Article Text

Abstract
Objective Gestational diabetes mellitus (GDM), gestational hypertension (GH) and pre-eclampsia (PE) are associated with short and long-term health issues for mother and child; prevention of these complications is critically important. This study aimed to perform a systematic review and meta-analysis of the relationships between prenatal exercise and GDM, GH and PE.
Design Systematic review with random effects meta-analysis and meta-regression.
Data sources Online databases were searched up to 6 January 2017.
Study eligibility criteria Studies of all designs were included (except case studies) if published in English, Spanish or French, and contained information on the Population (pregnant women without contraindication to exercise), Intervention (subjective or objective measures of frequency, intensity, duration, volume or type of exercise, alone [“exercise-only”] or in combination with other intervention components [e.g., dietary; “exercise + co-intervention”]), Comparator (no exercise or different frequency, intensity, duration, volume and type of exercise) and Outcomes (GDM, GH, PE).
Results A total of 106 studies (n=273 182) were included. ‘Moderate’ to ‘high’-quality evidence from randomised controlled trials revealed that exercise-only interventions, but not exercise+cointerventions, reduced odds of GDM (n=6934; OR 0.62, 95% CI 0.52 to 0.75), GH (n=5316; OR 0.61, 95% CI 0.43 to 0.85) and PE (n=3322; OR 0.59, 95% CI 0.37 to 0.9) compared with no exercise. To achieve at least a 25% reduction in the odds of developing GDM, PE and GH, pregnant women need to accumulate at least 600 MET-min/week of moderate-intensity exercise (eg, 140 min of brisk walking, water aerobics, stationary cycling or resistance training).
Summary/conclusions In conclusion, exercise-only interventions were effective at lowering the odds of developing GDM, GH and PE.
- exercise
- pregnancy
- diabetes
- evidence-based review
- meta-analysis
Statistics from Altmetric.com
Introduction
In 2011, the American Heart Association Effectiveness-Based Guidelines for the Prevention of Cardiovascular Disease in Women listed pregnancy complications including pre-eclampsia (PE), gestational hypertension (GH) and gestational diabetes mellitus (GDM) as risk factors as strong as smoking for the future development of cardiovascular disease.1 The strength of this relationship is supported by evidence of elevated risk for future type 2 diabetes (risk ratio (RR) 7.43), hypertension (RR 3.70), ischaemic heart disease (RR 2.26) and stroke (RR 1.8) in the 5–15 years following delivery.2 3 Furthermore, GDM, GH and PE are also associated with adverse outcomes in the offspring, such as excessive or inadequate fetal growth, fetal growth restriction, preterm delivery, perinatal death and long-term metabolic and cardiovascular morbidity.4–6 Prevention of these disorders during pregnancy is therefore essential for the future health of two generations.
Gestational diabetes is defined as ‘glucose intolerance with onset or first recognition during pregnancy’ and affects up to 6%–9% of the obstetric population.7 Hypertensive disorders of pregnancy include GH and PE and affect 10% of women.8 Although the disorders are distinct, GDM, GH and PE are often superimposed.9 These disorders have similar risk factors (eg, obesity, insulin resistance, advanced maternal age, excessive gestational weight gain)8 10 and are associated with inflammation, vascular dysfunction, oxidative stress and vascular disease.6 Exercise is a cornerstone for prevention and treatment of hypertension and diabetes in general populations; however, the effectiveness of exercise in prevention during pregnancy is poorly understood.
International and national guidelines for exercise during pregnancy recommend that women without contraindications be physically active throughout pregnancy.11 12 The present systematic review and meta-analysis was conducted as part of a series of reviews which will form the evidence base for the development of the 2019 Canadian guideline for physical activity throughout pregnancy (herein referred to as Guideline).13 The purpose of this review was to evaluate the effect of prenatal exercise on the odds of developing GDM, GH and PE.
Methods
In October 2015, the Guidelines Consensus Panel assembled to identify priority outcomes for the Guidelines update. The Panel included researchers, methodological experts, a fitness professional and representatives from the Canadian Society for Exercise Physiology (CSEP), the Society of Obstetricians and Gynaecologists of Canada (SOGC), the College of Family Physicians of Canada, the Canadian Association of Midwives, the Canadian Academy of Sport and Exercise Medicine, Exercise is Medicine Canada and a representative health unit (the Middlesex-London Health Unit). The Guidelines Consensus Panel identified 20 ‘critical’ and 17 ‘important’ outcomes related to prenatal exercise and maternal/fetal health. Three of the ‘critical’ outcomes (ie, GDM, GH and PE) are examined in this review. This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, and the checklist was completed.14
Protocol and registration
Two systematic reviews examining the impact of prenatal exercise on fetal and maternal health outcomes were registered a priori with PROSPERO, the International Prospective Register of Systematic Reviews (fetal health: Registration No CRD42016029869; maternal health: Registration No CRD42016032376). Since the relationships between prenatal exercise and GDM, GH and PE were examined in studies related to both fetal and maternal health, records retrieved from the searches for both of these reviews were evaluated for inclusion in the present study.
Eligibility criteria
The PICOS (population, intervention, comparison, outcome, study design) framework15 was used to guide this review.
Population
The population of interest was pregnant women without absolute or relative contraindication to exercise as defined by the 2003 SOGC/CSEP Clinical Practice Guidelines for Exercise During Pregnancy.11 16 Absolute contraindications to exercise were defined as: ruptured membranes, premature labour, persistent second or third trimester bleeding, placenta previa, PE, GH, incompetent cervix, intrauterine growth restriction, high-order pregnancy, uncontrolled type 1 diabetes, hypertension or thyroid disease, or other serious cardiovascular, respiratory or systemic disorders. Relative contraindications to exercise were defined as: a history of spontaneous abortion, premature labour, mild/moderate cardiovascular or respiratory disease, anaemia or iron deficiency, malnutrition or eating disorder, twin pregnancy after 28 weeks or other significant medical conditions.11 16
Intervention (exposure)
The intervention/exposure was subjective or objective measures of frequency, intensity, duration, volume or type of exercise. Although exercise is a subtype of physical activity, for the purpose of this review we used the terms interchangeably. Exercise was defined as any bodily movement generated by skeletal muscles that resulted in energy expenditure above resting levels.17 Acute (ie, a single exercise session) or habitual (ie, usual activity) prenatal exercise, as well as interventions including exercise alone (termed ‘exercise-only’ interventions) or in combination with other interventions (such as diet; termed ‘exercise+co-interventions’), was considered. Studies were excluded if exercise was performed after the beginning of labour.
Comparison
Eligible comparators were: no exercise; different frequency, intensity, duration, volume or type of exercise; different intervention duration; or exercise in a different trimester.
Outcome
Relevant outcomes were GDM (as defined by individual study authors), GH (defined as diastolic blood pressure ≥90 mm Hg on at least two measurements at ≥20 weeks’ gestation, or as pregnancy-induced hypertension without additional specification) and PE (defined as GH combined with proteinuria).8
Study design
Primary studies of any design were eligible, except case studies. Narrative or systematic reviews and meta-analyses were excluded.
Information sources
A structured search was created and run by a research librarian using the Ovid interface (MEDLINE, EMBASE, PsycINFO, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials), the EBSCO interface (CINAHL Plus with Full-text, Child Development & Adolescent Studies, ERIC, Sport Discus), Scopus, Web of Science Core Collection, ClinicalTrials.gov and the Trip Database up to 6 January 2017. See the online supplement for complete search strategies.
Supplemental material
Study selection and data extraction
Titles and abstracts of all retrieved articles were independently screened by two reviewers. Abstracts that were judged to have met the initial screening criteria by at least one reviewer were retrieved as full-text articles. The article was reviewed for relevant PICOS information by at least one person. If it was deemed that the article did not meet the inclusion criteria, it was reviewed by MHD and/or SMR prior to exclusion. If agreement could not be reached by discussion, the study characteristics were presented to the Guidelines Steering Committee who oversaw the systematic reviews (MHD, MFM, SMR, CEG, VJP, AJG and NB) and a final decision regarding inclusion/exclusion was made by consensus. Studies that were selected were imported into DistillerSR (Evidence Partners, Ottawa, ON, Canada) for data extraction. At this point, studies from the maternal and fetal reviews that were included were deduplicated against one another in DistillerSR and were considered as one review from this point forward.
Data extraction tables were created in DistillerSR in consultation with methodological experts and the Guidelines Steering Committee. Data were extracted by one person; a content expert (MHD, MFM or SMR) then independently verified the extracted data. Reviewers were not blinded to study authors. For each single study, the most recent or complete version (publication) was selected as the ‘parent’ paper; however, relevant data from all publications related to each unique study were extracted. Study characteristics (ie, year, study design, country) and population characteristics (eg, number of participants, age, pre-pregnancy body mass index (BMI), parity and pregnancy complications), intervention/exposure (actual and/or prescribed exercise frequency, intensity, duration and type, duration of the intervention, measure of physical activity) and outcomes (GDM, GH and PE) were extracted (see online supplement table 1). If data were not available for extraction, the authors were contacted for additional information.
Quality of evidence assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework was used to assess the quality of evidence across studies for each study design and health outcome.
Evidence from randomised controlled trials (RCT) began with a ‘high’ quality of evidence rating and was graded down if there was a concern with the risk of bias, indirectness, inconsistency, imprecision or risk of publication bias because these factors reduce the level of confidence in the observed effects. Evidence from all non-randomised interventions and observational studies began with a ‘low’-quality rating and, if there was no cause to downgrade, was upgraded if applicable according to the GRADE criteria (eg, large magnitude of effect, evidence of dose–response).18
Specifically, the risk of bias in RCTs and intervention studies was assessed following the Cochrane Handbook19 and the risk of bias in observational studies was assessed using the characteristics recommended by Guyatt et al,20 which has been used by other Physical Activity Guidelines.21 All studies (RCTs, intervention studies and observational studies) were screened for potential sources of bias including selection bias (RCT/intervention: inadequate randomisation procedure; observational: inappropriate sampling), reporting bias (selective/incomplete outcome reporting), performance bias (RCT/intervention: compliance to the intervention; observational: flawed measurement of exposure), detection bias (flawed measurement of outcome), attrition bias (incomplete follow-up, high loss to follow-up) and ‘other’ sources of bias. Risk of bias across studies was rated as ‘serious’ when studies having the greatest influence on the pooled result (assessed using weight (%) given in forest plots or sample size in studies that were narratively synthesised) presented ‘high’ risk of bias. The greatest influence on the pooled result was determined as follows: the studies that had the greatest individual % contribution in the meta-analyses, when taken together, contributed to >50% of the weight of the pooled estimate. Serious risk of bias was considered when the sample size of studies that were narratively synthesised was similar to the total sample size of studies contributing to >50% of the weight of the pooled estimate in the meta-analyses. Given the nature of exercise interventions, it is not possible to blind participants to group allocation. Therefore, if the only source of bias was related to the blinding of allocation, the risk of bias was rated as ‘low’. Performance bias was rated as ‘high’ when <60% of participants performed 100% of prescribed exercise sessions or attended 100% of counselling sessions (defined as low compliance) or when compliance to the intervention was not reported. Attrition bias was rated as ‘high’ when >10% of data were missing at the end of the study and intention-to-treat analysis was not used. Due to time constraints and feasibility, one reviewer evaluated the quality of the evidence across each health outcome using the protocol and a second person reviewed the GRADE tables as a quality control measure.
Indirectness was considered serious when exercise-only interventions and exercise+cointerventions were combined for analysis or when the effect of exercise+cointervention on odds of GDM, GH or PE was assessed. Inconsistency was considered serious when heterogeneity was high (I2≥50%) or when only one study was assessed (I2 unavailable). Imprecision was considered serious when the 95% CI crossed the line of no effect, and was wide, such that interpretation of the data would be different if the true effect were at one end of the CI or the other. When only one study was assessed, imprecision was not considered serious as inconsistency was already considered serious for this reason. Finally, in order to assess publication bias, funnel plots were created if at least 10 studies were included in the forest plot (see online supplement figures 25–39). If there were fewer than 10 studies, publication bias was deemed non-estimable and not rated down. Quality of evidence assessment is presented in online supplement tables 2–4.
Statistical analysis
Statistical analyses were conducted using Review Manager V.5.3 (Cochrane Collaboration, Copenhagen, Denmark). ORs were calculated for all dichotomous outcomes. Significance was set at p<0.05. Inverse-variance weighting was applied to obtain OR using a random effects model. Meta-analyses were performed separately by study design. For RCTs and non-randomised interventions, sensitivity analyses were performed to evaluate whether the effects were different when examining relationships between exercise-only interventions versus exercise+cointerventions and GDM, GH and PE. Exercise-only studies could include standard care. When possible, the following a priori determined subgroup analyses were conducted for exercise-only interventions and observational studies: (1) women diagnosed with diabetes (gestational, type 1 or type 2) compared with women without diabetes (named ‘general population’); (2) samples of women with overweight or obesity (mean BMI >25.0 kg/m2) prior to pregnancy compared with samples of women who were of various BMI (mean BMI <25 kg/m2 but possibly with some individuals with BMI >25.0 kg/m2; named ‘general population’); (3) women >35 years of age compared with women <35 years of age; (4) women who were previously inactive compared with those who were previously active (as defined by individual study authors). Tests for subgroup differences were conducted, with statistical significance set at p≤0.05. Only when statistically significant differences were found subgroup differences were interpreted. If a study did not provide sufficient detail to allow it to be grouped into the a priori subgroups, then a third group called ‘unspecified’ was created. The I-squared (I2) was calculated to indicate the per cent of total variability that was attributable to between-study heterogeneity. In studies where there were no observed events in the intervention or control group, data were entered into forest plots, but were considered ‘not estimable’ and excluded from the pooled analysis as per the recommendation in the Cochrane Handbook.22 In order to identify a clinically meaningful decrease in GDM, GH and PE, dose–response meta-regression23–25 was carried out by weighted no-intercept regression of log OR with a random effects for study, using the metafor 26 package in R27 V.3.4.1. It was determined that an accepted cut-point for a clinically meaningful decrease does not exist in the literature. As such, a reduction of 25% was chosen based on expert opinion. Models did not include an intercept term since the log OR is assumed to be zero when the exercise dose is zero. Restricted cubic splines with knots at the 10th, 50th and 90th percentiles of the explanatory variable28 were used to investigate whether there was evidence for a non-linear relationship. Fitting was performed by maximum likelihood, and non-linearity was assessed using a likelihood ratio test. When the model was statistically significant at p<0.05, the minimum exercise dose to obtain a clinically significant benefit was estimated by the minimum value of the explanatory variable at which the estimated OR was less than 0.75. Finally, subgroup analyses were conducted for exercise-only RCTs to identify whether a specific type of exercise was associated with greater benefit.
For outcomes or for subsets of studies where a meta-analysis was not possible, a narrative synthesis of the results was presented, organised around each outcome. Within each outcome, results were presented by study design. Unless otherwise specified, studies were not included in meta-analyses if data were incomplete (SD, SE or number of cases/controls not provided), if data were adjusted for confounding factors, or if the study did not include a non-exercising control group. In studies where data were included in the meta-analysis but additional information was available, the studies were included in both the meta-analysis and narrative synthesis.
Results
Study selection
The initial search was not limited by language. However, the Guidelines Steering Committee decided to exclude studies published in languages other than English, Spanish or French for feasibility reasons. A PRISMA diagram of the search results, including reasons for exclusion, is shown in figure 1. A comprehensive list of excluded studies is presented in the online supplement. The results of the meta-regression analysis are presented in the online supplement (Meta-regressions).

Flow diagram of studies selected for the present study. *Eighty-nine papers included in quantitative synthesis but three were from the same cohort study and counted as one unique study. #Five studies were included in both the qualitative and quantitative synthesis.
Study characteristics
Overall, 106 unique studies (n=273 182 women) from 27 countries and five continents were included. There were 65 RCTs, 9 non-RCTs, 13 cohort, 11 cross-sectional and 8 case–control studies. Among the included exercise interventions, the frequency of exercise ranged from 1 to 7 days/week, the duration of exercise ranged from 10 to 90 min per session, and the types of exercise included walking, swimming, cycling, water gymnastics, resistance training, stretching, yoga or pelvic floor muscle training. Additional details about the studies can be found in the online supplement (Study Characteristics and online supplement table 1). No studies looked at the effect of exercising in different trimesters on the odds of developing GDM, GH or PE. The results of the RCTs are presented below; the results of other study designs are presented in the online supplement.
Quality of evidence
Overall, the quality of evidence ranged from ‘very low’ to ‘high’ (see online supplement tables 2–4). The most common reasons for downgrading the quality of evidence were (1) serious risk of bias that reduced the level of confidence in the observed effects, and (2) indirectness of the interventions being assessed. Common sources of bias included poor or unreported compliance with the intervention and inappropriate treatment of missing data when attrition rate was high.
Synthesis of data
Gestational diabetes mellitus
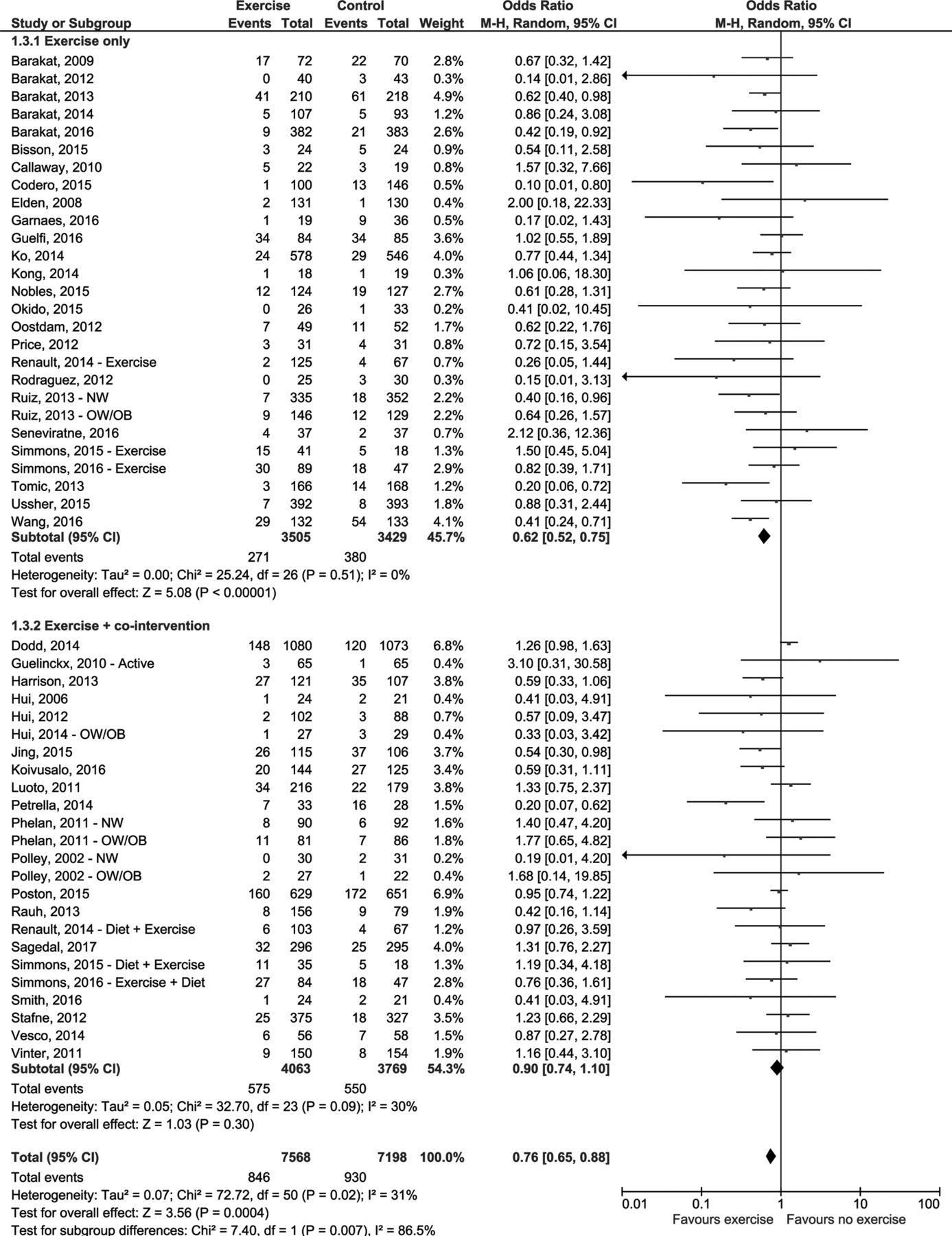
Overall, there was ‘low’-quality evidence from 46 RCTs (n=14 923) regarding the association between prenatal exercise and GDM.29–74 The quality of evidence was downgraded from ‘high’ to ‘low’ because of serious risk of bias and serious indirectness of the interventions. Overall, prenatal exercise was associated with 24% lower odds of developing GDM compared with no exercise (pooled estimate based on 45 RCTs, n=14 823; OR 0.76, 95% CI 0.65 to 0.88, I2=31%, figure 2).29–73 The one additional study74 that could not be included in the meta-analysis (no statistics provided) indicated there were no differences in GDM between women randomised to an intensive dietary and lifestyle counselling programme, including recommendations about physical activity (n=57), and those randomised to routine prenatal care (n=43) (online supplement table 1).
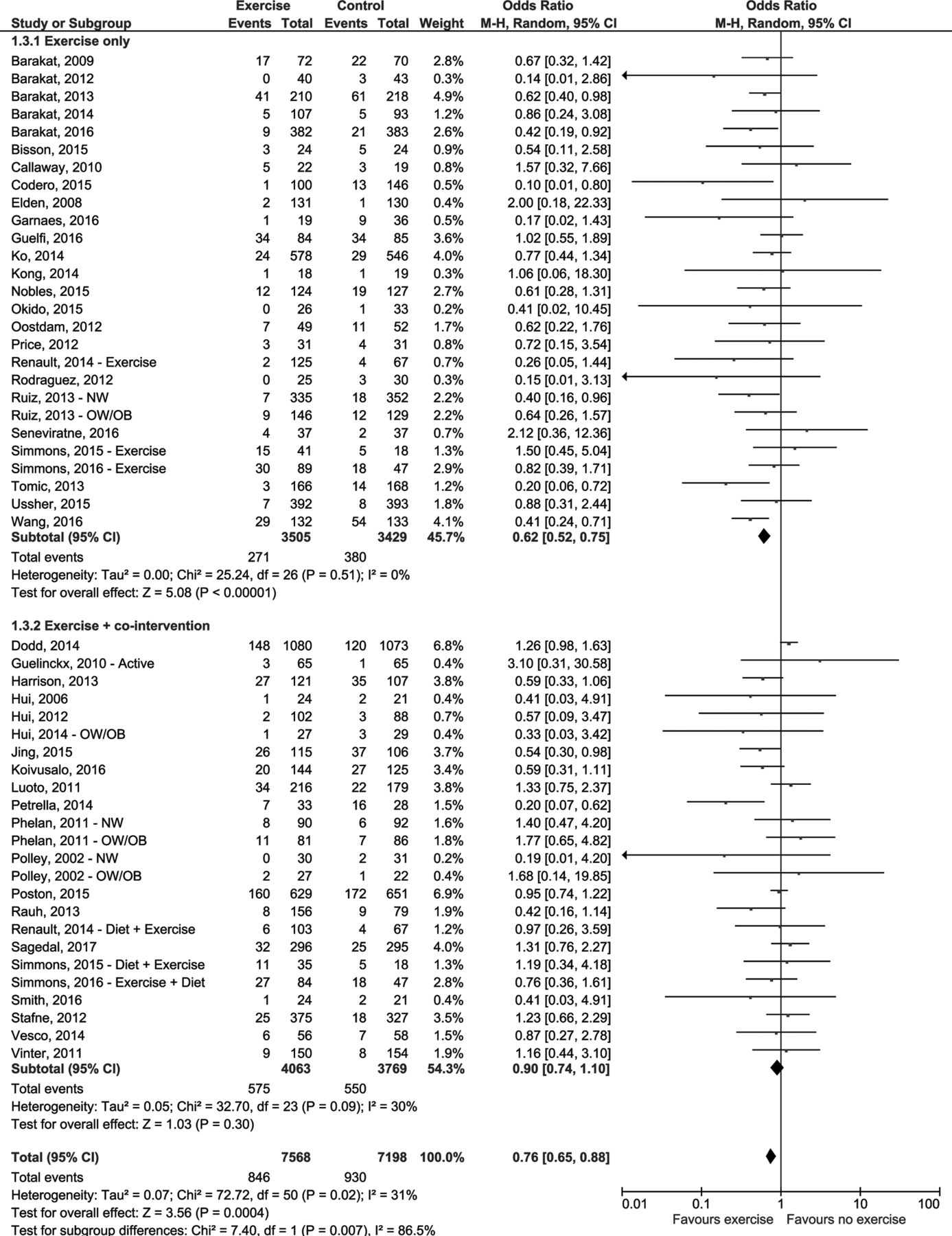
Effects of prenatal exercise compared with control on odds of gestational diabetes mellitus (RCTs). Sensitivity analyses were conducted with studies including exercise-only interventions and those including exercise +co- interventions. Analyses conducted with a random effects model. CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel method. Active: women who were previously active; Exercise: exercise arm of the intervention; Exercise + co-intervention; NW: subgroup of normal weight women; OW/OB: subgroup of women with overweight/obesity.
Sensitivity analysis
The pooled estimate for the exercise-only interventions was significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.007). Specifically, exercise-only interventions reduced the odds of developing GDM by 38% compared with no exercise (26 RCTs, n=6934; OR 0.62, 95% CI 0.52 to 0.75, I2=0%; ‘moderate’-quality evidence, downgraded due to serious risk of bias, figure 2).29–54 There was no statistically significant difference for those participating in exercise+cointerventions (figure 2).
Subgroup analyses
The tests for subgroup differences performed for exercise-only interventions were not statistically significant (see online supplement figures 1–4).
Observational studies
Findings from non-randomised interventions,75–80 cohort81–95 and cross-sectional96–102 studies were consistent with the findings from RCTs. The findings from case–control studies showed no significant relationship between prenatal exercise and GDM but had a point estimate similar to that from other study types103–105 (see the online supplement for more details and online supplement figures 5–8).
Gestational hypertension
Overall, there was ‘low’-quality evidence from 34 RCTs (n=9755) regarding the association between prenatal exercise and GH.29 31–38 41–43 45 46 50 51 56 59 60 63 66 68–70 106–115 The quality of evidence was downgraded from ‘high’ to ‘low’ because of serious risk of bias and serious indirectness of the interventions. The pooled estimate based on 32 RCTs (n=9648) indicated 19% lower odds of GH with exercise compared with no exercise (OR 0.81, 95% CI 0.65 to 1.00, I2=8%, figure 3).29 31–38 41–43 45 46 50 51 56 59 60 63 66 68–70 106–111 113 114 Two superiority trials (n=107) could not be entered into the meta-analysis because they did not include a control group (online supplement table 1). In one of these studies, Yeo et al 112 reported GH incidence to be 22% (95% CI 8.7 to 35.2) in women randomised to a walking intervention (n=41) and 40% (95% CI 23.2 to 55.8) in those randomised to a stretching intervention (n=38). In the other study, McAuley et al 115 reported two cases of GH in each intervention group (aerobic and muscular exercise group (n=14) and muscular exercise group (n=14)).

Effects of prenatal exercise compared with control on the odds of gestational hypertension (RCTs). Sensitivity analyses were conducted with studies including exercise-only interventions and those including exercise +co- interventions. Analyses conducted with a random effects model. CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel method. Active: women who were previously active; Exercise: exercise arm of the intervention; NW: subgroup of normal weight women; Non-Diabetic: subgroup of non-diabetic women; OW/OB: subgroup ofwomen with overweight/obesity. PE/GH:PE/GH combined as the outcome; Type 1 Diabetic: subgroup of type 1 diabetic women. Note: studies with zero events in both arms are included in the forest plot but are "not estimable" and not included in the pooled analysis.
Sensitivity analysis
The pooled estimate for the exercise-only interventions was significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.04). Specifically, exercise-only interventions reduced the odds of developing GH by 39% (22 RCTs, n=5316; OR 0.61, 95% CI 0.43 to 0.85, I2=0%; ‘high’-quality evidence, figure 3).29 31–38 41–43 45 46 50 51 106–111 There was no statistically significant difference for those participating in exercise+cointerventions (figure 3).
Subgroup analysis
The tests for subgroup differences performed for exercise-only interventions were not statistically significant (see online supplement figures 9–12).
Observational studies
Findings from non-randomised interventions 78 79 116 117 were consistent with findings from RCTs. The findings from cohort82 84 85 88 89 91 92 118 or cross-sectional96 119–122 studies showed no significant relationship between prenatal exercise and GH but had a point estimate similar to that from other study types (see the online supplement for more details, and online supplement figures 13–16).
Pre-eclampsia
Overall, there was ‘low’-quality evidence from 27 RCTs (n=10 256) indicating no association between prenatal exercise and PE.30 36 38 42 43 45 46 50 52 56 58–60 63 64 68–71 107 110 112 123–127 The quality of evidence was downgraded from ‘high’ to ‘low’ because of serious risk of bias and serious indirectness of the interventions. The pooled estimate was based on 26 RCTs (n=10 177; OR 0.89, 95% CI 0.73 to 1.08, I2=0%, figure 4).30 36 38 42 43 45 46 50 52 56 58–60 63 64 68–71 107 110 123–127 The one superiority exercise-only trial could not be entered into the meta-analysis because it did not include a control group (see online supplement table 1). Yeo et al 112 reported that PE incidence was 14.6% (95% CI 5.6 to 29.2) among women in a walking group (n=41) and 2.6% (95% CI 0.07 to 13.8) among those in a stretching group (n=38).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of prenatal exercise compared with control on odds of preeclampsia (RCTs). Sensitivity analyses were conducted with studies includinge xercise-only interventions and those including exercise +co- interventions. Analyses conducted with a random effects model. CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel method. NW: subgroup of normal weight women; OW/OB: subgroup of women with overweight/obesity; 13 weeks: subgroup of women who initiated exercise at 13 weeks of pregnancy; 20 weeks: subgroup of women who initiated exercise at 20 weeks of pregnancy. Note: studies with zero events in both arms are included in the forest plot but are "not estimable" and not included in the pooled analysis.
Sensitivity analysis
The pooled estimate for the exercise-only interventions was not significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.05). However, exercise-only interventions reduced the odds of developing PE by 41% (16 studies, n=3401; pooled estimate based on 15 studies, n=3322; OR 0.59, 95% CI 0.37 to 0.94, I2=0%; ‘moderate’-quality evidence, downgraded due to serious risk of bias, figure 4).30 36 38 42 43 45 46 50 52 107 110 123–126 There was no statistically significant difference for those participating in exercise+cointerventions (figure 4).
Subgroup analysis
The tests for subgroup differences performed for exercise-only interventions were not statistically significant (see online supplement figures 17–20).
Observational studies
Findings from cohort83 86–88 91 92 118 128–130 and case–control studies131–134 were consistent with findings from RCTs. The findings from non-randomised interventions78–80 135 and cross-sectional studies101 121 showed no significant relationship between prenatal exercise and PE but had a point estimate similar to that from other study types (see the online supplement for more details, and online supplement figures 21–24).
Meta-regressions
Meta-regression analysis using linear and spline regression was conducted for each outcome. Linear models were presented unless the fit of the spline was significantly better (p<0.05). Minimum exercise thresholds required to achieve a clinically meaningful reduction (ie, 25%) in health outcomes were identified. GDM (see online supplement figures 28–32): 2.9 METs (light intensity), 25.3 min, 2.1 days/week or 590.6 MET-min/week; GH (see online supplement figures 33–37): 3.2 METs (moderate intensity), 23.5 min, 3.1 days/week or 401.1 MET-min/week; PE (see online supplement figures 38–42): 3.2 METs (moderate intensity), 18.3 min, 2.5 days/week or 260.0 MET-min/week.
Discussion
In this comprehensive systematic review of 106 studies, there was ‘moderate’ to ‘high’-quality evidence from exercise-only RCTs indicating exercise was associated with a 38% decrease in the odds of developing GDM (26 RCTs, n=6934), 39% for developing GH (22 RCTs, n=5316) and 41% for developing PE (15 RCTs, n=3322). To achieve at least a 25% reduction in the odds of developing GDM, PE and GH, pregnant women need to accumulate at least 600 MET-min/week of moderate-intensity exercise (eg, 140 min of brisk walking, water aerobics, stationary cycling or resistance training). Results from meta-regression analyses suggested that the benefits would be attained when exercise is performed at a frequency of at least 3 days/week or at least 25 min per session. Accumulated exercise volumes above 600 MET-min/week were associated with a greater reduction in the odds of developing these gestational diseases. Our systematic review and meta-analysis builds on the work of recently published meta-analyses to include 59 new RCTs and observational studies concerning GDM (41 284 additional women),25 12 new RCTs concerning GH (2055 additional women)136 and 23 new RCTs and observational studies concerning PE (91 422 additional women).136 137
Our findings demonstrated lower odds of developing GDM, GH and PE with exercise-only interventions compared with no exercise. In contrast, interventions combining exercise+cointerventions were less effective than exercise alone for GDM (p=0.007), GH (p=0.04) and PE (p=0.05). These studies were typically counselling interventions about healthy lifestyle (including diet and physical activity) in pregnant women with overweight or obesity. In these interventions, women were unsupervised during exercise, and 67% of studies reported poor compliance (defined as <60% of participants performing 100% of the prescribed exercise sessions). Supervision has been suggested to be critical for compliance and the effect of the intervention.138 Compliance to the exercise intervention may therefore be a critical determinant of the protective effect of exercise on GDM and hypertensive disorders of pregnancy; this might be related to actually carrying out the intervention as intended. Although many studies reported poor compliance to the prescribed intervention, our findings demonstrated a substantial reduction in the risk of developing GDM, GH and PE. This suggests that the protective effect of exercise against these diseases may be even greater in women who are compliant to exercise.
Findings from other study designs were not always in agreement with those from RCTs. This inconsistency may be due, at least in part, to the method used to assess physical activity. Indeed, the quality of the evidence from the majority of observational studies was rated down because of risk of bias related to performance bias, specifically due to potentially flawed measurement of the physical activity. Unmeasured confounding variables might also explain different findings according to study design since subgroup analyses performed on exercise-only interventions clearly showed that the effect of prenatal exercise differs according to some characteristics of the women.
GDM and hypertensive disorders of pregnancy share several similar risk factors and pathophysiological features, such as maternal obesity, inflammation, insulin resistance, excessive gestational weight gain or impaired vascular function.6 8 10 It is therefore possible that some of the mechanisms underlying the association between prenatal exercise and the prevention of these conditions involve the prevention of excessive gestational weight gain,139 improvements in skeletal muscle insulin sensitivity and glucose uptake,140 141 or a reduction in oxidative stress and associated improvement in endothelial function.142 Abnormal placental development is also involved in the pathophysiology of PE, and it has been suggested that exercise promotes placental growth and vascular development.142
Women who develop GDM and hypertensive disorders of pregnancy are at long-term risk for type 2 diabetes,3 5 hypertension143 and cardiovascular diseases.144 Furthermore, offspring of women who develop these conditions are at increased risk for obesity, metabolic and cardiovascular diseases later in life.4 5 Lower odds of developing GDM and hypertensive disorders of pregnancy with prenatal exercise as we reported, therefore, have major implications for the long-term health of both women and children.
Rigorous methodological standards (GRADE) were used to guide the systematic review process, grey literature was examined, and articles in different languages were included. Twenty-seven countries from five continents were represented in the included studies. The level of quality evidence from RCTs was rated down mainly because of risk of bias and indirectness of the interventions. In future studies, more attention should be paid to monitoring compliance with exercise interventions, and to considering factors that may influence compliance and retention of study participants. More exercise-only interventions among pregnant women who are overweight or obese, diagnosed with GDM, compared supervised with unsupervised exercise, and previously inactive women are also needed to adequately power these subgroup analyses. Additional studies regarding the potential impact of specific types of exercise, timing of initiation of exercise and potential role of other mediating factors such as gestational weight gain are also strongly encouraged. Finally, no studies looked at the effect of exercising in different trimesters on the odds of developing GDM, GH or PE. Future studies addressing this question are also needed to establish the optimal time point to start an exercise intervention.
In conclusion, exercise-only interventions were effective at lowering the odds of developing GDM, GH and PE.
What is already known on this topic?
Gestational diabetes mellitus (GDM), gestational hypertension (GH) and pre-eclampsia (PE) are associated with short and long-term health issues for mother and child; prevention of these complications is therefore critically important.
Exercise is a cornerstone for prevention and treatment of hypertension and diabetes in general populations; however, the effectiveness of exercise in prevention during pregnancy is poorly understood.
What are the new findings?
Exercise-only interventions reduced the odds of developing GDM by 38%, GH by 39% and PE by 41%.
To achieve at least a 25% reduction in the odds of developing GDM, PE and GH, pregnant women need to accumulate at least 600 MET-min/week of moderate-intensity exercise (eg, 140 min of brisk walking, water aerobics, stationary cycling or resistance training).
Acknowledgments
The authors acknowledge the Canadian Institute of Health Research–Knowledge Translation Grant. The authors thank Bailey Shandro (UAlberta), Anne Courbalay (UQTR) and Meghan Sebastianski (Alberta SPOR SUPPORT Unit Knowledge Translation Platform), University of Alberta, for their assistance with the meta-analysis. The authors acknowledge Mary Duggan from the Canadian Society for Exercise Physiology who is one of the primary knowledge users.
References
Footnotes
MHD and S-MR contributed equally.
Contributors MHD, SMR, MFM, GAD and KBA conceived the study. MHD, SMR, MFM, VJP, AJG, CEG, NB and LS wrote the study protocol. MHD, SMR, RJS, VLM, LR, FS, MJ, AJK, AAM and TSN selected the studies. RJS, VLM, LR, FS, MJ, AJK, AAM, TSN, AW and NB extracted and analysed the data. MHD, SMR and MFM checked the extracted data. SMR and MHD wrote the first draft of the manuscript and all authors contributed to the writing of the final version.
Funding This study was funded by the Canadian Institute of Health Research Knowledge Synthesis Grant. MHD is funded by an Advancing Women’s Heart Health Initiative New Investigator Award supported by Health Canada and the Heart and Stroke Foundation of Canada. RJS is funded by a Canadian Institutes for Health Research Doctoral Research Award. AAM is funded by a Fonds de Recherche en Santé du Québec Doctoral Research Award.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.