Article Text

Abstract
Disorders of the shoulder are extremely common, with reports of prevalence ranging from 30% of people experiencing shoulder pain at some stage of their lives up to 50% of the population experiencing at least one episode of shoulder pain annually. In addition to the high incidence, shoulder dysfunction is often persistent and recurrent, with 54% of sufferers reporting ongoing symptoms after 3 years. To a large extent the substantial morbidity reflects (i) a current lack of understanding of the pathoaetiology, (ii) a lack of diagnostic accuracy in the assessment process, and (iii) inadequacies in current intervention techniques. Pathology of the rotator cuff and subacromial bursa is considered to be the principal cause of pain and symptoms arising from the shoulder. Generally these diagnostic labels relate more to a clinical hypothesis as to the underlying cause of the symptoms than to definitive evidence of the histological basis for the diagnosis or the correlation between structural failure and symptoms.
Diagnosing rotator cuff tendinopathy or subacromial impingement syndrome currently involves performing a structured assessment that includes taking the patient’s history in conjunction with performing clinical assessment procedures that generally involve tests used to implicate an isolated structure. Based on the response to the clinical tests, a diagnosis of rotator cuff tendinopathy or subacromial impingement syndrome is achieved. The clinical diagnosis is strengthened with the findings from supporting investigations such as blood tests, radiographs, ultrasound, magnetic resonance imaging (MRI), computed axial tomography (CT), radionucleotide isotope scan, single photon emission computed tomography, electromyography, nerve conduction and diagnostic analgesic injection. This process eventually results in the formation of a clinical hypothesis, and then, in conjunction with the patient, a management plan is decided upon and implemented.
This paper focuses on the dilemmas associated with the current process, and an alternative method for the clinical examination of the shoulder for this group of patients is proposed.
Statistics from Altmetric.com
Pathology of the rotator cuff and subacromial bursa is considered to be the principal cause of pain and symptoms arising from the shoulder. This is reflected in the variety of diagnostic labels given to describe the pathology: rotator cuff tendinopathy/tendinosis/tendinitis, supraspinatus tendinopathy/tendinosis/tendinitis, subacromial impingement syndrome, subacromial bursitis, bursal reaction, partial thickness, full thickness and massive rotator cuff tear. Generally these diagnostic labels relate to a clinical hypothesis attempting to explain the cause of presenting symptoms rather than to a definitive diagnosis based on robust and definitive biomechanical, histological and imaging evidence to explain the basis of the presenting symptoms.
The substantial morbidity associated with rotator cuff pathology reflects (i) a current lack of understanding of the pathoaetiology, (ii) a lack of diagnostic accuracy in the assessment process, and (iii) inadequacies in current intervention techniques. The dilemmas associated with current practice are discussed and an alternative method for the clinical examination of the shoulder for this group of patients is proposed.
ASSESSMENT OF ROTATOR CUFF PATHOLOGY
Historically, musculoskeletal assessment of the shoulder has been based around a premise that it is possible to isolate individual structures and apply a mechanical procedure that either compresses or stretches the tissue of interest or requires it to contract. However, it is unlikely that any test would not stretch or compress adjacent structures or cause them to contract during the procedure. Without doubt this is one of the reasons why more recent studies on the sensitivity, specificity and predictive accuracy of tests1–4 have concluded that, although they have a high sensitivity and reproduce symptoms, they have an associated low specificity which substantially reduces their utility in deriving a specific diagnosis. As such the commonly used orthopaedic special tests should be thought of as pain or symptom provocation tests, without the ability to contribute to a structural diagnosis.
Examples of clinical tests used to identify structural pathology in current use include the O’Brien active compression test for superior labral pathology,5 the posterior capsule length test to assess the extensibility of the posterior glenohumeral capsule6 and Jobe’s “supraspinatus test” to assess the strength and pain response from the supraspinatus musculotendinous unit.7 Other tests include the Neer sign,8 which has been embraced with other tests, such as the Hawkins’ test9 and the Internal Rotation Resistance Stress Test,10 as clinical methods to implicate the acromion as the cause of the presenting shoulder symptoms.
There are at least three reasons why the clinical assessment procedures for rotator cuff tendinopathy/impingement cannot isolate individual tendons and other structures and inform an accurate diagnosis. These are the morphology of the rotator cuff, the position and innervation of the subacromial bursa (SAB), and the lack of correlation between symptoms and contemporary methods of imaging.
The rotator cuff tendons do not function as separate entities.11 The clinical implications of the confluence of tendon, ligament (coracohumeral) and glenohumeral capsule are profound and clinical tests proposed to identify symptoms arising from any one individual tendon12 13 are groundless. The lack of specificity of the clinical tests for the rotator cuff has been demonstrated1 4 14 and clinical reasoning based on the response of these tests needs to be re-evaluated. In addition to the fusing of the rotator cuff tendons, the large SAB is innervated15 16 and appears to have a central role in the presentation of pain in the shoulder.15–20 Any test designed to assess the integrity and pain response from any of the rotator cuff tendons would involve bursal tissue. Two comprehensive systematic reviews of the diagnostic accuracy of the rotator cuff tests have been conducted1 4 and have reached similar conclusions. Both reviews reported that, although a myriad of clinical tests have been proposed to selectively assess the rotator cuff and subacromial bursal tissues and the integrity of the subacromial space, no test or series of tests have emerged that are capable of doing this.
The ability to achieve an accurate structural diagnosis is further challenged by the poor correlation between radiological imaging and symptoms. Using MRI, Frost et al21 reported that structural pathology in the rotator cuff in 42 individuals with a clinical diagnosis of subacromial impingement syndrome was similar to that in 31 age-matched asymptomatic individuals. Similar findings have been reported by others investigating the relationship between radiograms, diagnostic ultrasound (US) and MRI, and symptoms.22–26
A series of investigations involving analgesic injections for shoulder pain and weakness have concluded that the perceived weakness during clinical strength testing of the rotator cuff may be better explained as pain inhibition than as a result of structural failure.27–29 The role of the rotator cable may help to explain why tears of the rotator cuff identified in imaging investigations may not relate to a loss of shoulder function. The tendon tissue medial to the cable may act through the cable to produce normal shoulder movement even in the presence of structural failure of the rotator cuff located lateral to the cable. This requires ongoing investigation.
The gold standard for diagnostic comparison with the clinical tests has traditionally been direct intraoperative observation, or indirect methods such as MRI or US. As not all structural failure correlates with symptoms,21–26 it is apparent that these gold standard tests are not ideal reference tests, and this explains the high numbers of false negatives and false positives reported in these investigations. Of concern, clinical decision-making based upon practice that combines combinations of the currently recommended clinical tests supported by information gained from imaging or observational findings is potentially flawed and does not provide a robust framework for the clinician to clinically reason the structure(s) involved in the symptomatology and create a credible management plan. Smidt and Green30 have acknowledged that the reproducibility and validity of the diagnosis and classification system for shoulder complaints are inadequate. As such, the clinical reality is that a new method of assessment needs to be considered.
Difficulties in deriving a definitive structural diagnosis of symptomatic shoulder tissues have been recognised by others.1 3 4 14 31–33 In response to these difficulties, alternative methods of assessment have been suggested.34 35 These methods do not reject traditional methods of shoulder assessment but recognise their inability to achieve a definitive diagnosis due to low specificities. The poor specificities and inadequate likelihood ratios reduce the ability of these tests to inform the clinical decision-making process and patient management. Clinicians are increasingly aware of the limitations of current assessment procedures in the shoulder1 2 4 14 and alternative testing methods have been proposed.34 However, these procedures require rigorous assessment of their reliability and validity before being adopted.
THE SHOULDER SYMPTOM MODIFICATION PROCEDURE
The current proposal advocates the use of special orthopaedic tests only as pain or symptom-provoking procedures and that these procedures should be used clinically in conjunction with other physical movements identified by the patient that reproduce their shoulder pain. Once the movement or activity that reproduces the shoulder symptoms has been agreed upon, the Shoulder Symptom Modification Procedure (SSMP) is applied. The SSMP is a series of four mechanical techniques that are applied while the patient performs the activity or movement that most closely reproduces the symptoms experienced by the patient (fig 1). The reason these procedures may reduce symptoms is not known. It could be due to soft tissue or joint displacement, changing sensory motor control or neuromodulation.

The shoulder symptom modification procedure.
The starting point is to select a movement or activity that reproduces the patient’s symptoms. This may be a movement identified by the patient or one taken from the series of currently recommended clinical orthopaedic tests that most closely correlates with the patient’s symptoms. Information from the patient’s history will help to identify the most relevant position in which to examine the patient. For example, a freestyle swimmer complaining of shoulder pain during the pull through phase of swimming should be tested in prone and a tennis player experiencing shoulder pain during a backhand stroke should be tested in standing while performing this movement. Weights, sporting equipment, vocational tools and resistance tubing may be used to reproduce the symptoms if the free active movement proves insufficient. Any contraindications to movement and testing must be observed. Once the provocative activity has been identified, the SSMP process is commenced with the aim of identifying one or a series or techniques that reduce symptoms, by either decreasing pain and/or increasing movement. Examples of this type of assessment are already strongly entrenched in clinical practice to determine whether structures associated with the spine influence shoulder symptoms.36 37 The SSMP involves four principal procedures. However, additional techniques may be added to the four fundamental tests. The starting procedure and the order of testing are changeable. A brief description of each technique within the SSMP is as follows.
Humeral head procedure
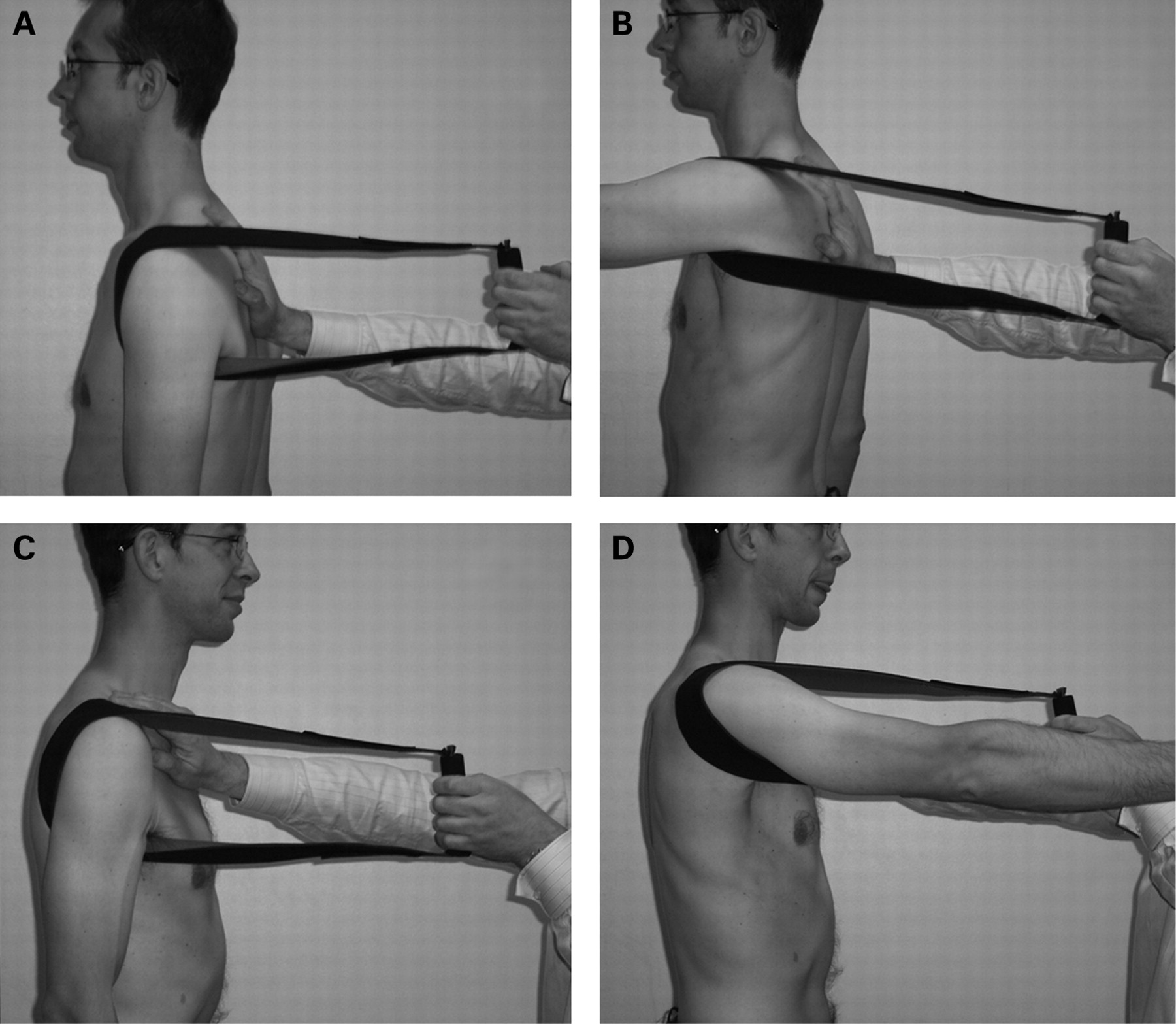
This component of the SSMP aims to influence the humeral head position in relationship to the glenoid fossa. These procedures involve a series of pressure/displacement techniques and muscle contraction techniques. The pressure techniques are applied in the region of the humeral head and include the use of manual pressure, mobilisation belts, resistance tubing or neoprene slings around the humeral head. Anteriorly or posteriorly directed pressure is maintained during the patient’s aggravating activity. Neoprene is preferred due to its comfort and the ability to modify the anterior or posterior force with a medial, lateral, inferior and/or superior force to determine which position has the most beneficial effect on symptoms (fig 2).

One example of a “humeral head” procedure.
Muscle contraction procedures involve resisted movements that modify muscle activity at the shoulder, altering the pattern of shoulder muscle contractions that may influence symptoms. Examples include repeating the aggravating activity during a sustained contraction of the shoulder external rotators, humeral head depressors and/or adductors. In this instance, lightweight resistance with rubber tubing is used to create the muscle contraction during the movement to determine its effect on symptoms (fig 3). Procedures that may influence the humeral head position via muscle contraction may be relevant in managing symptoms. Superior translation of the humeral head on the glenoid fossa is observed in patients with subacromial impingement syndrome and rotator cuff disease,38 39 and procedures that activate humeral head depressors may counter this translation.40 If a particular movement results in the complete cessation of symptoms then the testing process is over. If there is only a partial reduction in symptoms the amount is noted and other components of the SSMP are tested to determine whether a better response is achieved from another technique or whether a combination of techniques results in a greater reduction of symptoms.

One example of a technique to assess the influence of altered muscle activation on shoulder movement.
Changing scapular position
A series of manual techniques to slightly modify the scapular position are applied to see whether symptoms change during the aggravating movement. The changes made to the scapular position should be relatively small. If manual techniques are not possible, the application of tape to facilitate a change in scapular position may be considered.35 The changes may be in one plane of movement or in combinations of planes of movement.
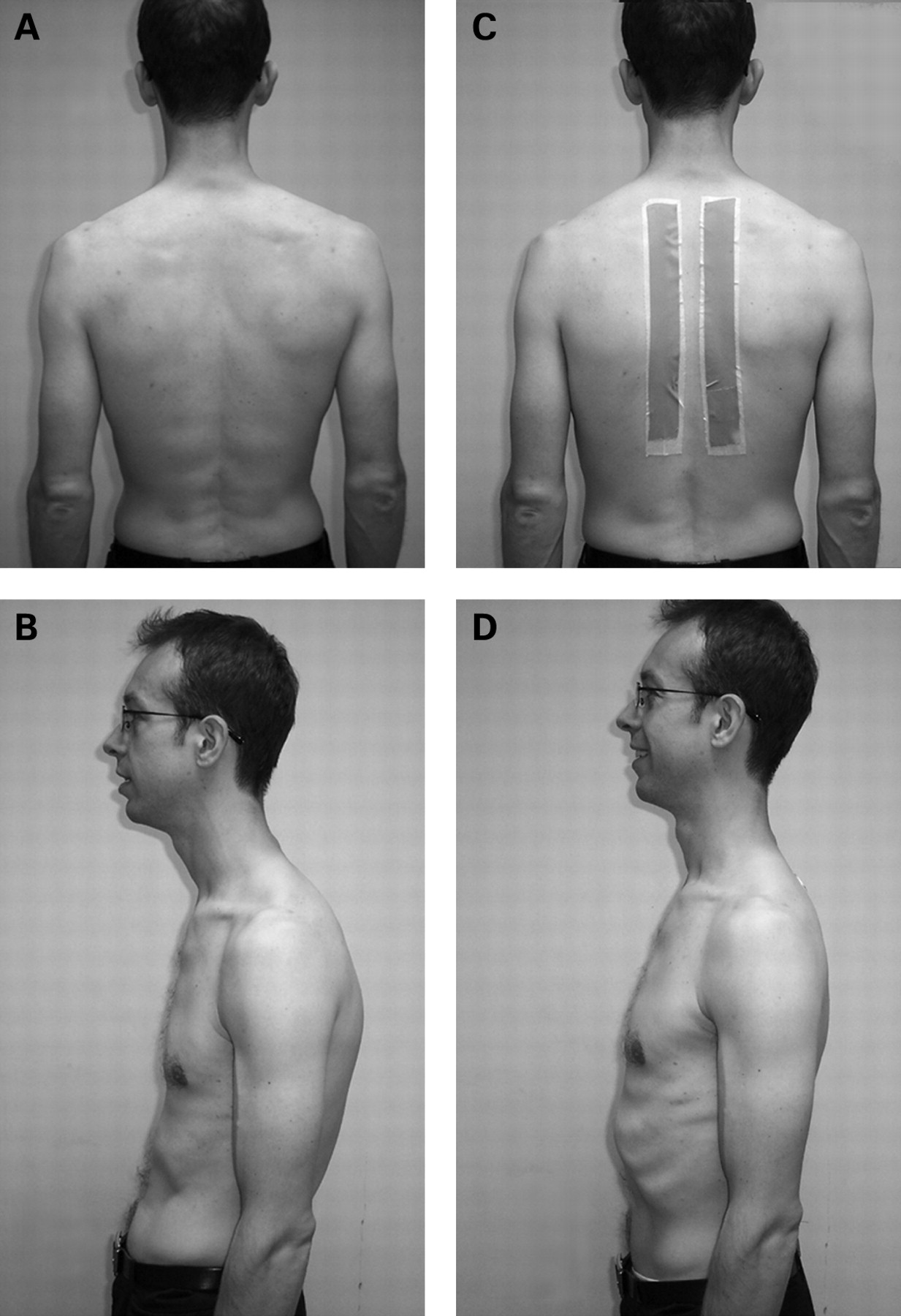
Cervical and thoracic region procedures
Structures within the cervical and thoracic region may refer pain to the shoulder. A variety of procedures, often described as muscle, soft tissue, osseous and joint-based techniques, should be applied to determine their effect on the patient’s aggravating movement. The effect of changing the thoracic kyphosis is also investigated. The patient’s thoracic kyphosis is reduced either through gentle manual reduction or via taping (fig 4). Once this is achieved the aggravating activity is retested to determine the response. Taping the thoracic region and shoulder does not appear to have a placebo effect on pain and range of shoulder movement.35
{kind=link}
{kind=link}
{kind=link}
{kind=link}
One example of a thoracic kyphosis modification procedure.
Although the order of the techniques used in the SSMP is interchangeable, two important aspects need to be considered. First, the magnitude of the change in pain experienced by the patient as a result of one or a combination of techniques during the SSMP process should ideally be a minimum of 30% change from the baseline pain using a numerical pain rating scale (NPRS). Although any single SSMP or combination of SSMPs that both the patient and clinician agree on can be used, a 30% change represents a substantial and meaningful change for patients.41 42 Second, there should be consistency of response to the SSMPs that have been selected. There should be a similar change in symptoms with the SSMP when tested at least twice within the assessment session, with the response being consistent on both occasions. This will increase both the patient’s and the clinician’s confidence in the process.
Once the clinician and patient agree on the SSMPs that have resulted in the greatest reduction in symptoms, a rehabilitation programme based on these responses is formulated. It is beyond the scope of this paper to discuss treatment options, but in general they include techniques that are similar to the testing procedures. If the SSMP process does not produce any change, the clinician should consider other treatment options such as injection therapy, pain-relieving techniques, general or specific shoulder rehabilitation exercise programmes, modalities, taping or surgery.
EVIDENCE TO SUPPORT THIS MODEL
The SSMP is not meant as a replacement for current clinical practice but as an adjunct to help support the clinical decision-making process by identifying factors that alleviate the patient’s shoulder symptoms. Some evidence exists to support this model. Lewis et al35 used taping as a method of changing the thoracic kyphosis and scapular position and reported that, when compared with no tape or a placebo taping procedure, the postural correction taping led to an increase in shoulder movement in people with and without shoulder symptoms. Other investigations have also reported that a reduction in the thoracic kyphosis leads to an increase in shoulder movement.43 Similarly, in patients with shoulder pain, posteriorly directed pressure applied to the region of the humeral head led to an immediate increase in shoulder elevation range and concomitant decrease in pain when compared with a sham and a control technique.44 Boyle45 reported that manual therapy techniques in the upper thoracic region substantially reduced pain in a case series of two patients presenting with impingement syndrome. Although these examples are limited, they suggest that a variety of techniques may influence shoulder symptoms in patients who present with a clinical presentation of rotator cuff tendinopathy/subacromial impingement.
ADVANTAGES OF THIS MODEL
A definitive clinical diagnosis of rotator cuff tendinopathy and subacromial impingement cannot currently be made. Clinicians treating low back pain have recognised the complexity of making a definitive diagnosis,46 and terms such as non-specific low back pain have been used in research investigations.47 The same diagnostic dilemma faces the clinician when examining a patient with shoulder pain, and a more appropriate diagnosis for rotator cuff tendinopathy/subacromial impingement may be mechanical shoulder pain. As we gain a better understanding of the aetiology and pathology, clinical assessment techniques will improve in their ability to delineate reliable, valid and robust clinical diagnostic categories.
The SSMP recognises the inadequacies of the present method of assessment and proposes that patient management may be guided by the response to symptom modification. These assessment procedures may be applied sequentially with one building upon the previous until the most positive single procedure or combination of procedures has been identified. The assessment procedures are then used as treatment techniques for the management of the patient’s condition. For example, a reduction in the thoracic kyphosis may result in a partial reduction in pain and partial improvement in shoulder flexion range, and if, in addition to this, an anteriorly to posteriorly directed pressure on the humeral head results in total alleviation of pain and restoration of full range of movement then the rehabilitation programme may include exercises to decrease the thoracic kyphosis together with shoulder movement activities performed while an anterior-to-posterior pressure in the region of the humeral head is applied. The programme is graduated according to the individual’s needs and aims to restore normal function.
The SSMP model is flexible and is capable of modification and evolution. As techniques that modify shoulder symptoms are identified, they may be incorporated into the model and procedures that are found to be less useful should be withdrawn.
LIMITATIONS TO THIS MODEL
Patients, health commissioning bodies and clinicians are embracing an evidence-based practice model of healthcare.48 49 Evidence-based practice (EBP) uses the most robust and appropriate research evidence available, in conjunction with the clinician’s experiences and the patient’s beliefs and values,48 49 to inform practice. Where evidence is not available, the EBP model allows for clinical experience to guide practice. It is becoming increasingly evident that the special musculoskeletal tests used in current practice are little more than symptom provocation tests and, from an EBP perspective, their use to inform diagnosis is limited.1–4 14 50 Although research evidence to justify the SSMP model is unavailable, EBP allows clinicians to propose models of assessment and management that are based on clinical experience with an understanding that research to verify or refute the clinical claims will follow. Research to investigate the usefulness of this model of assessment is being conducted and the utility of this model is its ability to change and adapt in response to new and emerging information.
In conclusion, current clinical tests used in the diagnosis of rotator cuff tendinopathy and subacromial impingement syndrome are of limited value due to their poor specificity. This suggests that they are useful as procedures that reproduce symptoms but not as a means of determining the origin of those symptoms. Patient management based on clinical reasoning derived from the findings of the currently recommended clinical orthopaedic tests may lack validity. The SSMP model assesses the individual or combined response to mechanical procedures performed around the shoulder, during aggravating movements. If individual or combined techniques improve symptoms, then similar techniques may be used in patient management. The Shoulder Symptom Modification Procedure is presented as one model of assessing the shoulder and informing patient management. Considerable research is required before this model should be accepted as a clinical alternative.
What is already known on this topic
The lack of specificity of the clinical tests for the rotator cuff and subacromial impingement has been demonstrated in a number of research investigations and systematic reviews. Clinical practice and clinical reasoning based on the response of these tests need to be re-evaluated in light of this. The reasons for the poor specificity include (i) an inability to selectively test the individual rotator cuff tissues, (ii) the presence of the subacromial bursa, which contains nociceptors and pain chemicals that will be stretched and compressed during all the clinical tests of the shoulder, and (iii) a lack of correlation between the current clinical tests and structural pathology identified with imaging in the form of ultrasound and magnetic resonance imaging.
What this study adds
Based on the lack of diagnostic accuracy of the clinical tests currently used, a new model of clinical assessment is proposed. The Shoulder Symptom Modification Procedure involves comparing symptomatic activities and movements identified by the patient before and after the application of a series of clinical techniques. The aim of this process is to find one or a combination of techniques that reduces the patient’s symptoms. This proposal requires considerable research before it becomes an accepted clinical alternative.
REFERENCES
Footnotes
Competing interests: None declared.
Patient consent: Obtained.