Article Text

Abstract
Background Sedentary time is increasing in all societies and results in limited non-exercise physical activity (NEPA) of daily life. The importance of low NEPA for cardiovascular health and longevity is limited, especially in elderly.
Aim To examine the association between NEPA and cardiovascular health at baseline as well as the risk of a first cardiovascular disease (CVD) event and total mortality after 12.5 years.
Study design Cohort study.
Material and methods Every third 60-year-old man and woman in Stockholm County was invited to a health screening study; 4232 individuals participated (78% response rate). At baseline, NEPA and exercise habits were assessed from a self-administrated questionnaire and cardiovascular health was established through physical examinations and laboratory tests. The participants were followed for an average of 12.5 years for the assessment of CVD events and mortality.
Results At baseline, high NEPA was, regardless of regular exercise and compared with low NEPA, associated with more preferable waist circumference, high-density lipoprotein cholesterol and triglycerides in both sexes and with lower insulin, glucose and fibrinogen levels in men. Moreover, the occurrence of the metabolic syndrome was significantly lower in those with higher NEPA levels in non-exercising and regularly exercising individuals. Furthermore, reporting a high NEPA level, compared with low, was associated with a lower risk of a first CVD event (HR=0.73; 95% CI 0.57 to 0.94) and lower all-cause mortality (0.70; 0.53 to 0.98).
Conclusions A generally active daily life was, regardless of exercising regularly or not, associated with cardiovascular health and longevity in older adults.
- Cardiovascular epidemiology
- Health promotion through physical activity
Statistics from Altmetric.com
Introduction
The importance of regular exercise for health and longevity is evident,1 ,2 and at least 150 min/week of moderate–vigorous leisure-time physical activity (MVPA) is recommended for a healthy lifestyle. Meanwhile, prolonged sitting has recently been recognised to increase the risk for several common diseases and mortality, regardless of regular MVPA.3–5
Sedentary behaviour, leading to a lack of muscular contractions within the large muscle groups of the body, refers to activities equal to an energy expenditure of 1.0–1.5 METs such as lying down or sitting.6 Sedentary time mainly replace time spent in non-exercise physical activities (NEPAs) embedded into much of daily life, mainly performed with low intensity, but is poorly correlated with time spent in intentional exercise.7–9 One reason for this is that the proportion of time spent doing intentional exercise usually consists of only a fraction of the day, leaving a great deal of time for NEPA or sitting.
The most feasible approach to reduce sedentary time is to promote NEPAs. This is particularly important for older adults, as they tend to sit more compared to other age groups10 and spend a relatively greater proportion of the remaining day performing NEPA as they more often find it difficult to achieve the recommended exercise intensity levels.9–11 Previous cross-sectional studies have demonstrated negative associations between NEPA and cardiovascular health,12 ,13 cardiovascular disease (CVD) risk14–16 and all-cause mortality.17–19 However, the epidemiology as well as the underlying mechanisms are still incompletely understood. There is a need for further evidence of the beneficial effects of an active daily life on health and longevity in older adults. Therefore, in a population-based study of 60-year-old men and women, we examined the importance of NEPA for cardiovascular health in a cross-sectional study as well as for the risk of a CVD event and total mortality after 12.5 years.
Materials and methods
Study population
From August 1997 to March 1999, every third man and woman born between 1 July 1937 and 31 June 1938 and living in Stockholm County, Sweden, was invited to participate in a health screening study. Of the 5460 individuals invited, 4232 (2039 men, 2193 women; 78% response rate) agreed to participate and underwent physical examinations and laboratory tests and completed a self-administrated questionnaire. The ethics committee of the Karolinska Institutet approved the study.
NEPA index, exercise habits and lifestyle factors
A NEPA index was derived from the questionnaire at baseline. Participants were asked to report how frequently (‘never’, ‘occasionally’ or ‘frequently or regularly’) during the last 12-month period they performed 24 different activities typical for older adults of the Swedish and Scandinavian culture (see online supplementary appendix 1). Five of these activities predominantly promoted NEPA of daily living: ‘performing home repairs’, ‘cutting the lawn, hedge, etc’, ‘car maintenance’, ‘taking bicycle rides, skiing, ice-skating, going hunting or fishing’ and ‘gathering mushrooms or berries’. These activities are mainly elucidating the context in which physical activity (PA) is performed (as part of daily life) and is not referred to a specific intensity span. Regarding the other 19 activities, 12 could not clearly be defined as promoting daily activity or not, four activities were predominantly promoting sitting, two were mainly intentional exercise, and one asked for an exclusive activity not available for all study participants. For construction of the NEPA index, reporting ‘never’ was equal to one point, ‘occasionally’ to two points and ‘frequently or regularly’ to three points, thus resulting in a possible range of 5–15 points.
A reliability analysis revealed moderate internal consistency of the five single items (Cronbach’s=0.67). Seventy-one participants had internal missing observations for one of the five NEPAs; these were replaced by the estimated gender-specific series mean to obtain a full score and inclusion in the analysis. The score was subsequently divided into tertiles; low, moderate and high levels of NEPA. Since some of the NEPAs were more common in men than women, sex-specific tertiles were used to ensure that the NEPA index analyses elucidated differences in NEPA patterns and not gender differences (cut-off points were ≤8, 9–10, >10 points in women and ≤10, 11–12, >12 points in men).
To determine exercise habits, the participants were asked to report their PA level in leisure-time during the past year as either 1 ‘sedentary’ (light-intensity activity less than 2 h a week); 2 ‘light-intensity PA’ (≥2 h a week); 3 ‘regular moderate-intensity PA’ (at least 30 min, 1–2 times a week) or 4 ‘regular high-intensity PA’ (at least 30 min, ≥3 times a week; see online supplementary appendix 2). In line with current guidelines for health promotion and risk prevention recommending regular exercise (defined as PA on at least moderate intensity level), these were further dichotomised into regular exercise on at least moderate intensity (3 or 4 above) or not (1 or 2 above).
Lifestyle-related factors for potential confounding analysis were reported in the questionnaire and dichotomised: marital status (married/living together or not), education level (university degree or not), current smoking (yes or no), dietary intake of vegetables (high intake; one portion daily/almost daily or low intake; occasionally/never), general well-being (very/quiet good or not) and living conditions (apartment or house/townhouse). Regarding alcohol, consuming 4–6 bottles of strong beer, 2–3 bottles of wine or 0.35–0.75 L spirits weekly were considered as a high intake, while not reporting any of this was considered as a low intake. Self-rated financial status was based on a seven-degree scale ranging from ‘very bad’ to ‘excellent’ and scoring 1–4 was considered bad and 5–7 good. Heredity of high blood pressure (BP), dyslipidemia, diabetes mellitus or CVD was determined as self-reported presence of the condition, respectively, in either the individual's mother or father.
Individual risk factors and the metabolic syndrome
Waist circumference was measured with a tape measure in a standing position midway between the lower rib margin and the iliac crest. Systolic and diastolic BP was measured twice with an automatic device (HEM 71, Omron Healthcare, Illinois, USA) after 5 min of rest in a sitting position and the mean of the measurements was calculated. A venous blood sample was drawn from an antecubital vein after overnight fasting to determine levels of serum high-density lipoprotein (HDL) cholesterol, low-density lipoprotein cholesterol, total cholesterol, triglycerides, insulin, glucose and plasma fibrinogen. All blood samples were analysed continuously. The specified laboratory procedures have been described previously.20
Nine individual dichotomised risk factors were defined using conventional cut-off points between these risk factors and CVD risk (see table 2). Dichotomised risk factors were used in order to evaluate how the exposure coincides with and predicts the presence of an ‘unhealthy’ level of risk factors. Metabolic syndrome was classified using the criteria proposed by the American Heart Association and the National Heart, Lung and Blood Institute.21
CVD event and mortality surveillance
All participants were followed from the date of completion of the baseline investigation until the date of their death or until 31 December 2010. Incident cases of first-time CVD event (fatal or non-fatal myocardial infarction, angina pectoris or ischaemic stroke) and death from any cause were ascertained through regular examinations of the national cause of death registry and the national in-hospital registry. We could guarantee registration of first CVD events only, as care was taken to exclude participants with a history of CVD in the analysis.
Statistical analysis
Logistic regression models were used to assess the OR and 95% CI associated with higher tertiles of NEPA for each individual risk factor as well as for prevalence of metabolic syndrome at baseline. For the prospective analyses, Cox regression models were used to assess the HR and 95% CI between higher NEPA tertiles and the risk of a CVD event and mortality from any cause, respectively. Both the baseline and prospective analyses were tested for confounding by sex, marital status, education level, current smoking, regular exercise, dietary intake of vegetables, alcohol intake, self-rated financial status, living conditions and heredity. To identify possible confounding, univariate models were used for the different outcomes, respectively. The outcomes (the individual risk factors and metabolic syndrome at baseline, and CVD event and mortality of any cause after follow-up) were included one by one as the dependent variable and each confounder included together with the NEPA variable as independent variables. Confounders were regarded as significant and introduced into the main analysis if the 95% CI for the OR or HR did not include one. However, any that did not remain significant (under the same criterion) after the inclusion of the other significant confounders in the main analysis, were then excluded. As the cross-sectional outcomes of this study are commonly present in older adults, as well as that the incidence of the prospective outcomes are rather high, even small significant changes of the OR and HR, respectively, are regarded as clinically meaningful. Kaplan-Meier survival curves were plotted to examine differences in cumulative survival across the cross-tabulated variable of NEPA level and regular exercise.
Results
After exclusion of 205 individuals with reported myocardial infarction (n=110), heart failure (n=53) and stroke (n=60) and 66 individuals with missing data on two or more NEPAs, 1816 men and 2023 women remained to be included in the analysis.
Cross-sectional analysis
Table 1 shows the characteristics of the study population and different life-style variables by NEPA tertiles. In women and men, higher levels of NEPA were in general associated with more favourable life style profile. Cross-tabulation analysis revealed low association between the NEPA tertiles and the dichotomised exercise variable, γ=0.33 for women and γ=0.30 for men.
Characteristics of the study population (top) and commonly recognised favourable lifestyle factors in relation to sex-specific tertiles of non-exercise physical activity (NEPA) (bottom)
For the individual risk factors, regardless of regular exercise and other confounding factors, high reported NEPA level was significantly associated with more preferable profile of waist circumference, HDL cholesterol and triglycerides in women and men and also with insulin, glucose and fibrinogen in men (table 2).
OR (95% CI) for different NEPA levels in relation to being at risk for each dichotomised risk factor
Concerning metabolic syndrome, figure 1 shows the interaction effect between higher levels of NEPA and regular exercise, with the reference group set as low NEPA and no regular exercise. Participants with moderate or high NEPA levels but no regular exercise showed lower ORs than the reference group. Those exercising but with low NEPA showed a lower OR than for the reference group, though this was not significantly different from that of the non-exercisers with higher levels of NEPA. Exercisers with high NEPA levels had the lowest OR.
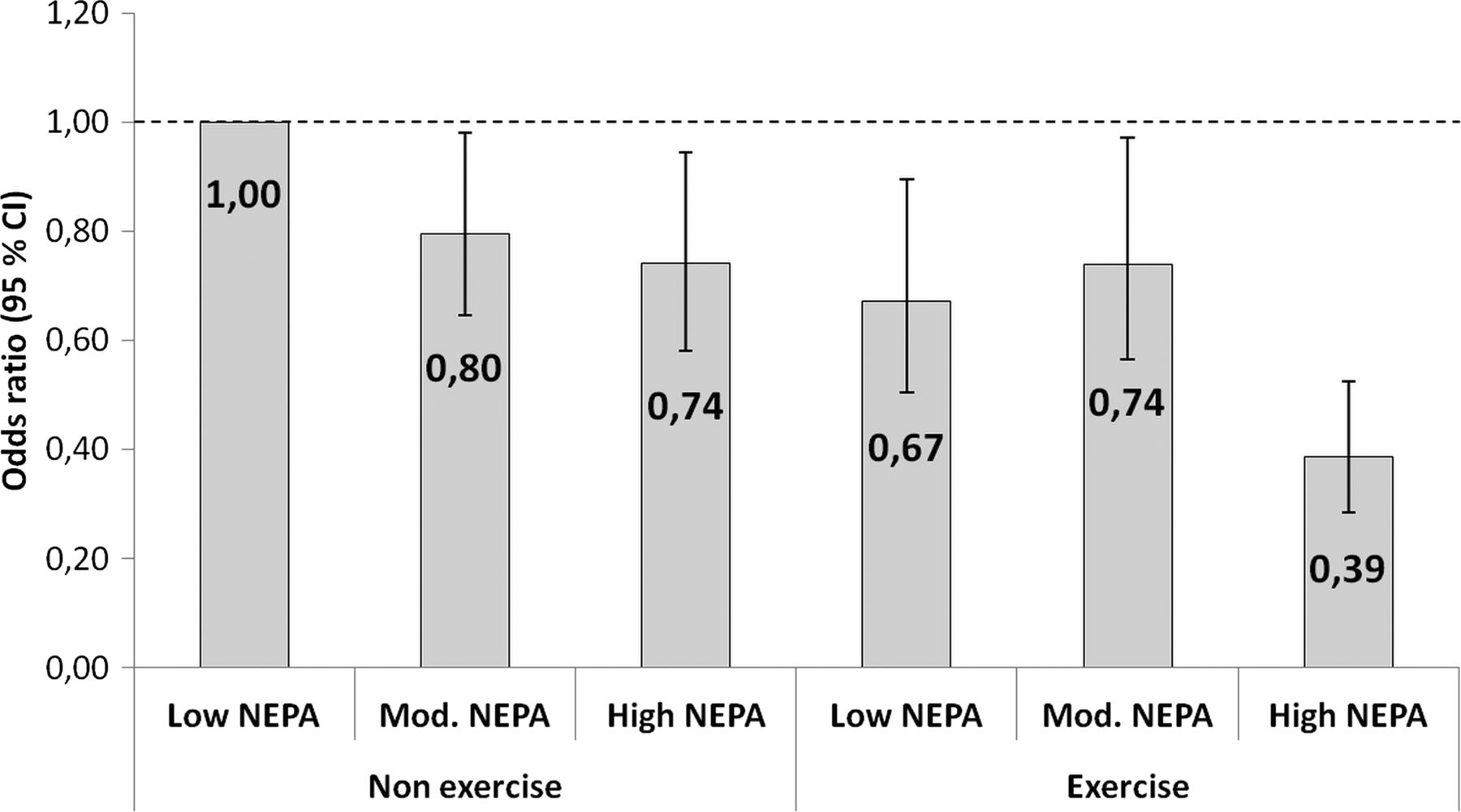
ORs for metabolic syndrome at baseline in relation to tertiles of non-exercise physical activity (NEPA) and exercise. 95% CIs were 0.65–0.98 for non-exercise and moderate NEPA, 0.58–0.95 for non-exercise and high NEPA, 0.50–0.89 for exercise and low NEPA, 0.56–0.97 for exercise and moderate NEPA, and 0.28–0.52 for exercise and high NEPA. The analysis was adjusted for sex, marital status, education level, smoking habits, dietary intake of vegetables, alcohol intake, self-rated financial status and living conditions. The dashed line is representing OR=1.
Prospective analysis
During the 12.5 years of follow-up, 476 participants experienced a fatal or non-fatal first-time CVD event and 383 deaths were registered from all causes. Figure 2 shows the adjusted HR for higher levels of NEPA at baseline compared with low in relation to first-time CVD event (figure 2A) and all-cause mortality (figure 2B). High NEPA level was associated with a 27% lower HR for CVD event compared with low NEPA and with 30% lower HR for all-cause mortality. In further sensitivity analysis, we excluded cases and deaths, respectively, occurring in the first, second or third year of follow-up, with no significant change of the results.
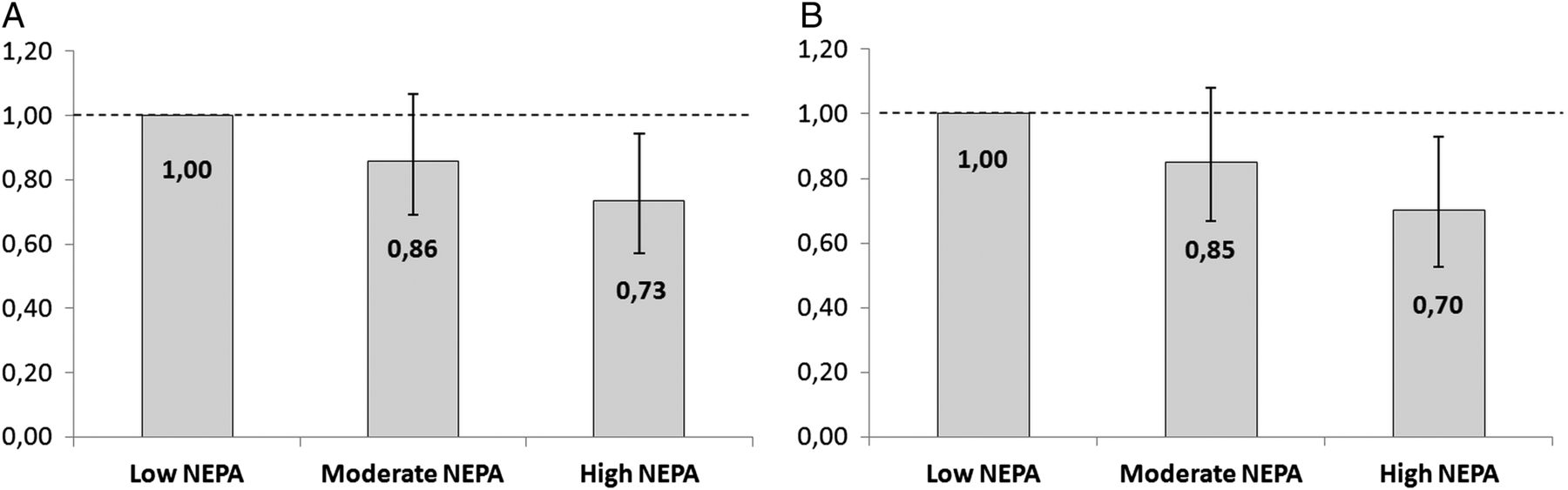
HR for higher levels of non-exercise physical activity (NEPA) compared with low levels for a first cardiovascular disease (CVD) event (A) and all-cause mortality (B). For CVD event, 95% CIs were 0.69–1.07 for moderate NEPA and 0.57–0.94 for high NEPA. For all-cause mortality, 95% CIs were 0.67–1.08 for moderate NEPA and 0.53–0.93 for high NEPA. All analyses were adjusted for sex, marital status, education level, smoking habits, regular exercise, dietary intake of vegetables, alcohol intake, self-rated financial status, living conditions and a family history of CVD events. The dashed line is representing OR=1.
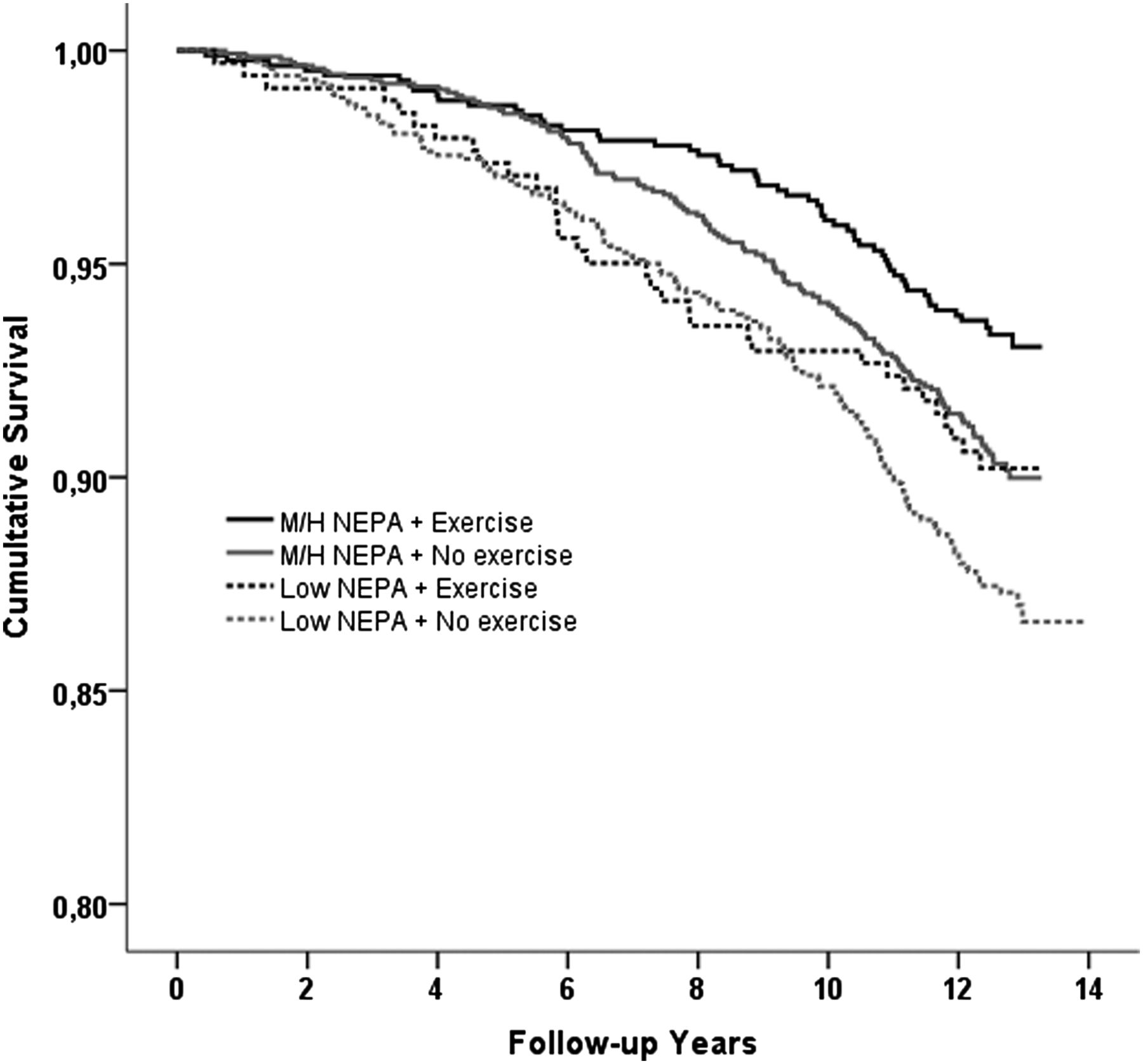
The cumulative survival across the cross-tabulated variable of NEPA level (low vs moderate/high) and regular exercise is presented in figure 3. There was a significant difference in survival probability across the different levels of exercise and NEPA (log-rank χ2=20.81, df=3, p<0.0001), with the lowest probability seen for those reporting no regular exercise and low NEPA.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves for all-cause mortality across the cross-tabulated variable of non-exercise physical activity (NEPA) level (low vs moderate/high) and regular exercise. Log-rank χ2=20.81, df=3, p<0.0001.
Discussion
The present study in a representative sample of 60-year-old Swedish men and women revealed that a generally active daily life, regardless of regular exercise habits, reduced the risk of a first time CVD event with 27% and all-cause mortality with 30%, in comparison to low daily activity, during a 12.5-year follow-up. Sensitivity analysis revealed that the results were not changed after exclusion of cases and deaths, respectively, occurring in the first 3 years, minimising potential reverse causality issues. At baseline, the association with metabolic syndrome was significantly lower for those with higher NEPA levels in the non-exercising and the regularly exercising group. High NEPA was also associated with more preferable profile of waist circumference, HDL and triglycerides in both sexes and insulin, glucose and fibrinogen in men.
The results from the cross-sectional analysis are in concordance with two previous studies both of which evaluated NEPA objectively with an accelerometer.12 ,13 Interestingly, neither the present study nor the two studies found any associations between NEPA and systolic or diastolic BP. This might reflect that while NEPA has important metabolic effects, a higher intensity is needed to have effect on BP. Further, two experimental studies indicated adverse metabolic health effects after reducing NEPA in exercising and non-exercising young men and women.22 ,23 Promising findings from recent experimental trials on the acute negative metabolic effects of prolonged sitting have shown benefits of intermittent light intensity PA, which further strengthen the findings of the present study.24–26
The prospective results of this study are in line with previous research in older adults.14 ,17 A meta-analytic review including eight studies found an integrated risk reduction of 11% in cardiovascular risk associated with active commuting (walking and cycling) compared with non-active commuting (mainly by car).15 Further, a meta-analysis found that the all-cause mortality risk was 36% lower for the highest level of PA of daily living compared with the lowest19 and the authors of a systemic review concluded that the largest benefit was found from moving from no activity to low levels of activity.27 In the light of a recent report in Lancet which revealed high sitting time in older adults especially, the present results of lower risk for CVD event and mortality by higher NEPA level are relevant.10
A central point is that the associations between NEPA and cardiovascular health and longevity seem to be evident regardless of intentional exercise habits. As it is widely known that regular exercise has a major impact on health, our findings have high clinical significance. Epidemiological studies have implied that in today’s society it is not only possible, but also very common, to exercise regularly yet be highly sedentary during the day (an ‘active couch potato’), and in the present study, there was a rather low association between NEPA and exercise. Finni et al28 studied how sedentary and NEPA time varied between days with and without intentional exercise by measuring electromyography activity in the quadriceps and hamstring muscle and found that a day including exercise did not significantly alter the time distribution between sedentary pursuits and NEPA, compared to a day without exercise.
Potential mechanisms to explain the observed independent importance of NEPA are largely interchangeable with the proposed mechanisms of prolonged sitting. One important mechanism is linked to energy expenditure, where prolonged sitting results in low energy expenditure close to the basal metabolic rate, while standing up and engaging in NEPA multiplies it.29 Comparisons of different daily movement patterns have shown that the daily energy expended in activity for standing or ambulatory workers might be double the energy expended in seated workers.30 A study among healthy, normally active men revealed a reduction in daily steps taken from an average 10.501 to 1344 over 2 weeks resulted in a significant increase in intra-abdominal fat and impairment of other important metabolic markers (with habitual dietary intake kept constant).31 Even if the model in this study reflects deconditioning effects rather than effects of inactive, highly sedentary adults over a longer period, it provides valuable insights.
Another potential mechanism is the hypothesis of myokine released from the contracting skeletal muscle.32 Lack of muscular contractions (as a consequence of sitting still) will undermine the endocrine function of the skeletal muscle and cause malfunction of several organs and tissues of the body. However, activation of the skeletal muscle per se and not necessarily the intensity of the activity, will ensure sustained endocrine function. Several potential myokines are proposed: lipoprotein lipase (important for fat metabolism and linked to CVD risk), interleukin 6 (IL-6; with central anti-inflammatory effects), contraction-induced GLUT-4 translocation in skeletal muscle and IL-15 (which may have a role in the muscle–fat cross talk through modulation of the visceral fat mass).
Along with the technology revolution of recent decades, there has been a shift in the balance between time spent in NEPA and time spent sitting in favour of the latter, resulting in an ‘unnaturally’ high amount of sitting time in the general population.33 A study among the Old Order Amish, who still live a traditional agricultural lifestyle and maintain a high level of daily movement, demonstrated that Amish men and women took on average three times as many steps per day as compared to other adults in the USA34 As the human genetic constitution has probably changed little in the past 30 000 years,35 and is therefore not selected for a sedentary lifestyle, it is hardly surprising that the contemporary lifestyle has generated health consequences for the humans of the 21st century.
The strengths of the present study are the large and representative cohort of women and men of the relevant age in Stockholm County, the high participant rate and the long follow-up period. The cohort was thoroughly characterised by a well-defined questionnaire and physical examination, which enabled adjustment for many possibly important confounders. Although the cross-sectional part of the study cannot prove causality for the metabolic factors, the prospective part is a strength. The Swedish national population registers used to ascertain the prospective outcomes are highly valid and particularly suitable for large-scale population-based epidemiological research.36 ,37 A methodological limitation is the use of self-reported data for the daily activities and NEPA index, intentional exercise and confounding variables. The NEPA index has not yet been validated and we cannot rule out potential bias for not reflecting actual NEPA in the population. Therefore, the NEPAs are not defined as activities within a specific intensity span, but rather elucidating the context of NEPA as part of daily living and not as intentional exercise. However, the nature of the questions constituting the NEPA score was well-suited for the study population, as they asked for NEPAs commonly performed by older adults in Sweden. Though, as one has to consider differences in NEPAs between different cultures, the present NEPA index should be used with cautiousness in populations of other cultures. An additional limitation of this study includes our inability to rule out possible effects of residual or unmeasured confounding. Though, to minimise the potential for reverse causality, we excluded all individuals with reported myocardial infarction, heart failure and stroke at baseline as well as deaths occurring in the first, second and third year of follow-up in the prospective analysis. All participants in the study were 60-year-old at baseline and interpretation of the results should be restricted to individuals around this age.
Conclusion
In the present study, a generally active daily life had important beneficial associations with cardiovascular health and longevity in older adults, which seemed to be regardless of regular exercise habits. As it is widely known that regular exercise has a major impact on health, these results have high clinical relevance. Our findings are particularly important for older adults, because individuals in this age group tend, compared to other age groups, to spend a relatively greater portion of their active day performing NEPA as they often find it difficult to achieve recommended exercise intensity levels. Along with the demographic shift towards an older population, this is important not only for individual well-being but also for the national and global burden of disease. For future health, promoting everyday NEPA might be as important as recommending regular exercise for older adults.
What are the new findings?
-
In a population-based sample of older adults, an active daily life was, independently of regular exercise habits, associated with significant beneficial effects on cardiovascular health in cross-sectional analyses.
-
Prospective analysis found a risk reduction of approximate 30% for a first time cardiovascular disease event and all-cause mortality, respectively, for those with an active daily life, compared to being sedentary.
How might it impact on clinical practice in the near future?
-
In clinical practice, promoting everyday non-exercise physical activity (NEPA) is as important as recommending regular exercise for older adults for cardiovascular health and longevity.
-
This is particularly important for older adults as they tend, compared to other age groups, to spend a greater portion of their active day performing NEPA as they often finds it difficult to achieve recommended exercise intensity levels.
-
Along with the demographic shift towards an older population, this is important not only for individual well-being but also for the national and global burden of disease.
Acknowledgments
The authors would like to thank Merja Heinonen and Gunnel Gråberg for their assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
Footnotes
-
Funding This study was supported by grants from the The Swedish Order of Freemason—Grand Swedish Lodge, Stockholm County Council, the Swedish Heart and Lung Foundation, the Swedish Research Council (Longitudinal Research) and the Tornspiran Foundation.
-
Competing interests None.
-
Ethics approval Ethical committee at the Karolinska Institutet, Stockholm, Sweden.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com