Article Text

Abstract
Background: The relation between knee meniscal structural damage and cartilage degradation is plausible but not yet clearly proven.
Objectives: To quantitate the cartilage volume changes in knee osteoarthritis using magnetic resonance imaging (MRI), and determine whether meniscal alteration predicts cartilage volume loss over time.
Methods: 32 patients meeting ACR criteria for symptomatic knee osteoarthritis were studied. MRI knee acquisitions were done every six months for two years. The cartilage volumes of different knee regions were measured. Three indices of structural change in the medial and lateral menisci were evaluated—degeneration, tear, and extrusion—using a semiquantitative scale.
Results: 24 patients (75%) had mild to moderate or severe meniscal damage (tear or extrusion) at baseline. A highly significant difference in global cartilage volume loss was observed between severe medial meniscal tear and absence of tear (mean (SD), −10.1 (2.1)% v −5.1 (2.4)%, p = 0.002). An even greater difference was found between the medial meniscal changes and medial compartment cartilage volume loss (−14.3 (3.0)% in the presence of severe tear v −6.3 (2.7)% in the absence of tear; p<0.0001). Similarly, a major difference was found between the presence of a medial meniscal extrusion and loss of medial compartment cartilage volume (−15.4 (4.1)% in the presence of extrusion v −4.5 (1.7)% with no extrusion; p<0.001).
Conclusions: Meniscal tear and extrusion appear to be associated with progression of symptomatic knee osteoarthritis.
- ACR, American College of Rheumatology
- FISP, fast inflow with steady state precession
- JSW, joint space width
- Knee
- cartilage
- osteoarthritis
- quantitative MRI
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- FISP, fast inflow with steady state precession
- JSW, joint space width
Osteoarthritis is a common cause of disability in people over 60.1 Cartilage damage assessment is important for monitoring disease progression and evaluating therapeutic response in osteoarthritis. Serial radiographs of affected joints appear to be a logical means of documenting the progression of the disease over time2,3 provided that a validated, reliable, and easily reproducible technique is used.4–,8 Although it has been suggested that the measurement of knee femoro-tibial joint space width (JSW) provides information on cartilage change, the integrity of surrounding tissues, particularly the meniscus, could affect the reliability of this measurement.9,10 However, others have concluded that partial surgical meniscectomy11 or spontaneous meniscal changes10 do not influence femoro-tibial JSW on weight bearing x rays, suggesting that JSW loss mirrors cartilage degradation. Magnetic resonance imaging (MRI) allows precise visualisation of joint structures such as cartilage, bone, synovium, ligaments, and menisci, as well as their pathological changes.12–,14
Recently, we and others have developed a system to quantify cartilage volume using MRI acquisitions combined with sophisticated software.15–,22 Moreover, on our MR acquisitions,20,21 the medial and lateral menisci of the knee are easily visualised and provide concomitant information on this structure—that is, degeneration, tear, or extrusion from the joint space. Intuitively, meniscal damage is believed to be strongly associated with the neighbouring cartilage changes and is an important part of the pathophysiology of overall knee osteoarthritis, as suggested by many studies.23–,25 In an animal model, meniscal structural damage may occur at the early stages of the disease, while cartilage damage seems to appear later,26 though this is not generally accepted.27 However, whether meniscal damage or cartilage degradation occurs first remains unknown in humans. Moreover, it is not clear what type of meniscal damage (degeneration, tear, or extrusion) has the greatest impact on the progression of cartilage loss over time.
The objective of this pilot study was first, to assess semiquantitatively and longitudinally over a two year period the knee meniscal changes (degeneration, tear, and extrusion) in a cohort of symptomatic “primary” knee osteoarthritis patients from a typical rheumatology practice setting; and second, to contrast these findings with knee cartilage volume changes over time.
METHODS
Patient selection
Thirty two patients were recruited from the outpatient rheumatology clinic at Notre-Dame Hospital, Montreal, Canada. Rheumatologists at the arthritis division of Notre-Dame Hospital provided the patients. Men and women were eligible for the study if they were aged between 40 and 80 years, fulfilled the American College of Rheumatology (ACR) criteria for knee osteoarthritis,28 and had symptomatic disease requiring medical treatment in the form of acetaminophen, traditional non-steroidal anti-inflammatory drugs (NSAIDs), or selective COX-2 inhibitors. Eligible patients were required to have radiological evidence of osteoarthritis in the affected knee obtained within six months of the start of the study. In addition, they had to have a severity grade of 2 or 3 on the Kellgren–Lawrence scale29 for joint space narrowing, osteophytes, or sclerosis. Finally, patients had to have a minimum JSW of the medial femoro-tibial compartment of between 2 and 4 mm, as measured with a ruler. The measurements were done on weight bearing extended knee films obtained at recruitment. Patients with chondrocalcinosis were excluded. Patients were also excluded if they had isolated patello-femoral osteoarthritis; if osteoarthritis of the knee was secondary to other conditions, including inflammation, sepsis, metabolic abnormalities, and trauma; if they had acute or chronic infection (including tuberculosis); or if there were any contraindications to MRI evaluation. Additional exclusion factors consisted of a history (past or present) of gastrointestinal ulceration, intra-articular corticosteroid injections in the study knee within the previous six months, and radiological grade 4 osteoarthritis. Patients with severe (class IV) functional disability, candidates for imminent knee joint surgery, and those with contralateral total joint replacement were also excluded.
In patients in whom both knees were symptomatic, we chose the most symptomatic one for the investigation. Patients were permitted to receive simple analgesics, NSAIDs, or steroid injections. Analgesic regimens could be changed according to the rheumatologist’s preferences and the patient’s clinical course. The use of indomethacin was not permitted because of its potential to promote osteoarthritic cartilage degeneration.30–,32 Likewise, the use of glucosamine sulphate was not permitted because of its potential effect on osteoarthritis progression.33
The study was approved by the University of Montreal Hospital Center (Centre hospitalier de l’Université de Montréal—CHUM) ethics committee. Patients gave informed consent. No washout of drugs was done before the clinical evaluation.
Knee MRI
High resolution, three dimensional magnetic resonance (MR) studies were obtained for each osteoarthritis patient at baseline and at 6, 12, 18, and 24 months using the Magneton Vision 1.5 Tesla machine, with a dedicated knee coil commercially available from Siemens (Erlangen, Germany), as previously described.20,34 These examinations are optimised three dimensional FISP type (fast inflow with steady state precession) acquisitions with fat suppression.20,34 All parameters were set to produce images with the highest cartilage contrast, resolution, and signal to noise ratio within a reasonable acquisition time: repetition time (TR) = 42 ms, echo time (TE) = 7 ms, flip angle = 20°, 98 Hz per pixel bandwidth, and matrix size 410×512 pixels. The sagittal field of view was set to 160 mm and was rectangular whenever possible. About 80 to 110 1.0 mm thick slices yielded a volume dataset with an effective voxel size of 0.31×0.39×1.0 mm3. A strict positioning and immobilising protocol was used to reduce movement during acquisition. The total patient positioning and MR acquisition time ranged from 24 to 31 minutes. The patients were able to tolerate this procedure without any significant problem.
MRI cartilage volume determination
Cartilage thickness and the volume of the knee joint were measured by two trained and blinded readers, using a specially developed computer program (Cartiscope™, ArthroVision, Montreal, Quebec, Canada) running on a Windows NT/9x workstation, as previously described.20,34 The segmentation of the cartilage–synovial interfaces was then carried out.34
The change in cartilage volume over time was calculated for the entire knee (global), femoral condyles, tibial plateaus, and for each of the knee compartments (medial compartment: summation of medial femoral condyle and tibial plateau volume; and lateral compartment: summation of lateral femoral condyle and tibial plateau volume), respectively. The coefficients of variation (CV%) were computed as previously34 and were, respectively, for the global cartilage 2.2%, medial compartment 1.6%, lateral compartment 2.6%, total femur 3.1%, and total tibia 1.9%.
Meniscal damage
For the meniscal evaluation, we chose to use the same sequences as for the cartilage assessment, even though these may not be optimal for meniscus assessment. This was done mainly because the MRI procedure would have become too lengthy with the addition of another sequence. However, the FISP sequence (fig 1⇓) enabled us to visualise the meniscal tissue with enough clarity to apply the semiquantative scoring described in this section adequately and reliably. For the meniscal damage scoring system, we referred to the accepted MRI nomenclature for meniscal anatomy, which is in general agreement with the arthroscopic literature.35–,37 Meniscal degeneration is defined as an abnormal intrasubstance of grey signal intensity on all MR sequences, not considering the meniscal surfaces or the gross meniscal morphology. Data are initially acquired in the form of a sagittal view. This view was first examined and confirmation of the score verified by examining the other (coronal and axial) views. Both knee menisci were evaluated by an experienced radiologist (MJB) who was blinded for the time sequences and cartilage volumes, while the cartilage volume assessment was carried out separately by two different readers who were completely unaware of the radiologist’s grading. The proportion of the menisci affected by the degeneration, tear, or extrusion was scored separately using a semiquantitative scale as follows:

Different meniscal pathologies as seen by magnetic resonance imaging (MRI) contrasted to normal meniscus (top left panel). The MRI acquisitions are three dimensional fat suppressed FISP sequences as described in Methods.
Degenerative changes and tears—For meniscal degenerative changes and tears, the following scale was applied: 0 = no damage; 1 = one of three meniscal areas involved (anterior, middle, and posterior horns); 2 = two of three areas involved; 3 = all three areas involved.
Extrusions—The extent of meniscal extrusion on the medial or lateral edges of the femoral tibial joint space, not including the osteophytes, was evaluated for the anterior, middle, and posterior horns of the menisci in which 0 = no extrusion, 1 = partial meniscal extrusion, and 2 = complete meniscal extrusion with no contact with the joint space.
No patient had a posterior horn extrusion. Thus four indices were specifically analysed: meniscal tears, degeneration, anterior horn extrusion, and middle horn extrusion.
MRI sequences were obtained at baseline and at six month intervals over a two year period. The scores for each of the three types of meniscal damage (degeneration, tear, extrusion) were compared to examine associations at baseline and to use baseline information to predict change in cartilage volume over time. Once the score of each type of meniscal damage was assessed, the patients were classified according to the baseline and to the progression of such damage (if any) over time. For each type of meniscal damage, three subgroups were clearly identified according to clinical relevance: a “none” damage group, where no lesions were seen at baseline or at any time point; a “severe” group, where a score of 3 was present at baseline; and a “mild” group, representing the patients not already included in the “none” or “severe” groups.
Statistical analysis
All the data were systematically entered into a computerised database using a blinded double entry procedure. The cartilage volume losses are presented as percentage loss compared with baseline. A Spearman rank test was used to correlate meniscal damage indices at baseline and to follow their progression over time. The three subgroups of meniscal damage over time (“none,” “mild,” and “severe”) as described above were also evaluated to assess their respective effect on cartilage volume change over time. Mann–Whitney non-parametric tests were done to contrast the three pairwise comparisons among these subgroups for change in cartilage volume. Finally, a multilinear regression was used to find the best predictors of cartilage volume loss among the four meniscal damage indices. All statistical analyses were done using Statistica, version 6. All tests were two sided, and a p value ⩽0.05 was considered significant. Analyses were done without corrections for multiple comparisons.
RESULTS
Patient characteristics
As previously reported,34 40 patients were enrolled in this longitudinal and observational study: four were lost to follow up early in the study (two died, two rescinded their consent), and for four additional subjects one or more MR acquisitions was missing and they were therefore excluded from the MR analyses and demographic summaries. Thus 32 patients were analysed. The cohort was generally similar at baseline with respect to demographic and disease characteristics of the general population with symptomatic osteoarthritis.
Cartilage volume changes over time
These data were as previously reported.34 In brief, by six months, there were significant differences in cartilage volume loss for the entire knee (mean (SD), −3.8 (5.1)%), the medial compartment (−4.3 (6.5)%), the lateral compartment (−3.3 (4.9)%), the femur (−3.7 (6.6)%) and the tibia (−2.8 (5.9)%) compared with baseline (p<0.0001 for all compartments). Moreover, a statistically significant difference in cartilage volume loss was seen at each of the six month assessments compared with baseline from six months to 24 months (p<0.0001 for all the values—global, medial, and lateral compartments, femur and tibia). At 24 months, significant losses for the global (−6.1 (7.2)%), medial compartment (−7.6 (8.6)%), lateral compartment (−5.0 (7.0)%), femoral (−6.8 (8.8)%), and tibial (−4.4 (6.4)%) cartilage volume losses were seen compared with baseline (p<0.0001 for global, medial, and lateral compartments; p = 0.003 for femur; p = 0.0005 for tibia).
Correlations between baseline meniscal damage indices
Correlations between baseline meniscal damage indices are shown in table 1⇓. In the patient cohort, no posterior horn extrusion was observed. Meniscal damage (mild to severe tear) was seen upon the first visit in 24 patients (75% of the cohort) and 19 had some level of horn extrusion. A correlation between tear and extrusion was present at baseline (r = 0.65, p<0.001 middle horn extrusion; r = 0.60, p<0.002 anterior horn extrusion). An inverse correlation between meniscal degeneration and tear (r = −0.68, p<0.003) and extrusion was found (r = −0.29, p<0.01).
Correlations between baseline meniscal damage indices
Meniscal structural damage over time
Correlations of baseline meniscal damage indices with meniscal tears over time are shown in table 2⇓. The data show that the presence of one of the meniscal damage indices was not correlated with progression of the other damage indices over two years. Degeneration was inversely associated with a tear at baseline (r = −0.45, p<0.01) and over the two year follow up (r = −0.34 at six months, −0.20 at one year, and −0.14 at two years). In addition, the meniscal middle horn extrusion was associated with a tear at baseline (r = 0.67, p<0.004), but the correlation of extrusion at baseline with tear did not increase over time (r = 0.74 at six months, 0.64 at one year, and 0.53 at two years). The same results were found when contrasting the anterior extrusion and tear (r = 0.67 at baseline, 0.70 at six months, 0.66 at one year, and 0.60 at two years) (table 2⇓). Finally, similar results were also seen on investigation of the association between tear and the other meniscal damage indices (data not shown).
Correlation of baseline meniscal damage parameters with meniscal tear over time
Subgroups of meniscal structural damage and associated cartilage volume loss
On the basis of medial meniscal degeneration, we identified three subgroups with different damage progression over time. A first group of 14 patients did not present any such damage at baseline nor did these patients develop any damage over the two year follow up; hence they were called the “none” group. A second group, consisting of 10 patients who had a score of 1 for meniscal degeneration at baseline and four of whom progressed to a score of 2 over time, was called the “mild” group. Finally, eight patients, the “severe” group, had severe degeneration (score = 3) at baseline and persisting over the two years. For lateral meniscal degeneration, 19 had none, five had mild degeneration (all had a score of 1 and none progressed to a score of 2), and eight had severe degeneration at baseline.
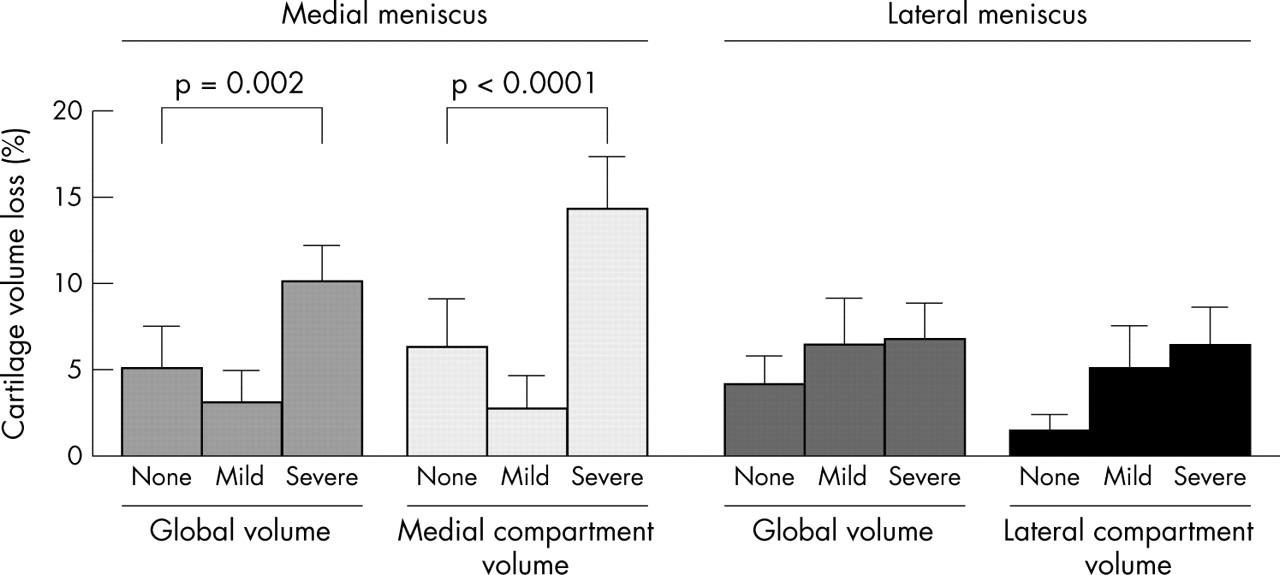
With respect to medial meniscal tears (fig 2⇓), eight patients did not have any tear at baseline or over the two year follow up; 13 patients had a score of 1 (“mild” group) at baseline, three of whom progressed to a score of 2 over time. Eleven patients, the “severe” group (score = 3), had a severe medial meniscal tear at baseline and over time. For the lateral knee meniscus, eight patients had no tear, eight had a mild tear (three progressed), and 16 had a severe tear.

Cartilage volume loss (%) at two years compared with baseline, divided by degree of meniscal tear, as described in the text. Non-parametric two sample tests showed significant differences in cartilage volume loss between the severe medial meniscal damage and no tear groups for both the cartilage global and medial compartment volume. No significant differences in cartilage volume losses were seen among the groups with lateral meniscal tear.
Finally, with respect to medial middle horn extrusion (fig 3⇓), 13 patients had none, 11 had mild extrusion, and eight had severe extrusion. The latter showed an almost complete extrusion of the meniscus from the joint space. Fifteen patients had no medial meniscal anterior horn extrusion (fig 3⇓), 10 had mild extrusion (no patients with progression), and seven had severe extrusion. No patient progressed from one grade to another over the two year period of observation.

{kind=link}
{kind=link}
{kind=link}
Cartilage volume loss (%) at two years divided by degree of meniscal extrusion, as described in the text. Non-parametric two sample tests showed significant differences in cartilage volume loss between the severe meniscal anterior horn extrusion and no extrusion for the medial compartment volume. No significant differences in cartilage volume loss were seen among the groups with middle horn extrusion.
We investigated the amount of structural meniscal damage as measured by the loss of cartilage volume over the two year assessment period (figs 2⇑ and 3⇑). A highly significant difference in average per cent global cartilage volume loss at two years was observed between the severe medial meniscal tear group and the no tear group (−10.1 (2.1)% v −5.1 (2.4)%; p = 0.002) (fig 2⇑). There was an even greater difference in the percentage of medial compartment volume loss between the severe and no-tear groups (−14.3 (3.0)% severe tear group v −6.3 (2.7)% no tear group; p<0.0001). Although there was a trend toward more lateral cartilage volume loss in the mild and severe meniscal tear groups for the lateral meniscus, this did not reach statistical difference.
Additionally, a large difference in the percentage loss of medial compartment cartilage volume was found between the groups with severe v no presence of a medial meniscal anterior horn extrusion (−15.4 (4.1)% for severe extrusion v −4.5 (1.7)% for no extrusion; p<0.001) (fig 3⇑). A significant increase in global cartilage loss with meniscal anterior horn extrusion severity was also found (global volume loss was −10.3 (2.9)% when severe anterior horn extrusion was present v −4.0 (1.7)% when there was no extrusion; p<0.001).
Although a similar pattern was also found for the meniscal middle horn extrusion, the differences were not significant. A higher level of medial cartilage compartment volume loss was found when severe meniscal middle horn extrusion was compared with the “none” group (p<0.001). Finally, when examining the loss of the total cartilage of the tibial plateaus and femur condyles separately, no significant differences were found between the none v severe groups for any index of meniscal damage (data not shown).
Meniscal degeneration was also contrasted with cartilage volume loss. For this specific type of meniscal damage, no relation was seen with cartilage volume loss in any of the compartments, or in the femoral condyles or tibial plateaus.
Multilinear regression analysis
A multilinear regression analysis investigating the association of global and medial cartilage volume loss at two different times (at two years v baseline (table 3⇓) and at six months v two years (table 4⇓)) with the four medial meniscal structural damage indices (anterior horn extrusion, middle horn extrusion, meniscal tear, degeneration) showed that extrusion of the meniscus middle and anterior horn was most predictive of global cartilage volume loss (p = 0.01 and p = 0.02, respectively) and medial cartilage compartment loss (p = 0.01 and p = 0.03) at two years (table 3⇓). For the same baseline meniscal damage indices, a stronger association was found for change in global cartilage volume loss between six months and two years (p = 0.001 for anterior horn extrusion; p = 0.002 for middle horn extrusion) (table 4⇓). A strong association was also seen with medial meniscal damage and medial cartilage volume loss from six months to two years (p = 0.007 for anterior extrusion; p = 0.01 for middle horn extrusion), suggesting a lag time between this type of meniscal damage and subsequent cartilage loss.
Multilinear regression of medial meniscal damage indices at baseline predicting cartilage volume loss over two years
Multilinear regression of medial meniscal damage indices at baseline predicting cartilage volume loss from six months to two years
No association was found for the lateral meniscal damage indices and cartilage volume loss except for the lateral middle and anterior horn extrusion and loss of cartilage for the second year (p = 0.01, data not shown).
DISCUSSION
A striking finding of this study was that over 75% of our patients with so called “primary” symptomatic osteoarthritis had meniscal damage. These patients did not report knee trauma or experience an acute knee pain exacerbation; they were selected according to the well recognised ACR criteria for the classification of knee osteoarthritis.28 This finding is in agreement with previous studies that reported that 52–92% of patients with symptomatic knee osteoarthritis present with meniscal damage when assessed by MRI.38–,40 So far, very few studies have used MRI to examine the in vivo change in cartilage volume over time in correlation had damage in a population with symptomatic knee osteoarthritis. Our original longitudinal MRI study of 32 subjects with symptomatic osteoarthritis of the knee already showed a significant global cartilage volume loss (−6.1%) at two years of follow up (p<0.0001).34 We further showed in this study that the loss of cartilage volume in the medial compartment of the knee was even more striking when medial meniscal tears and extrusion were present, reflecting more rapid disease progression in this area. The more striking progression of the disease in the medial compartment may be explained by the greater weight bearing pressure in this compartment, as suggested by Cerejo et al.41
The ability of MRI studies to assess the entire joint structure—including the cartilage, menisci, bone, synovial tissue, and ligaments—may help to redefine primary osteoarthritis. Cicuttini et al42 proposed that there is accelerated loss of cartilage over time in patients who undergo partial meniscectomy. These results suggest a strong role of the meniscal apparatus in protecting cartilage, especially in elderly subjects with obesity or joint instability. Using MRI, Biswal et al43 also recently studied risk factors associated with progressive cartilage loss in the knee in 43 patients. Patients were evaluated at baseline and after an average of 1.8 years of follow up. Meniscal and anterior cruciate ligament tears were associated with more rapid cartilage loss. Moreover, Biswal’s study also showed that the central portion of the medial compartment had more rapid progression of cartilage loss than the anterior or posterior portions, a clear indication that cartilage loss in osteoarthritis is not evenly distributed in the knee. Another study, by Felson et al,44 also stressed the influence of structural changes in the assessment of knee osteoarthritis. These investigators showed that subchondral bone marrow oedema, as assessed by MRI, was strongly associated with pain in knee osteoarthritis.
What we do not yet know is whether this at risk population, as identified in the present study, could benefit from “chondroprotective” agents, or whether their disease course is relentless. The implications of these MRI findings relating to knee cartilage and the surrounding tissues may also affect the definition of “primary” osteoarthritis in the future. The ACR criteria for primary osteoarthritis of the knee28 are based on clinical and radiological findings. As cartilage is neither vascularised nor innervated, the pain experienced in osteoarthritis is likely to originate from other structures such as bone, synovial tissues, capsule, ligaments, and obviously, the menisci. Therefore, loss of cartilage volume over time, if chosen to define primary osteoarthritis, may not be reflected by changes in symptoms, may precede the radiological changes, and may be accelerated by unsuspected concomitant structural damage such as meniscal tears and extrusions. This view is in contrast with the results of Link et al,40 who found that cartilage lesions alone were associated with more severe osteoarthritic symptoms. However, one must take into account that their study was cross sectional and may have significant limitations.
There are also some limitations to the present study. We advise caution when making generalisations on the basis of our results because of the relatively small number of subjects. The absence of a control group prevented us from assessing the role of age, weight, weight bearing activities, or drug treatment as factors affecting disease progression. Moreover, the timing of the meniscal damage was not known, so we could not establish the degree of chronicity of the meniscal changes. Nevertheless, the cohort is representative of the average patient population with typical symptomatic knee osteoarthritis seen at an outpatient rheumatology clinic. Whether our results reflect the findings in asymptomatic knee osteoarthritis is debatable. It is quite possible that meniscal changes of asymptomatic disease may differ in severity from those of symptomatic disease, and the relation of the former to osteoarthritis progression is presently unknown.
One could also question the potential for bias because of the non-blinding of the cartilage when meniscal assessment was done. However, as the radiologist’s evaluation was made completely separately from the assessment of cartilage volume, it is unlikely that the grading of meniscal damage was biased by the concomitant visualisation of the cartilage.
Our study considered global and compartmental cartilage volume change. However, the potential of quantitative MRI was not fully utilised. As osteoarthritis is often a focal disease which does not affect the entire cartilage at the same rate, smaller areas of the knee cartilage—for example, the central portion of the medial femoral condyle and its corresponding area of the tibial plateau—may show proportionally greater relative changes when contrasted with corresponding meniscal damage. We deliberately chose to assess greater areas of cartilage to avoid the problem of the a priori selection of an area of greater relative change that may differ quite substantially from one patient to another. The assessment of cartilage volume compartments is very relevant to the meniscal damage, as this structure is intimately related to both the femoral condyles and the tibial plateaus on each side of the knee. Is this therefore likely that the meniscal damage will affect both aspects of the knee and that this concept of “compartment” makes good sense.
As no patients progressed from no meniscal damage to established damage over the two year period of observation, it is difficult to predict precisely whether cartilage loss or meniscal damage occurs first in the degenerative process. A study on subjects at an earlier phase in the osteoarthritic process might give us a sense of the temporal sequence. However, the greater association seen between meniscal extrusion and cartilage volume loss from six months to two years suggests that meniscal damage may indeed precede cartilage volume loss. In support of this finding is a recent study by Englund et al,45 which investigated the long term radiographic and clinical outcome of isolated limited meniscectomy and suggested that a meniscal tear signals the first symptom of the disease.
Conclusions
We have shown that meniscal damage variables already seen in MRI acquisitions and which are easily quantifiable may help to identify subgroups at risk of faster disease progression, which in turn may affect patient selection for eventual treatment with structure modifying osteoarthritis drugs. Our data show that meniscal tears and extrusions are associated with the progression of knee osteoarthritis. Meniscal damage could be a factor to consider in selecting patients who will eventually require structure modifying osteoarthritis drugs.
Acknowledgments
The development of Cartiscope™ was supported by a Natural Science and Engineering Research Council (NSERC)/Industry (ArthroVision) grant (No CRDPJ216488-98).
We would like to thank Raymonde Grégoire and France Frenette for providing their outstanding patient support and the secretarial staff for manuscript preparation. This study was supported in part by a grant from Procter & Gamble Pharmaceuticals, Mason, Ohio, USA.
REFERENCES
Footnotes
↵* The first two authors contributed equally to this work