Article Text

Abstract
Introduction Basketball is a contact sport with complex movements that include jumps, turns and changes in direction, which cause frequent musculoskeletal injuries in all regions of the body.
Objective This is an integrative systematic review of the epidemiology of musculoskeletal injuries in basketball.
Methods This is an integrative review based on the following sources of information: PubMed/MEDLINE, Embase, LILACS, BBO-Biblioteca Brasileira de Odontologia, IBECS-Índice Bibliográfico Espanhol em Ciências da Saúde, nursing journals, dental journals and core clinical journals in the last 10 years with studies addressing the general epidemiology of sports injuries in basketball.
Results In total, 268 articles were selected, of which 11 were eligible for the integrative review. A total of 12 960 injuries were observed, most of which occurred in the lower limbs (63.7%), with 2832 (21.9%) ankle injuries and 2305 (17.8%) knee injuries. Injuries in the upper limbs represented 12%–14% of the total injuries. Children and adolescents received head injuries more often compared with the other age and skill categories. In the adult category, there was an increased prevalence of injuries in the trunk and spine. In the upper limbs, hands, fingers and wrists were affected more frequently than the shoulders, arms and forearms. In the masters’ category, there was an increase in the incidence of thigh injuries.
Conclusion The lower limbs were the most affected, with the ankle and knee joints having the highest prevalence of injuries regardless of gender and category. Further randomised studies, increased surveillance and epidemiological data collection are necessary to improve knowledge on sports injuries in basketball and to validate the effectiveness of preventive interventions.
- basketball
- epidemiology
- athletic injuries
- sprains and strains
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Created in the USA more than a century ago by James Naismith,1 basketball has become one of the most popular sports in the world, particularly in the USA.2 3 In Brazil, basketball is one of the four most popular sports according to the Ministry of Sports.4
Despite all the benefits resulting from participation in sports—such as improved body composition, cardiorespiratory function, increased strength, improved self-esteem/psychosocial well-being, weight control, and less abuse of alcohol and drugs, among others5–7—participating in a sport with so much physical demand, such as basketball, where the athlete performs repetitive jumps during games and training, abrupt changes in direction, running and deceleration,8 may result in a greater risk of injury. This leads to an increase in health expenses and visits to doctors and hospitals, reduction in court time, and increased risk of new injuries.9 10
Several studies have already been published describing injuries in basketball. Some focus on professional athletes,11 others focus on college students12 or high school students,13 14 and others on adult athletes.15 Some studies focus only on a specific region of the body or a specific diagnosis, such as concussion,16 shoulder17 or ankle injury,18 and many compare injury rates between sexes.19
The understanding of basketball injury epidemiology is an important first step in the development of targeted, evidence-based interventions to provide recommendations for injury prevention. The objective of this study was to perform an integrative review of the epidemiology of musculoskeletal injuries in basketball.
Methodology
Literature search
An electronic search was performed in the following databases: PubMed/MEDLINE, Embase, LILACS, and thematic databases included in the Portal de Pesquisa da Biblioteca Virtual em Saúde (Virtual Health Library Research Portal): BBO-Biblioteca Brasileira de Odontologia (Brazilian Library of Dentistry) and IBECS-Índice Bibliográfico Espanhol em Ciências da Saúde (Spanish Bibliographic Index in Health Sciences). Other sources of information were also included, such as nursing journals, dental journals, core clinical journals, and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES; Brazilian Federal Agency for the Support and Evaluation of Graduate Education) Thesis Bank, which is a representative of the so-called grey literature and internet sites. Language or region filters were not included. The elaboration of the search strategies gave the research greater sensitivity by combining the terms extracted from the DeCS/MesH and synonyms: basketball, epidemiology, athletic injuries, sprains and strains. Thus, the eligibility criterion was to identify articles that discussed the general epidemiology of sports injuries in basketball.
To determine whether a study should be included, the titles and abstracts of all references obtained were evaluated by two medical reviewers. The extracted studies were assessed based on the inclusion and exclusion criteria. The inclusion criteria were as follows: (1) articles published in the last 10 years; (2) studies addressing the general epidemiology of sports injuries in basketball; and (3) athletes of any age, of both sexes, and professional, amateur and recreational basketball practitioners. The exclusion criteria were as follows: (1) review articles; (2) case reports; (3) articles dealing with Paralympic sports; (4) studies on the general epidemiology of sports injuries, including basketball, that did not present specific injury percentages for each sport; (5) items that solely addressed some type of specific basketball injury, for example, articles reporting knee injuries in basketball, or basketball dental injuries and basketball concussions; (6) articles that presented in the results section the percentages of the injuries without specifying the region of the body (eg, foot, ankle, knee and so on), referring to only general terms as upper limbs, lower limbs and trunk; and (7) articles that only addressed more prevalent injuries in emergency departments or surgical basketball injuries because these data reveal a portion of possible basketball injuries rather than overall totality/epidemiology. The possible inconsistencies were identified, discussed and resolved by consensus.
Procedures for creating the database
To create this database, the following steps were taken: (1) extraction of the number of injuries detailed by the site of each study—when the study did not present the total number of injuries but did report the relative frequency, the absolute frequencies were computed by multiplying the total number of injuries by the relative frequencies; (2) checking and rechecking of total injuries in each study; and (3) organisation of the total absolute frequencies, by sex and by category of the participant.
Eleven studies were included in this review, as shown in figure 1. The main characteristics of the studies included in the integrative review are described in table 1.

Selection of the studies surveyed in the electronic databases and grey literature. Preferred Reporting Items for Systematic Reviews and Meta-Analyses algorithm. BBO, Biblioteca Brasileira de Odontologia (Brazilian Library of Dentistry); IBECS, Índice Bibliográfico Espanhol em Ciências da Saúde (Spanish Bibliographic Index in Health Sciences).
Main characteristics of the studies included in the integrative review on basketball epidemiology
The objectives of the 11 studies included in the analysis (table 1) were as follows: to verify the association between game schedule and injuries; to compare basketball with other sports/physical activities or sports; to compare subsequent injuries among sports; to verify differences in injuries between sexes; to compare injury patterns in emergency departments and in the athletic training setting; to assess the incidence of injuries; and to assess the association between physical activity level, physical activity dependence and injuries with the dimensions related to the perception of health-related quality of life and health. Despite the different objectives of the included studies, in all studies it was possible to verify the number of basketball injuries in each part of the body, either through the absolute number that was indicated in the study or through the absolute frequencies multiplied by the total number of injuries. In this way, the following results were obtained.
Inferential procedures
In the inferential analysis, the following software were used: R (V.3.3.2) and RStudio (V.1.0.136). The ‘meta’ library was adopted for the estimation of meta-analysis models. The overall proportions of knee and ankle and foot injuries were estimated, along with the respective CIs and weights for each study. Tests were also performed to verify whether the OR between injuries at different sites was the same (OR=1). For this analysis, the knee was adopted as a reference site.
Results
Characteristics of the identified studies
Descriptive statistics of the studies
A total of 268 articles were selected, of which 11 articles were eligible for the integrative review. Of the studies included in the study, it was possible to extract the number of absolute injuries in females in seven studies.20–26 For males, five studies were used to extract the number of injuries.20 24 26–28 Two other studies did not specify the gender, and the data were only used for the total sum of the injuries.29 30
With regard to the region of the participants, seven (63.6%) studies were from the USA, two (18.2%) were from Brazil, one (9.1%) was from France and one (9.1%) was from Nigeria. With regard to the age and level of skill category, most of the studies addressed injuries in adolescents (45.5%, 5 studies), followed by injuries in professionals (36.4%, 4 studies, table 1). Children and masters were cited in only one study each, which represented 9.1% and 9.1% of the studies, respectively.
Descriptive statistics of injuries
In total, 12 960 injuries were computed and extracted from the studies (table 2). The knee and the ankle were the most affected sites, with 2832 (21.9%) and 2305 (17.8%) injuries, respectively. When analysed separately, this trend was repeated for injuries in both females and males. With regard to injuries in females, 19.5% of injuries occurred in the ankle and 20.6% occurred in the knee. The third most affected region in females was the thigh, hip and leg, which accounted for 17.5% of injuries. In males, 28.4% of injuries occurred in the ankle and foot, followed by the thigh, hip and leg (19.3%) and the knee (17.5%). When the injuries were analysed according to the age/level of skill category, the site with the most injuries in children and adolescents was the ankle and the foot (37.7%, 2807 injuries), followed by the knee (16.3%, 1214 injuries), head and neck (13.7%, 1024 injuries), and the hands, fingers and wrists (8.9%, 662 injuries). For professional athletes, the injury frequencies were as follows: 24.8% (1310 injuries) of injuries occurred in the foot and the ankle, followed by the thigh, hip and leg with 1074 injuries (20.4%), the knee with 19.5% (1027 injuries), and the trunk and spine with 586 injuries (11.1%). Only one study referred to the masters’ category, and in this study 31.4% of the injuries (75 injuries) occurred in the thigh, hip and leg, followed by the knees with 64 injuries (26.8%) and the ankle and the foot with 39 injuries (16.3%) (table 2).
Injury percentages by anatomical segments in relation to total number, female sex, male sex, children and adolescents, professionals, and masters
Inferential analysis
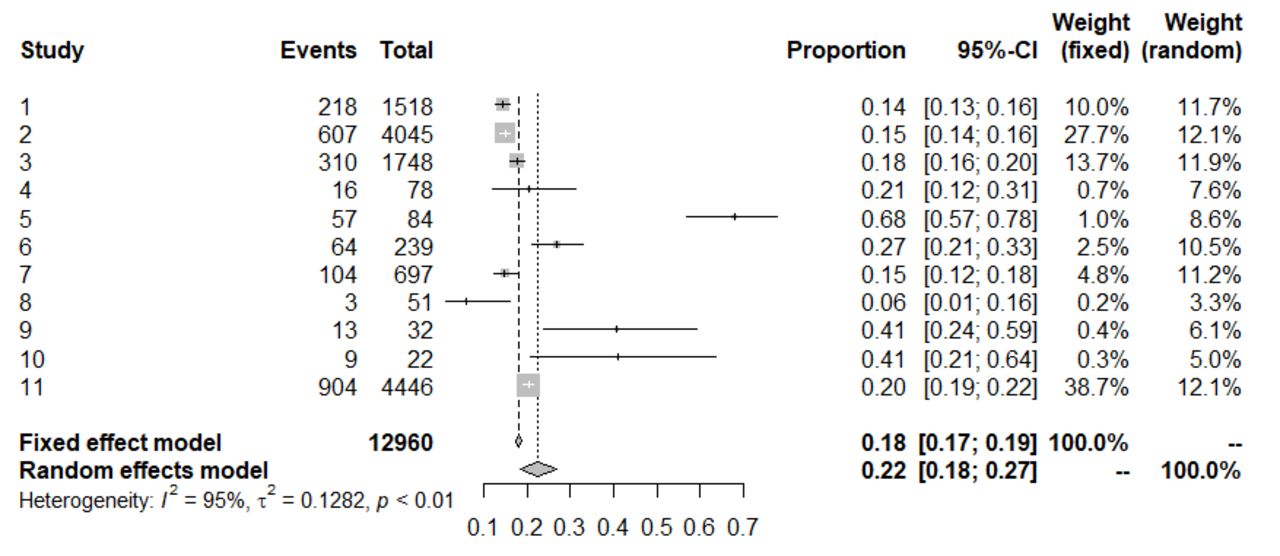
The proportions of injuries were estimated by meta-analysis models, which weighted injury frequencies by study sizes. Figure 2 presents the proportions of knee and ankle and foot injuries estimated by fixed-effects and random-effects models and the CIs and weight of each study in this estimation. Notably, there is significant heterogeneity in the studies, measured by the I2 statistic (95% and 97%, respectively). The estimated proportion of knee injuries was 0.18 (95% CI 0.17 to 0.19) for the fixed-effects model and 0.22 (95% CI 0.18 to 0.27) for the random-effects model. The estimated proportion of ankle and foot injuries was 0.33 (95% CI 0.32 to 0.33) for the fixed-effects model and 0.29 (95% CI 0.24 to 0.34) for the random-effects model.

{kind=link}
{kind=link}
Proportions of knee and ankle and foot injuries estimated by fixed-effects and random-effects models and the CIs and weight of each study in this estimation knee.
ORs between injury sites
The ORs between injuries were also estimated using a meta-analysis model, using knee injuries as the reference, which was the most frequent site of injury. With ankle and foot combined, this category of injuries proportionally exceeded that of knee injuries. However, this category is less specific.
The results of the OR comparison tests in the fixed-effect models are presented in table 3. The test evaluates whether the OR is equal to 1 and rejects the hypothesis in cases of low p values (p<0.05). All OR values were greater than 1, except for the ankle and foot, which had a value less than 1. The p value for all comparisons was statistically significant (p<0.0001). Thus, the probability of knee injury was greater than the probability of injury to the thigh, hip and leg, head and neck, trunk and spine, shoulder arm and forearm, and hands, fingers and wrists. The probability of knee injury was only lower than the probability of ankle or foot injury. It was not possible to calculate the comparisons of knee with ankle only and knee with foot only using the set of studies.
Estimated values of OR compared with knee injuries, limits of the 95% CI and p value for the hypothesis of OR=1
Discussion
In this study, more than 12 000 basketball injuries were analysed from the 11 included studies, and the results showed that there were more injuries in the lower limbs (63.7% of the injuries), regardless of gender (male, 65.2%; female, 68.4%) or level (professionals 64.7%, master 74.5%, and children and adolescents 62.5%). These data are in accordance with the literature.31–33 In a Women’s National Basketball Association and NBA six-season retrospective study, Deitch et al 24 concluded that the lower limbs (65%) were the most common site of injury in basketball. Of the 5272 injuries of the professional category included in this study, 3411 occurred in the lower limbs, representing 64.7% of the total injuries reported.
According to the specific anatomical region, the largest proportion of injuries occurred in the ankle (2832 injuries, 21.9%), followed by the knee (2305 injuries, 17.8%). Most authors point to the ankle as the most common site of injury13 14 31–34; however, some authors report that the knee is the most affected region.35 36
When analysed separately, 19.5% of injuries occurred in the ankle and 20.6% in the knee in females, whereas these values were 14.6% and 17.5% in males, respectively. In the children and adolescent category, ankle injuries accounted for 25.6% and knee injuries accounted for 16.3%. In professionals, ankle and knee injuries accounted for 17.5% and 19.5% of all injuries, respectively. Finally, in master athletes, knee injuries accounted for 26.8%, and foot and ankle injuries accounted for 16.3%. It was not possible to differentiate between foot and ankle injuries for the masters’ category. In that category, only one study and a small number of injuries were found compared with the other categories. The percentages in knee and ankle injuries varied between the sexes and the levels of sport, making it difficult to affirm which is the most prevalent, as previously described.
Both knee and ankle injuries are the most prevalent. As shown by the inferential analysis and the OR values (table 3), which uses knee injuries as a reference and compares it with the other anatomical regions categorised in this study, the probability of knee injury occurring is higher than that of all regions except for the ankle and foot, which is statistically significant because in all comparisons p was <0.001.
Because basketball is a sport that involves sudden changes in direction, side shifts, jumps, and more importantly landings, these results are not surprising. It would be logical and expected that injuries in the lower limbs would be the most prevalent.8
With regard to upper limb injuries, injuries to the hands, fingers and wrists (1133, 8.7%) predominated over shoulder, arm and forearm injuries (585, 4.5%).37 This was observed in all categories analysed: for females, hands, fingers and wrists represented 8.6% (369) of injuries, and shoulders, arms and forearms represented 4.2% (182) of injuries; for males, hands, fingers and wrists represented 8.4% (386) of injuries, and shoulders, arms and forearms represented 5.8% (267) of injuries. For the age/level of skill categories, the data were similar except for the masters’ category, which presented essentially the same number of injuries in the hands, fingers and wrists, and in the shoulder, arm and forearm. However, for this category, only one study and a small number of injuries were reported. For children and adolescents, injuries in the hands, fingers and wrists represented 8.9% (662) of injuries, and injuries in the shoulders, arms and forearms represented 3.2% (238) of injuries. For professionals, injuries in the hands, fingers and wrists represented 8.6% (454) of injuries, and injuries in the shoulder, arm and forearm represented 6.2% (328) of injuries. For masters, injuries in the hands, fingers and wrists represented 7.1% (17) of injuries, and injuries in the shoulders, arms and forearms represented 7.9% (19) of injuries. These data are also consistent with the literature, with some studies reporting 12%–14% of injuries occurring in the upper limbs.33 38
The percentage of injuries in the upper limbs increases when the sample is obtained from emergency departments, as reported by the studies.39 40 When hand, finger and wrist injuries were analysed separately among children and adolescents and professionals, 662 injuries occurred in children and adolescents and 454 occurred in professionals. These numbers represent 50.81% and 49.19% of all injuries in children and adolescents and professionals, respectively. Therefore, for these categories, the probability of injury to the hands, fingers and wrists is the same.
Considering the importance of the increase in the diagnosis of concussions, a brief analysis of the injuries in this anatomical region is valid, although combined with neck injuries. In total, there were 1468 injuries in this region, representing 11.3% of total injuries. In females, 417 injuries (9.7%) occurred in this region, and in males 384 injuries (8.3%) occurred in this region. Because in some studies it was not possible to differentiate injuries by sex, the sum of injuries between males and females was not equal to the total injuries reported. The value reported by the studies for the injuries in these anatomical regions varied between 8.9% and 14%.24 31–33
Excluding the masters’ class, which had a much smaller number of reported injuries, head and neck injuries were compared between the professional and children and adolescents categories, with 437 and 1024 injuries, respectively. Proportionally, in relation to the total number of injuries reported by each category, these numbers represent 62% and 38% of injuries in children and adolescents and adults, respectively. Therefore, there is a tendency for children and adolescents to suffer more head and neck injuries than those in the professional category. There is also a study showing that this is a trend in teenage male basketball players because of the increase in the level of physical contact now observed among players of this category.31
A total of 975 injuries occurred in the trunk and spine, representing 7.5% of all injuries. Of these 975 injuries, only 371 occurred in children and adolescents, and 586 occurred in professionals. Of the total trunk and spine injuries reported, 31% and 69% occurred in children and adolescents and professionals, respectively. A higher prevalence of trunk and spine injuries was observed in professionals.
Only 5% of all injuries reported for children and adolescents occurred in the trunk and spine. For professionals, this number was 11.1%. According to Starkey33 in a study on NBA players, only 6.9% of all injuries occurred in this region; however, only injuries to the lumbar and thoracic spine were counted, and other injuries that occurred in the trunk were not considered. This fact could explain the observed difference between the values reproduced by this study and the study by Starkey.33
Other authors have obtained results for adolescents in which trunk and spine injuries account for 11.4% to 13.5% of all injuries.31 32 In this study, there was not a category for adolescents only, which could explain the difference in results: adolescents may have a greater proportion of injuries in the trunk and spine compared with the group of children and adolescents together. Because adolescence is an intermediary phase between the child and the adult phases, it seems logical that adolescents have a higher spinal injury rate than children. The trunk and spine was the fourth most prevalent injury region in professionals. For the masters’ category, only 18 trunk and spine injuries were reported; this number is very small compared with the other categories. Again, this occurred because there was only one study reporting injuries in the masters’ category.
Limitations of the study
Among the existing limitations is the fact that after applying the search strategy, only one study was found in the masters’ category and it included only male athletes, accounting for a total of 239 injuries. In addition, only one study in the children category was also found, with only 84 injuries in 162 female athletes. For the descriptive statistics of the injuries, the study with children was included along with the adolescents’ category, resulting in 7449 injuries among children and adolescents.
Another limitation was the set-up of the database: because each study used a standard to divide the injuries between the various parts of the body, some regions were common, such as the knee. However, the injuries were often grouped into categories such as the foot and ankle and trunk and spine. These regions were divided according to the previous tables, minimising possible errors, but at times it was impossible to differentiate injuries grouped into specific categories, such as separating foot and ankle injuries in some studies. Other times, injuries classified as head and thorax in the original study were included in the head and neck category.
The most adequate technique for the calculation of this epidemiology would be the injury index given the athlete’s exposure (in game, training or total) per thousand hours. Limitations prevented calculating the index of injuries due to the athlete’s exposure, given the different calculation methods. To obtain this index, each athlete’s hours spent training or playing and the number of injuries must be considered. Not all studies have reported this injury index given the athlete’s exposure. Additionally, there was great heterogeneity in the studies, measured by the I2 statistic (95% and 97%, respectively).
Conclusion
Knowledge of the general epidemiology of basketball injuries is a first step for effective preventive measures to be implemented to reduce the incidence of injuries and their losses, including expenses associated with doctors, hospitals and athletes’ leave of absence. The lower limbs are the most affected injury region in basketball players, regardless of sex and category. Within anatomical regions, knee and ankle injuries are the most prevalent. The probability of injury to the hands, fingers and wrist is the same for children, teenagers and professional adults. In the category of children and adolescents, there was a higher prevalence of head and neck injuries compared with the other categories. For professionals, there was a higher prevalence of trunk and spine injuries.
References
Footnotes
Contributors Federal University of São Paulo.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.