Article Text

Abstract
Gluteal pain is a common presentation in sports medicine. The aetiology of gluteal pain is varied, it may be referred from the lower back, mimic other pathology and refer to the hip or the groin. The complex anatomy of the buttock and pelvis, variability of presentation and non specific nature of signs and symptoms make the diagnostic process difficult. To date the approaches to this problem have focused on individual pathologies.
The paper proposes a novel educational system based on patho-anatomic concepts. Anatomical reference points were selected to form a diagnostic triangle, which provides the discriminative power to restrict the differential diagnosis, and form the basis of ensuing investigation.
This paper forms part of a series addressing the three dimensional nature of proximal lower limb pathology. The 3G approach (groin, gluteal and greater trochanter triangles) acknowledges this, permitting the clinician to move throughout the region, considering pathologies appropriately. These papers should be read in conjunction with one another in order to fully understand the conceptual approach.
Statistics from Altmetric.com
Gluteal pain is common in athletes and is often ascribed to hamstring origin pain however; back pain may be a source of referred gluteal pain.1
It can be seen how this can present a diagnostic conundrum. The presentation of gluteal strains, hamstring tears or sacroiliac joint pathology is similar and for the clinician, eliciting the significant features in order to differentiate the diagnosis can be a challenge.
This paper sets out a method based on patho-anatomic principles for a systematic examination of the chronically painful gluteal region and posterior thigh. This enables the clinician to discriminate more easily between pathological conditions and target their management to specific diagnoses.
THE GLUTEAL TRIANGLE
The 3G point
From anthropometric measurements in previous cadaveric dissection studies,2 the authors have defined a new reference point at the apex of the triangle. This point was termed the “3G point” in reference to the three-dimensional pathology and the groin, gluteal and greater trochanteric regions. The relationship of this point in the posterior coronal plane is that of, double the distance from the spinous process of L5 lumbar vertebrae to the ischial tuberosity, as a continuation of that line to the femur.
The specific anatomical landmarks and borders of the gluteal triangle are set out in fig 1:
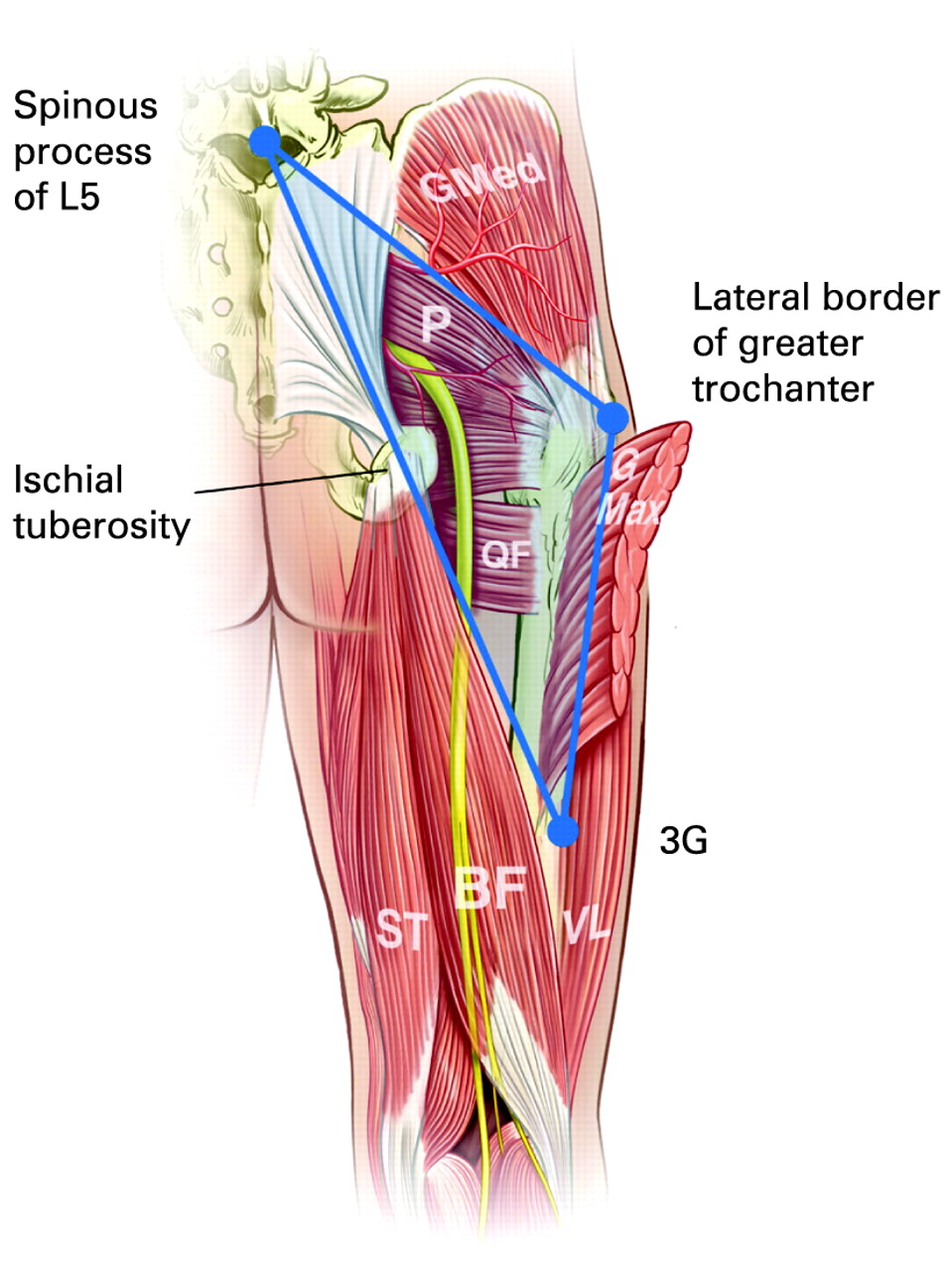
The gluteal triangle. G Max, gluteus maximus; G Med, gluteus medius; P, piriformis; QF, quadratus femoris; SM, semimembranosus; ST, semitendinosus; BF, biceps femoris; VL, vastus lateralis.
Spinous process of L5 lumbar vertebrae
Lateral edge of greater trochanter
3G point

The ischial tuberosity clock face. ST, semitendinosus; BF, biceps femoris; QF, quadratus femoris; P, piriformis; G Med, Gluteus medius.
ANATOMICAL RELATIONSHIPS OF THE BORDERS OF THE GLUTEAL TRIANGLE
Superficially in all cases the skin provides the surface covering, with epidermis and dermis, with underlying superficial fat superficial to the fascia.3 Last’s Anatomy was used as the reference text along with the authors current anatomical work.2 4 The fascia overlying the gluteal triangle is a continuation of the posterior lumbar fascia, in which Gluteus maximus is embedded then extending to join tensor fasciae latae and form the iliotibial band with a slip insertion into the greater trochanter. This gives rise to a continuous layer of fascia which plays a significant role in the pathology.
SUPERIOR BORDER OF TRIANGLE
Iliolumbar ligament and fascia
Gluteus maximus
Gluteus medius
Gluteus minimus
The spinous process of L5 lumbar vertebrae was selected for its ease of location and the associated lumbar pathology. This is an easily palpable reference point located at the midline, at a level just below the line drawn between the posterior iliac crests. The posterior layer of the thoracolumbar fascia makes a major contribution to the supraspinous and interspinous ligaments in the lower thoracic spine. Multifidus combines with the thoracolumbar fascia to form the lumbar supraspinous and interspinous ligaments. The spinal attachments of these ligaments form a dense connective tissue and support the composition by both muscle tendon and aponeuroses along the length of the lumbar spine. Specific attachments at the L5 spinous process are difficult to differentiate on palpation. The supraspinous ligament is the deepest structure with the proximal insertion of multifidus, erector spinae and thoracolumbar fascia more superficially.
The line between L5 and the greater trochanter forms the superior border of the triangle which corresponds to the medial border of gluteus medius muscle.2 This fan-shaped muscle arises from the outer surface of ilium between the posterior and anterior gluteal lines and converges to form a tendon, this is attached to the oblique ridge sloping downwards and forwards on the lateral surface of the greater trochanter. The posterior border of gluteus medius may merge with piriformis at its insertion. Gluteus maximus overlies medius and is transected by the superior border of the triangle. It arises from the ilium behind the posterior gluteal line, the iliac crest, the thoracolumbar fascia, and the posterior surfaces of the sacrum, coccyx, and the sacrotuberous ligament and from the fascia covering gluteus medius. The fibres descend inferolaterally, the deeper fibres inserting into the greater trochanter whilst the superficial fibres and the upper part of the muscle end in a tendonous band, passing lateral to the greater trochanter and inserting into to the iliotibial band.

Medial to the gluteal triangle.

Superior to the gluteal triangle.
Lateral to the gluteal triangle.

Within the gluteal triangle.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ischial tuberosity.
MEDIAL BORDER
L5 lumbar vertebrae
Gluteus maximus
Sacroiliac joint
Sacrotuberous ligament
Ischial tuberosity and common hamstring origin
Semimembranosus origin
Gemellus superior, inferior
The medial border runs from the 3G point on the femur to the spinous process of L5. The mid point of this line is the ischial tuberosity, which allows for its easy location. The ischial tuberosity marks the lateral boundary of the pelvic outlet but also is found at the midpoint of the medial border of the gluteal triangle. The importance of palpable knowledge here is critical. From a posterior view, in the 2 o’ clock position is palpable the origin of semimembranosus and from the 4 o’clock position round to 7 o’clock, the combined tendonous insertion of the long head of biceps femoris and semitendinosus. The sacrotuberous ligament at 10 o’clock is palpable at the 8 o’clock position and the insertion of the gemellus at the 7 o’clock position.
Inferiorly, the medial border of the triangle transects the posterior compartment. The bellies of semimembranosus and semitendinosus along with biceps femoris are palpable working from medial to lateral. Superiorly, the border follows the line of the sacrotuberous ligament, with gluteus maximus palpable superficially. The medial line of the triangle also serves to remind us of the vector of referred pain from the sciatic nerve which is an important differential diagnosis in the buttock.
LATERAL BORDER
Tensor fasciae latae
Iliotibial band
Vastus lateralis
Biceps femoris
The lateral border of the triangle is marked from the greater trochanter along the shaft of the femur to the 3G point. The iliotibial band runs parallel to this border. It blends with the capsule of the knee joint to attach to Gerdy’s tubercle, the lateral condyle of the tibia and the head of the fibula. Vastus lateralis and biceps femoris form the bulk of this muscular compartment, with the bellies of these muscles the only palpable structures. The apex of the triangle is at the 3G point which lies in line with the femur at a point double the distance from the spinous process of L5 to the ischial tuberosity.
WITHIN THE TRIANGLE
Gluteus maximus
Piriformis
Sciatic nerve
Structures contained within the triangle are the causal agents in much gluteal pathology, but lie deep to gluteus maximus and are palpable at best, at their insertion to the greater trochanter. Piriformis, which arises from the anterior aspect of the sacrum, between and lateral to the sacral foramina. As the muscle leaves the pelvis, some slips arise from the pelvic surface of sacrotuberous ligament. The muscle passes out of the pelvis through the greater sciatic foramen. Its rounded tendon is attached to the upper border and medial aspect of the greater trochanter, close to the insertion of the obturator internus and the gemellus with which it may be partially conjoined. The sciatic nerve, from the ventral rami of the fourth lumbar to third sacral spinal nerves exits the pelvis through the greater sciatic foramen, deep to piriformis, and descends between the greater trochanter of the femur and the ischial tuberosity. The sciatic nerve is sandwiched on its exit from the greater sciatic foramen by the pririformis muscle superiorly and the gemmulus inferiorly5 and there has been much variation in anatomy described potentially infringing on the nerve on its extra pelvic course.
A PATHO-ANATOMIC APPROACH USING GLUTEAL TRIANGLE
The diagnostic process of history and examination, although taught as integral to determining the differential diagnosis may be abbreviated, due to time pressures, coaching and management pressures,6 or to ward off potential litigation, with a tendency to rely on investigational studies as an initial diagnostic step (eg, a magnetic resonance scan to check for an anterior cruciate ligament rupture), or much earlier than required.7 8
The authors propose a four step compartmentalisation of the diagnostic process re-emphasising history and examination and limiting investigation to the final step as follows:
Step 1: define & align
Define the anatomical points and borders of the triangle on the patient (L5 spinous process, greater trochanter, ischial tuberosity and 3G point).
Step 2: listen & localise
Listen to the patient’s history and obtain as many localising factors as possible then pinpoint the pain in relation to the gluteal triangle.
Step 3: palpate & re-create
Carefully palpate the identified area and determine which anatomical structures are painful. The use of provocative examinations to re-create the patient’s pain can be a vital diagnostic stage, although to describe all of these tests in detail is beyond the scope of this text, and these have been described comprehensively elsewhere.9 10
Step 4: alleviate & investigate
Where a number of anatomical structures are in close proximity, clinical presentations can be very similar. The manner in which pain can be removed may be very helpful. A decrease in pain following removal from aggravating activity, or the elimination of symptoms following guided injection of local anaesthetic into the structure can be as diagnostic as a positive sign.
THE DIAGNOSTIC TRIANGLE
The step-wise approach using the gluteal triangle is summarised in tables 1–5. This gives the clinician a guide to the diagnostic process and pathological cause of the chronic gluteal pain in relation to the triangle. Each table shows the differential diagnosis for conditions presenting within that anatomical area, and the combined sieve represents a comprehensive assessment of the region. Prior to each table the most common diagnosis is drawn out but the reader is directed to the table for a comprehensive differential.
It is recognised that some argue the discriminatory nature of clinical tests11 but where appropriate, the evidence based examination of choice is given,10 some tests are widely utilised in clinical practice with limited or conflicting evidence, as the best available, and in this case these are included.
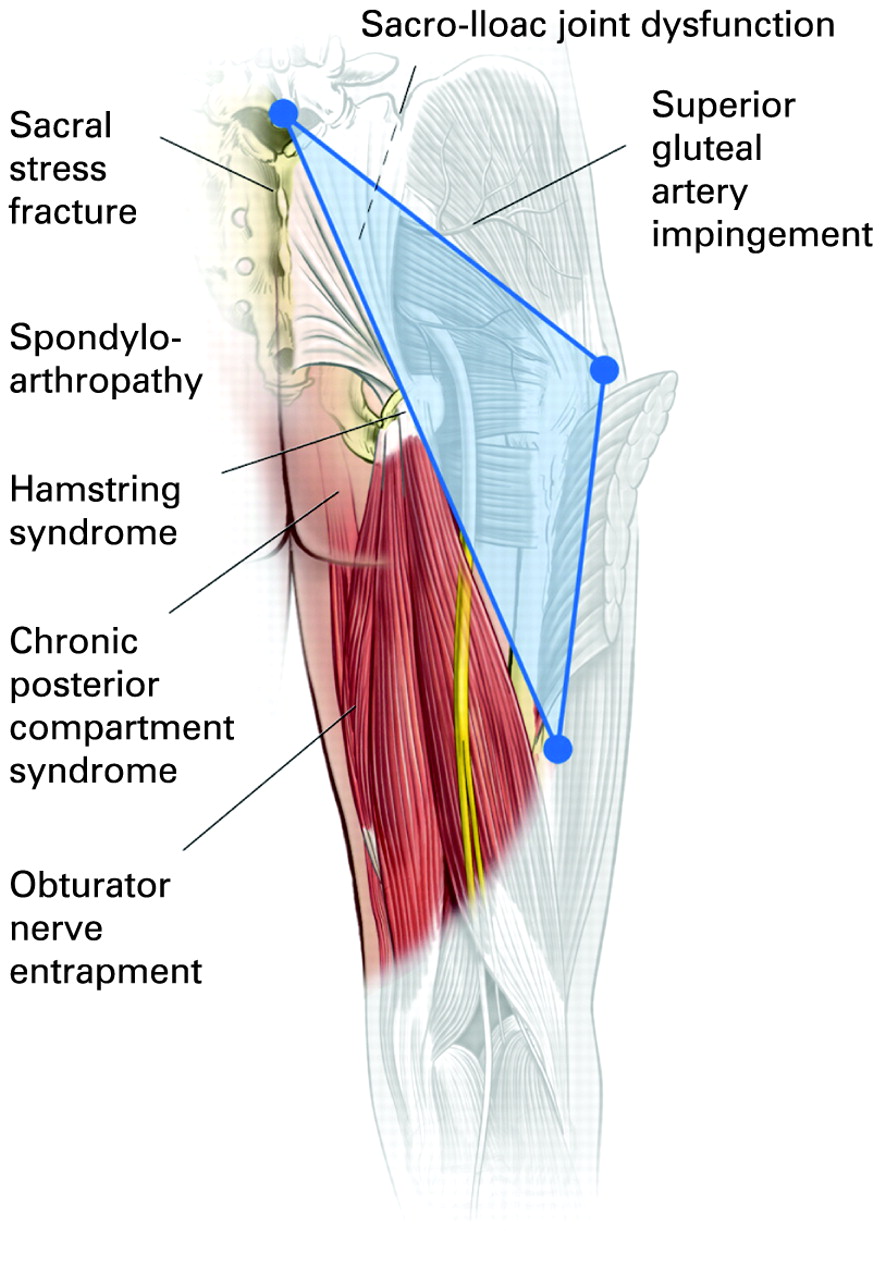
MEDIAL
The area lying medial to the line from spinous process of L5 vertebrae to apical point of the gluteal triangle highlights the sacro-iliac joint (SIJ) and the most common presentation within this region of the triangle is that of sacro-iliac pain. The SIJ is a joint with limited mobility, acting as a force transducer and a shock absorber. This is affected as part of three closed kinematic chains involving the lumbar spine, sacrum, pelvic girdle and lower extremities.
SUPERIOR
The area lying superior to the line from spinous process of L5 vertebrae to the greater trochanter transects the postural and locomotor muscles of the gluteals of which the muscle bellies and insertions are the cause of much pathology located in this area.
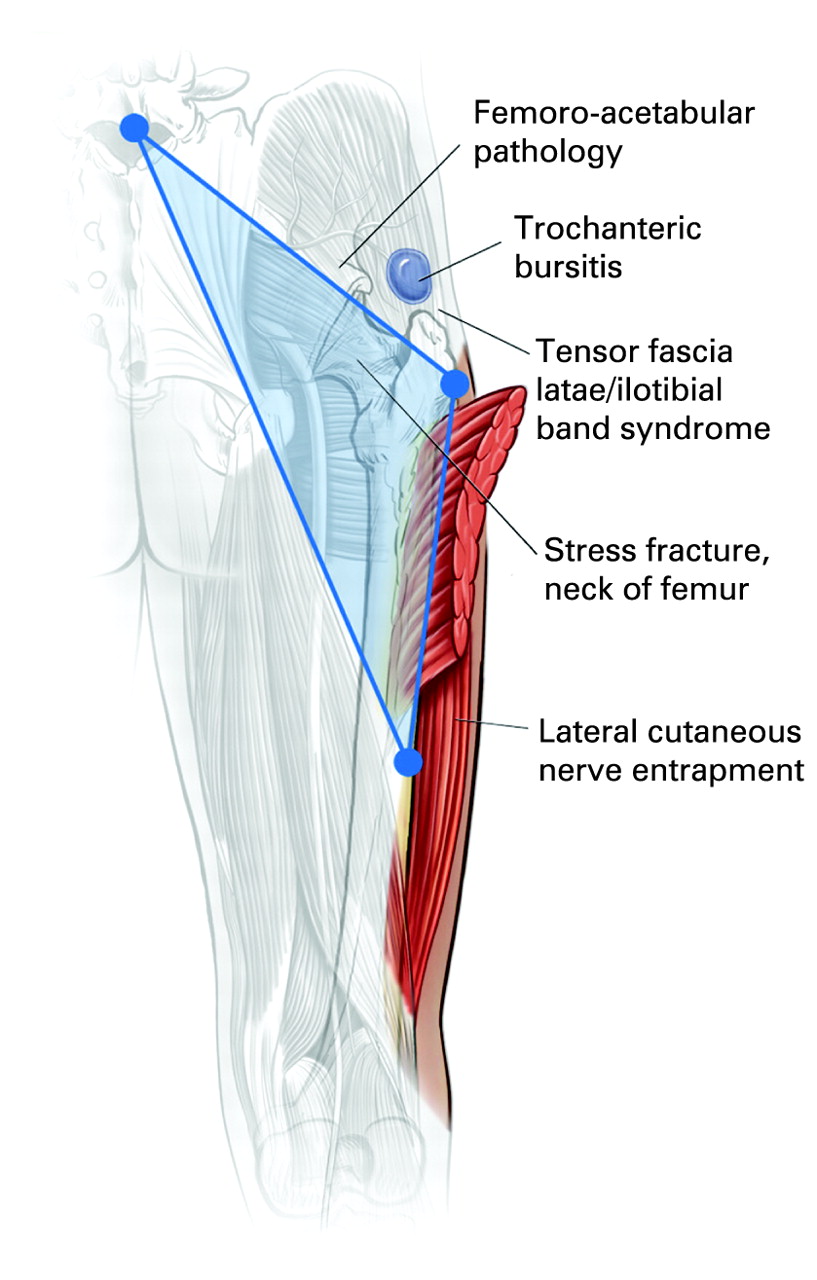
LATERAL
The area lying lateral to the line from greater trochanter to the 3G point on the shaft of the femur highlights the hip and structures around it as potential origins of pathology in particular the acetabulum.
WITHIN THE TRIANGLE
Within the space marked by the lines described above, are contained the lateral rotators of the hip which sit deep to the gluteal muscles in particular piriformis, but this region is also transected by the sciatic nerve an important cause of referred pain.
ISCHIAL TUBEROSITY
The significant point at the midline of the medial triangle is the ischial tuberosity. The anatomy of the insertions and relations here has been discussed above but are highlighted again in the associated figure. The high incidence of hamstring strains and their causation of long periods of absence from sport and frequent recurrence rates make them particularly significant in causes of gluteal pain.57
INTRA-ABDOMINAL PATHOLOGY
A cause of gluteal pain which has not been discussed in this article is that of intra-abdominal causes. Endometriosis is known to widely radiate pain and the gluteal region is not immune. Vascular causes such as abdominal aortic aneurysm can present as gluteal pain, alongside rarer vascular insufficiencies such as Leriche syndrome or common iliac stenosis.61 Colo-rectal pathology can present with referred pain and inflammatory bowel disease is seen inn association with the spondyloarthritidies. Malignancy either of the pelvis or of soft tissues cannot be ignored and must be excluded but is beyond the scope of this diagnostic sieve which restricts itself necessarily to musculoskeletal diagnoses.
CONCLUSION
This paper presents a method of teaching the causes of chronic pain in the gluteal region and posterior thigh. This also serves as a means of making the differential diagnosis through history, appropriate discriminative diagnostic examination and ultimately, we accept in many cases, directed investigation.
This paper is but a part of the 3G approach to proximal lower limb pain, and for a comprehensive approach, should be read in conjunction with the groin and greater trochanter 3G companion papers.
In delivering this as a diagnostic tool we recognise that experience, expertise and a thorough knowledge of the anatomy of the area cannot be supplanted but may help narrow the differential diagnosis, to the benefit of patient and clinician.
Acknowledgments
Thanks to the medical illustrator Dr Levent Efe for the high standard of illustrations.
REFERENCES
Footnotes
Competing interests: None.
Funding: AFM was supported by an educational grant from RS Scan Lab UK. EF was supported by the Irish Centre for Arthritis Research and Education (ICARE).