Article Text

Abstract
Objective: To measure the graded relation between cardiorespiratory fitness and sum of skinfolds, waist circumference, and blood pressure in children and adolescents participating in the European youth heart study.
Methods: The participants were 4072 children and adolescents (aged 9 and 15) from Denmark, Portugal, Estonia, and Norway. Cardiorespiratory fitness was indirectly determined using a maximal ergometer cycle test. The sum of four skinfolds, waist circumference, and blood pressure were assessed with a standardised protocol. Linear regression analysis was used to test the graded relation between cardiorespiratory fitness and the dependent variables adjusted for pubertal stage, sex, and country.
Results: A significant curvilinear graded relation was found between cardiorespiratory fitness and waist circumference and sum of skinfolds (partial r2 for cardiorespiratory fitness was 0.09–0.26 for the different sexes and age groups). Systolic and diastolic blood pressure also showed a curvilinear relation with cardiorespiratory fitness, and fitness explained 2% of the variance in systolic blood pressure. The difference in systolic blood pressure between the least and most fit was 6 mm Hg.
Conclusion: A curvilinear graded relation was found between cardiorespiratory fitness and waist circumference, sum of skinfolds, and systolic blood pressure. The greatest difference in these health variables was observed between low and moderate fitness levels.
- cardiorespiratory fitness
- fatness
- anthropometry
- blood pressure
- children
Statistics from Altmetric.com
Obesity assessed using body mass index, skinfolds, or waist circumference is a strong risk factor for diabetes type 2 and cardiovascular disease in the adult population.1–6 Hypertension is a major risk factor for stroke, coronary heart disease, and congestive heart failure.7 The clinical symptoms of many chronic diseases do not become apparent until late in life, but it is generally accepted that the origin of many diseases and conditions such as hypertension and obesity lies in early life. The aetiology of such diseases is of course multifactorial, but cardiorespiratory fitness may play an important role.
The association between cardiorespiratory fitness and obesity and hypertension is documented in the adult population, showing that people with low fitness have increased risk of both obesity and hypertension.8,9 In children and adolescents, an association between cardiorespiratory fitness and different measures of body composition and blood pressure has been observed.10–12 However, studies analysing the graded relation between cardiorespiratory fitness, obesity, and blood pressure in this population are scarce.
Knowledge about the shape of the relation between cardiorespiratory fitness and health outcome is important, because such information adds essential aspects to the aggregated data that serve as the basis for physical activity guidelines.13 The European youth heart study focuses on cardiovascular disease risk factors, and their associated influences, in children and adolescents. A large number of children and adolescents have been included in this study, and the purpose was to evaluate whether or not there exists a graded relation between cardiorespiratory fitness, obesity measures, and blood pressure, and if so whether this relation is linear or curvilinear.
METHODS
Children and adolescents from Denmark (Odense), Portugal (Madeira), Estonia (Tartu), and Norway (Oslo) participated in the European youth heart study. The written consent of parents and children were obtained before they entered the study, and the approval of the regional ethical committee in each country was acquired. A common test protocol was followed by all participating centres to ensure similarity with respect to data collection.
Participants and sampling
Participants were children and adolescents from both sexes aged 9 and 15 years. Approximately 20 schools from each study location were stratified by the socioeconomic background of the school’s catchment area and randomly selected using probability proportional to school size. In the second stage, children and adolescents were randomly selected from the school’s register and asked to participate in the study. The overall participation rate was 77.4%, and the total population consisted of 4072 participants (9 years, 1066 girls and 1042 boys; 15 years, 1038 girls and 926 boys).
Cardiorespiratory fitness
Cardiorespiratory fitness, defined as maximal power output per kilogram (Wmax/kg), was indirectly determined by a cycle test with progressively increasing workload using an electronically braked cycle ergometer (Monark 839 Ergomedic; Monark, Vansbro, Sweden). Initial and incremental workloads were 20 W for children weighing less than 30 kg and 25 W for children weighing 30 kg or more. For 15 year old girls and boys, the initial and incremental workloads were 40 W and 50 W respectively. The workload was increased every three minutes until the maximal effort of the participants was reached. Heart rate was registered continuously (Polar Vantage, Kempele, Finland) throughout the test. Criteria defined for a maximal effort were heart rate ⩾185 beats/min and a subjective judgment by the observer that the participant could no longer continue, even after encouragement. These criteria eliminated 421 participants from further analysis. The cycle ergometer was electronically calibrated once every test day and mechanically calibrated after being moved. Maximal power output (Wmax) was calculated according to the following formula 14:
Wmax = W1 + (W2t/180)
where W1 = workload at the fully completed stage, W2 = workload increment at the final incomplete stage, and t = time (seconds) at the final incomplete stage.
The test was validated against direct measurement of Vo2max in 42 children aged 9 and 262 adolescents. Correlations between maximal power output and Vo2max were 0.89 in both the 9 year olds and adolescents. Reproducibility of Wmax and Vo2max was tested in 35 participants. No difference was found in Wmax between the two tests: 235.8 W in the first and 235.6 W in the second (r = 0.95). The difference in Wmax between the two tests was not related to the absolute level of Wmax.15 The correlation between Vo2max measurements in the two tests was 0.96, but Vo2max was 0.1 litres/min higher in the first test (p<0.01).
Anthropometry
Height was measured to the nearest millimetre. Body mass was measured to the nearest 0.1 kg using a calibrated beam balance weight. Body mass index was calculated using body mass divided by height squared (kg/m2). The sum of the thickness of four skinfolds (triceps, biceps, subscapular, and suprailiac) was measured using a Harpenden caliper and expressed in millimetres.16 Two measurements were taken at each position. If the difference between the two measurements was more than 2 mm, a third measurement was taken. The mean value of the two closest measurements was used for analysis. Waist circumference was measured with a metal anthropometric tape midway between the lower rib margin and the iliac crest, at the end of a gentle expiration.
Pubertal stage
Pubertal stage was assessed as described by Tanner,17 and the judgment made by a doctor or exercise physiologist. However, in the Norwegian 15 year old cohort, both self report (all) and test leader assessment (in 167 participants) were used. There was good agreement between self assessment and test leader assessment (κ = 0.80).
Resting blood pressure
Blood pressure was measured automatically using a Dinamap XL Vital Signs blood pressure monitor (Critikron, Inc, Tampa, Florida, USA). The Dinamap XL has been validated for use with children.18 The subject was seated and the appropriate sized cuff (either child or adult) was placed around the left upper arm. The Dinamap XL was programmed to take five measurements at two minute intervals. For all analysis the mean value of the last three measurements was used.
Data analysis
For all analyses, the Statistical Package for the Social Sciences (SPSS) version 11.0 was used. The univariate general linear model was used to test for interaction. If interaction was found for sex and age, the analysis was conducted for each group separately. Linear regression analysis was conducted to find the graded relation between the independent variable (cardiorespiratory fitness) and the dependent variables (sum of four skinfolds, waist circumference, and systolic and diastolic blood pressure). There were differences between countries with respect to sum of skinfolds, waist circumference, blood pressure, and cardiorespiratory fitness. We therefore constructed dummy variables for each country for adjustment. As puberty is known to influence both the dependent variables and cardiorespiratory fitness, all analyses were adjusted for pubertal stage. We analysed the different dependent variables and entered cardiorespiratory fitness as the independent variable with adjustment for sex, pubertal stage, age, and country. To analyse if the relation was linear or curvilinear, a squared factor of the cardiorespiratory fitness was entered into the model. The constants for the second degree polynomial equation y = a + bx + cx2 + (d×sex + e×pubertal stage + f×dummies for country) formed the basis of the curves. Partial correlations were calculated for all independent variables. Finally, the model was tested for cardiorespiratory fitness in the third degree term to check how robust the models were.
RESULTS
Table 1 presents descriptive variables of the study population. There was a strong relation between cardiorespiratory fitness and waist circumference after adjustment for country and pubertal stage for the 9 year old girls (r = 0.70, p<0.001), the 9 year old boys (r = 0.62, p<0.001), the 15 year old girls (r = 0.52, p<0.001), and the 15 year old boys (r = 0.50, p<0.001). Derivation of the second degree polynomial equation for the 9 year old girls (y = 63.0 − 16.0x + 1.9x2), the 9 year old boys (y = 81.0 − 20.3x + 2.5x2), the 15 year old girls (y = 68.7 − 17.8x + 2.5x2), and the 15 year old boys (y = 95.7 − 23.7x + 2.7x2) gave a significant non-linear relation. R2 for cardiorespiratory fitness was 20–26% in waist circumference in the 9 year olds. In the 15 year old girls and boys, the cardiorespiratory fitness explained 9% and 17% respectively of the variance in waist circumference. Pubertal stage explained about 15% of the variation in waist circumference in the 9 year old girls, 0% in the 9 year old boys, 6% in 15 year old girls, and 2% in the 15 year old boys. The third degree variable was significant for waist circumference in 9 year old girls only, and it only explained 0.2% of the variance.
Descriptive variables by age and sex
Figures 1 and 2 show the relation between cardiorespiratory fitness and the sum of four skinfolds (9 year olds, r = 0.67, p<0.001; 15 year olds, r = 0.68, p<0.001). These relations were curvilinear in the 9 year olds (y = 83.8 − 50.4x + 5.9x2) and 15 year olds (y = 93.3 − 39.3x + 3.5x2). The percentage explained variance from cardiorespiratory fitness was 24% for the 9 year olds, and about 11% for the 15 year olds. Pubertal stage explained to a lesser extent the variance of the sum of four skinfolds (9 year olds, 5%; 15 year olds, <1%).

Graded relation between sum of skinfolds and cardiorespiratory fitness in 9 year old boys and girls.

Graded relation between sum of skinfolds and cardiorespiratory fitness in 15 year old boys and girls.
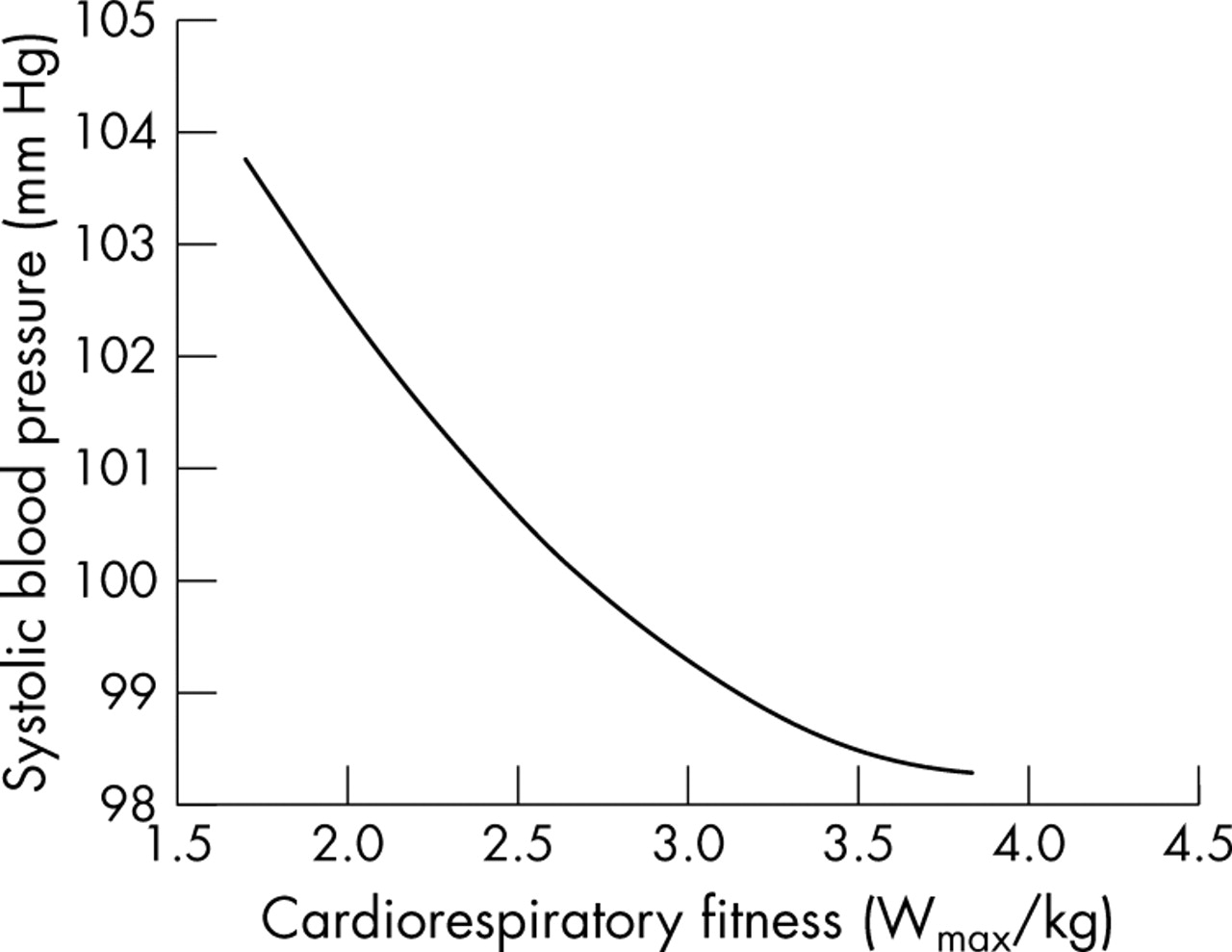
Figures 3 and 4 show the relation between cardiorespiratory fitness and systolic blood pressure for 9 and 15 year olds respectively. The systolic blood pressure showed a curvilinear relation with cardiorespiratory fitness for both age groups (9 year olds, total r = 0.43, p<0.001; 15 year olds, total r = 0.49, p<0.001). The equation for the 9 year olds was y = 92.9 − 8.4x + 1.0x2, and for the 15 year olds y = 106.7 − 11.4x + 1.5x2. Cardiorespiratory fitness explained 2% in both 9 and 15 year olds, whereas the variables pubertal stage and country explained a further 16% in 9 year olds and 22% in 15 year olds of the model.

Graded relation between systolic blood pressure and cardiorespiratory fitness in 9 year old boys and girls.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graded relation between systolic blood pressure and cardiorespiratory fitness in 15 year old boys and girls.
With regard to the diastolic blood pressure, there was no interaction with age group, therefore the two age groups were analysed together in the polynomial regression (y = 45.0 − 3.7x + 0.4x2). The percentage contribution to the variance from cardiorespiratory fitness was less than 1%, whereas the combination of sex, pubertal stage, and country contributed an additional 19%.
DISCUSSION
This study evaluated the graded associations between cardiorespiratory fitness and health outcome variables including waist circumference, skinfolds, and blood pressure. Our results show a strong graded relation between cardiorespiratory fitness and anthropometrical measures (waist circumference and sum of four skinfolds), and the relation was curvilinear. The relation between cardiorespiratory fitness and systolic blood pressure in both age groups and diastolic blood pressure in the whole group were also shown to be curvilinear. The third degree term of the fitness variable, which could indicate a more complex association than a second order polynomial, was only significant for waist circumference in 9 year old girls and only explained 0.2% of the variation in waist circumference. Hence the curvilinear relations were robust, as was found in both sexes and both age groups.
The results in terms of the anthropometrical variables show a consistent and strong relation with cardiorespiratory fitness, which has also been reported earlier in children and adolescents.19–22 However, none of these studies analysed whether the association was curvilinear. The strongest relation was seen for waist circumference. Waist circumference can be an indicator of visceral adiposity, which has been shown to relate to an unfavourable lipid profile23 and blood pressure24 in children and adolescents. Results from the Muscatine study25 have pointed out that children who improve their cardiorespiratory fitness during childhood have less overall adiposity and less abdominal adiposity than their counterparts during adolescence. Participation in vigorous physical activities has been shown to relate inversely to fat deposition in male adolescents.26
Diastolic and systolic blood pressure were significantly related to cardiorespiratory fitness, with a somewhat weaker association for diastolic than systolic blood pressure. These results are in accordance with those of Hansen et al,27 Andersen,28 and Boreham et al.29 The association was weak, but may be clinically relevant. The difference in systolic blood pressure between the subjects with low and high fitness was 6 mm Hg. According to the Framingham studies, this difference could account for about 20% difference in cardiovascular disease rates in adults.30
What is already known on this topic
-
A beneficial association between cardiorespiratory fitness and different measures of body composition and blood pressure has been observed in children and adolescents
-
Studies analysing the graded relation between cardiorespiratory fitness, obesity, and blood pressure are lacking in this population
What this study adds
-
This study is the first to show that there is a curvilinear graded relation between cardiorespiratory fitness and waist circumference, sum of skinfolds, and systolic blood pressure in children and adolescents
-
The greatest difference was observed between low and moderate fitness
In this study, we analysed the association between physical fitness and selected health outcomes. However, an intervention would be targeting behavioural changes, namely physical activity. Therefore a discussion of the association between physical activity and physical fitness is appropriate. The relation between physical activity and cardiorespiratory fitness is found to be stronger in adults than in children and adolescents.31 In a review, Morrow and Freedson32 reported that in 17 out of 37 studies the authors suggested a small to moderate relation (median correlation r = 0.17) between cardiorespiratory fitness and physical activity in the adolescent population. Somewhat higher correlations have been found in other studies.33,34 The reasons for these relatively poor relations are probably at least partly related to difficulties with measuring physical activity. In addition, genetics is believed to explain 25–40% of the variation in cardiorespiratory fitness.35 Nevertheless, there is evidence that suggests that cardiorespiratory fitness is likely to be associated with physical activity levels in children and adolescents.36,37 In the light of the present results which identify the health impact of small increases in cardiorespiratory fitness at the lower levels, it is important that initiatives should be put forward to promote physical activity.
In this relatively large and representative cohort of children and adolescents, a curvilinear relation was found between cardiorespiratory fitness and health parameters. Therefore the greatest benefit may be achieved when increasing the fitness from low to moderate. It is therefore important to direct action towards those children and adolescents who are the least physically fit.
Acknowledgments
This study was supported by the following grants. Denmark: Danish Heart Foundation, Danish Medical Research Council, Health Foundation, Danish Council for Sports Research, Foundation of 17-12-1981, Foundation in Memory of Asta Florida Bolding née Andersen. Estonia: Estonian Science Foundation grant nos 3277 and 5209. Norway: Norwegian Council of Cardiovascular Diseases. Portugal: European Social Fund.
REFERENCES
Commentary
This study focuses on an important issue and adds information about children’s exercise and risk factors for non-communicable diseases. Further, it uses a large sample from a joint European project, which should be highlighted.
Footnotes
-
Competing interests: none declared