Article Text

Abstract
Objectives While the health benefits of running are legitimately advocated, participation in running can also lead to health problems. There is a high range of reported prevalence rates especially of running-related overuse injuries in high-level athletes and during competition. Little consensus exists for acute injuries and illnesses especially in recreational runners. Therefore, the aim of this study was to record the prevalence of health problems in recreational long-distance runners preparing for an event.
Methods Recreational runners aged 18–65 years who were registered 13 weeks prior to a half-marathon running event were invited to take part in this study. Participants were prospectively monitored weekly over 13 weeks by applying a standardised surveillance system for injuries and illnesses (Oslo Sports Trauma Research Center questionnaire). From this, prevalence and severity of acute and overuse injuries, as well as illnesses, were calculated.
Results We received 3213 fully answered questionnaires from 327 participants (40.7% female, 40.9±11.7 years of age, 31.5±21.1 km weekly mileage, 8.3±7.8 years of running experience). At any point in time over the preparation phase, 37.3% of the participants had health problems. Overuse injuries were the major burden (18%). They were followed by illnesses (14.1%) and acute injuries (7.9%). The median weekly severity score was 56.5 (IQR 37.0–58.0).
Conclusion The high prevalence of health problems in our cohort suggests that future efforts are needed to further specify the underlying mechanism and develop adequate prevention strategies for recreational runners.
- injuries
- injury
- overuse
- epidemiology
- running
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What are the new findings?
This study prospectively monitored injuries and illnesses occurring during the 12-week preparation to a road race using the Oslo Sports Trauma Research Center questionnaire.
While having a good response rate (>75%), the overall prevalence of health problems was 37.3%.
Overuse injuries (18%) were the major problem, followed by illnesses (14.1%) and acute injuries (7.9%).
How might it impact on clinical practice in the near future?
Prospective injury surveillance in recreational runners can be a promising approach to better understand running injury epidemiology.
New technologies (like smartphones) could be used to implement injury surveillance into training documentation.
Risk factors have to be detected and preventive strategies should be implemented to reduce health problems in recreational runners.
Introduction
Participation in running at both competitive and recreational levels has increased over the last decades.1 2 The health benefits associated with running are well-documented.3 However, participation in running, like all sports, is associated with a certain level of risk, particularly the risk of sustaining injuries and illnesses.4 5 The prevalence of running-related injuries is high, with epidemiological studies reporting prevalence rates between 19% and 92% in middle-distance and long-distance runners.6–9 This large range may be due to different study designs (retrospective vs prospective) and due to heterogeneous populations (elite vs recreational) being studied. Some epidemiological studies report that up to 55% of runners can be expected to sustain at least one injury over a 12-month period.8 Lower limb injuries, such as medial tibial stress syndrome, Achilles tendinopathy and plantar fasciitis, are the most frequent injuries sustained by runners.7 9 10
The ability to contextualise the results of epidemiological studies in sports medicine is dependent on a number of factors, including injury definitions, the mechanism of injury surveillance and the methods used to calculate athlete exposure to sport.11–13 Injuries can be defined as any problem an athlete sustained during execution irrespective of receiving medical attention or time loss.14 Furthermore, Fuller et al 14 classified injuries according to location, type, body side and mechanism (acute or overuse, depending on the presence of an identifiable event). The Oslo Sports Trauma Research Center (OSTRC) questionnaire is an injury surveillance system that has been evaluated in Olympic and Paralympic athletes preparing for the London Olympic Games in 2012.15 It is a prospective continuous standardised injury surveillance system that records acute and overuse injuries, as well as illnesses. It can be used with athletes competing in different sports and at different levels of competition, as well as across jurisdictions.16–19
A number of studies have evaluated illnesses in high performance athletes.12 20 In contrast, few studies have investigated illnesses experienced by recreational running athletes, specifically during the preparation phase for an event.21 22 Risk factors for running-related injuries are widely debated,23 and good evidence exists that a sudden increase in weekly running mileage is a primary risk factor.9 During the preparation phase for running events such as the half marathon, a weekly increase in running mileage is a constituent component of physiological conditioning.24 The aim of this study was to monitor prospectively the prevalence and severity of injuries and illnesses in recreational long-distance runners preparing for a half-marathon road race.
Methods
Study design and participants
We conducted a prospective cohort study among recreational runners preparing for the Hamburg Half Marathon. The Hamburg Half Marathon is an annual road race over 21.1 km for runners at every level. In 2017, 11 117 runners registered, of whom 8730 finished the race. In 2015, the race record was set at 1:00:52 hours by Merhawi Kesete.
For inclusion, participants had to be registered runners and between 18 and 65 years of age. There were no further exclusion criteria such as preinjuries, current health problems or specific fitness levels. Thirteen weeks prior to the race, 5395 runners who had signed up at the date of recruitment received an email with an invitation to participate in this study. Participants interested in the study could sign an informed consent form electronically and were then contacted by the study staff via mail.
Data collection
Before the start of the study, an online baseline questionnaire was sent asking participants about their running experience, training history, personal bests, as well as illnesses and injuries in the past 3 months. During the course of this study, every Sunday a secure link to an online OSTRC questionnaire was sent to each of the participants by email. To enhance compliance, all participants were entered into a draw, whereby the prizes included a running performance evaluation, running equipment and entry places for next year’s event. The online questionnaire was developed electronically in LimeSurvey (V.2.62.2+170 203, LimeSurvey, Hamburg, Germany). During the preparation period the questionnaire was sent each week on an anonymous basis.
To register running-related injuries and illnesses, the German version of the OSTRC Questionnaire on Health Problems Oslo was used.15 17 Participants reported on questions across four specific domains as follows: (1) health problems, injuries or illnesses interfering or inhibiting training during the last week; (2) the extent to which injury, illness or other health problems affected their training volume in the last week; (3) the extent to which injury, illness or other health problems affected their running performance in the last week; and (4) the extent to which symptoms or health problems were experienced during the last week.
If no problems were marked in these four specific domains, the questionnaire was finished. In case of a problem in at least one of these four main questions, the questionnaire asked to specify the problem as well as the severity (time loss in number of missed training sessions). Disorders of the musculoskeletal system were categorised as injuries, whereas illnesses were classified as disorders that involved other body systems, such as (but not limited to) the respiratory, digestive and neurological systems, as well as non-specific/generalised, psychological and social problems.15 As per the recommendations of Fuller et al,14 injuries were classified as acute or overuse. All health problems were self-reported.
Data analysis
Data were analysed following the original outline of Clarsen et al 15 and further research that has applied the OSTRC questionnaire.17 21
Prevalence
Prevalence is the number of cases (individuals) who reported health complaints (illness, overuse or acute injury) in a defined population at a certain point in time (equation 1).25
 (1)
(1)
Every week, the number of respondents differed. Thus, the prevalence was calculated for each week by dividing the number of individuals who reported any kind of health problems (illness, acute or overuse injury) over the number of respondents who answered the questionnaire completely for that certain week. The mean prevalence of illnesses, overuse injuries and acute injuries was calculated.
Severity
The severity was recorded to measure consequences and progress of the reported health problems. The severity score was calculated for all reported health problem as per Clarsen et al.13 The score ranges from 0 to 100 and is the sum of the answers to the first four main questions. Each question score varies from 0 to 25, where 0 represents no problems and 25 the maximum stage.13
The mean severity score gives an estimation of the impact that health problems had at any point in time over the 13 weeks. It is measured by taking the mean of the weekly severity score.26 The results were stated as mean and 95% CI, as well as median and IQR of 25%–75%.
Results
Response rate and participants
A total of 327 participants agreed to take part in the study, of whom 287 (87.8%) gave information about age, sex, height, weight, personal bests, weekly mileage and running experience (table 1). Over the course of 13 weeks, 4240 requests to complete the questionnaire were sent to all included participants (n=327) and 3213 were fully answered. One person withdrew after the second week because participation in the half marathon was cancelled, so that the average weekly number of questionnaires sent out was 326. The average weekly response rate to the OSTRC questionnaire over 13 weeks was 75.8% (95% CI 71.5% to 80.0%), which equals an average number of 247 respondents. The flow of participants and weekly response rates can be found in figure 1.
Participants’ baseline characteristics shown as mean±SD

Flow of the participants and response rates through the course of the study.
Prevalence
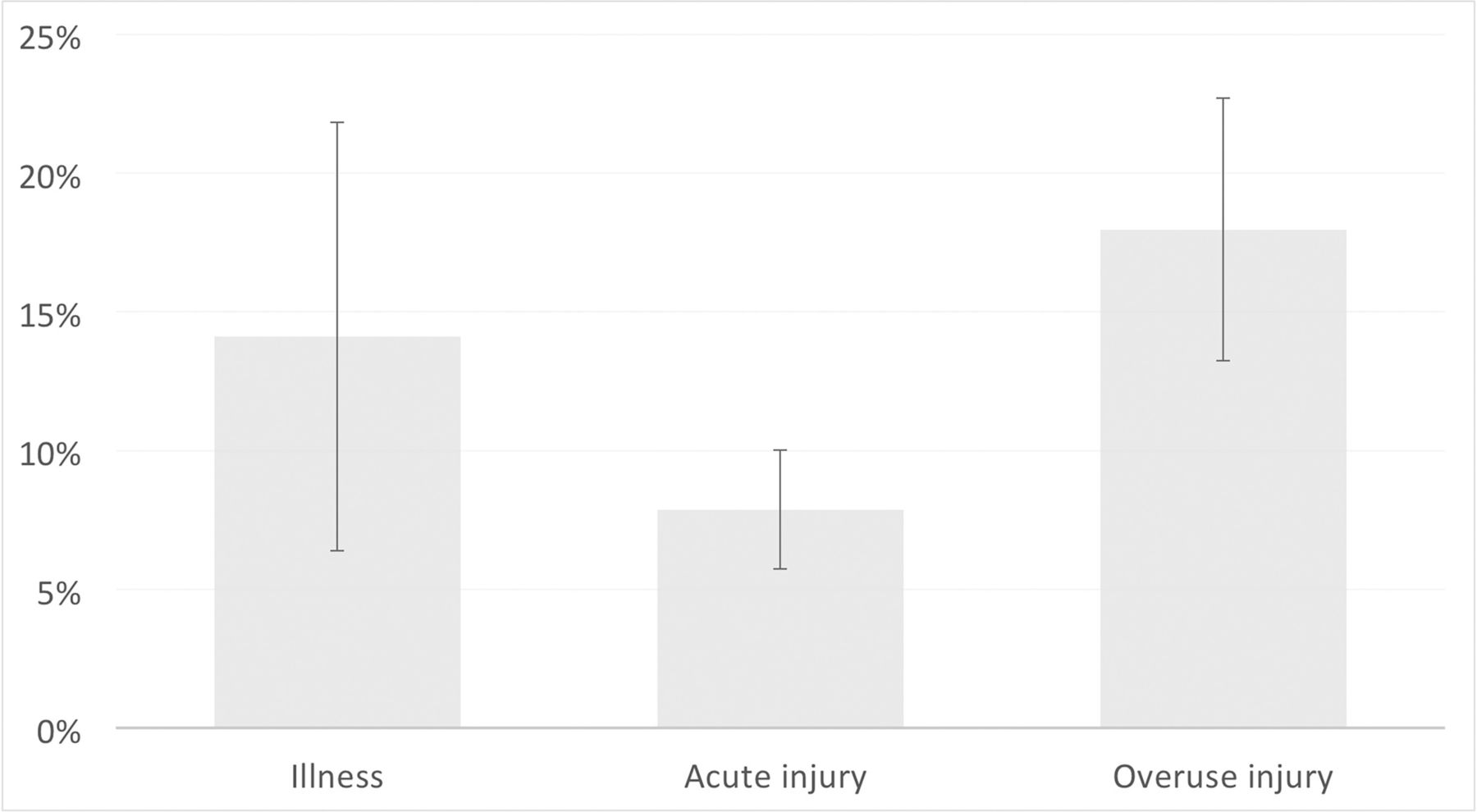
Over the course of 13 weeks, 37.3% (95% CI 31.9% to 42.8%) of participants reported health problems. As shown in figure 2, the mean prevalence of overuse injuries was 18.0% (95% CI 13.2% to 22.7%), followed by illnesses with 14.1% (95% CI 6.4% to 21.8%) and acute injuries with 7.9% (95% CI 5.7% to 10%). The progression of the prevalence for illness, overuse and acute injuries over the full preparation phase of 13 weeks is depicted in figure 3. An overview of the absolute numbers and prevalence is demonstrated in table 2. The most common health problem over all weeks was knee pain with a mean of 24.3% (n=206), followed by foot or toe pain with a mean of 15.6% (n=133) and lower leg pain with a mean of 12.4% (n=104). Thigh pain (9.2%, n=74), hip and groin pain (8.8%, n=74), as well as ankle pain (7.6%, n=66) were also frequent.

Mean and 95% CI prevalence for illness, acute and overuse injuries.
{kind=link}
{kind=link}
{kind=link}
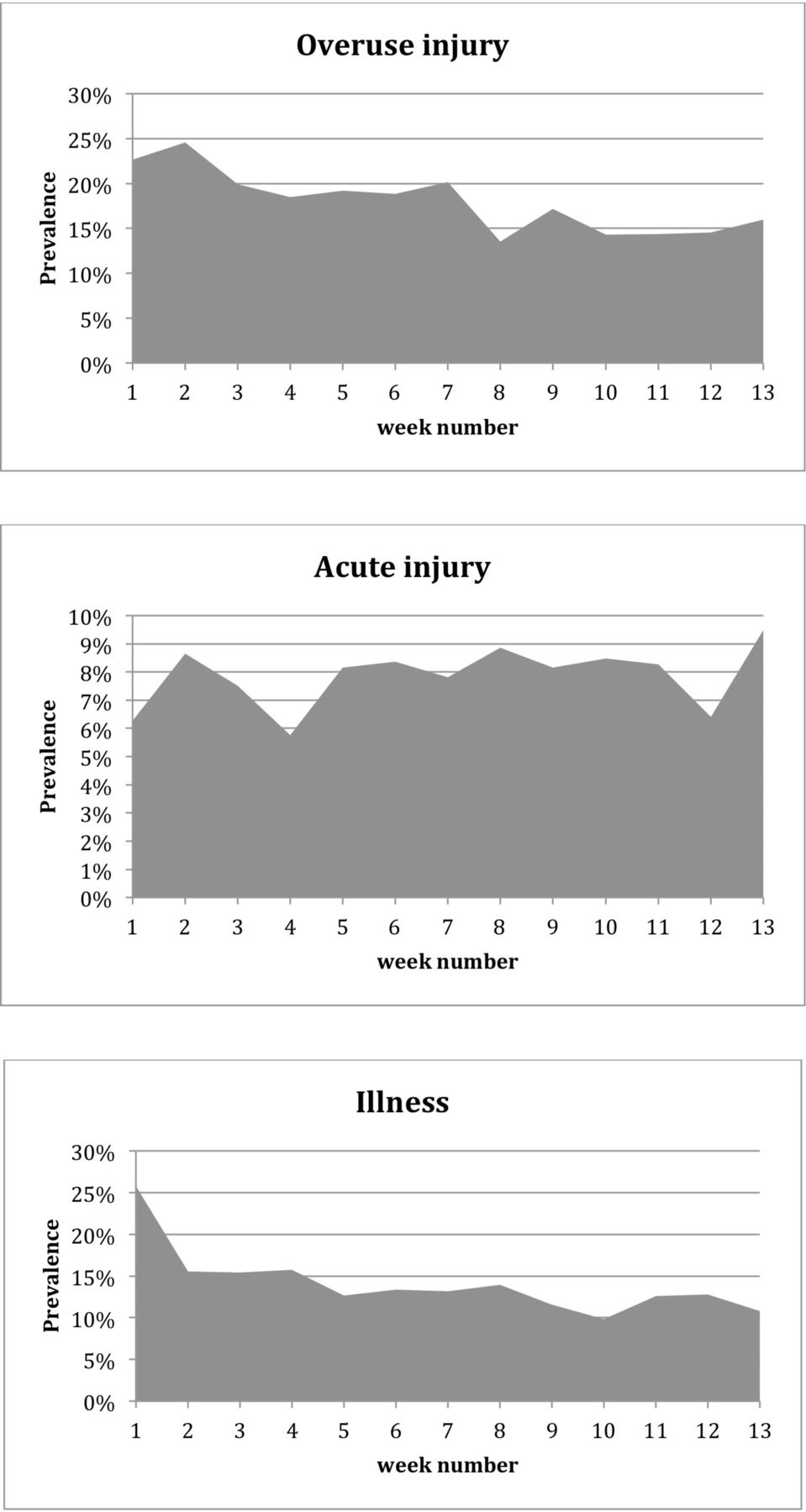
Course of the mean prevalence rates for illness, overuse and acute injuries over 13 weeks.
Overview over absolute numbers, mean prevalence rates and median weekly severity scores.
Severity score
The median total weekly severity score was 56.5 (IQR 37.0–58.0). For illnesses, the median severity score was 60.0 (IQR 58.0–60.0). Similarly, acute injury showed a median severity score of 57.5 (IQR 37.0–66.0), whereas for overuse injury a median severity of 30.0 (IQR 28.0–37.0) was recorded (table 2). Based on the mean, the total weekly severity score was 54.1 (95% CI 53.7 to 54.5). No differences were found between acute injuries that had a mean weekly severity score of 53.4 (95% CI 52.8 to 54.0), overuse injuries with a mean of 54.0 (95% CI 53.4 to 54.6) and illnesses with a mean of 54.9 (95% CI 54.5 to 55.3).
Discussion
This paper describes the prevalence of overuse injuries, acute injuries and illnesses, as well as the severity of health problems, during a 13-week preparation phase for a running event, as recorded by an online questionnaire. Of the participants, 37.3% experience an illness, an acute or overuse injury at any point in time during the 13 weeks.
The OSTRC questionnaire has already been used in several other sports. For example, in tactical and Paralympic sport disciplines, there were less health problems reported (21%–30%),15 17 27 while in team sports the prevalence of health problems has been reported higher (45%–61%).15 28 In endurance sports, there were similar prevalence rates reported for athletes preparing for a sport competition15 or in preparation for a running event.21 Clarsen et al 15 reported a mean prevalence of 30% of health problems in endurance athletes, and Hespanhol Junior et al 21 30.8% in runners. Hence, the mean overall prevalence of all health problems of 37.3% in our cohort was in between different sports and on the top of the range of the current literature on endurance sports. Possible reasons for this could lie in different levels of athletes and time frames of monitoring. While Clarsen et al 15 monitored athletes over the course of 40 weeks preparing for Olympic/Paralympic games, Hespanhol Junior et al 21 monitored recreational runners over 18 weeks preparing for a road race. Another explanation could lie in the selection of participants. Hespanhol Junior et al 21 recruited their participants from a running club that offered an organised training programme. We, on the other hand, recruited from a database of all registered participants to a half-marathon race. Therefore, selection bias could play a role in the interpretation of our higher prevalence.
In our study, overuse injuries represented the main burden (18.0%), followed by illnesses (14.1%) and acute injuries (7.9%). This is consistent with the literature where overuse injuries are the most common health problems in endurance sports.15 26 29 Studies that used the OSTRC questionnaire in other sports also found the highest prevalence for overuse injuries and the lowest for acute injuries.15 18 27 The study of Hespanhol Junior et al 21, which worked with recreational runners, found a prevalence of 28% for overuse injuries. Thus, the prevalence of 18% in this study was within the range of the literature. Nevertheless, it is a wide range that is reported in the current literature. This might be due to the different types of sports and levels that were studied or to differences in injury definition and time frames investigated. It should also be considered that in this study, the classification between overuse and acute injuries was completed by the participants and not reclassified by medical staff, as in several other studies.15 21 27 This difference in injury classification might also be a reason for the wide range of prevalence rates in overuse injuries that can be found in the literature. The prevalence of illnesses of 14.1% and acute injuries of 7.9% was also congruent with the literature.15 Clarsen et al 15 found a prevalence of 13% for illnesses and 4% for acute injuries for different sports.
Noteworthy, overuse injuries and illnesses declined over the 13-week period (figure 3). The same was mentioned in the study by Clarsen et al.15 They discussed the feedback of medical experts to the athletes regarding the observed medical conditions as a potential reason for the decline.15 In the present study no medical feedback was given to participants. One may speculate that the decrease might be due to a dropout of participants due to suffering from illnesses and overuse injuries. This suggestion is supported by a slight decrease in response rates (figures 1 and 2). Unfortunately the anonymous surveillance method over the 13 weeks did not allow the possibility to track back possible dropouts due to health problems. Further research is needed to prove this assumption.
In contrast to overuse injuries, acute injuries showed a slight increase over the 13-week preparation phase (figure 3). A similar increase in acute injuries was found in elite athletes.15 In this study, the large increase in the last week might be due to the fact that the questionnaire was answered on the race day after the half marathon when the participants might suffer from more acute health problems than during the preparation phase. Alternative explanation could be an increase of the training load during the course of the preparation. It has been argued that the competition itself should be regarded as a rapid increase in load and therefore could result in an increase in acute injuries during a competition period.23 30 This has especially been documented for running events.31
The severity of the health problems was measured using a severity score.13 For acute injuries, it was twice as high as for overuse injuries with respect to the median. Overuse injuries had a median severity score of 30.0 (IQR 28.0–37.0), whereas acute injuries reached a median severity score of 57.5 (IQR 37.0–66.0), which was similar to illnesses scoring 60 (IQR 58.0–60.0). However, no difference was seen, with respect to the mean severity score, between overuse injuries (54.0, 95% CI 53.4 to 54.6), acute injuries (53.4, 95% CI 52.8 to 54.0) and illnesses (54.9, 95% CI 54.5 to 55.3). The different findings between the median and the mean are consistent with the literature where acute injuries represented a higher median than overuse injuries and illnesses,21 whereas the mean severity score showed no significant differences between overuse and acute injuries.15 21 Nevertheless, the literature described a significant higher mean weekly severity score on illnesses.15 It can be concluded that the severity score for injuries was consistent with the literature. Acute injuries caused a higher severity score than overuse injuries and illnesses. Thus, acute injuries represented the most severe problems.
The average weekly response rate was 75.8% (95% CI 71.5% to 80.0%) in this study. This affirms the average weekly response rate of non-elite athletes in the literature.21 Literature about elite athletes reported higher response rates of between 80% and 91.5%.15 16 19 Hence, it can be suggested that the response rate was higher in elite athletes. This might be due to a higher interest of elite athletes to be free of health problems and capable to participate in sports at any point in time during the preparation and event period.
Strengths and limitations
To our knowledge, only few studies collected data on illnesses in addition to injuries during the preparation for a recreational competition. One strength of this study was, therefore, that the prevalence and severity of illnesses during a preparation phase for an event in running were monitored in addition to injuries. Another strength of this study was that health problems of mostly non-elite athletes were monitored during a preparation phase. Literature has mainly studied elite athletes while training for or performing at events.12 15 20 Lastly, most of the studies about sports injury prevalence were not sport-specific.13 15 18 19 This study focused solely on one sport so that it was possible to investigate the prevalence rates of health problems in running.
The study also had limitations. In this study answers to the weekly questionnaires were not linked to individuals. Direct access to the survey was chosen in favour of a higher response rate. Nevertheless, the response rate was similar to studies that individualised questionnaires.21 Hence, the mean weekly prevalence and mean weekly severity score could be analysed. Also the trend of mean prevalence rates of overuse injury, acute injury and illnesses over 13 weeks could be calculated. However, the responses to the questionnaires need to be individualised instead of being anonymous in order to analyse data for cumulative prevalence and cumulative severity score. This allows tracking of individual athletes’ health problems and severity thereof. Additionally, complete time loss of running sessions should be analysed on the basis of individualised responses. This enables the calculation of the impact that a certain injury or illness had on training participation. Otherwise, it cannot be distinguished between health problems that cause no time loss and problems that lead to a longer period of time loss. This is why calculating the mean time loss is not a very useful measure. Sending individualised keys to the participants could be a promising approach to this. Therefore, we could not link the individual data to half-marathon performance. Another limitation is that injuries and illnesses were self-reported and therefore not further classified in order to provide a diagnosis for each health complaint. This could be done by using the Orchard Sports Injury Classification System V.10,21 32 which requires contacting the athletes who report problems. Nevertheless, contacting participants was not possible in this study.
Perspectives
The results show to what a meaningful extent overuse injuries occured in recreational runners during preparation for an event. It is, therefore, important to include an appropriate monitoring of training load and to create awareness for overuse injuries in recreational runners. Medical care and preventive programmes should especially focus on the knee, lower leg and foot or toe pain. Possible mechanisms of injuries aside from participating in competitions and increasing weekly mileage could lie in altered biomechanics and foot morphology, as well as (habitual) footwear use.33–37 The risk of injury can be reduced by increasing the distance and duration of training gradually.38 A main point in reducing the prevalence of health problems is to monitor the athletes’ health by a standardised surveillance method. This study showed that this can be done effectively by using the OSTRC questionnaire.15 The wide range of prevalence of overall health problems and overuse injuries recommends the need for more research on homogeneous sample groups with regard to sport and performance level, so that the range can be reduced and be more sport-specific. Also, future studies should focus on the severity of illnesses, the specific classification of health problems and on time loss during the preparation phase for an event. In addition, more research is needed on the reason for the decline of overuse injuries and illnesses over the period of preparation for an event.
Conclusion
This paper monitored the prevalence of injuries and illnesses of recreational runners during the preparation period for a road race. At any point in time during the preparation period over 13 weeks, 37.3% of the participants reported health problems. Overuse injuries represented the main burden (18%), followed by illnesses (14.1%) and acute injuries (7.9%), which are the most severe problems. Further research is needed on homogeneous cohorts with regard to sport and performance level and on the reason for the decline of overuse injuries and illnesses over the preparation phase. Lastly, more research is needed on the severity of illnesses, the specific classification of health problems and on time loss during the preparation period for an event.
Acknowledgments
We would like to thank BMS Sportveranstaltungs GbR (Hamburg, Germany) for making it possible to conduct this study during their running event.
References
Footnotes
Contributors All authors participated in the conception and design of the study, and the drafting of the manuscript. AB and KH were responsible for data collection. All authors have contributed to, read and approved the final manuscript.
Funding This study was funded by the Ministry for Science and Research in Hamburg (grant number LFF-FV13).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The recruitment process and study were approved by the Ethics Committee of the University of Hamburg, Germany (ID 2017_94).
Provenance and peer review Not commissioned; externally peer reviewed.