Article Text

Abstract
Background Participation in sports as a child improves physical and psychological health. Schools need to promote sport while protecting against injury. It is not clear whether increasing evidence on injury prevention generated from professional sport is influencing school sports practices. This study reviewed policies promoting sport safety in schools to determine whether exposure to injury risk is recognised and whether evidence based prevention and management are included.
Methods A search strategy to identify policies for children aged 4–18 years was applied to electronic databases and grey literature sources. Safeguarding policies were excluded. Included policies were critically appraised and synthesised using modified framework analysis.
Results Twenty-six policies were analysed. Most (57.7%) were from the USA. Ten (38.5%) focused solely on concussion. Synthesis identified primary, secondary and tertiary injury prevention measures relating to people (staff, students and parents), systems, school physical environment and national-level factors.
Conclusions Robust, evidence-based policies for reducing injury risk in school sports are limited. Guidelines with the largest evidence base were focused on concussion, with other school sport guidelines showing limited inclusion of evidence. Where included, evidence focused on injury management rather than prevention and frequently applied evidence from adult to children. Guidance was not specific to the child’s age, gender or developmental stage.
- primary school
- secondary school
- school
- children
- injury prevention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Sporting injuries can have significant effects on society and individuals. Schools often follow health and safety guidance, yet practice is infrequently based on research evidence. Effective interventions for preventing injuries exist.
What are the main findings?
In this original overview of existing polices on the prevention of sports injuries for schools, we found a paucity of evidence-based guidelines.
The need to evaluate the effectiveness of guidelines and to establish injury surveillance were not adequately recognised.
The review highlights the need for guidelines that incorporate existing and emerging evidence on effective school sports injury prevention.
Further research should explore the impact of age, gender and stage of development on the effectiveness of new interventions for children.
Background
Participation of children and young people in sport helps prevent obesity, improves physical and mental health1–3 and is associated with higher physical activity levels as an adult.4 5 Consequently, governments internationally are producing strategies to increase sports participation.6–8 Sports are an important cause of injuries among children, and injuries can lead to reduced participation in, or withdrawal from, sports.9 10 Although it is often assumed that sports injuries are the results of ‘accidents’, they are more often the result of circumstances that predictably lead to injuries. Routine injury surveillance data are not available in the UK,11 but estimates show that 8% of children drop out of sport altogether due to injuries.12 Furthermore, sports injuries generate significant costs for the National Health Service9 and indirect costs through parents taking time off to care for injured children.9 13 There have been calls for effective policies and interventions aimed at reducing injury rates to be introduced alongside or integrated into policies promoting participation in sport.9 10
Schools have a direct duty of care towards children and have responsibility to both encourage physical activity and protect children from injury. The school environment offers all children an opportunity to participate in sport.14 However, school sport has particular risks for injury due to the wide range of experience and fitness of participants, and multiple providers, both school teachers and external coaches, organising and facilitating training.15 Students with less experience, decreased endurance or previous injuries are at higher risk of becoming injured.16
Head injuries associated with concussion have received more attention than other sports injuries. Pollock et al have argued for greater injury surveillance of concussive injuries to inform policy and practice, highlighting the issue to the public media.17 18 Increased awareness of chronic traumatic encephalopathy in American football players alerted the rugby game to the risks of concussion. There has been a resultant increase in concussion guidelines in UK rugby.19 Evidence shows that exercise-based injury prevention schemes for children and adolescents can reduce injury by up to 46%,10 but there is little known about how changes within the professional game have influenced sports undertaken within the school environment.
Schools need clear guidance on how to optimise safe and widespread participation in sports. In the absence of published summaries of policies available for schools to help them provide safe sports for children, we undertook a study to systematically identify and review policies, guidelines and consensus statements designed to enable schools to deliver school sports safely. This review aimed to better understand the extent to which such policies are informed by the scientific evidence base and to identify areas for focused research and policy improvements.
Methods
Inclusion criteria
Policies, guidelines and consensus statements on school sport injury prevention were all eligible for inclusion. To improve sensitivity of the search strategy, all terms were used to identify any document that may provide guidance for schools and were not primary research intervention studies. Policies, guidelines and consensus statements (hereafter referred to as ‘guidelines’ as this was the most common document type included) focusing on sports for children aged 4–18 years undertaken as a compulsory part of the school curriculum and that reported actions to enable the reduction and/or monitoring of physical sports-related injuries were included. We sought guidelines aimed at professionals working in either state or private schools that addressed injury risks across a range of different sports. All-age guidelines (ie, adults and children) were included provided child-specific recommendations were available or could be extracted separately.
Exclusion criteria
We excluded guidelines published before 1990, the year the National Curriculum was introduced in Great Britain20 to ensure that guidelines were relevant within the current school environment. An English language restriction was applied. Exclusions included guidelines focusing on safeguarding as these were outside the scope of the review and older versions of current guidelines in order to avoid duplication of findings. In addition, guidelines specifically written to optimise clinical care pathways were excluded as these are not applicable within schools. Guidelines focusing on only one sport, such as the ‘Headcase’ resources from Rugby England,21 were also outside the scope of the review as we focused on guidelines for school sports generally.
Search strategy
A search strategy was developed in Embase, adapted for nine other electronic databases (see online supplementary appendix 1) and incorporated published search filters where possible. The following databases were searched between August and October 2016: Embase (1974–2016), MEDLINE (1980–2016), Social Policy and Practice (1981–2016), Sports Discus (1990–2016), Cumulative Index to Nursing and Allied Health Literature (1982–2016), Educational Resources Information Center (1980–2016), Physiotherapy Evidence Database (1980–2016), Cochrane Database of Systematic Reviews (1980–2016), Evidence for Policy and Practice Information and Co-ordinating Centre (1990–2016) and Safety Lit (1990–2016). A comprehensive grey literature search was developed that included searching reference lists of included guidelines, proceedings of injury conferences and websites of relevant UK Government, sports and non-governmental organisations. To identify grey literature from other Organisation for Economic Co-operation and Development (OECD) countries, we searched the internet using the terms ‘country name’ and ‘safe school sports’ or ‘sports injury prevention’ (online supplementary appendix 2).
online supplementary appendix 1.
online supplementary appendix 2.
online supplementary appendix 3.
online supplementary appendix 4.
Titles and abstracts of potentially eligible documents were screened to identify guidelines meeting inclusion criteria. Full texts were obtained where necessary. Guidelines of uncertain eligibility were discussed within the research team. Authors were contacted for clarification where possible. The initial list of included guidelines was reviewed by two independent expert contacts; no omissions or additional texts were identified. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews were followed.22
Quality appraisal
Guidelines meeting all inclusion criteria were quality appraised against seven criteria using a modified TAPUPAS framework,23 24 which enabled a maximum score of 21 (online supplementary appendix 3). All guidelines were scored by AG, and quality scores were independently verified by JM. Guidelines scoring below 11 were deemed to be at higher risk of bias and were discussed with all authors before exclusion from the synthesis. If guideline development methods were poorly reported, authors were emailed, and the quality score was adjusted if additional methods were supplied.
Analysis
Synthesis was achieved using a modified framework analysis method developed from the framework analysis described by Brunton et al 25 and modified to fit the context considering key injury prevention opportunities identified by Dougherty.15 The framework consists of primary (reduction of injury risk/prevention of injury event), secondary (minimisation of injury sustained) and tertiary (minimisation of impact from injury) prevention measures classified into people factors (staff, students and parents), system factors, school physical environment factors and national-level factors. AG coded all included guidelines. Fifteen per cent were double coded by MVH to ensure consistency in application of the coding framework.
Findings
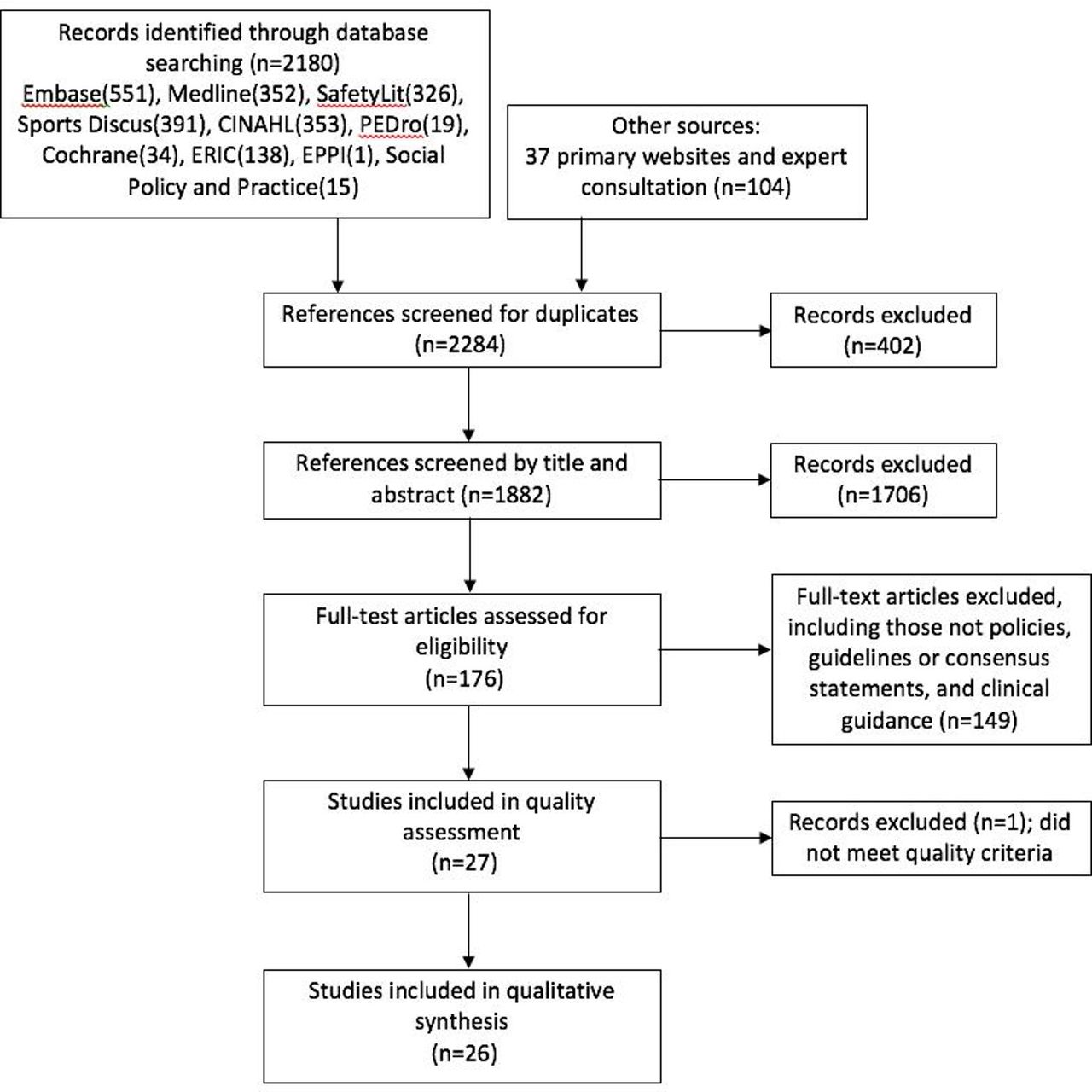
A total of 27 policies, guidelines and consensus statements were identified meeting the inclusion criteria (online supplementary appendix 4). One document was excluded due to a quality score of 10. Of the remaining 26 documents, the majority were described by authors as guidelines (n=21),26–46 with two position statements,47 48 one policy49 and two consensus statements.50 51 See figure 1 for PRISMA diagram.

PRISMA flow diagram illustrating identification of included guidelines. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Guidelines were heterogenous with regards to scope, length (2–500 pages), level of detail reported, country of origin and methods of development. Four guidelines specifically referred to physical education classes,26–28 44 52 with six broadly covering safe sports in the school environment.29–32 38 49 Three guidelines produced by the National Athletic Trainers Association in the USA focused only on emergency planning, ‘accountability for the management of emergencies’.34 35 50 Sixteen guidelines included guidance on prevention of concussion and were therefore afforded a concussion-specific analysis.
Guidelines originated from the USA (n=15),29 31–38 43 45–48 50 the UK (n=3),26 39 40 Canada (n=5),27 28 41 42 44 52 Australia (n=1),30 New Zealand (n=1)49 and one international consensus statement.51 Documents were produced by national professional associations (n=9),26 31 33–36 46 47 50 health organisations (n=5),30 37 38 43 48 national sports organisations (n=3),32 39 40 research organisations (n=2),41 42 statutory bodies (n=3),29 45 49 non-profit organisations (n=3)27 28 44 52 and one international consensus statement,51 Guidelines used a range of methods, including literature review and expert consultation (n=12),29 33–36 41 42 45 46 48 50 51 expert consultation and case law review (n=5)26–28 31 44 52 or expert consultation only (n=1).40 The remaining guidelines did not report methods of development.30 32 37–39 43 47 49
Table 1 illustrates key findings in the framework analysis. Consistent recommendations to reduce injury risk included the need for appropriately trained staff and sessions that include a warm-up, cool-down and skills progression (through both the session and the season) appropriate to the level of the participants. Little evidence was referenced to support these recommendations.
Injury and injury event prevention methods reported across >1 guideline
Two themes cut across more than one source, or level of prevention: distribution of responsibilities for injury prevention and emergency planning.
The responsibility for sports injury prevention varied throughout the included guidelines. Nine documents recommended that staff should be aware of students’ medical histories with either parents or teachers responsible for providing the information.27 28 30–32 35 37 38 50 Furthermore, there is inconsistency between guidelines as to who is responsible for providing personal protective equipment with schools (n=3)29 35 38 or parents (n=1)32 suggested. However, some guidelines are vague with no specific responsibility attributed for these roles.
Nine guidelines made recommendations for emergency planning. The common themes for a successful emergency action plan included developing the plan in conjunction with schools, teachers and local emergency services (n=7),27 28 33–35 47 49 communicating and distributing the plan to all stakeholders (n=5)30 32 34 35 49 and including regular staff education of management of an emergency (n=4).32 34 35 49
Concussion
A concussion-specific analysis was completed as this was the topic with most evidence for policy. Ten guidelines referred solely to concussion,39–46 48 51 52 with a further six guidelines referring to aspects of concussion prevention, identification and management.26 29–32 35 Some guidelines contained 1–2 sentences on concussion,30 32 where others were entire guidelines focusing on only one aspect such as safely returning children to school or activity after concussion.41–43
There is consensus that there should be immediate removal from play of any participant with suspected concussion and that any child with a suspected concussion should not return to play that day (n=13).26 29–32 35 39 40 44–46 48 51 52 Seven guidelines discuss the use of specific assessment tools for players with suspected concussion including Maddock’s questions,39 Standardised Assessment of Concussion (SAC),48 Balance Error Scoring System (BESS),48 Sport Concussion Assessment Tool 3 (SCAT3),35 51 Sensory Organisation Test (SOT),48 Post-concussion Scale48 and a graded symptom checklist.48 It was outside the scope of this review to analyse these tools.
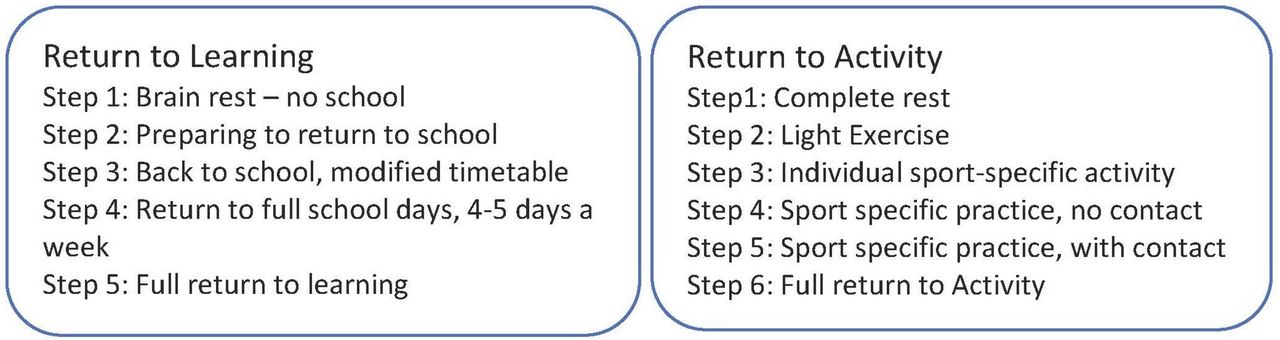
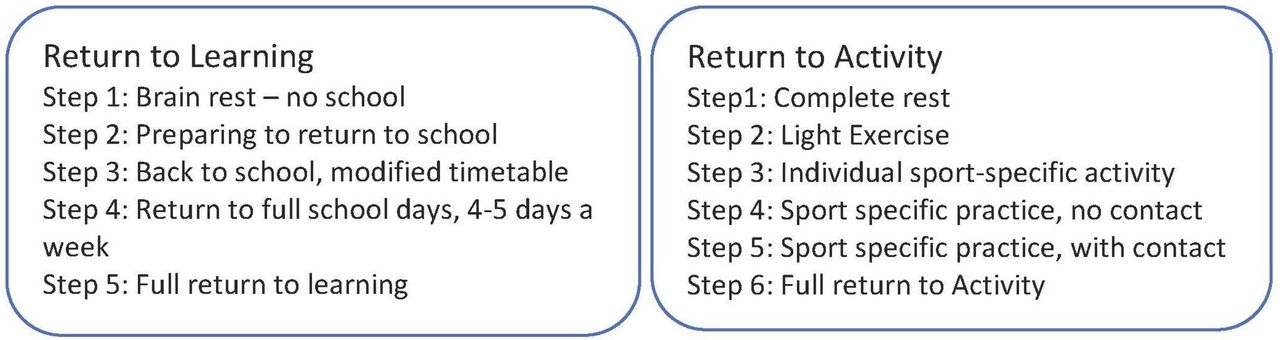
Regarding returning to learning and activity after concussion, most guidelines detailed the need for individualised return to learning (n=10)26 32 39–41 43–46 51 52 and return to activity (n=13)26 29 32 35 39 40 42–46 48 51 52 plans for children with concussion, developed jointly between parents, medical staff and school staff. Return to any activity was not recommended until return to learning had been completed.26 39 40 42 51
A five-step plan was commonly recommended for return to learning, and a six-step plan for return to activity (see figure 2). DeMatteo et al’s41 protocol was the only guideline to limit step 1 to 2 weeks due to risk of depression for children kept away from school.
{kind=link}
{kind=link}
A typical return to learning and return to activity plan.38 39 At each stage a child should be symptom free for 24 hours before progressing to the next stage.
The most frequently recommended method for the primary prevention of concussion was education (n=10)31 35 39 42–46 48 51 52 ‘education of athletes, colleagues and the public is the mainstay of progress in (the field of concussive injury)’.51 Additional primary prevention methods include rule changes and adherence to rules during games. There is consensus among guidelines that equipment such as helmets are not universally protective against concussion (n=6).35 44–46 48 51 52
Two physical education specific guidelines26 44 recommended that schools develop a concussion policy or incorporate concussion policy into existing head injury policies. Two guidelines recommend surveillance of sports injuries among children.45 48
Discussion
Main findings of this study
This review identified 26 school sports injury prevention guidelines that met our inclusion criteria. A range of primary, secondary and tertiary injury prevention activities and interventions were identified, and the degree to which identified activities were supported by other existing evidence varied.
First, few guidelines referenced original scientific research to support their recommendations. Concussion-specific guidelines are however better supported by evidence than other guidelines. Nevertheless, many included guidelines make assumptions for children based on evidence generated from adults. Therefore, the overall quality of evidence used to generate guidelines was considered to be poor. For example, with regards to concussion, the biochemistry of a developing brain is different from an adult brain, and children are more susceptible to physical trauma.53 Although there are likely to be similarities in effective injury prevention across age groups, additional research specifically for children is required in order to establish the efficacy of interventions with children and whether alternative interventions may be required.
Preparticipation examinations and introducing defibrillators at schools were suggested in guidelines from the US guidelines. UK guidelines did not advise preparticipation examinations, in line with UK Screening Committee recommendations.54 UK guidelines also did not advise defibrillators in schools; recent guidance from the Department of Education (UK), however, encourages schools to purchase automated external defibrillator (AEDs).55 Currently, the specific benefit of AEDs in school settings is unclear and needs further research to establish for whom, and in what circumstances, the presence of AEDs in school settings are an effective intervention.
Primary prevention measures were commonly reported including rule changes for specific sports, the use of protective equipment and education of involved stakeholders. Education, involving families and school staff, is the most commonly mentioned primary prevention intervention. The evidence reviewed in this study supports the use of education as a prevention measure for sports injury. Nevertheless in the UK, clear guidance on who is responsible for providing such education, and to whom it should be offered, needs to be developed. Guidelines would be strengthened by referencing of research evidence underpinning prevention recommendations. Further comprehensive evaluation of the most effective education content and strategies is also necessary.
There is evidence that rule changes, such as mandatory use of protective equipment or rules limiting dangerous play, are an effective method of primary prevention; Vriend et al identified that over 75% of rule change studies reported a significant effect on injuries.56 57 Yet, this is only mentioned in a few of the included guidelines in this review. Vriend et al 56 identified a paucity of research on rule-change interventions (14 studies) compared with other sports injury prevention interventions, which is likely to have contributed to infrequency of reporting the potential value of rule changes within school guidelines. Therefore, the effectiveness of rule change would be an area for further focus in developing future guidelines for preventing injury in school sport.
Helmets are an example of protective equipment, which is recommended in some included guidelines. The effectiveness of helmets for prevention sports injuries including concussion remains unclear, and even if helmets are effective protection in one sport, this evidence may not be applicable to other sports. Much of the evidence on helmet use is generalised from adult professional American football. In addition, the positive effects of protective equipment may be outweighed by concurrent riskier behaviour patterns. Further research is needed to evaluate the degree to which ‘risk compensation’ (ie, risky behaviour among children and adolescents once wearing helmets) influences their likelihood of concussion.51 Evidence generated with children within the UK context is required to ensure findings can be generalised to across school sports policies.
Secondary and tertiary measures to prevent and mitigate consequences of injuries are discussed throughout the studied guidelines. Effective first response to injury is likely to minimise the short-term and longer term consequences of injuries for players. First aid training is commonly mentioned in guidelines, but there was insufficient detail to compare recommendations across guidelines, and recommendations were poorly referenced with research evidence. Sideline concussion assessment tools are often recommended for triaging concussive injuries. Guidelines lack consensus on which tools are appropriate for assessing children (as opposed to adults), or on which tools are suitable for use by non-clinicians. Therefore, guidelines for schools should include guidance on the use of suitable concussion assessment tools.58
There were three guidelines specifically focusing on tertiary prevention such as return to learn and return to activity plans following concussion.41–43 We did not identify guidance for returning to activity after other common sports injuries such as sprains or fractures. The New Zealand government health and safety policy49 reviewed in this study provides broad guidelines for schools and could provide a model for other governments. The policy includes guidance on managing the risk of sport provided by multiple providers, checklists for event organisation and guidance for the head-teacher specifically relating to national law. Principles for safe return to sport after any injury type could be included in such a policy. There was no mention of monitoring the efficacy of the policy, a component that should be inherent to all such policies so that effective injury prevention strategies can be identified.
Clearly defining roles and responsibilities is a key component of effective policy making59 60 yet was lacking in the reviewed guidelines. Not defining these roles in injury prevention risks a lack of accountability for safety initiatives. The lack of accountability in the UK has been acknowledged, and the government is currently drafting ‘duty of care’ guidance for sport. The content and how this guidance may be applied to schools remains to be seen.
Only two guidelines45 48 included a recommendation for injury surveillance. Currently, there is no national data collection of child injuries in the UK. Developing any effective injury prevention strategy requires an understanding of the burden of sports injuries. In turn, this would permit monitoring the effectiveness of interventions or guidelines that have been introduced to reduce injuries. Such a surveillance system should include documentation on the type of injury obtained and the type of sport that caused the injury, as recommended by the WHO.61 Effective sports injury prevention in the UK will remain challenging in the absence of effective monitoring systems. We wait with interest to determine the degree to which the Emergency Care Data Set, due for introduction in October 2017, can provide the required level of detail,62 although recognise that this system will only capture injuries presenting to emergency departments.
Finally, none of the included documents acknowledged that there is differential risk between girls and boys for some injuries. New work investigating anterior cruciate ligament injuries is one example for the importance of this63 and needs to be considered in further research into sports injury prevention and subsequently incorporated into policies and guidelines for schools.
In conclusion, high-quality guidance for schools on this topic is sparse, and we have specified key areas that merit further research and attention. Importantly, interventions such as rule changes, introduced within the last few years in professional and youth games, have not yet been considered in school sport guidelines. The findings of the review have implications for policy, practice and research. A national policy is required specifically for schools, building on recent attention to concussion as a public health problem. Any new policy or guideline must incorporate existing and emerging research on sports injury prevention. In practice, existing guidelines reviewed in this study need to be publicised and adopted by schools. Finally, further research is required to develop an understanding of the effectiveness of child-specific injury prevention interventions. When assessing effective sport injury prevention interventions for children, the age, stage of development and gender of the child must be taken into account.
Limitations
Despite efforts to develop a comprehensive electronic database and grey literature search strategy, we are aware that further guidelines meeting our inclusion criteria may exist. Polices, guidelines and consensus statements are infrequently indexed in electronic databases making identification challenging. We limited our search to the English language and to OECD countries to identify guidelines with the potential to be relevant in the UK. The heterogeneity of guidelines and policies meant synthesis was limited to narrative process.
Acknowledgments
The authors would like to thank Caroline Finch, Keith Stokes, Mike England, Ginny Brunton, Angela James and all the authors of guidelines who assisted with data gathering for the project. This study was conducted by AG as part of a Severn Deanery Foundation Programme Year 2 placement under the supervision of JM and AE and supported by MVH.
References
Footnotes
AGöp and MVH are joint first authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Not required.
Contributors This study was conducted by AG as part of a Severn Deanery Academic Foundation Programme Year 2 research placement under the supervision of JM and AE and supported by MvH.
Data sharing statement There are no unpublished data.