Article Text

Abstract
Objectives Massage therapy (MT) enhances recovery by reducing pain and fatigue in able-bodied endurance athletes. In athletes with disabilities, no studies have examined similar MT outcomes, yet participation in sport has increased by >1000 athletes from 1996 to 2016 Olympic games. We examined the effect of MT on pain, sleep, stress, function and performance goals on the bike, as well as quality of life off the bike, in elite paracycling athletes.
Methods This is a quasi-experimental, convergent, parallel, mixed-methods design study of one team, with nine paracycling participants, in years 2015 and 2016. One-hour MT sessions were scheduled one time per week for 4 weeks, and then every other week for the duration of the time the athlete was on the team and/or in the study. Closed and open-ended survey questions investigating athlete goals, stress, sleep, pain and muscle tightness were gathered pre and post each MT session, and every 6 months for health-related quality of life. Quantitative analysis timepoints include baseline, 4–6 months of intervention and final visit. Additional qualitative data were derived from therapists’ treatment notes, exit surveys, and follow-up emails from the athletes and therapists.
Results Significant improvement was found for sleep and muscle tightness; quantitative results were reinforced by athlete comments indicating MT assisted in their recovery while in training. There were no improvements in dimensions measuring quality of life; qualitative comments from athletes suggest reasons for lack of improvement.
Conclusion This real-world study provides new information to support MT for recovery in elite paracyclists.
- massage therapy
- disability
- athletes
- muscle tonus
- sleep
- quality of life
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Massage therapy aids able-bodied athlete recovery. Until now, no studies have investigated the effects of massage therapy in a para-athlete population.
Massage therapy, however, showed no improvement in health-related quality of life for a small sample of elite paracyclists.
Our study showed that massage therapy assisted in para-athletes’ recovery, particularly in the area of reducing muscle tightness and in improving sleep.
Background
In the past 20 years, the number of disabled athletes competing at elite levels has increased, as is witnessed in the number of participants at the 1996 Summer Paralympics in Atlanta (n=3255) compared with the number of participants in 2016 in Rio (n=4328).1 The Paralympics is not the only venue for disabled athletes, as positive health and social benefits have been noted for those who participate in both professional and recreational adaptive sports.2–5 Yet studies demonstrate that para-athletes also have higher incidence and prevalence of injures compared with able-bodied athletes.6–9
The increasing number of disabled athletes, as well as increased risk of injuries, gives credence for investigation into ways to support disabled athletes during their training and sport competition. Massage therapy (MT) has been shown to improve recovery by reducing pain and fatigue in endurance able-bodied athletes.10 11 Additionally, a recent analysis of treatments pursued by athletes at the Pan American games indicates that MT was the most sought treatment, and more than half of MTs were performed by massage therapists.12 Reports suggest MT availability for para-athletes6 13 14; however, to our knowledge, outcomes of MT treatment have not been tracked for athletes with disabilities. While no identifiable evidence exists to support MT for disabled athletes, there is evidence for MT benefiting those with health conditions seen in para-athletes, such as spinal cord injury,15–17 cerebral palsy18 19 and amputation.20 21
Best and Crawford,22 as well as Poppendieck et al,23 suggest the need to investigate multiple bouts of massage during an athletic season for athletes to advance the science of massage and sport recovery.22–26 The purpose of this paper is to examine the effect of MT on pain, sleep, stress, function and performance goals on the bike, as well as the quality of life off the bike, in elite paracycling athletes in training from January 2015 until the Rio Olympics in 2016.
Methods
Participants
All members of Greenville Health System Team Roger C Peace (Greenville, South Carolina, USA), an elite paracycling team, were invited to join the study in 2015 and 2016. In 2015, a total of 9 of the team’s 11 athletes began the programme; two athletes left the team in 2015 and two athletes dropped from the study prior to completing the intervention. At the beginning of 2016, four new athletes joined the team and began the study protocol. While a total of 13 athletes completed the study visits; the data from only of nine athletes were used for this analysis after reviewing study visit timeline due to lack of consistent survey completion by the athletes and massage therapists. All participants signed a written informed consent.
Study design and intervention description
A quasi-experimental, convergent, parallel, mixed-methods design was used.27 Both qualitative and quantitative data were gathered in one phase of the research, analysed separately and then merged to find where the results converged. Merging the quantitative/qualitative data strengthened the overall outcome by providing more comprehensive results.27
In 2014, a standardised MT programme was designed with the intention to help a decentralised team of elite paracyclists to improve recovery, rest, performance and quality of life both on and off the bike. The decentralised nature of the paracycling team allowed for athletes to be on the same team and also to live across the country. Development of the programme is described elsewhere28 and included input from relevant stakeholders including athletes, coaches and massage therapists. In brief, the intervention allows for five different protocols (1, general relaxation; 2, muscle relaxation; 3, combination of general and muscle relaxation; 4, injury rehabilitation; and 5, integrated injury rehabilitation and general and/or muscular relaxation) to be integrated into clinical MT treatment based on an intake assessment survey, which also specified the athlete’s specific goals for the session.28 This type of flexible and adaptive protocol allows for individualised treatment of athletes based on their treatment goals and allows for the programme implementers (ie, massage therapists) to work within their strengths and skillsets.29–31 Massage therapists used to implement the programme were identified either by the athlete, through a search through a locator service, or through local and national contacts. For massage therapists to be qualified as implementers, they had to practise sports MT, be willing to be trained in and follow study protocols, and be willing to work with their assigned athlete. A total of 17 massage therapists were recruited and trained as implementers via online live webinar; more therapists were recruited than athletes, as some athletes worked with multiple massage therapists. Of the 17 massage therapists, 11 (64.71%) were female and all therapists had an average of 14 years (SD 8.59) in practice. Ten of the 17 therapists (58.8%) held a bachelor’s degree or higher; 58.8% had more than 600 hours of initial MT education. All massage therapists were paid their standard fees for their services and provided MT treatment in either their offices or in the athlete’s home.
On entering the study and signing informed consent, athletes were asked to schedule a 1-hour MT sessions one time per week for 4 weeks (eg, loading phase) and then every other week for the duration of the time (eg, maintenance phase) they were on the team and/or in the study. This schedule was chosen to try to minimise time burden on the athletes, as well as mirror ‘real-world’ clinical implementation. The maximum amount of MT sessions an athlete could obtain if they remained on the team and in the study over the 18-month period was 39 MT sessions.
Outcome measures
Quantitative data were gathered from the RAND Medical Outcomes Survey MOS Short Form Health Survey 36 (SF-36),32 33 or SF-36V34 (for non-ambulatory athletes), and on an MT session intake and exit questionnaires to measure stress, sleep, muscle tightness, spasticity and pain on a 10-point scale, with higher numbers indicating greater impairment.28 Qualitative data were obtained from open-ended questions on the massage intake and exit questionnaires, from the massage therapists’ treatment notes, from the programme exit questionnaire, as well as programme feedback emails provided by the athletes.
Data collection
On entering the programme, the athletes completed a health history form as well as either the SF-36 V.2 or SF-36V. The athletes subsequently filled out the SF-36 (or SF-36V) after the 14th MT session (approximately 6 months into the programme) and at the end of the programme. The MT session intake surveys were emailed to each athlete on the morning of their scheduled MT session; once the survey was completed, an email notification was sent to their massage therapist. Massage therapists also received an email link to their treatment notes on the morning of the scheduled session with their athlete. The morning after the MT session, athletes received the session exit survey to follow up on progress after treatment. All surveys were managed through the REDCap system, a secure and Health Insurance Portability and Accountability Act (HIPAA)-compliant system for survey and database development.35
Data analysis
Quantitative analysis (SAS Enterprise Guide Software, V.7.1) included comparing the nine dimensions of SF-36 questionnaire and the 10-point scales for pain, sleep, function, spasticity and stress before, during and after the intervention. Repeated-measures analysis of variance (ANOVA) was used to analyse the differences in comparison variables at three timepoints: baseline, at 4–6 months and at final visit. Further, multiple pairwise comparison was performed using Tukey’s test whenever a significant difference was revealed by repeated-measures ANOVA. The difference between intake and exit outcome variables was analysed at each timepoint separately using paired t-test. P values less than 0.1 are considered significant for this feasibility study.
Qualitative analysis (NVivo V.11 qualitative data analysis software; QSR International, Doncaster, Victoria, Australia) began with data immersion by reading and rereading the text provided by the athletes and therapists. Next, word count queries were performed for each qualitative survey question, athlete feedback emails and the therapists’ notes to begin to understand potential patterns in the data.36 Then initial codes were created from the textual data through an iterative thematic analysis process of reading the data and highlighting text and assigning a code identifier.37 Once all the data were coded, emergent themes were identified by gathering similar codes together.37 The coding scheme evolved to have four major themes: goals for MT sessions, perceived benefits of MT sessions, beliefs and expectations about MT, and the interaction and importance of the therapeutic relationship with their massage therapist. These themes are mentioned here, in the Methods, as they then guided the integration of the quantitative and qualitative data. The quantitative results tables were integrated with athlete and therapist comments from the representative themes. These qualitative quotations were used to explore and expand the understanding and of the quantitative findings.38 39
Results
Participants
Seven male and two female athletes of the Roger C Peace paracycling team (analysis n=9) with an average age of 39.14 (SD 9.23) years and an average time since injury/impairment of 19.09 years (SD 12.02) provided sufficient data for analysis. Figure 1 indicates the states where the athletes lived; it should be noted that one athlete split his time living in two separate states (Ohio and Florida) and received the intervention in both locations.

State residence of athletes.
The athletes presented with varying impairments that limited activity: three with spinal cord injuries, two with amputations, one with stroke, one with traumatic brain injury, one with a lower limb crush injury leading to neuromuscular impairment, and one with cerebral palsy. In the sport of paracycling, an athlete’s level of impairment is evaluated and graded to allow athletes of similar abilities to compete against each other. Of the grades (1–5), a lower grade represents a greater physical impairment and limitation for activity; an athlete with a grade of 2 has a greater impairment and a higher level of disability than an athlete with a grade of 5.40 Additionally, there are four types of sport class categories in which athletes can compete: handcycle, tricycle, tandem and upright bicycle.40 The categories in which the athletes compete include three handcyclists (two H3, one H4), one tricycle (T1), and five cyclists (three C5, one C4, one C2).
Athlete perceptions of quality of life
Athletes’ quality of life was quantitatively assessed with the SF-36 and confirmed with qualitative data (figure 2). The dimensions within the SF-36 are created by averaging items together, each scale totalling up to 100, with higher scores indicating higher quality of life. Athletes’ comments (figure 2) point to other indicators for lack of improvement, including the level of disability of the athletes, less than desired frequency of MT, amount of intense training and continued health issues for many of the athletes.
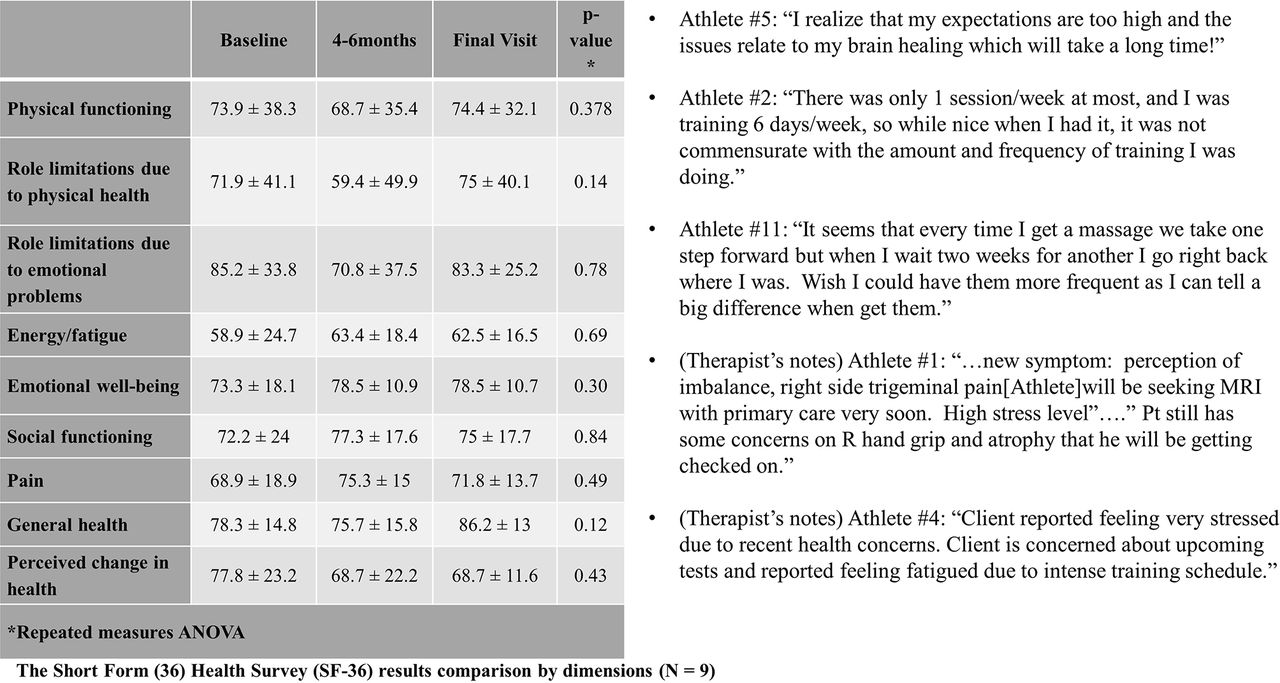
Athletes’ perceptions of quality of life. Integration of quantitative and qualitative data. Results of SF-36 and quotes from athletes from quality of life and massage expectations themes. ANOVA, analysis of variance.
Athlete goals point to benefits and outcomes
The athletes indicated that reducing muscular tension was their most often sought goal for treatment, while pain reduction was mentioned less often on the session intake form (figure 3). However, within the therapist’s notes, pain reduction was mentioned as an athlete’s session goal (figure 3).
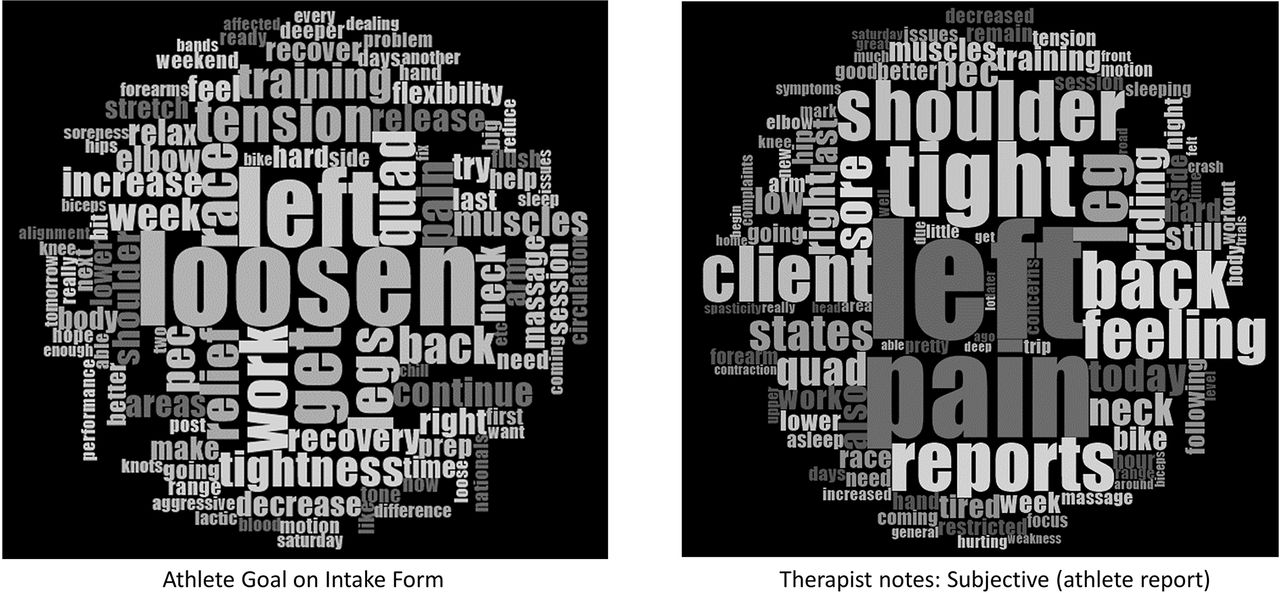
Word frequencies displayed in a word cloud exploring the athlete’s goals for sessions from the athlete reported goal on the intake form and from the athlete report (verbal) to therapist as indicated by the therapist in their notes.
In figures 4 and 5, it should be noted that pain is not included in the outcome variable comparison, as the athletes did not sufficiently answer both intake and exit questions for this variable. Figure 4 looks at each variable longitudinally by pre-MT or post-MT. Figure 5 examines the variables pre-MT and post-MT to each other and longitudinally. The athletes report several benefits of treatment, with the most often reported benefit of assisting in recovery from training and racing including relief from symptoms and helping with sleep. These benefits from recovery led to improved training and racing performance.

Athletes’ goals point to perceived benefits and outcomes. Integration of quantitative and qualitative data. Outcome variables comparison from intake (pre-MT) and exit forms (post-MT) and quotes from athletes and from therapist notes. ANOVA, analysis of variance; MT, massage therapy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Athletes’ perceived benefits and outcomes. Integration of quantitative and qualitative data. Comparison at each timepoint from intake exit (pre-MT and post-MT) forms and quotes from athletes and from therapist notes. MT, massage therapy.
Programme implementation
Programme implementation data and programme exit survey data indicated that the recommended protocol of one massage per week for 4 weeks and then every other week for the length of the study appeared to be difficult to follow. Athlete travel, life events, transportation issues and busy athlete schedules were indicated as barriers to maintaining the protocol. Additionally, while surveys were delivered electronically to both athletes and therapists, and therapists were expected to check the completion of the surveys prior to initiation of therapy session, survey completion for all sessions (intake, exit and therapist’s notes) was not consistently completed by all athletes or massage therapists.
Discussion
In this quasi-experimental, mixed-methods design study, elite paracycling athletes reported an improvement in muscular tension and sleep after MT treatment. This study found three noteworthy results: (1) Athletes’ expectations and programme implementation may have impacted the expected improvement in athletes’ quality of life. (2) Verbal intakes may be important when compared with written intake forms to help elucidate goals and improve treatment. (3) The athletes’ perceptions of the benefits of MT, mainly assisting in recovery, support the quantitative improvement in reduced muscle tightness and sleep.
MT improves the quality of life in many populations.41–45 Yet MT did not significantly improve quality of life as measured by the SF-36 instruments for the paracyclists. This could be because some of the expectations of treatment did not lead to the desired outcomes (as noted by the athletes’ comments from the qualitative data) or it could result from the inconsistent programme implementation.
The scarcity of reporting pain reduction as a goal of treatment in written form by the athletes versus the greater indication of pain reduction as a goal as indicated in the therapists’ notes may indicate the importance of communication between the therapist and the patient. Communication within an MT practice has not yet been investigated, but it has been mentioned as a critical component of care within the MT setting.46 47 Other healthcare literature indicates improved outcomes for patients with good healthcare provider communication48–51 and findings could be similar for MT treatment.
Additionally, while MT did not significantly improve pain or stress, another hypothesis could be an actual focus of the athletes to shift more from relieving pain to improving function, as is indicated by their most indicated goals of reducing muscle tightness/tension. This shift, from pain management to functional improvement, is mentioned as a new suggestion in the management of subacute and chronic pain in elite athletes by the International Olympic Committee (IOC); the IOC also suggests that treatment should take a multidisciplinary approach.52 In the IOC report, the committee does take special note of Paralympic athletes indicating they may have more pain than able-bodied athletes and therefore may have higher usage of pain medications, yet there is not mention of the multidisciplinary approach for these athletes.52 This lack of mention of additional approaches could be due to the current lack of evidence for MT benefiting Paralympic athletes.
Our study extends previous studies in various non-athlete and athlete populations (including those with breast cancer, pregnant women, older individuals, patients with fibromyalgia, osteoarthritis, athletes and healthy individuals) indicating MT can aid in improving sleep44 53 54 and muscle tightness.45 55–57 Ours is the first study to investigate these outcomes in a para-athlete population. Integrating the qualitative results indicates that athletes felt that MT helped with recovery and training. The athletes clearly indicated in the qualitative data that they felt MT helped them to train harder, rest better and possibly perform better. These results mirror previous studies showing MT assisting in recovery from exercise in able-bodied individuals.11 58–60
Limitations and future directions
Results should be viewed with caution as the limitations include a small sample size with no comparison group. Furthermore, the measures used to evaluate change in the population are largely subjective, and the athletes and therapists did not consistently supply data via forms or consistently follow the recommended protocol. However, this study was implemented in real-world settings, and lack of consistent survey completion still led to positive outcomes.
Additionally, this is the first known study to follow decentralised athletes for this length of time, as most massage studies are short in duration (one to six sessions generally). This study shows continued improvements in muscle tightness and sleep over time. Further research is needed to explore the impact of MT on pain in this population, as well as investigate the effect of MT on para-athletes in other adaptive sports.
Conclusion
Previous work reported MT as a common technique for athletes to use to reduce recovery time,11 25 26 although to date no literature has explored the effects of MT in a para-athlete population. This real-world implemented study provides new information to support MT for recovery in elite paracyclists.
Acknowledgments
The authors would like to thank and acknowledge the massage therapists who implemented the study throughout the country. Their work and willingness to engage in the training and research process made this project possible. We would also like to thank the athletes of Team Roger C Peace, the team manager Jerry Page and the Director Sportif Jim Cunningham for their tireless efforts to train harder, recover quicker and find the best ways to support each other in the sport of paracycling as well as in life.
References
Footnotes
Contributors ABK designed the intervention, analysed the qualitative data and prepared the manuscript. NP analysed the quantitative data and helped to prepare the manuscript. JLT helped to design the intervention and helped to prepare the manuscript.
Funding This project was funded by the generous sponsorship of Team Roger C Peace by the American Massage Therapy Association.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the Institutional Review Board at the Greenville Health System Office of Research Compliance and Administration (Pro00036860).
Provenance and peer review Not commissioned; externally peer reviewed.