Article Text

Abstract
Background/aim Exercise imparts a load on tendon tissue that leads to changes in tendon properties. Studies suggest that loading immediately reduces tendon thickness, with a loss of this response in symptomatic tendinopathy. No studies investigating the response of tendon dimensions to load for the rotator cuff tendons exist. This study aimed to examine the short-term effect of loading on the thickness of the supraspinatus tendon and acromiohumeral distance those with and without rotator cuff tendinopathy.
Methods Participants were 20 painfree controls, and 23 people with painful rotator cuff tendinopathy. Supraspinatus tendon thickness and acromiohumeral distance were measured using ultrasound scans before, and at three time points after loading (1, 6 and 24 hours). Loading involved isokinetic eccentric and concentric external rotation and abduction.
Results There was a significant increase in supraspinatus tendon thickness in the pain group at 1 (7%, ∆=0.38, 95% CI 0.19 to 0.57) and 6 hours (11%, ∆=0.53, 95% CI 0.34 to 0.71), although only the 6 hours difference exceeded minimal detectable difference. In contrast, there was a small non-significant reduction in thickness in controls. The acromiohumeral distance reduced significantly in both groups at 1 hour (controls: ∆=0.64, 95% CI 0.38 to 0.90; pain: ∆=1.1, 95% CI 0.85 to 1.33), with a larger change from baseline in the pain group.
Conclusion Those diagnosed with painful supraspinatus tendinopathy demonstrated increased thickening with delayed return to baseline following loading. Rehabilitation professionals may need to take into account the impact of loading to fatigue when planning rehabilitation programmes.
- shoulder
- tendinopathy
- exercise rehabilitation
- eccentric
- concentric
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings?
The supraspinatus tendon in painful shoulders significantly increased in thickness in response to acute fatigue loading compared with pain-free controls.
Loading the rotator cuff to fatigue also resulted in a reduced subacromial space, with recovery to baseline delayed up to 24 hours in people with painful rotator cuff tendinopathy.
Rehabilitation programmes for rotator cuff tendinopathy need to take into account the potential for increased tendon thickness and reduced subacromial space after loading, by allowing appropriate recovery periods after loading to fatigue.
Introduction
Mechanical loading induces positive adaptive changes in mechanical, morphological and biomechanical properties in healthy tendon.1 2 However, overloading may lead to tendinopathy, characterised by pain and reduced function.3 Tendon loading may therefore have both beneficial and detrimental effects on the tissue in both the short and long term.
There may be a differential effect of loading in normal (asymptomatic) and symptomatic tendons. A systematic review of the immediate effects of exercise on the Achilles tendon, reported that healthy Achilles tendons reduced in diameter immediately after exercise, in particular with eccentric contractions. In contrast, symptomatic Achilles tendons increased in thickness and MRI signal after eccentric and concentric loading indicating possible higher water content or tendon hyperaemia.4 Other studies support slower return to baseline tendon characteristics5 6 in those with tendinopathy. Therefore, it is important to compare both healthy and pathological tendons when evaluating loading responses.
Due to different functional roles and composition, the rotator cuff (RC) tendons may respond differently than the lower limb tendons, yet the response of the RC tendons to loading has not been extensively investigated. In one of the few studies to examine tendon responses in vivo in the upper limb, van Drongelen et al 7 examined acute changes in biceps tendon diameter in wheelchair athletes (a third of the athletes had shoulder pain) after a single basketball or rugby game. The authors reported a non-significant increase in tendon thickness and ultrasound echogenicity related to duration of play.
Impingement of the supraspinatus tendon due to acromial compression in a reduced subacromial space is a widely held pathomechanical theory for the development of RC tendinopathy.8 However, studies examining subacromial space, represented by the linear acromiohumeral distance (AHD), in RC tendinopathy do not consistently report changes compared with pain-free shoulders, except in those with substantial RC tendon tears.9 10 Increased supraspinatus tendon (SsT) thickness is a feature of RC tendinopathy.11 The interaction between a thickened tendon and a potentially reduced subacromial space was examined by Michener et al,12 calculating the occupation ratio (the ratio between supraspinatus thickness and AHD), in people with shoulder pain and age-matched controls. This study reported a thicker tendon in the group with shoulder pain resulting in a larger occupation ratio, despite no significant between-group difference in subacromial space.
These results suggest that tendon thickening may be an early pathological response that may subsequently lead to tendon compression as a secondary phenomenon, due to the larger tendon occupying a fixed subacromial space.12 While cross-sectional studies inform mechanisms of supraspinatus tendinopathy, it is important to examine these processes longitudinally in response to loading, as this better replicates the clinical presentation of painful RC tendinopathy. Therefore, the aim of this study was to examine the short-term effect of loading on thickness of the SsT and the AHD in people with and without painful RC tendinopathy.
Methods
Participants (both controls and shoulder pain group) were recruited from community-based settings. Controls were men and women aged over 18 years, and included if they were free of shoulder pain over the last year, had full pain-free range of motion (ROM), did not have neurological or systemic rheumatological disorders, history of shoulder fracture, dislocation or surgery or any contraindications to ultrasound imaging. Shoulder pain participants were men and women aged over 18 years with a current history of unilateral shoulder pain, but still able to undertake some physical exercise with their shoulder (defined as 15 min of moderate arm exercise, such as tennis or housework). They were excluded if they had bilateral shoulder pain, had ever undergone shoulder surgery, had >50% restriction of shoulder ROM (to rule out frozen shoulder), had any neurological or systemic rheumatological disorders or contraindications to ultrasound imaging. The study received ethical approval from the relevant Research Ethics Committee and all volunteers provided written informed consent.
The diagnosis of RC tendinopathy is challenging, with both imaging-based and clinical diagnostic approaches having significant flaws.13 While Hegedus et al reported that no shoulder clinical diagnostic tests in isolation provide an accurate diagnosis of pathology,14 a combination of five tests (painful arc, empty can, external rotation resistance, Neer and Hawkins and Kennedy) were best able to predict RC tendinopathy.15 A cut-off of three out of five positive tests was used to clinically confirm RC pathology,15 while less than three positive tests ruled it out. Control participants were required to have a maximum of two positive tests, with a minimum of three positive tests in the pain group. Tendon pathology has been reported in many imaging studies of symptom-free shoulders.13 To best reflect current clinical practice, we combined both clinical and ultrasound diagnoses for the symptomatic participants.
Ultrasound examinations were undertaken using a GE Logiq e ultrasound scanner (GE Medical, Wauwatosa, Wisconsin, USA), with a 12 MHz linear probe, by a physiotherapist also qualified as a musculoskeletal sonographer, specialising in shoulder and tendon imaging. To enhance validity, static ultrasound images were independently reviewed by a radiologist to confirm imaging diagnoses for the symptomatic group. To produce as homogeneous sample as possible, control participants were excluded at this stage if any tendinopathy (loss of the normal fibrillar structure of the tendon with an abnormally hypoechoic appearance), partial tear of the SsT (flattening of the tendon surface or presence of hypoechoic defect within, or on either surface of, the tendon) or full-thickness tears (focal defect extending from the bursal to the humeral side of the tendon, or complete non-visualisation of the tendon) was found. Only one control volunteer (who had met the clinical testing criteria) was excluded using these criteria. For participants with unilateral shoulder symptoms, the painful shoulder was required to show some evidence of tendon pathology, however volunteers with full-thickness tears were excluded.
All participants provided details of their age, height and weight. Those with shoulder pain recorded the nature and duration of their shoulder pain. A Numerical Pain Rating Scale (NRS) for average shoulder pain intensity,16 and the Shoulder Pain and Disability Index (SPADI) to assess shoulder disability,17 were also completed. The NRS was completed again at 24 hours postexercise.
Measurement of the SsT thickness and AHD were undertaken according to a previously published reliable protocol, with minimal detectable difference (MDD) values of 0.7 mm for AHD and 0.6 mm for SsT thickness.18 For the AHD measures, the participant was sitting, shoulder neutral, with the hand resting on the lap. An ultrasound image was taken with the transducer positioned along the line of the humerus, over the anterior part of the acromion, with the subacromial space and humeral head visible. The AHD was then measured as the shortest distance between the inferolateral edge of the anterior acromion and the humeral head, parallel to the acoustic shadow cast by the acromion.18
For the SsT measures, the arm was placed into the modified Crass position that is, palm of the hand on the iliac crest, with the elbow directed posteriorly. The SsT was viewed in the transverse plane, the transducer was moved anteriorly until the intra-articular portion of the long head of biceps was seen, at which point the image was taken. On-screen callipers were used to measure between the echogenic tendon boundaries, at points 5, 10 and 15 mm posterior to the edge of the biceps tendon, with the mean of these measures used for analysis. Subacromial occupation ratio expresses the relationship between tendon thickness and the space occupied, calculated by dividing SsT thickness by the AHD, expressed as a percentage. A normal subacromial bursa is either invisible or measures <2 mm on ultrasound.19 In this study, no participant had a subacromial bursa thicker than 2 mm at baseline or after exercise, therefore no further analysis of bursal thickness was carried out.
Measures of AHD and SsT thickness were obtained immediately before, and then at three intervals (1, 6 and 24 hours) postexercise. All images were taken by the same examiner, with the participant in the same position. All scans were coded to ensure blinding to group allocation and time the scan was taken at.
Immediately after the initial ultrasound measurements, participants performed the loading protocol in a seated position using an isokinetic dynamometer (System 3, Biodex Medical Systems, Shirley, New York, USA). The shoulder pain group exercised the painful shoulder; the control group exercised the shoulder randomly chosen by coin toss. Participants undertook a 5 min shoulder warm-up, involving range of motion exercises. The loading protocol involved two bouts of exercise; one of concentric and eccentric shoulder abduction, and a second of concentric and eccentric shoulder external rotation; with order of completion determined randomly by coin toss. The isokinetic protocol was based on that described by Roy et al, 20 where 60 repetitions at 60°/s resulted in mean fatigue levels of 38% for external rotation. For this study, we increased the speed to 120°/s in order to increase the tendon loading, and set the fatigue level at a 35% drop in overall torque for each of the exercise bouts. For external rotation, the participant was seated, arm in 45° abduction in the neutral plane and ROM was set at minimum arc of 45° for external rotation, commencing from a position of 20° internal rotation to at least 25° of external rotation. Abduction was performed in sitting, with the arm in the neutral plane, and ROM from neutral to as close to 90° as was tolerable for the participant. Three sets of 10 repetitions of each direction were completed with 10 s rest between sets. Additional sets were undertaken if the requisite fatigue level was not reached after completion of the prescribed sets, or testing was ceased if the required fatigue level was reached before the three sets were complete. Testing was also ceased if pain beyond usual resting levels was experienced, however all participants completed at least two sets of each movement direction. Participants were advised to refrain from any further exertion involving their shoulder until the 24 hours measures were taken.
Data were normally distributed. Significance level was set at P=0.05. Repeated measures analysis of variance (ANOVA) was used to model the changes in the tendon thickness and AHD compared with baseline over the subsequent three time points (1, 6 and 24 hours postexercise). A time by group interaction term was used to compare the change scores between the pain and control groups.
Results
A total of 20 healthy controls (mean age 43 years, range 28–59, 10 men) and 23 people with RC tendinopathy (mean age 47 years, range 23–67, 12 men) took part in the study. Demographic characteristics of participants were not significantly different between groups (table 1). Control participants completed slightly more exercise sets (mean 5.8) than the shoulder pain group (mean 4.9).
Participant characteristics
There was a significant reduction in SsT thickness in the control group 6 hours after exercise; however, the mean difference was small (0.2 mm, 4%, <MDD). There was no significant difference in SsT thickness relative to baseline at any other time point in the control group (table 2). There was a statistically significant increase in SsT thickness between baseline and the 1, 6 and 24 hours time points for the pain group; however, only the 6-hour difference (0.53 mm, 11%) reached the MDD. A significant time-by-group interaction term in a repeated measures ANOVA analysis indicated that the changes in SsT from baseline for the pain group were statistically different to the control group (time-by-group interaction: F(3,39) = 9.23, P<0.001).
Mean values of supraspinatus thickness and acromiohumeral distance for both groups and differences from baseline
Twelve participants from the RC tendinopathy group had SsT thickness increases that equalled or exceeded the MDD at 1 hour and/or 6 hours postexercise, and four of these had sustained thickness change at 24 hours. While too small for detailed analysis, these four participants were observed to have higher NRS pain scores at 24 hours postexercise, compared with the rest of the group with normalised tendon thickness.
There was a significant reduction in AHD between baseline and 1 hour postexercise in the control group, with a mean difference equal to the MDD. There was no difference in AHD between baseline and either the 6 or 24 hours measures for controls. There was a significant reduction in AHD at both 1 and 6 hours after exercise in the pain group, with the 1 hour difference exceeding MDD, while there was no difference at 24 hours. Repeated measures ANOVA analysis for AHD revealed a significant main effects for time (F(2,40)=42, P<0.001) and group (F(1,41) = 5.59, P=0.023), but no significant time-by-group interaction effect (P=0.454), indicating that the effects of time were similar in both groups but that the change scores from baseline were significantly greater in the pain group compared with the control group.
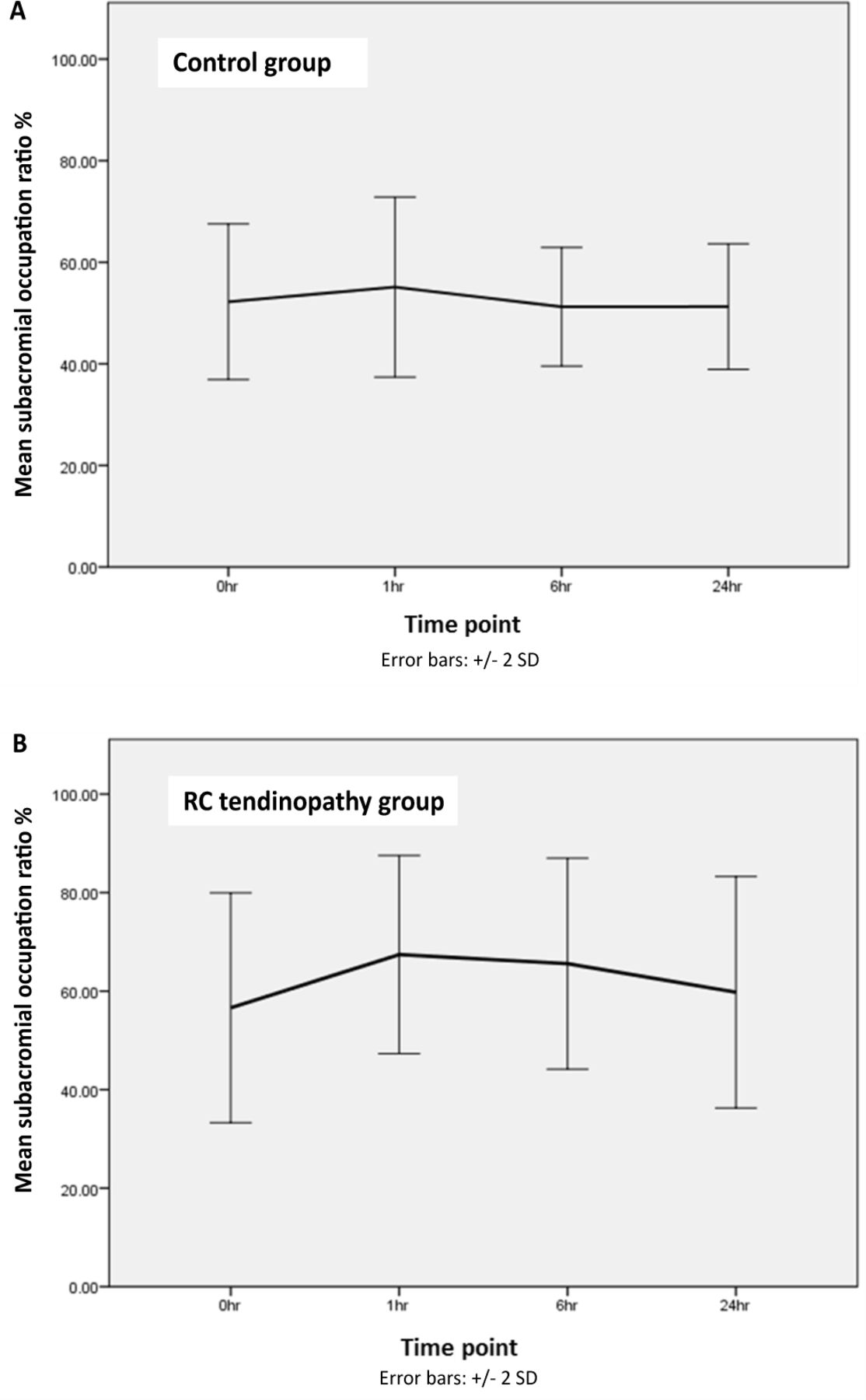
The occupation ratio (SsT as a percentage of AHD) increased in both groups over time, with a greater increase and slower return to baseline in the RC tendinopathy group as illustrated in figure 1A,B.
{kind=link}
Occupation ratio (supraspinatus tendon/acromiohumeral distance%) at baseline (0 hour) and three subsequent time points of 1, 6 and 24 hours postexercise for (A) controls and (B) painful shoulders. RC, rotator cuff; hr, hour.
Discussion
This study demonstrated that SsT thickness increased in people with painful RC tendinopathy 1 and 6 hours following isokinetic concentric and eccentric external rotation and abduction exercise, with only the increase in SsT thickness at 6 hours exceeding the MDD for this measure. Control tendons very slightly reduced in thickness in response to loading, but not beyond the relevant MDD. In addition, AHD was reduced in both groups 1 hour after exercise, with a significant reduction maintained only in the pain group at 6 hours. The composite measure, subacromial occupation ratio, was consequently also seen to rise at the 1 hour time point in both groups, returning towards baseline more rapidly in the control group.
Alterations in tendon fluid are the most commonly theorised mechanisms for short-term changes in tendon size or shape in vivo, matching those directly measured in vitro.21 Increased tendon glycosaminoglycan content in tendinopathy, causing more binding of water, may provide some explanation for the changes in fluid metabolism.22 Studies of the acute response of normal tendons to exercise have described a multitude of physiological processes including changes in vascularity,23 genetic expression24 and mechanical properties.25 Our results extend those of a number of studies of lower limb tendons, where pathological tendons exhibit an altered loading response compared with healthy tendon. People with Achilles tendinopathy have been found to have an altered response to loading, either in the form of a smaller initial reduction in tendon thickness (5% reduction vs 21% reduction in thickness in controls) and a slower return to normal tendon dimensions in response to eccentric exercise5 or as an increase in tendon thickness after concentric and eccentric exercise.6
Reductions in AHD have been noted in response to fatiguing shoulder exercise,26 27 as reflected in the current study. Both superior humeral migration27 and alterations in scapular alignment may contribute to this.26 Chopp et al 26 examined the mechanisms of subacromial space reduction with fatiguing exercise in 10 healthy volunteers. They reported that since the scapular alterations observed in their study (ie, increased posterior tilt) functioned to increase the subacromial space, the reduction in subacromial space was more likely to be due to increased superior humeral head migration, due to reduced RC muscle function. Our study is the first to examine both the AHD and SsT response to exercise simultaneously. It appears that a dynamic process operates, where fatigue can lead to superior humeral head migration, along with swelling of a pathological tendon, providing possible evidence for an interaction of intrinsic (tendon swelling) and extrinsic (tendon compression) mechanisms in painful RC tendinopathy. The subacromial occupation ratio, which incorporates both aspects, may help to indicate patients more at risk of compression due to a thickened tendon occupying a smaller subacromial space.
Current surgical approaches for RC tendinopathy tend to focus on extrinsic causes of tendon impingement, directed at altering acromial shape, an approach which has come under increasing scrutiny, due to equivalence of outcomes with more conservative approaches.13 The lack of enhanced effectiveness of acromioplasty suggests that the surgery may be targeting the incorrect mechanism of injury to the tendon. Restoring homeostasis to the RC tendons may be a more relevant treatment approach in early painful RC tendinopathy than surgical alteration of the coracoacromial arch.
In rehabilitation, while some exercise approaches emphasise the role of posture and scapular alignment to increase the subacromial space, most also include some elements directed towards tendon conditioning and pain relief.13 The findings of this study, as well as the work of Chopp et al,27 support exercise approaches designed to improve load tolerance of the RC tendons, as well as providing better control of humeral head depression. Ideal conditions for tendon adaptation to loading are the provision of adequate time, absence of further overloading, in addition to the right metabolic and mechanical environment.3 This study suggests that fatigue loading of the shoulder may produce unfavourable conditions for adaptation in people with RC tendinopathy. Swelling as a response to loading suggests altered tendon fluid metabolism, and a reduced subacromial space may increase vulnerability to compression. Titrating exercise to the appropriate form and intensity is a critical part of restoring normal tendon homeostasis. Clinicians prescribing exercise for people with RC tendinopathy may be advised to initially avoid loading to fatigue; however, this suggestion requires ongoing research enquiry. In addition, based on the recovery rate of >6 hours, it may be advisable to limit RC strengthening exercise to no more than one session per day, or possibly even longer intervals in the early stages of rehabilitation. Again, ongoing research is necessary to determine the individual’s optimal effective exercise dose.
We included both concentric and eccentric exercise in the study protocol as no literature examined the effect of exercise type on RC tendon morphology. It is possible that different responses may be elicited to each of these exercises in isolation; however, many sporting and occupational activities are composite movements, using a variety of contraction modes. Electromyographic studies by Tardo et al 28 and Reed et al,29 suggesting a role for supraspinatus in both external rotation and abduction, provided the basis for the choice of movement directions for this study; however, other shoulder movements may provide greater loading or a different response. The pain group performed slightly fewer exercise sets than the control group. The population studied were recruited from community and sports club settings, rather than from a clinical environment, with the aim of identifying people with less severe pain who could still perform the exercise protocol required by the study. It is possible that those with more severe shoulder pain might not be able to complete the protocol used in this study, or may have a different response.
Conclusion
The SsT responded immediately following fatiguing concentric and eccentric shoulder exercise, with increased and decreased thickness noted in those with and without RC tendinopathy, respectively. The AHD reduced in both groups, but recovered to baseline more slowly in those with shoulder pain. The occurrence of tendon swelling in response to fatigue loading potentially supports a theory of intrinsic tendon pathology as a primary event in RC tendinopathy. Rehabilitation programmes to restore tendon homeostasis are recommended in the early management of RC tendinopathy, with exercise type and dosage titrated to avoid excessive loading to fatigue.
References
Footnotes
Contributors KM, JSL and AD designed the study protocol, and received ethical approval. KM collected the data. KM and HP performed the statistical analysis. All authors read and approved the final manuscript.
Funding KM was supported by a Research Fellowship from the Health Research Board of Ireland to conduct this study.
Competing interests None declared.
Ethics approval The University of Limerick Faculty of Education and Health Sciences Ethics Committee(s) (Limerick, Ireland) approved this study. All participants gave written informed consent before data collection began.
Provenance and peer review Not commissioned; externally peer reviewed.