Article Text

Abstract
Background The effectiveness of exercise referral schemes (ERS) is influenced by uptake and adherence to the scheme. The identification of factors influencing low uptake and adherence could lead to the refinement of schemes to optimise investment.
Objectives To quantify the levels of ERS uptake and adherence and to identify factors predictive of uptake and adherence.
Methods A systematic review and meta-analysis was undertaken. MEDLINE, EMBASE, PsycINFO, Cochrane Library, ISI WOS, SPORTDiscus and ongoing trial registries were searched (to October 2009) and included study references were checked. Included studies were required to report at least one of the following: (1) a numerical measure of ERS uptake or adherence and (2) an estimate of the statistical association between participant demographic or psychosocial factors (eg, level of motivation, self-efficacy) or programme factors and uptake or adherence to ERS.
Results Twenty studies met the inclusion criteria, six randomised controlled trials (RCTs) and 14 observational studies. The pooled level of uptake in ERS was 66% (95% CI 57% to 75%) across the observational studies and 81% (95% CI 68% to 94%) across the RCTs. The pooled level of ERS adherence was 49% (95% CI 40% to 59%) across the observational studies and 43% (95% CI 32% to 54%) across the RCTs. Few studies considered anything other than gender and age. Women were more likely to begin an ERS but were less likely to adhere to it than men. Older people were more likely to begin and adhere to an ERS.
Limitations Substantial heterogeneity was evident across the ERS studies. Without standardised definitions, the heterogeneity may have been reflective of differences in methods of defining uptake and adherence across studies.
Conclusions To enhance our understanding of the variation in uptake and adherence across ERS and how these variations might affect physical activity outcomes, future trials need to use quantitative and qualitative methods.
- Exercise referral schemes
- physical activity
- primary care
- uptake
- adherence
- systematic reviews
- meta analysis
- public health
- health behaviour
- ageing
- mental health
- exercise
- epidemiology
- health promotion
Statistics from Altmetric.com
- Exercise referral schemes
- physical activity
- primary care
- uptake
- adherence
- systematic reviews
- meta analysis
- public health
- health behaviour
- ageing
- mental health
- exercise
- epidemiology
- health promotion
Background
Primary care is a key potential setting for the promotion of physical activity.1 One popular primary care-based model of promoting physical activity interventions is the exercise referral scheme (ERS). First established in the early 1990s,2 the number of schemes in the UK has grown to over 600.3 In the context of cardiovascular risk, ERS is characterised by a member of the primary care team identifying and referring a sedentary individual with evidence of at least one cardiovascular risk factor to a third-party service (often a sports centre or leisure facility), where the third-party service prescribes and monitors an exercise programme tailored to the individual needs of the patient.4
Although beneficial effects of ERS have been shown,5–8 effectiveness is influenced by the proportion of those referred who initially participate in an ERS (‘uptake’) and, of these individuals, how many continue to participate (‘adherence’). A recent UK survey reported a range of uptake across schemes, with 30–98% of referred patients attending the initial exercise referral consultation.3 The same survey identified that scheme ‘completion rates’ ranged from 20% to 90%. In a qualitative review, factors appearing to predict adherence and scheme completion include baseline activity, extent of obesity and increasing age.5 Two previous systematic reviews have considered the issue of uptake and adherence to ERS. Williams concluded that uptake and adherence were low, with 33% of individuals not participating in the scheme and 12–42% completing a 10–12-week period of ERS.7 Gidlow et al9 reported uptake rates of 23–60% with approximately 80% of participants dropping out before the end of the scheme.
It may be that those most in need of physical activity advice have the lowest uptake and adherence, and thus ERS schemes could run the risk of increasing health inequalities.10 ,11 Furthermore, low uptake and adherence have important cost-effectiveness implications that may put such schemes at a disadvantage when competing for already scarce resources. The identification of factors influencing low uptake and adherence could lead to the refinement of schemes to optimise investment. It is therefore important to understand the factors that might influence ERS uptake and adherence. The aims of this systematic review were to quantify, for the first time, the levels of ERS uptake and adherence and to identify factors predictive of uptake and adherence. Given the potential bias in terms of sample recruited that a randomised controlled trial (RCT) may introduce, we also aimed to identify differences in uptake and adherence between those recruited into observational studies and RCTs.
Methods
This review was conducted and reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.12
Search strategy
The following electronic databases were searched: MEDLINE In-Process (Ovid) and MEDLINE (Ovid) 1950 to October 2009, EMBASE (Ovid) 1980–2009 week 28, Cochrane Library (Wiley) 2009 Issue 3 (CDSR, DARE, CENTRAL NHS EED and HTA database), SportsDiscus (Ebsco) 1990 to October 2009, ISI Web Of Knowledge 1900 to October 2009, Science Citation Index Expanded (SCI-EXPANDED) 1900 to October 2009, Social Sciences Citation Index 1898 to October 2009. In order to maximise the specificity, an initial scoping search was undertaken to develop ‘exercise referral’ and related synonym terms which were then combined with ‘primary care’ search terms and a controlled trial filter. Studies were also sought by reviewing the bibliographies of included studies and those known to the researchers involved in this study. Limitations were also applied for English language and year of publication (1990 onwards) (see Pavey et al8 for full search strategies).
Inclusion and exclusion criteria
Studies were considered eligible for inclusion if they met the following criteria:
Study design: RCTs or observational studies (including non-randomised controlled and uncontrolled studies).
Population: any individual with or without a medical diagnosis.
Intervention: an ERS was defined as comprising three core components: (1) referral by a primary care healthcare professional to a third-party service provider with the aim of achieving an increase in physical activity or exercise; (2) physical activity/exercise programme tailored to individual needs; and (3) initial assessment and monitoring throughout the programme. The ERS exercise/physical activity programme was required to be more intensive than simple advice and needed to include one or a combination of counseling (face-to-face or via telephone), written materials and supervised exercise training.
Outcomes: outcomes were defined as follows: ‘uptake’ is the proportion of those individuals offered entry to ERS who participate in an initial consultation with a ‘qualified exercise professional’ or participate in a first exercise session; ‘adherence’ is the proportion of those individuals who take up ERS that participate in at least 75% of the programme sessions available.
Studies were sought that reported (1) a numerical measure of ERS uptake or adherence and (2) an estimate of the statistical association (eg, correlation or regression coefficient) between participant demographic (eg, age, medical diagnosis), participant psychosocial factors (eg, level of motivation, self-efficacy), programme factors (eg, centre vs home-based delivery, group vs individual sessions, dose of exercise) and uptake or adherence to ERS.
We excluded studies not published in a peer review journal (eg, annual reports of ERS programmes), editorials, opinions and studies available only as meeting abstracts; programmes or systems of exercise referral initiated in secondary or tertiary care such as conventional comprehensive cardiac or pulmonary rehabilitation programmes; and exercise programmes where individuals were recruited from primary care but there was no clear statement of referral by a member of the primary care team.
Study selection process
Titles and abstracts were screened in a three-stage process. At stage 1, a single reviewer (TP) initially excluded clearly irrelevant titles and abstracts. At stage 2, two reviewers (TP and RT or KF or MH or AT) then independently screened the remaining titles and abstracts. At stage 3, full papers of abstracts categorised as potentially eligible for inclusion were then screened in a consensus meeting of at least two reviewers (TP and RT or KF or MH or AT) and disagreements were resolved in real time by consensus.
Data extraction
Data were extracted by one reviewer (TP) using a standardised data extraction form and checked by another (RT). Discrepancies were resolved by discussion with involvement of a third reviewer when necessary. Data extracted included: patient level characteristics (eg, age, disease diagnosis); intervention characteristics (eg, duration, location, intensity and mode of the exercise intervention delivered); and reported estimates on the association and mediators of uptake and adherence to ERS.
Data analysis and synthesis
Meta-analysis was used to pool data on the levels of uptake and adherence across studies. Randomised and observational studies were pooled separately. A random effects meta-analysis model was used in order to take into account the clinical and statistical heterogeneity in studies and the various definitions of uptake and adherence across studies. Given the range of methods of reporting predictors of ERS uptake and adherence, it was not possible to quantitatively pool these data across studies. Instead, we categorised findings in each study based on the strength and direction of the association.13 Analyses were conducted using STATA V.11.0.
Results
Identification and selection of studies
A total of 20 studies were included, six RCTs and 14 observational studies. Figure 1 summarises the selection process. In addition, our searches identified a published protocol for a further ERS trial.14 Although not made fully available to us and unpublished at the time of this review, a report of the trial is available as a press release15 and has therefore been included. A list of excluded studies is reported elsewhere.8
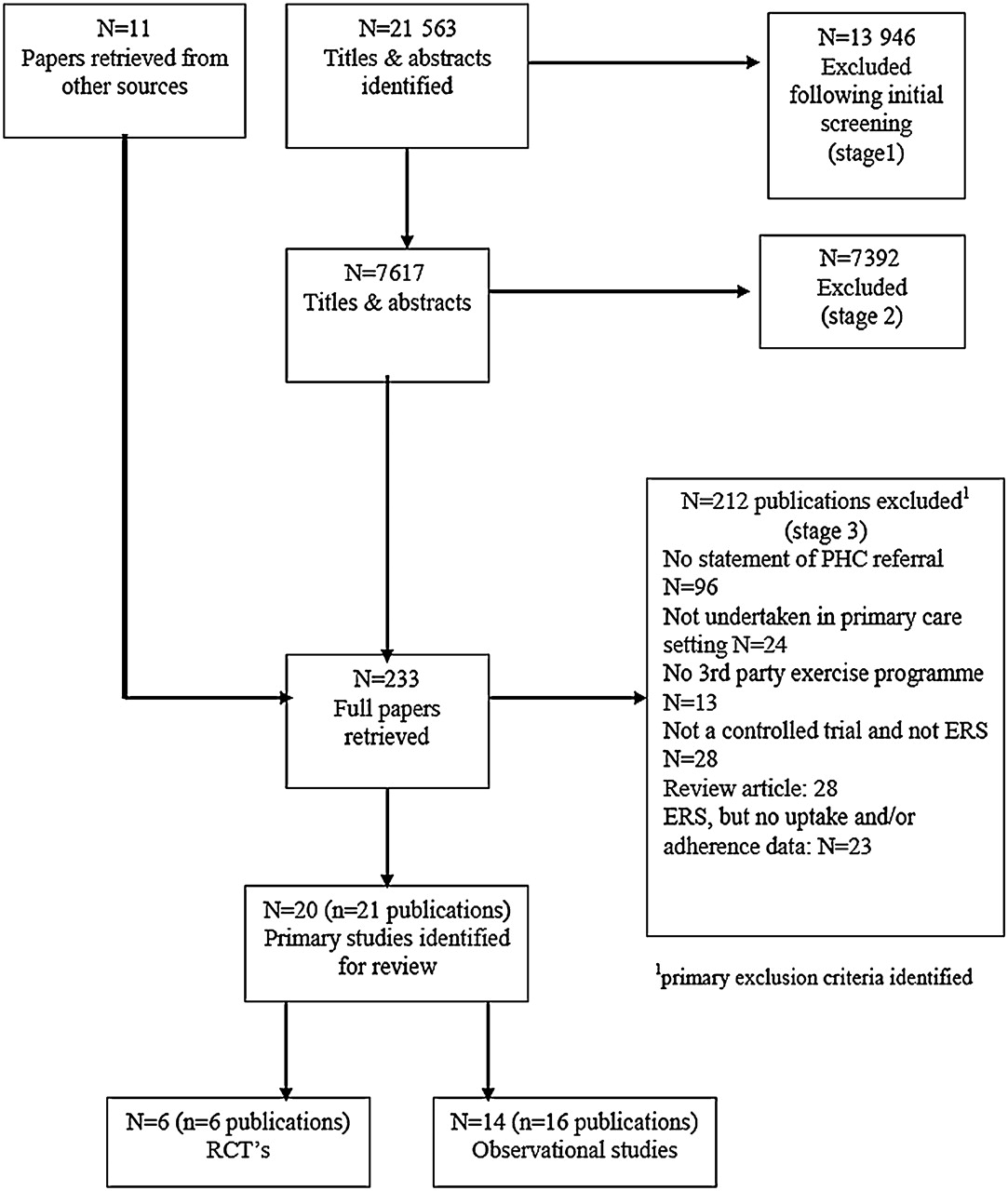
PRISMA flow diagram of study inclusion process for systematic review of predictors of uptake and adherence to exercise referral schemes (ERS).
Characteristics of included studies
The majority of studies were undertaken in the UK (n=17). Sample sizes ranged widely across studies from 28 to 6610 participants (median 419). Participants in individual studies were predominately middle aged (mean age 51–64 years) and female (57–100%).
ERS uptake and adherence levels
Uptake was broadly defined in one of two ways: attendance at the initial consultation with the exercise professional or attendance at ≥1 exercise session (see appendix in online supplement). The level of uptake in ERS ranged from 28% to 100% across studies. The pooled level of uptake in ERS was 66% (95% CI 57% to 75%) across observational studies and 81% (95% CI 68% to 94%) across RCTs (figure 2). There was evidence of a high level of statistical heterogeneity for observational studies (I2=99.4%, p<0.0001) and for RCTs (I2=99.2%, p<0.0001). The studies of Stevens and colleagues19 and Damush and colleagues21 reported the lowest levels of uptake in ERS for an RCT and observational study, respectively (35% and 28%). Notably, the referral method was different for these two studies19 ,21—that is, referral by letter compared with face-to-face referral in the other studies where the uptake ranged from 58% to 100%.

Pooled level of uptake of exercise referral schemes (ERS).
The majority of studies (n=14) broadly defined adherence as the number of individuals who completed a minimum set number of exercise sessions (see online appendix). In four studies27–30 an attendance at a post-ERS consultation was also required to meet their definition of adherence. Levels of adherence to ERS ranged from 12% to 93%. The pooled level of ERS adherence was 49% (95% CI 40% to 59%) across observational studies and 43% (95% CI 32% to 54%) across RCTs (figure 3). There was a high level of statistical heterogeneity for both observational studies (I2=99.1%, p<0.0001) and for RCTs (I2=91.9%, p<0.003). The observational study by Martin and Woolf-May30 reported particularly low levels of adherence (12%), but there was insufficient information in their report to determine the explanation for this low adherence rate. However, the authors did state that ‘of the available 490 subjects there were only 60 known finishers’, suggesting that some individuals who may have adhered may not have been followed up.

{kind=link}
{kind=link}
{kind=link}
Pooled level of adherence to exercise referral schemes (ERS).
Predictors of participant uptake
In six observational studies21 ,23 ,24 ,25 ,27 ,28 and two RCTs,17 ,20 potential predictors of uptake to ERS were reported, with bivariate analysis undertaken in five studies17 ,20 ,23 ,24 ,27 and multivariate analysis in four studies.21 ,24 ,25 ,28 The results are summarised in table 1 where we identify if and how different demographic and programme factors related to uptake within bivariate and multivariate analyses and our overall findings. In addition, we consider the medical diagnosis as a predictor of uptake.
Summary of analysis of predictors of uptake of exercise referral schemes (ERS)
Demographic factors
In two studies27 ,28 women were reported to be more likely to uptake ERS than men while, in two studies,16 ,24 no association between gender and uptake in ERS was seen. Increasing age was positively associated with increased levels of uptake in ERS in three studies23 ,24 ,28 while, in three other studies,17 ,21 ,27 no such association was found. Gidlow and colleagues24 reported that participants residing in more deprived neighbourhoods were less likely to attend at least one session and those individuals living in a more rural location where less likely to uptake ERS. Damush and colleagues21 found no association between ethnicity and participation in ERS.
Medical diagnosis
Given the variation in reporting reason for referral (medical history) and analysis, it was not possible to tabulate this in a meaningful way. Harrison and colleagues16 reported that those with mental health problems (OR 1.79, 95% CI 1.24 to 2.39, p<0.01) were more likely to participate in ERS than those with no specified reason for referral whereas Gidlow and colleagues35 ,36 reported that patients referred with mental health problems (OR 0.33, 95% CI 0.27 to 0.57, p<0.01) were less likely to participate in ERS than patients with cardiovascular disease or those with physical health problems (60% vs 69%; p<0.001). Gidlow et al36 also reported that patients referred with musculoskeletal problems (OR 0.75, 95% CI 0.58 to 0.99, p<0.05) were less likely to participate in ERS than those with cardiovascular disease. In contrast, Sowden and colleagues28 found that patients referred with a musculoskeletal problem (OR 1.18, 95% CI 1.01 to 1.38, p<0.05) problem were more likely to participate in ERS. Gidlow and colleagues36 reported that patients referred for overweight/obesity problems (OR 0.63, 95% CI 0.50 to 0.81, p<0.01) were less likely to participate in ERS than patients with cardiovascular disease. Taylor et al20 found that more individuals referred for obesity participated in ERS than those referred for smoking (p<0.01). Harrison and colleagues16 reported that those with low physical fitness (OR 10.33, 95% CI 1.44 to 74.3, p<0.05) were more likely to participate in ERS than those with no specified referral reason. Furthermore, patients with respiratory problems and who were most deprived were more likely to participate in ERS than those with respiratory problems and least deprived (OR 1.45, 95% CI 1.06 to 1.99, p<0.05).16
Programme factors
Gidlow and colleagues36 reported that GP referrals were more likely to lead to uptake in ERS than referrals by another individual. Sowden and colleagues28 and Damush and colleagues21 both observed no association between the area in which the scheme or the referring clinic was located and uptake in ERS.
Predictors of ERS adherence
Predictors of adherence were reported in eight observational studies23 ,24 ,26–28 31–33 and two RCTs.17 ,20 Bivariate statistical analysis was used in seven studies17 ,20 ,23 ,24 ,26 ,27 ,33 and multivariate statistical analysis was undertaken in four studies.24 ,28 ,31 ,32 The results are summarised in table 2 where we identify if and how different demographic, programme factors and psychosocial factors relate to adherence in bivariate and multivariate analyses and our overall findings. In addition, we consider medical diagnosis and programme factors as predictors of adherence.
Summary of analysis of adherence to exercise referral schemes (ERS)
Demographic factors
In two studies23 ,24 men were found to be more likely to adhere (ie, complete 75–100% of available exercise sessions) to ERS than women while no such association was found in three studies.27 ,28 ,32 Increasing age was a predictor of increased ERS adherence in five studies,23 ,24 ,27 ,28 ,32 but two studies showed no association with age.17 ,27 Deprivation, rurality, referrer, leisure provider24 and occupation32 were not found to be significant predictors of ERS adherence. Dugdill and colleagues23 reported that fewer patients adhered to ERS (p<0.01) when referred by the GP (32%) compared with a practice nurse (45%) or a cardiac nurse (57%).
Medical diagnosis
Given the variation in reporting the reason for referral (medical history) and analysis, it was not possible to tabulate this in a meaningful way. In the study by James and colleagues,32 patients with pulmonary problems were less likely to adhere to ERS than those with cardiovascular disease. Sowden and colleagues28 reported that patients with diabetes were less likely to adhere to ERS (OR 0.76, 95% CI 0.63 to 0.93, p<0.01) while those with cardiovascular disease (OR 1.22, 95% CI 1.03 to 1.45, p<0.05) were more likely to adhere to ERS compared with those without either diabetes or cardiovascular disease. Gidlow et al24 reported that patients referred for mental health problems were less likely to adhere to ERS than those referred for physical health problems (22% vs 34%, p<0.001). Taylor et al20 reported no difference in adherence between individuals who were referred as smokers, overweight, obese or hypertensive.
Psychosocial
Three studies26 ,31 ,33 assessed the psychosocial predictors of adherence (table 2). Morton and colleagues33 found that participants who adhered to ERS had significantly higher self-determination at baseline while Edmunds et al31 found no such association. Jones et al26 found that participants who did not adhere to ERS had significantly higher expectations for change in personal development.
Programme factors
Sowden et al28 reported variable levels of patient adherence across six different ERS schemes in the London area, indicating the potential influence of programme level factors such as time between referral and initial session, characteristics of exercise leaders and availability of exercise opportunities.
Discussion
Main findings
There has been little consideration of uptake and adherence in previous systematic reviews of ERS.5–7 We identified 14 observational studies and six RCTs where the level of ERS uptake and/or adherence was reported. A wide range of uptake (28–100%) and adherence (12–93%) levels was found across studies. While there was evidence of a higher level of uptake in ERS for RCTs (pooled mean 80%) than observational studies (pooled mean 66%), the levels of adherence to ERS appeared to be similar across study types (pooled mean 43% vs 49%). However, it is important to note that there was a high degree of statistical heterogeneity in the levels of uptake and adherence across studies.
The observed heterogeneity in the uptake and adherence levels across studies can at least be partly explained by the differing referral methods and number of exercise sessions on offer. Referral by letter appeared to produce lower uptake rates than face-to-face consultation with a healthcare professional. For example, Stevens et al hypothesised that the level of uptake in ERS may have been reflective of the nature of the invitation letter sent to participants (eg, it could have been less focused on exercise) and the point of randomisation (pre-invitation letter). They also hypothesise that a change in the format of the letter (eg, including a specific date offered for the first ERS appointment) would have improved participation. Similarly, Damush et al used a letter-based recruitment in conjunction with a pre-exercise test before participants commenced the exercise intervention, as required by the study funders, and potentially this could have further deterred eligible patients from consenting to the study.
When considering levels of adherence, schemes with fewer available sessions are potentially more likely to provide a higher number of adherers at the 75–100% completion rate. Without a standardised definition, there is a risk of patients being classified as adherer or non-adherer simply because of a difference in definition applied by study. For example, completing eight out of 10 sessions (>75%) is categorised as adherence whereas 12 out of 20 sessions is not.
Six of 13 included studies undertook multivariate analyses (ie, adjusted for potential confounders) and seven used unadjusted bivariate analyses to assess the association between potential predictors and levels of uptake or adherence. Few studies considered anything other than gender and age. Women were more likely to begin an ERS but were less likely to adhere than men. Older people were more likely to begin and adhere to an ERS.
Uptake of ERS as reported through observational studies was lower than for RCTs. This may be explained by the fact that those entering an RCT were required to give full consent to a research trial and were therefore more highly committed initially than those entering an exercise referral programme without such a commitment. Observational studies may more closely reflect the level of uptake and adherence under normal circumstances.
Strengths and limitations
Every effort was made to reduce potential bias in this review. We used comprehensive electronic searches including searching of reference lists of included studies and predefined inclusion criteria which were applied by consensus across two or more reviewers. In order to directly compare studies we applied standard definitions of uptake (the proportion of those individuals offered entry to ERS who attend an initial consultation with an exercise professional or attend a first exercise session) and adherence (of those that uptake ERS, the proportion undertaking 75–100% of the programme). Although we sought studies that examined predictors of ERS uptake or adherence using multivariate analysis to adjust for potential confounders, we found few such studies.
Finally, this is the first systematic review of the extent and predictors of uptake and adherence. In conducting it we had to make some important decisions about defining adherence, and this was not easy with different indicators being used across studies. Also, adherence was strictly linked to attendance data at an exercise centre and did not encompass any increase in daily physical activity. There is an implicit assumption that a higher level of adherence is better whereas, in reality, some people are motivated after a few sessions to become more active through other forms of lifestyle physical activity or exercise sessions away from the ERS. The relationships between predictors and adherence may well be different for broader measures of physical activity.
Implications for research and policy
While the variable uptake and adherence rates may simply be a reflection of differences in definition, they may also reflect a less than optimal ERS referral process (eg, the GP did not explain fully to patients what to expect at the gym), a lack of individual tailoring of exercise options (ie, lack of patient autonomy and choice and convenient facility access) and inappropriate referrals (ie, some patients were not ready to begin an exercise programme). Evidence from the physical activity promotion literature demonstrates the importance of behaviour change techniques for the adoption and maintenance of a physically active lifestyle. ERS need to incorporate such behaviour change techniques and evaluate whether these have a positive impact on uptake and adherence.37 Furthermore, it would be helpful to develop a consensus definition for uptake and adherence for application in future physical activity promotion intervention studies.
What is already known on this subject
The effectiveness of exercise referral schemes is influenced by the levels of uptake and adherence to the schemes.
A recent UK survey reports uptake across schemes ranging from 30% to 90% and ‘completion rates’ from 20% to 90%.
Factors appearing to predict adherence and scheme completion include baseline activity, extent of obesity and increasing age.
What this study adds
Overall uptake and adherence rates to exercise referral schemes are relatively low but also highly variable across different programmes.
Only being female and increasing age were found to be consistent predictors of higher levels of uptake of exercise referral schemes.
Only being male and increasing age were found to be consistent predictors of higher levels of adherence to exercise referral schemes.
Future physical activity promotion research would greatly benefit from a consensus definition of uptake and adherence.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This project was funded by the NIHR Health Technology Assessment programme (project number 08/72/01) and will be published in full in the Health Technology Assessment (HTA) journal around September (see HTA programme website for further project information).
Disclaimer The views and opinions expressed here are those of the authors and do not necessarily reflect those of the Department of Health.
Competing interests JS is Chief Medical Officer of the Fitness Industry Association (FIA). The FIA meets his receipted expenses. The post attracts neither a salary nor fees.
Ethics approval This is a systematic review for which ethical approval is not required.
Provenance and peer review Not commissioned; externally peer reviewed.