivery date until the first RRI (event), the end of the observation period (shoe return date) or the right censure (drop out). A participant was considered a dropout when no data were uploaded in the system for more than 2 weeks despite the automatic reminders sent by the system and the direct contacts from the research team. A Cox proportional hazards regression was used to identify if time to RRI varied across individuals using soft-SS and hard-SS as well as other variables characterising the runners and their sports participation patterns. Exposure volume to running activities (hours) during the period of interest was used as the outcome variable. First, an unadjusted analysis was performed, entering each variable separately into the Cox regression model. For the final adjusted model (forward likelihood ratio (LR) method), all variables with a p value below 0.250 were introduced in the model. Additionally, the variables used for stratification of the sample (age, sex, BMI and recent regular running practice) were controlled for by introducing them in a first block (enter method). Forward LR was chosen because of the low number of events (69 RRIs) observed and the high number of potential predictors (n=12) identified with the unadjusted model. The proportional hazard assumption was verified for all explanatory variables. Results are presented as mean±SD. Significance was accepted for p<0.05.
Results
The shock absorption properties of the study shoes are presented in table 1. The Asker C values show that the midsole hardness was higher (13.1%, p<0.001) for the hard-SS compared to the soft-SS. Similarly, the standard impact test revealed a 14.9% greater overall stiffness of the hard-SS (p<0.001).
Comparison of the two types of study shoes regarding shock absorption properties
From the 252 participants in the intervention, five were excluded from the analysis (3 from the hard-SS group and 2 from the soft-SS group) because they did not use their study shoes or got injured before receiving them. Eventually, of the 299 volunteers present at the initial visit, 52 were not included in the study (cf. figure 1). None of their baseline characteristics were significantly different from those of the 247 participants in the final analysis. Table 2 presents separate results for the two study groups, which were similar except for running experience.
Sport participation pattern and participants’ characteristics according to their study shoes (hard midsole vs soft midsole)
During the follow-up, 32 participants stopped reporting their training sessions for other reasons than RRI before the scheduled date of shoe return. Sixty-nine participants (27.9%) declared a first-time RRI, the overall incidence being 12.1 RRIs/1000 h of running. The specific period of interest ranged from 1 week for participants who got injured at the beginning of the observation to 22 weeks for those who did not get injured (mean 12.9±5.8 weeks). Table 3 presents the main characteristics of the reported RRIs. Sixty injuries (87%) concerned the lower limbs, with a majority of knee injuries (24.9%), and muscles and tendons were the most affected body tissue. Injury profile was not influenced by the type of shoe.
Characteristics of reported running-related injuries (RRIs, n=69)
Age, BMI, previous injury and recent regular running practice were or tended to be independently associated with RRIs as revealed by the unadjusted Cox proportional hazard regression analysis (table 4). Some aspects related to sport participation were or tended to be associated with RRI occurrence: proportion of running sessions with the study shoes and mean subjective intensity (risk factors), as well as average volume of other sports practiced, running frequency, weekly running volume and weekly distance (protective factors). Contrary to expectations, the midsole hardness of the study shoes was not associated with RRIs (HR=0.92; 95% CI 0.573 to 1.478)). The adjusted model revealed that BMI (p=0.007) and previous injury (p=0.036) were risk factors, and that recent regular running practice was a protective factor (p=0.006). Moreover, the sport participation pattern also had an impact on RRI occurrence, with mean subjective intensity being a risk factor (p=0.026) and weekly volume of other sports being protective (p=0.002). Additionally, to test if body mass (kg) (coded ‘high’ and ‘low’, based on the median) could modify the association between midsole hardness and RRI risk, its interaction with shoe type was tested using the final regression model. However, the results were not significant (HR=0.94; 95% CI=0.354 to 2.495).
Results of the unadjusted and adjusted (n=242) Cox regression models for the variables tested
Discussion
To the authors’ knowledge, this is the first double-blind randomised controlled trial on the effect of running shoe midsole hardness on RRIs in leisure-time distance runners. Previous investigations have analysed the influence of shock-absorbing footwear on biomechanical aspects in running and could only speculate on the possible effects on RRIs.5–7 The present results fill an important knowledge gap, demonstrating that, within the conditions of this study, running shoe midsole hardness influences neither the overall risk nor the profile of RRIs. This is in line with earlier findings that the use of shock-absorbing insoles did not modify lower limb injury rate in military recruits during basic training.8
Our participants used commercially available standard running shoes with an overall stiffness that was probably located within the lower 10–15% range of commonly available models, according to data by Shorten and Mientjes5 based on over 200 shoe types available between 2008 and 2010. We had maximised the difference between the midsole hardness of the study shoes within the technical limitations of production. This resulted in a 15% difference of the shock-absorbing properties determined by the standard impact test (table 1). Considering that all other components, geometries and structures were strictly similar between the two shoe types, our data suggest that midsole hardness is not a characteristic that modulates RRIs. In addition, body mass was not an effect-measure modifier on the association between midsole usage and risk of RRIs, meaning that midsole hardness does not change RRI risk, independent of whether a runner is heavy or light. Therefore, our results do not support the common argument from the running shoe industry that runners with higher body mass should be recommended shoes with greater shock-absorption characteristics.
One explanation as to why the shock-absorbing quality of footwear generally does not influence RRIs is that individuals are likely to adapt their running style to avoid excessive impact transients of the vertical ground reaction force. The most dramatic illustration of this phenomenon comes from comparisons of habitually shod and habitually barefoot endurance runners. The latter tend to adopt a supposedly more protective forefoot strike pattern, which has been associated with a lower magnitude and rate of impact transients, contrary to the former who predominantly use a rearfoot strike generating greater collision forces.17 Less striking but nevertheless interesting observations18 revealed that midsole hardness had an acute effect on running kinematics during the stance phase, especially in the sagittal plane. Biomechanical adaptations have also been observed in runners who gradually wore out their running shoes and modified their pattern so as to maintain constant external loads.19 Although not analysed here, it is possible that adaptations of running style cancelled out the differences in shock-absorbing characteristics of the shoes used by our participants and thus the RRI risk. Alternatively, the difference between our study shoe models may have been too small to induce differences in RRIs.
Some participant-related features were associated with RRIs and confirm prior research. Runners who had sustained a previous injury showed a higher RRI risk. Our HR of 1.735 compares well with the results reported by Hootman et al20 for previous lower extremity injuries in recreationally active men (HR=1.93) and women (HR=1.73). In a systematic review, van Gent et al2 reported ORs of 1.7 to 7.6, the magnitude of the effect depending on the population investigated and the definition of previous injury. Several authors have suggested that a history of running practice influences RRIs.13 ,21–23 Here we described the running history of our participants in two different ways. Long-term running experience (years of running) was not associated with RRIs, but recent (past 12 months) regular running practice had a protective effect (HR=0.422). This is consistent with the findings that previous participation in sport activities with axial loading was a strong protector against RRIs.24 Furthermore, these results suggest that regular runners are more skilled in ‘listening to their body’,3 and that individuals newly engaging in running are more prone to training errors. Finally, BMI was a risk factor, possibly as a result of greater forces acting on the musculoskeletal system during running. Similar results have been reported in novice runners24 and recreationally active women.20
Our methodology provided ample opportunity to examine if sport participation patterns are related to RRIs, as recently recommended.3 Subjectively perceived intensity is one of the risk factors identified in our adjusted model (table 4), in accordance with prior results obtained with the same methodology in young elite athletes of different sport disciplines.25 Furthermore, participation in other sports next to running practice was protective. The beneficial effect of alternation between sporting activities has been previously reported26 and could be explained by additional benefits of other sports on health or the adaptation of the musculoskeletal system allowing one to cope better with the strain induced by running.
A limitation of this study is the relatively limited duration of follow-up and the resulting low number of events of interest (69 RRIs). Since this normally limits the number of predictors which are introduced in the final Cox regression model, the forward LR method was applied here. Our final model includes eight variables, which is slightly more than the general rule of thumb (10 outcome events per predictor variable) would allow. However, recent results showed that the latter may be relaxed27 and that the conclusion about our main hypothesis remains valid. Another consideration to keep in mind is the fact that, although significant, the difference in midsole hardness of the study shoes used here may have been too moderate to disclose an effect on RRI risk. Further research should therefore be directed towards comparing shoe models with more extreme shock-absorption characteristics, with particular focus on so-called ‘minimalistic’ shoes. An aspect we did not investigate and control for is the potential adaptations in running style caused by our shoe models. Future investigations could provide a better insight into the factors involved in RRIs by using biomechanical and clinical measures in combination with an epidemiological approach.
Conclusion
Our results suggest that midsole stiffness in standard cushioned running shoes does not modify the risk of RRIs in amateur runners. Injury in the previous 12 months, no prior regular running practice and a higher BMI were risk factors for RRIs. Running at subjective high intensities increases injury risk, while practicing other sports beside running is protective. Awareness about these modulators of RRI risk will make leisure-time running a safer sport and an attractive intervention to induce positive health benefits.
What are the new findings?
-
Within our study conditions, midsole hardness of modern cushioned shoes did not influence running-related injury (RRI) risk.
-
Body mass is not decisive for the selection of a pair of running shoes.
-
Previous injury is one of the factors that are most consistently associated with increased RRI risk.
-
Individuals are at a higher RRI risk if they have a greater body mass index, engage newly into running activity or train at high intensities.
How might it impact on clinical practice in the near future?
-
Shock-absorbing properties of running shoes are not critically related to running-related injuries (RRI) risk.
-
Individuals engaging newly in leisure-time running might be more prone to training errors and require appropriate counsel from certified trainers.
-
Leisure-time runners should be encouraged to include other sporting activities into their training plan.
Acknowledgments
The authors would like to thank Dr Stephen Senn for preparing the randomisation and Mr Joseph Ramesh for his precious assistance with data collection.
References
Footnotes
-
Contributors Substantial contribution to conception and design, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; approval of the submitted version to be published.
-
Funding The present study was financially supported by the National Research Fund, Luxembourg (AFR Laurent Malisoux: ref.1189878), and by Oxylane Research, France.
-
Competing interests None.
-
Ethics approval Comité National d'Ethique de la Recherche (CNER; ref.201201/02).
-
Provenance and peer review Not commissioned; externally peer reviewed.