Article Text

Abstract
Objective To identify risk factors for injury in youth ice hockey (ie, body checking, age, player position, player experience and level of play).
Study design Systematic review and meta-analysis.
Methods A systematic review of the literature, including a meta-analysis component was completed. Ten electronic databases and the American Society for Testing and Materials Safety in Ice Hockey series (volumes 1–4) were systematically searched with strict inclusion and exclusion criteria to identify articles examining risk factors for injury in youth ice hockey.
Results Participation in games, compared with practices, was associated with an increased risk of injury in all studies examined. Age, level of play and player position produced inconsistent findings. Body checking was identified as a significant risk factor for all injuries (summary rate ratio: 2.45; 95% CI 1.7 to 3.6) and concussion (summary odds ratio: 1.71; 95% CI 1.2 to 2.44).
Conclusions Findings regarding most risk factors for injury remain inconclusive; however, body checking was found to be associated with an increased risk of injury. Policy implications regarding delaying body checking to older age groups and to only the most elite levels requires further rigorous investigation.
- Risk factors
- body checking
- ice hockey
- youth
- athletic injury
- adolescent
- safe community
- systematic review
- child
- sports
Statistics from Altmetric.com
- Risk factors
- body checking
- ice hockey
- youth
- athletic injury
- adolescent
- safe community
- systematic review
- child
- sports
Introduction
In Canada, ice hockey is one of the most popular sports for young athletes. Hockey Canada reports over 550 000 registered players under the age of 19 in 2008, and these numbers appear to be rising.1 In the USA there were 345 000 youth players registered in the same season.2 Other countries registering more than 30 000 youth players in 2008 include the Czech Republic, Finland, Russia and Sweden.3
Due to the speed of play, the equipment used, and the allowance of body checking, hockey has been recognised as a high-risk sport.4–6 Canadian data suggest that hockey injuries may account for up to 10% of all adolescent injuries.7 Injury rate estimates are high but vary significantly in the literature,8 reflecting differences in the injury definitions, age and skill level of players studied.
Considering the long-term implications of sport injuries, and their associated public health costs, much effort has been devoted to identifying risk factors for injury in this population.8 Unfortunately, with methodological discrepancies, differing injury definitions, and inconsistent reporting, the studies published to date have yielded an unclear picture of injury causation in youth hockey. Of particular interest are those risk factors which consistently emerge in the literature. An understanding of which factors are potentially modifiable is crucial in order to develop targeted interventions. To accomplish this, data from existing research must be synthesised into single measures of association between risk factors and injury outcomes, allowing for direct assessment of injury risk.
The results from the following systematic review will aid in identifying potential risk factors for youth ice hockey injuries, and in determining which risk factors provide the most promising avenues for future intervention. These findings may ultimately help to inform the policies of youth ice hockey organisations across Canada. The discussion presented may also provide the impetus to change the way epidemiological studies examining hockey injury are conducted and reported, in the interest of clarity, accuracy and consistency in this field of study.
Research objectives
The primary objective of this systematic review and meta-analysis was to identify all risk factors for injury in youth ice hockey. The secondary objective was to determine the risk factors for severe injury in this population. Directions for future research will also be discussed, based on the findings of this analysis.
Methods
Data sources
The following electronic databases were systematically searched using the terms listed in table 1: Medline (1950–present), EBM Reviews, EMBASE (1980–present), Health STAR (1966–present), PubMed (1980–present), CINAHL (1982–present), Sport Discus (1980–present), Web of Science, Dissertation Abstracts at Proquest, ASTM (American Society for Testing and Materials Safety in Ice Hockey, volumes 1–4) and Safetylit (Injury Prevention Literature update; accessed November 2008).
Medical subject headings and text words used for article extraction
Study selection criteria
The following inclusion criteria were applied to all potential articles; initial search results were screened based on a priori study selection criteria:
The article was based on primary research with original data.
The study population included youth ice hockey players (under age 18).
The outcome measure included only injuries sustained during ice hockey participation.
The study included one or more potential risk factors and/or prevention strategies for ice hockey injury.
The article was published in English.
Two independent reviewers examined all selected manuscripts, to determine whether the inclusion criteria were met. Disagreements were resolved by consensus or a third reviewer.
Data extraction
The data extracted included study design, study population, risk factor of interest measured, injury definition(s) and results. Point estimates (including 95% CIs) of odds ratios (ORs) or rate ratios (RRs) were calculated where study data were adequate to do so if these were not reported. If the authors provided any data differentiating ‘minor injury’ and ‘severe injury’, risk factors were considered for each. The quality of evidence was assessed qualitatively based on Downs and Black criteria regarding internal validity.9 The internal validity of each study was assessed based on strength of study design, quality of reporting (ie, objectives, participants, risk factor(s)/intervention, outcome measure(s), main findings, appropriate analysis, follow-up), presence of selection bias, misclassification bias and control of potential confounding. External validity was also assessed based on representativeness of study population. An overall Downs and Black score was not derived for each study as some criteria were not appropriate to assess given the nature of the observational study designs examined.
Data synthesis
Characteristics of the studies are summarised, including study design, population, risk factor of interest measured, injury definition(s) and results. When appropriate, a meta-analysis for risk factors was conducted for available outcomes to produce combined estimates of measures of effect based on a random effects model.10 Combined study estimates were based on ORs or RRs depending on the nature of the outcomes in the included studies. Only studies of equivalent effect measures were combined. Assessment of the studies with respect to internal validity is summarised. Specific recommendations are made for future research.
Results
The citations identified from the search strategy that met the inclusion criteria included 12 papers from the initial database searched (Medline (1950–present) OVID), two additional papers from EMBASE (1980–present) OVID, three additional papers from CINAHL (1982–present), one additional paper from Sport Discus (1980–present), two dissertations from Dissertation Abstracts ProQuest and two additional papers from ASTM Safety in Ice Hockey (volumes 1–4). Twenty-two studies met the criteria for inclusion in this review. The study designs, populations, injury definitions, risk factors and effect estimates are detailed in online supplemental files 1 and 2.
Injury rates
Overall injury rates ranged from 11.7 injuries per 1000 player hours11 to 34.4 per 1000 player hours,12 and from 1.18 per 100 players11 to 43.99 per 100 players.13 These injury rates must be compared with caution and within the context of the individual studies given the different definitions of injury and the different study populations.
Risk factors for injury
The most commonly investigated risk factors in the literature were age (N=8), session type (N=4), level of play (N=4), player position (N=3) and body checking (N=10). Additional factors (ie, participation in a fair play programme,14 aggression and empathy,15 weight and height,16–18 level of hockey experience,18 19 relative age20 and gender) have received limited attention and have generally produced conflicting results. The following sections outline the most commonly investigated significant risk factors for ice hockey injury.
Age and relative age
Eight of the 22 articles investigated age as a potential risk factor for injury in youth hockey. The majority (N=5) of these studies found that the risk of injury increased with increasing age.11 12 17 21 22 While these studies present compelling evidence, there are some studies that suggest there is no increased injury risk in older age groups. Roberts et al23 reported that the RR of injury in Bantam (13–14 years old) compared with Pee Wee (11–12 years old) was 0.71. Similarly, Williamson24 found that older players were at lower risk than their younger counterparts. Wattie et al,16 20 however, found no significant difference in injury risk by age group.
While chronological age is one way to examine the effect of age, relative age has been proposed as a way to examine variations within age groupings. One study identified for this review examined relative age between players competing in the same age group and found no evidence that younger or older players within a grouping were at increased injury risk.20
Session type
Injury risk was universally higher (N=4) in games than in practice or training sessions and RR estimates ranged from 2.45 to 6.32.12 17 22 25 Further, Wiggins16 reported that injury rates were higher in regular season games than in preseason, postseason or tournament games. In one study, game injuries accounted for up to 63% of all injuries.22
Level of play
Level of play was investigated in four studies. Emery and Meeuwisse22 found that players in the highest skill division were at the greatest risk of injury in Pee Wee (11–12 years old), but there was no significant increase by skill level in other age groups. The remaining three studies, however, found that risk increased with increasing skill level across age groups.13 20 26
Player position
Player position was identified as a risk factor in three studies. While both Wiggins16 and Roberts et al23 found forwards to be at higher risk of injury than defensemen and goalies, Stuart et al12 reported that the RR of injury for defensemen was 2.18 times that of forwards. In all three studies, goalies were at much lower risk than other players.
Gender
Roberts et al23 found an increased risk of injury in male players (RR=2.31) when compared to a female referent group. However, this study examined male leagues with a very small number of girls participating. As such, the sample size was not large enough to draw any conclusions about gender as a risk factor for injury.
Body weight and height
Three studies examined body size (height and/or weight) as a potential risk factor for youth ice hockey injury. Bodyweight was identified in two studies as a significant risk factor for injury as lighter players were more likely to be injured than heavier players.16 18 Brust et al17 found this to be the case at the Bantam level of play only (p=0.007), and Wiggins16 reported a significant difference in weight between those who sustained an injury due to body checking and those that did not (F1,144=7.42, p<0.01). Finke et al18 examined body weight as a risk factor for shoulder injury and found heavier players to be at greater risk. One study examined height as a possible risk factor for injury, suggesting a relationship between height and injury effect at the Bantam (13–14 years old) level of play (p=0.05).17
Injury prevention strategies
Brunelle et al14 examined a fair play programme that awarded points for good conduct based on penalty minutes. At the end of each game, the fair play points contributed to the general standings points for an overall point rating. Overall, the odds of injury in the league without the fair play programme were 2.43 times that of the league with the fair play programme, but this result was not statistically significant (OR=2.43; 95% CI 0.68 to 9.05).14
Body checking
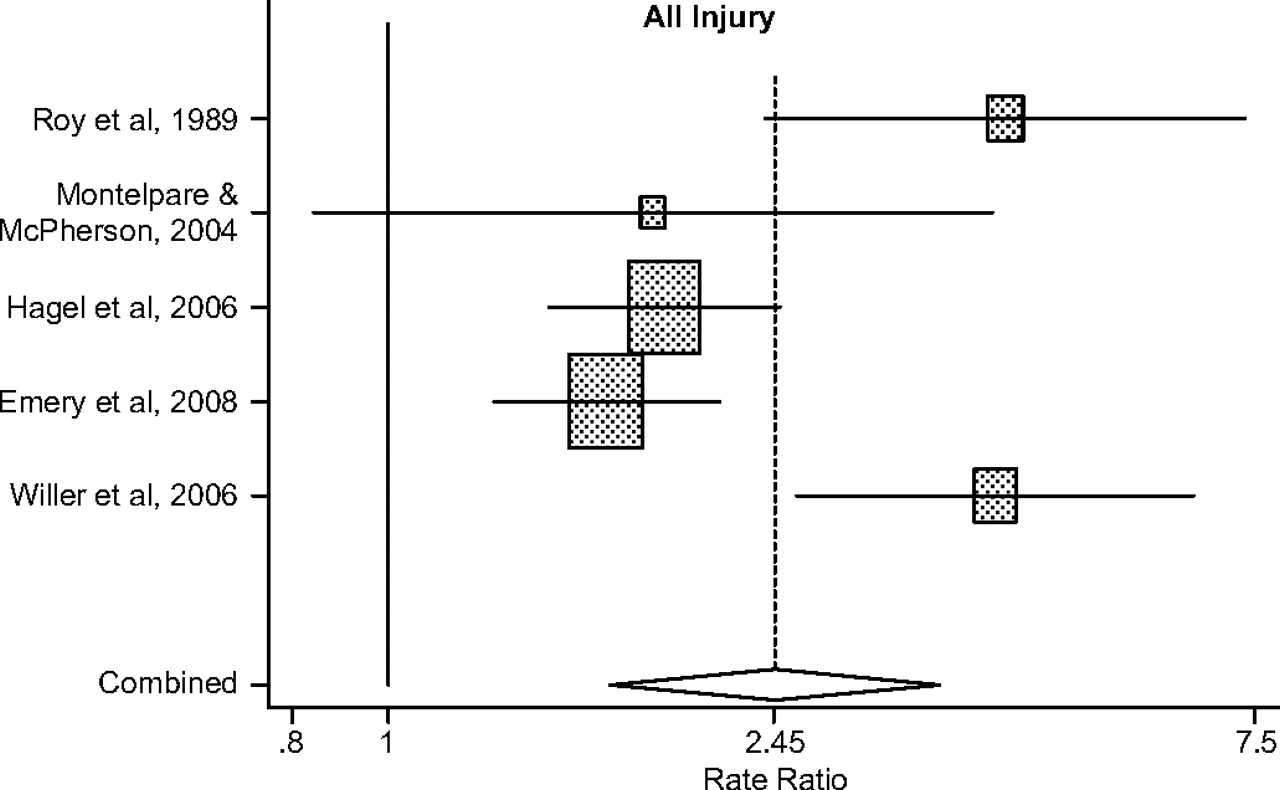
Body checking policy was included as a risk factor for injury in 10 of the 22 studies in this review.11 13 16 19 26–31 A meta-analysis was conducted in order to synthesise the varying results and increase the power available to draw a conclusion about body checking policy (ie, body checking allowed or not allowed within the rules of the league) as a risk factor. For all injury, five studies with incidence rate data were identified and a combined RR of 2.45 (95% CI 1.7 to 3.6) was estimated (figure 1). RR estimates for each of the included studies were based on the published data. The estimate from Montelpare and McPherson19 (RR=1.85; 95% CI 0.84 to 4.07) is based on the conservative subanalyses as suggested by the authors. Further, the crude combined estimate from Willer et al26 was used (RR=4.10; 95% CI 2.58 to 6.51); however, crude rate ratio estimates ranged from 1.93 (95% CI 0.64 to 5.78) in Pee Wee to 9.79 (95% CI 3.15 to 30.36) in Atom.
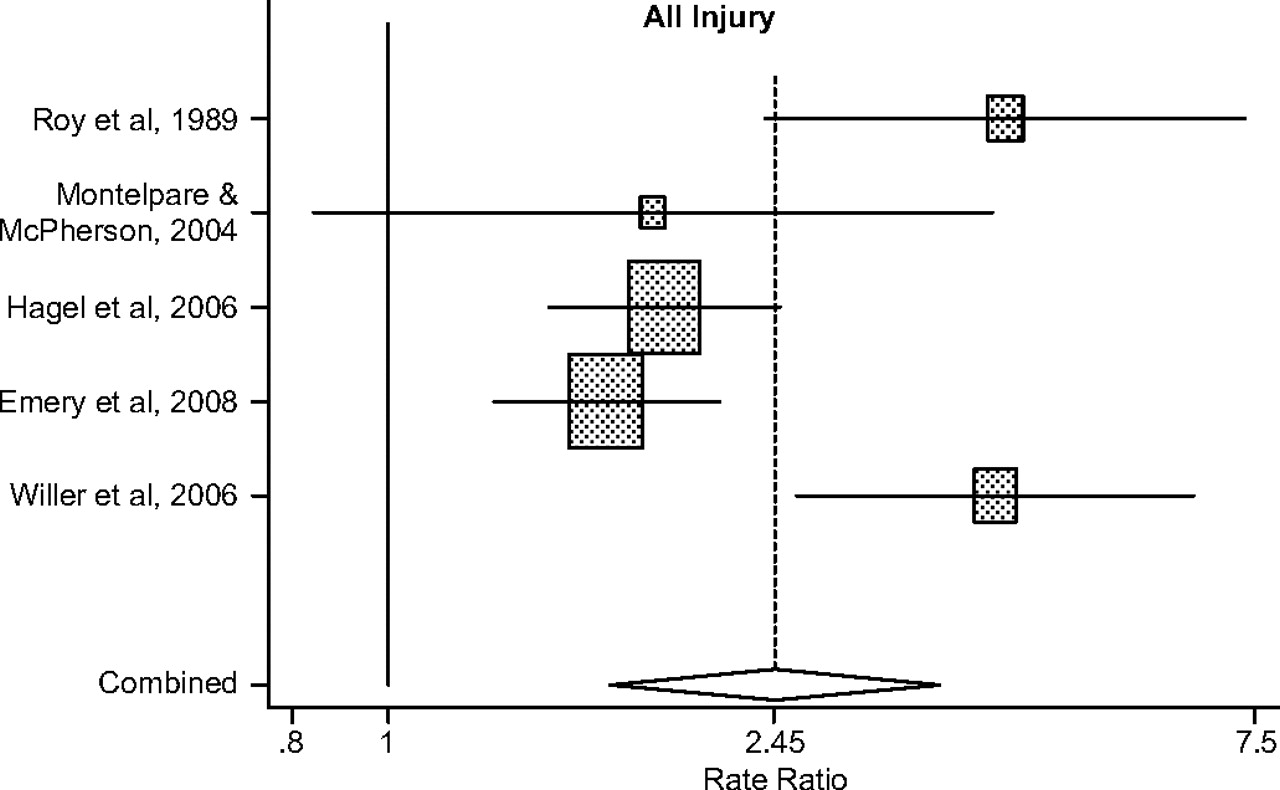
Body checking as a risk factor for all injury.
Risk factors for severe injury
Of the 22 studies identified for this review, 11 examined severe injury as a separate outcome and/or provided a severe injury definition. Definitions of severe injury differed by study and were primarily based on time loss or specific injury types such as fractures, dislocations, concussions, neck injuries or any injuries that required hospitalisation or emergency medical attention. Risk factors for severe injury consistently included age and body checking. Studies examining age as a risk factor were inconsistent. Brust et al17 found that older players were at higher risk of concussion compared with younger players. However, Emery et al22 found that players in Bantam (age 13–14) and Pee Wee (age 11–12) had a higher risk of concussion (RR=4.04 and 3.14, respectively) when compared with players in Atom (age 9–10).22 Age was found to increase the risk for all severe injury in three studies.11 22 23
Body checking policy was examined as a risk factor for severe injuries, including concussions and fractures. Hagel et al28 found that the odds of incurring a severe injury in the body checking group were 2.01 times that in the non-body checking group. Macpherson et al19 and Regnier et al30 also found an increased risk of severe injury of 1.20 and 11.7, respectively, in the body checking group, although injuries considered severe were not clearly defined in either study. To examine body checking as a risk factor for concussion, a meta-analysis of four studies was conducted and a combined OR of 1.71 (95% CI 1.2 to 2.44) was estimated (figure 2).

{kind=link}
{kind=link}
Body checking as a risk factor for concussion.
Study quality assessment
All studies identified were examined for methodological criteria related to internal and external validity as identified based on methodological criteria outlined by Downs and Black.9 An overall score was not provided for each study as some criteria were not appropriate to assess given the nature of the observational study designs examined. There was a diversity of study designs (ie, comparative case series, cross-sectional, historical cohort and cohort) used to examine risk factors for injury in youth ice hockey. All studies met the criteria for clearly describing the study's objectives, study population, main exposure(s), main outcome(s) and main findings. Eleven of the 22 studies did not provide an effect estimate12 16 18 21 23 25 29–32 and of these, six also did not report any assessment of random error (ie, confidence limits or p-values).12 21 23 30–32 Effect estimates from six studies were calculated where data were available.12 16 21 23 29 31 Other general limitations are summarised.
Discussion
Among the various risk factors examined in the literature, age, session type, level of play, player position and body checking have received the most attention. While session type has yielded the most straightforward results, and games do appear to increase risk levels, the evidence on most other factors has not provided a clear picture of injury aetiology. It is therefore important to determine which of these potential risk factors require further investigation, and which may be the most salient for predicting and preventing hockey injuries. The strength of the evidence for risk factors for injury in youth ice hockey is limited by differing research designs and injury definitions.
The examination of gender as a potential risk factor from this review suggests a possible increase in risk for male players. However, research conducted at the Canadian University varsity level of play comparing male and female injury rates (6 male and 6 female teams) found no significant difference in injury rates in these two populations (p=0.258; RR=1.18, 95% CI 0.89 to 1.57).33 Further research is required to examine risk factors in female youth ice hockey.
The role of body weight as a risk factor for ice hockey injury also remains inconclusive; however there are still large size differentials between players in some age groups. Brust,17 for example, reported a weight difference of 53 kg and a height difference of 55 cm between the largest and smallest Bantam players.17
More research is needed to determine the effect of various intervention programmes at reducing the incidence of injury. While the point estimate identified by Brunelle et al14 based on a fair play programme, which awarded points for good conduct based on penalty minutes, was not statistically significant (OR=2.43; 95% CI 0.68 to 9.05), this finding may be clinically relevant.
Injury rates in youth ice hockey also remain unclear as a result of inconsistent injury definitions, varying sample sizes and a lack of exposure data. Many studies yield injury rates per 100 players, which does not take into account exposure to risk. As such, this area of research would benefit from consistent reporting of injury rates by player hours (ie, 1000 player hours) to allow for more accurate comparisons. Further, injury definitions differed widely, affecting the ability to make accurate comparisons. Finally, because each study examined a different set of risk factors, injury rate comparisons were made based on overall injury rates without adequate control for potential confounders.
The meta-analysis examining body checking as a risk factor for injury clearly showed an increased risk of injury and concussion for the body checking groups when compared with the non-body checking groups. These meta-analyses were based on random effects models which accounted for differences in variance in each sample. As a result, these meta-analyses provide conservative combined estimates of the increased risk of injury and concussion in the body checking groups. Further, the concussion meta-analysis had one study (Roy et al31) in which the OR was below 1; however, this was based on a very small sample size (n=23), thus this result must be interpreted with caution and may be extremely conservative. Despite these conservative combined estimates, the CIs in both the injury and concussion analyses did not encompass the null; therefore, it can be concluded that body checking significantly increases the risk of injury and the odds of incurring a concussion. Although there is a relatively large body of literature examining body checking in youth ice hockey, only four studies met the inclusion criteria for each of the injury and concussion analyses. While two studies (Emery et al,22 Molsa et al11) examined body checking, they were excluded from the injury meta-analysis as these studies did not have a body checking and a non-body checking group to compare and could not control for age as a potential confounder. In addition, McKay et al13 reported a rate ratio of 5.28 (95% CI 1.27 to 46.78) associated with a body checking league; this estimate was also excluded as one must consider the implications of a self selected recreational hockey league where level of play differs considerably.
Our findings were also consistent with those recently published by Warsh et al34 who conclude, based on a descriptive systematic review of the literature, that increased injuries attributable to checking were found where checking was allowed.
Despite the number of papers examining risk factors for injury in youth ice hockey, most of these papers examine risk factor data that can be readily gathered through questionnaires (eg, age, gender, height, weight, level of play) and little attention has been paid to biological measures such as anatomical (eg, skeletal maturity), physiological (eg, endurance, flexibility, strength, neuromuscular control) and biomechanical (eg, alignment) measures. In addition, little attention has been paid to psychosocial, behavioural and sociocultural risk factors that may play a role in risk taking and injury risk in youth ice hockey. McKay et al15 examined attitudes towards body checking, levels of empathy and levels of aggression, and found none to be predictive of injuries, though the study was limited by sample size.
Strengths
This is the first comprehensive systematic review of its kind to examine all published risk factors for injury in youth ice hockey that combines the results of analytical studies to strengthen the results. Given the consistency of results examining risk factors for injury in youth ice hockey across studies and the typically large studies examining youth ice hockey players across a number of diverse regions, the findings in this systematic review are likely generalisable to youth ice hockey players in many organised leagues of play.
Limitations
Reviews and meta-analyses are subject to the same limitations present in each of the included articles. It appears that measurement bias, including self report bias, is the most prevalent bias in our review. The measurement bias with regard to injury definition would likely be non-differential as the probability of an injured player being classified as non-injured or a non-injured player being classified as injured would likely be the same regardless of risk factor category. This would push the study rate ratio estimates towards the null. The use of convenience samples in the various studies may have affected the ability to show an age or gender effect because it may not achieve a representative sample. Poor reliability of exposure measurements (ie, player weight) may have resulted in non-differential measurement bias that would also underestimate the association between exposure and injury.
The majority of studies included an entire league or randomly selected teams from a league, with fairly complete follow-up on all players and, as such, selection bias is unlikely to have affected the results. While confounding of all known risk factors was not considered in all studies, the studies examining the risk of body checking did consider the potential effects of age and level of play. For the body checking effect estimates, the factors affecting a player's decision to join a body checking league versus participating in a non-checking league were not considered and may thus represent a source of unmeasured confounding.
It must also be acknowledged that publication bias may have affected our results. Studies with significant results may be more likely to be submitted by authors and accepted for publication. However, many studies included a number of risk factors for injury in youth ice hockey, some of which were found to be significant risk factors and others not. This should, at least in part, guard against a substantial publication bias in our report.
Future directions
Given the aforementioned limitations, the field would benefit from further research on the risk factors for injury in youth ice hockey using prospective and valid injury surveillance systems. These studies should utilise definitions of injury consistent with international consensus guidelines35–37 and should take into consideration exposure (ie, player participation) data to accurately measure injury rates.
Conclusion
Despite a myriad of studies examining risk factors and injury rates in youth ice hockey, some findings remain inconclusive. A clear understanding of potentially modifiable risk factors is required in order to design, implement and evaluate appropriate interventions to reduce youth ice hockey injury. In addition, risk factors that are evidence-based but also those that have less evidence but are plausible must be considered as potential confounders or effect modifiers in evaluating any injury prevention strategy in youth ice hockey. Body checking is the single most consistent risk factor for injury in youth ice hockey. Policy implications regarding delaying body checking to older age groups and to only the most elite levels requires further rigorous investigation. Further, a clear understanding of the mechanism by which body checking increases the risk of injury is essential for informing policy. Future research utilising video-analysis to better understand injury risk behaviours and mechanisms of injury associated with the rules of the sport will better inform policy decisions related to body checking. In addition, in a unique sport culture such as youth ice hockey, psychological and sociocultural factors clearly play a role in the potential uptake of any injury prevention strategy, including policy change, and these should not be neglected in future research.
What is already known on this subject
There are high participation and injury rates in youth ice hockey.
Individual studies have provided information regarding risk factors for injury in youth ice hockey.
What this study adds
This study provides a summary of the combined evidence for all risk factors for injury in youth ice hockey.
Based on combining studies examining body checking, there is a 2.5-fold increased risk of all injury and 1.7-fold increased risk of concussion in youth ice hockey leagues where body checking is allowed.
Further research is required to examine the mechanisms and policy implications related to body checking in youth ice hockey.
Acknowledgments
Olivia McCreary and Leo Tam helped with the initial literature search, obtaining the articles and data extraction.
References
Footnotes
Funding Dr Emery and Dr Hagel are supported by a Population Health Investigator Award from the Alberta Heritage Foundation for Medical Research. Dr Emery also holds and a New Investigator Award from the Canadian Institutes of Health Research and a Professorship in Paediatric Rehabilitation funded through the Alberta Children's Hospital Foundation. Dr Hagel holds a Professorship in Child Health and Wellness funded by the Alberta Children's Hospital Foundation, through the support of an anonymous donor and Canadian National Railway Company. Melissa Decloe's MSc was supported by the Social Sciences and Humanities Research Council of Canada (SSHRCC), a Department of Paediatrics Child Health Research Group Scholarship and the Joanne A. Vincenten Scholarship from the Alberta Centre for Injury Control. Carly McKay is supported by SSHRCC.
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.